Abstract
Osteoporosis is a chronic disease and public health issue in aging populations. Inadequate intake of micronutrients increases the risk of bone loss during an adult’s lifespan and therefore of osteoporosis. The aim of the study was to analyze the effects of consumption of biofortified crops with the micronutrient molybdenum (Mo) on bone remodeling and metabolism in a population of adults and seniors. The trial enrolled 42 senior and 42 adult people randomly divided into three groups that consumed lettuce biofortified with molybdenum (Mo-biofortified group) or without biofortification (control group) or molybdenum in a tablet (Mo-tablet group) for 12 days. We chose an experimental period of 12 days because the bone remodeling marker levels are influenced in the short term. Therefore, a period of 12 days allows us to determine if there are changes in the indicators. Blood samples, obtained at time zero and at the end of the study, were compared within the groups adults and seniors for the markers of bone resorption, C-terminal telopeptide (CTX) and bone formation osteocalcin, along with the markers of bone metabolism, parathyroid hormone (PTH), calcitonin, albumin-adjusted calcium, vitamin D, phosphate and potassium. Consumption of a Mo tablet did not affect bone metabolism in the study. Consumption of Mo-biofortified lettuce significantly reduced levels of CTX and PTH and increased vitamin D in adults and seniors while levels of osteocalcin, calcitonin, calcium, potassium and phosphate were not affected. The study opens up new considerations about the role of nutrition and supplementation in the prevention of chronic diseases in middle-aged and older adults. Consumption of Mo-biofortified lettuce positively impacts bone metabolism in middle-aged and older adults through reduced bone resorption and improved bone metabolism while supplementation of Mo tablets did not affect bone remodeling or metabolism. Therefore, Mo-biofortified lettuce may be used as a nutrition intervention to improve bone homeostasis and prevent the occurrence of osteoporosis in the elderly.
Keywords:
nutrition; human health; Lactuca sativa L.; micronutrients; supplementation; gut-bone axis 1. Introduction
Aging is associated with a decline of functional capacity and the inability to adapt to stress responses. The aging condition itself impacts the physiological performance of the human body and increases the susceptibility to age-related diseases and death. Common conditions in older age are reduction in metabolism (e.g., glucose, lipid, bone, skeletal muscle) and reduction in hearing and eyesight [1]. There is general bone and central nervous system deterioration, although new pieces of evidence suggest that the aging process can be delayed and modifiable [2]. Osteoporosis is an age-related disease that results in reduced bone mass, disruption of bone architecture and increased risk of fractures [3]. At a molecular biology level, deregulation in signals and pathways of Wnt, RUNX2, RANKL, OPG, Osx, CBFB, BMP-2, FoxOs, Nrf2, Gsα and sclerostin leads to osteoporosis [4]. For example, changes at the genetic and epigenetic levels may lower or over-activate the Wnt signaling pathway and thereby cause osteoporosis. In addition, the mutations in LRP5 cause osteoporosis-pseudoglioma syndrome (OPPG) autosomal disorder [5]. Thus, the Wnt signaling pathway is a candidate for therapeutic intervention for osteoporosis [6]. There are several risk factors accounting for osteoporosis development; some are unmodifiable, such as age, gender, menopause, previous fractures, family history [1] and medication, and some can be amended, such as lifestyle issues, including diet [7] exercise, smoking and alcohol [8]. Adequate nutrition, in terms of macronutrients and micronutrients, can have a central role in osteoporosis prevention and treatment.
Micronutrient needs for optimizing well-being in theory can be met by a healthy diet. However, most of the population does not have such a diet, especially during times when their well-being is challenged [3,7,9,10,11]. Among different agronomic practices [12,13,14], agronomic biofortification is recognized as one of the most promising, efficient, sustainable and cost-effective strategies for overcoming mineral malnutrition [15,16,17,18,19,20]. Therefore, biofortified food could be considered a good option for meeting nutrient needs during different stages of life and aging [21]. It could be easily supported by sustainable, safe agriculture [22] and prescribed together with a nutritious diet [7,10,23].
Molybdenum (Mo) is a micronutrient essential for many processes in the body. A Mo cofactor activates essential enzymes, such as sulfite oxidase, aldehyde oxidase, xanthine oxidase and mitochondrial amidoxime reducing component (mARC) [24]. It is contained in soil and transferred to us when we consume plants, legumes and grains, as well as animals that fed on those [25]. Remarkably, molybdenum is rapidly excreted in urine [26]. The recommended dietary allowance (RDA) is 45 μg/day and the biomonitoring equivalent (BE) molybdenum values associated with toxicity in serum and urine are 31 μg/L and 7500 μg/L, respectively. These values were calculated by considering the tolerable daily intake exposure guidance values and the reference dose [27]. In one study, a nutritional intervention with Mo-biofortified lettuce ameliorated iron metabolism in healthy adult individuals [28]. Furthermore, in another, the ingestion of Mo-enriched lettuce improved glucose homeostasis by increasing, within the physiological range, endogenous gut peptide levels of peptide YY (PYY) and gastric inhibitory polypeptide (GIP) [29]. Gut peptides are released following food intake, and they are able to influence bone remodeling [30,31] and inhibit bone resorption [32]. Hence, we hypothesized that bone turnover would be influenced by a short-term nutritional intervention with biofortified molybdenum lettuce and it would impact the essential regulators of bone metabolism such as calciotropic hormones and markers of calcium metabolism. Therefore, this nutritional research aimed to investigate whether 12 days of consumption of Mo-biofortified lettuce could affect bone turnover markers in a population of adults and seniors. Furthermore, we compared the obtained results to a cohort of people supplemented with a molybdenum tablet in their diet.
2. Materials and Methods
2.1. Research Design of the Study
This research is part of the larger project, Nutri-Mo-Food, that is registered at Clinicaltrials.gov (accessed on 12 February 2023) with the approbation number NCT04985240. The protocol, conducted in accordance with the Declaration of Helsinki, was approved by the Palermo University Hospital Ethics Committee, and the approbation number is 2/2020 AIFA CE 150109. From an initial 95 subjects (47 adults age range 23–54 and 48 seniors age range 55–73), on the basis of the eligibility criteria, 11 subjects were excluded (5 in the adults and 6 in the senior group), and 84 subjects (42 adults comprising 25 males and 17 females and 42 seniors comprising 24 males and 18 females) were randomized into the control group, the Mo-tablet and the biofortified group for a total of 14 subjects in each group of adults and seniors (Figure 1). The participants at the study, the medical staff and the investigator staff were blinded to the allocation during the whole period of data collection. The investigators were also blinded during the sample assessment and data analysis. The control group received 100 g of lettuce and the intervention group received 100 g of Mo-fortified lettuce to consume every day for a total of 12 days. The molybdenum supplementation tablet (150 µg/tablet) was purchased from Zein-pharma (Germany). The Mo-tablet group received one tablet of Mo to consume daily for a total of 12 days. Samples of blood were collected before (T0) and at the end (T1) of the trial, after 12 days (Figure 2).
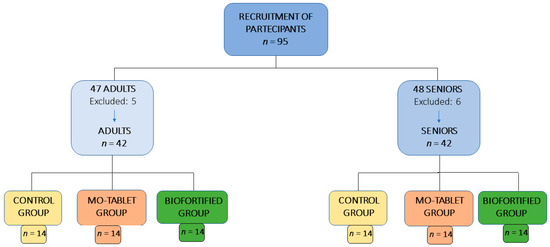
Figure 1.
Process of participants’ recruitment in the study.
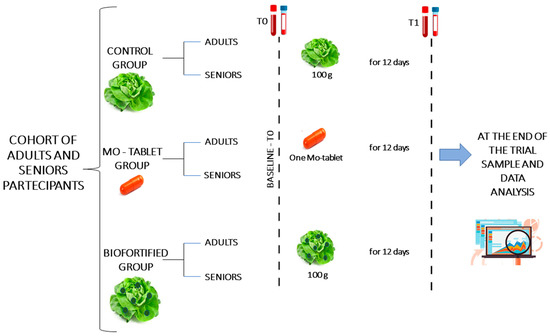
Figure 2.
Overview of the experimental design. Samples of blood were taken at baseline and after 12 days. The control group consumed 100 g of lettuce containing 0.21 mg of sodium molybdate, and the intervention group consumed 100 g of Mo-biofortified lettuce containing 8 mg of sodium molybdate every day for a total of 12 days. The Mo-tablet group was supplied with one tablet of Mo containing 150 µg of sodium molybdate every day for a total of 12 days. Biofortification of lettuce with molybdenum was used, with a dose of 3 µmol Mo L−1 supplied in foliar spray as sodium molybdate (Na2MoO4) during the period of growth [17].
Exclusion and inclusion criteria are reported in Table 1.

Table 1.
Characteristics of the study participants defined by eligibility criteria.
In the first visit, the subjects underwent anthropometric measurement and completed a habitual dietary intake assessment [23]. Participants were recommended not to change their habits and diet during the study period, which was reiterated throughout the study. Body composition (fat and lean mass) was measured by electrical bioimpedance measurements (InBody 320 Body Composition Analyzer). Barefoot standing height and body weight were measured by using a wall-mounted stadiometer (Gima 27088, Italy) and an electronic scale (Gima 27335) [30]. Body mass index (BMI) was reported as weight, measured in kilograms, per standing height, measured as meters squared.
2.2. Sample Size
We conducted an a priori power calculation based on previous studies with hematological parameters [29,30,33], and by setting a level of statistical significance for α of 5% and a probability for β of 20%, we estimated a sample size of eight participants was required in each group. We included 14 subjects in the study to reduce the type-two error risks and to enhance the power of evaluation for the secondary outcomes.
2.3. Analysis of the Bone Markers and Metabolism
The samples of blood were collected at the same time of day, in the morning between 07:00 and 08:00 a.m., in order to reduce the circadian variation. The samples were collected after overnight fasting from 8:00 p.m. the day before. The blood was dispensed in EDTA tubes for plasma collection (centrifugation at 1509× g for 10 min at 4 °C) while it was dispensed in VACUETTE ® serum tubes and allowed to clot for 30 min at room temperature before centrifugation for serum collection. Samples were analyzed by using a method that is FDA cleared and CE marked. Specifically, electro-chemiluminescence immunoassay (ECLIA) (Roche Diagnostics, Burgess Hill, UK) on a Cobas e601 analyzer for dosage in sample serum of CTX, cat. number 11972308122, vitamin D, cat. number 07464215190, osteocalcin, cat. number 12149133122, PTH, cat. number 11972103122 and calcitonin, cat. number 06445853190. We used Roche COBAS c501 and standard commercial assays supplied by Roche Diagnostics for dosage in plasma samples of calcium, cat. number 106443, albumin, cat. number 05166861, phosphate, cat. number 05171377 and potassium, cat. number 11208764202. The total calcium concentrations may change independently of the ionized calcium concentration because of fluctuations in albumin protein concentrations. Therefore, the concentration of calcium was corrected using the following equation: (−0.8 × ([albumin] − 4)) + [total Ca] to give an albumin-adjusted calcium (aa calcium) value [34].
2.4. Statistical Analysis
Student’s t tests were used to analyze and compare the characteristics at baseline of the study groups, and one-way ANOVA followed by Tukey’s post-test were used to compare differences between baseline and time 1. p ≤ 0.05 was considered statistically significant. Data are presented as means ± standard deviations.
3. Results
The anthropometric data of the participants enrolled in the study are shown in Table 2 for the beginning (baseline), before starting the nutritional intervention. There were no significant changes in BMI, body weight or lean and fat body masses within the groups during the nutritional protocol intervention.
Table 2.
Characteristics of participants at the beginning of the study (baseline, T0). Values are indicated as means ± standard deviations (SD).
3.1. Mo-Biofortified Lettuce and Markers of Bone Remodeling
The nutritional intervention with Mo-biofortified lettuce significantly affected circulating concentrations of CTX, the marker of bone resorption. In fact, in the Mo-biofortified group, plasma concentrations of CTX were significantly reduced after 12 days compared to baseline (Figure 3A). In the adult group, the serum concentration of CTX at the end of the nutritional intervention decreased by 52% from baseline (0.47 ± 0.1 vs. 0.24 ± 0.1 µg/L). In the senior group, the serum concentration of CTX at the end of the nutritional intervention decreased by 58% from baseline (0.48 ± 0.2 vs. 0.28 ± 0.1 µg/L). The CTX concentration detected was within the physiological range in both adult and senior groups. Osteocalcin, the marker of bone formation, was not affected by the nutritional intervention with Mo-biofortified lettuce after 12 days compared to baseline (adults: 22.5 ± 8 vs. 21.6 ± 6 µg/L; seniors 21.1± 7.2 vs. 20.7 ± 5.7 µg/L) (Figure 3B). In the control group of both adults and seniors who consumed lettuce for 12 days, there were no differences in the bone remodeling markers compared to baseline at the end of the intervention (Figure 3). Moreover, consumption of a Mo-tablet for 12 days did not affect markers of bone remodeling in adults or seniors within the group with respect to the control group (Figure 3). The Mo-tablet group was supplemented with a tablet of Mo containing 150 µg of sodium molybdate and the Mo-biofortified group was supplemented with 100 g a day of molybdenum-enriched lettuce containing 8 mg of sodium molybdate.
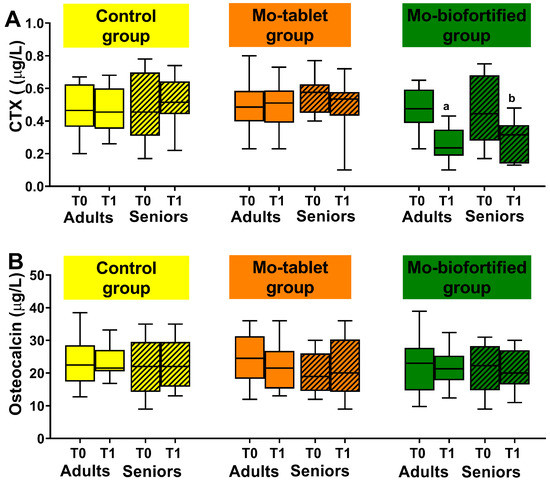
Figure 3.
Bone remodeling markers were measured at baseline and after 12 days in the three groups: the control group (supplemented once a day with 100 g a day of lettuce), the Mo-tablet group (supplemented once a day with molybdenum in tablet form) and the Mo-biofortified group (supplemented with 100 g a day of molybdenum-biofortified lettuce). (A) Box plot showing serum concentration of the marker of bone resorption, CTX, in control, Mo-tablet and Mo-biofortified groups. (B) Box plot showing serum concentration of the marker of bone formation, osteocalcin, in control, Mo-tablet and Mo-biofortified groups. The letter a denotes a significant difference (p < 0.05) of Mo-biofortified lettuce compared with the control (T0 and T1), Mo tablet (T0 and T1) and T0 of Mo-biofortified lettuce in the adult group. The letter b denotes a significant difference (p < 0.05) of Mo-biofortified lettuce compared with the control (T0 and T1), Mo tablet (T0 and T1) and T0 of Mo-biofortified lettuce in the senior group.
The comparisons between the groups (control vs. Mo-biofortified and Mo-tablet vs. Mo-biofortified) showed significant changes in CTX but not in the osteocalcin concentration after 12 days of nutritional intervention in the Mo-biofortified group with respect to the control and Mo-tablet groups in both adults and seniors (Figure 3).
3.2. Mo-Biofortified Lettuce and Markers of Bone Metabolism
The nutritional intervention with Mo-biofortified lettuce significantly affected the marker of bone metabolism, PTH. In the Mo-biofortified group, PTH concentrations decreased with time. Specifically, PTH at baseline was significantly different from day 12 (adults: 36.5 ± 8.3 vs. 22.3 ± 6.7 ng/L; seniors: 42.4 ± 8 vs. 32.8 ± 5.4 ng/L) (Figure 4A). The PTH levels at the end of the nutritional intervention were decreased by 39% from baseline in adults and by 23% in seniors. Moreover, the nutritional intervention increased the level of vitamin D. In fact, it significantly increased after 12 days from 29 ± 7.3 µg/L (baseline) to 46 ± 8.5 µg/L in the adult biofortified group (Figure 4B). Meanwhile, the increase in vitamin D was from 28.4 ± 7.1 µg/L (baseline) to 44 ± 10 µg/L in the seniors biofortified group. Calcium, phosphate, calcitonin and potassium levels did not differ between baseline and time 1 (Figure 4C–F). The concentrations detected were within the normal range. In the control and Mo-tablet groups, there were no changes in the bone metabolism markers at time 1 compared to baseline (Figure 4). The comparison between the groups (control vs. biofortified and Mo-tablet vs. biofortified) showed that there were significant changes in the PTH and vitamin D in the Mo-biofortified group compared to the control group and the Mo-tablet group in both adults and seniors (Figure 4A,B). Calcium, calcitonin, phosphorus and potassium were not affected by the nutritional intervention (Figure 4C–F).
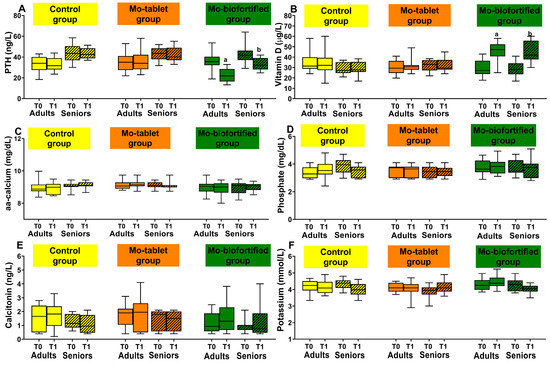
Figure 4.
Bone metabolism markers were measured at baseline and after 12 days in the three groups: the control group (supplemented with 100 g a day of lettuce), the Mo-tablet group (supplemented once a day with molybdenum in tablet form) and the Mo-biofortified group (supplemented with 100 g a day of molybdenum-enriched lettuce). (A) Box plot showing concentration of PTH in control, Mo-tablet and Mo-biofortified groups. (B) Box plot showing concentration of vitamin D in control, Mo-tablet and Mo-biofortified groups. (C) Box plot showing concentration of aa calcium in control, Mo-tablet and Mo-biofortified groups. (D) Box plot showing concentration of phosphate in control, Mo-tablet and Mo-biofortified groups. (E) Box plot of calcitonin in control, Mo-tablet and Mo-biofortified groups. (F) Box plot showing concentration of potassium in control, Mo-tablet and Mo-biofortified groups. The letter a denotes a significant difference (p < 0.05) of Mo-biofortified lettuce compared with the control (T0 and T1), Mo tablet (T0 and T1) and T0 of Mo-biofortified lettuce in the adult group. The letter b denotes a significant difference (p < 0.05) of Mo-biofortified lettuce compared with the control (T0 and T1), Mo tablet (T0 and T1) and T0 of Mo-biofortified lettuce in the senior group.
4. Discussion
New requests in food and human nutrition are arising, with the goals of ensuring well-being, longevity and sustainability of resources, especially in aging. Thus, innovative nutritional interventions in the field are required. In the present study, we investigated the impact of the micronutrient molybdenum provided through a vegetable matrix in a cohort of adult and senior participants.
Before this work, no studies had investigated the effect of a Mo-biofortified crop on bone homeostasis in the human population. A previous study, conducted in rabbits, showed that molybdenum supplementation of the diet increased the deposition of calcium in the femur bone by 22% [35], highlighting the importance of dietary molybdenum supplementation for optimal bone metabolism.
We used a vegetable matrix (lettuce) as a carrier to supplement the diet with molybdenum. Our previous studies suggested a vegetable matrix was a good carrier for the mineral because the concentration of Mo was within the physiological range in serum and urine [28]. Thus, in the present study, we investigated the effect on bone metabolism and tested the effect with respect to a Molybdenum tablet supplementation group.
Biofortification using vegetable matrix (lettuce) was chosen because vegetables are consumed by most of the population. In this set up, we analyzed the effect on bone homeostasis and metabolism in the cohort of participants, and the results were compared within and between the groups. We found that consumption of 100 g of Mo-biofortified lettuce was able to improve bone homeostasis in the groups, while supplementation of molybdenum in tablets for 12 days did not affect the bone markers. The crop, consumed by the study population every day in a quantity of 100 g per day, contained 0.21 mg of sodium molybdate for the control group and 8 mg of sodium molybdate for the Mo-biofortified group. The tablet of molybdenum contained 150 µg of sodium molybdate. This quantity of molybdenum was chosen because 45 μg/day is the recommended dietary allowance of molybdenum [26] but deficiencies occur at low intakes, while excesses are eliminated at high intakes. An average intake of 65 µg/day of molybdenum was proposed for adults by the EFSA, while a tolerable upper intake level (UL) of 0.9 mg/kg body weight per day [36] has shown no adverse effect because it is used up in the body. This is very important because it reduces the risks of toxicity or deficiency, and molybdenum is fast eliminated in the urine [37]. Therefore, we provided a quantity of molybdenum that was safe (in line with the biomonitoring equivalent values fixed to protect against deficits and nutritional toxicity, and very distant from 31 μg/L, which is the biomonitoring equivalent toxicity value reported for plasma and serum) [27]. The serum level of molybdenum was 5 μg/L at baseline [38] and reached 6 μg/L with the intake of 150 µg of sodium molybdate in tablet form [39] and 7 μg/L with the intake of biofortified lettuce for 12 days [28].
Scientists agree that the nutritional recommendations on micronutrients should be adjusted to improve the metabolism [40,41]. This is necessary, for example, to reduce mitochondrial decay, a hallmark of aging, related to many disease processes. The idea that higher doses than the current recommendation may be necessary for preserving body homeostasis of specific tissue, such as bone tissue in the elderly, is supported by studies in the field, showing that the elderly can benefit from increased quantities of micronutrients, for example, calcium and vitamin D [42]. In the present study, a micronutrient’s effect was observed in reductions in circulating markers of bone resorption, CTX and PTH, indicating slowing of bone resorption in response to the mineral supplementation of Mo-biofortified lettuce, but not when participants were given molybdenum supplied in tablet form. Moreover, the nutritional intervention affected vitamin D levels. Vitamin D can influence bone homeostasis, both directly and indirectly. Vitamin D regulates serum calcium and phosphate levels for optimal skeletal mineralization. It influences calcium absorption and reabsorption from bone and the kidneys [43]. The mineral supplementation with the Mo-biofortified lettuce increased vitamin D levels in adults and seniors, confirming the ability of the nutritional intervention to impact two of the main regulators of bone metabolism, vitamin D and PTH. Vitamin D exerts a negative feedback on PTH [44]. Presently, we do not know the exact mechanism of action. The effect of consumption of Mo-biofortified lettuce on bone metabolism could be indirect by modulation of the gut peptide GIP and PYY levels, which are known to inhibit bone resorption [29,32,45]. However, considering the molybdenum function as an essential cofactor for mitochondrial bone physiology [46], it is possible to hypothesize that consumption of Mo-biofortified lettuce boosts the mitochondrial function and reduces osteoclast activity. Mitochondrial function is essential in the maintenance of osteoblasts’ and osteoclasts’ activity in bone. Mitochondrial dysfunction not only impairs osteogenesis but also increases osteoclast activity [47]. This accelerates age-related bone loss. Therefore, consumption of molybdenum through biofortification for 12 days could lead to optimal mitochondrial function that ameliorates bone mineral homeostasis.
In conclusion, this study showed that mineral supplementation with Mo-biofortified lettuce (8 mg/day) for 12 days in a cohort of adult and senior participants reduced bone resorption and PTH and increased vitamin D levels. Molybdenum supplementation using one tablet a day (150 ug/day) of Mo did not show any influence on the same bone markers during the intervention. The results are encouraging for preservation of bone health, especially in the elderly.
Author Contributions
Conception S.B. and S.V.; performance of work S.B., L.D.R., S.V., D.B. and L.S.; interpretation of data S.B., S.V. and R.C.; writing the article S.B. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by FFR 2023 to Sara Baldassano.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Palermo University Hospital Ethics Committee Policlinico Paolo Giaccone approbation number 150109 AIFA CE of 2 February 2020 Univerity of Palermo.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available on request due to privacy/ethical restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hussain, S.M.; Ebeling, P.R.; Barker, A.L.; Beilin, L.J.; Tonkin, A.M.; McNeil, J.J. Association of Plasma High-Density Lipoprotein Cholesterol Level With Risk of Fractures in Healthy Older Adults. JAMA Cardiol. 2023, e225124. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-K. Antiaging agents: Safe interventions to slow aging and healthy life span extension. Nat. Prod. Bioprospect. 2022, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Proia, P.; Amato, A.; Drid, P.; Korovljev, D.; Vasto, S.; Baldassano, S. The Impact of Diet and Physical Activity on Bone Health in Children and Adolescents. Front. Endocrinol. 2021, 12, 704647. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Patil, S.; Jia, J. The Development of Molecular Biology of Osteoporosis. Int. J. Mol. Sci. 2021, 22, 8182. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Slee, R.B.; Fukai, N.; Rawadi, G.; Roman-Roman, S.; Reginato, A.M.; Wang, H.; Cundy, T.; Glorieux, F.H.; Lev, D.; et al. LDL receptor-related protein 5 (LRP5) affects bone accrual and eye development. Cell 2001, 107, 513–523. [Google Scholar] [CrossRef]
- Baron, R.; Gori, F. Targeting WNT signaling in the treatment of osteoporosis. Curr. Opin. Pharm. 2018, 40, 134–141. [Google Scholar] [CrossRef]
- Amato, A.; Baldassano, S.; Cortis, C.; Cooper, J.; Proia, P. Physical activity, nutrition, and bone health. Hum. Mov. 2018, 19, 1–10. [Google Scholar] [CrossRef]
- Wilson-Barnes, S.L.; Lanham-New, S.A.; Lambert, H. Modifiable risk factors for bone health & fragility fractures. Best Pract. Res. Clin. Rheumatol. 2022, 36, 101758. [Google Scholar] [CrossRef]
- Messina, G.; Amato, A.; D’Amico, G.; Baldassano, S.; Proia, P. Effects of protein supplementation in fitness world: A 12-week cross-over studio. J. Hum. Sport Exerc. 2019, 15, S308–S314. [Google Scholar] [CrossRef]
- Baldassano, S.; Accardi, G.; Vasto, S. Beta-glucans and cancer: The influence of inflammation and gut peptide. Eur. J. Med. Chem. 2017, 142, 486–492. [Google Scholar] [CrossRef]
- Baldassano, S.; Alioto, A.; Amato, A.; Rossi, C.; Messina, G.; Bruno, M.R.; Stallone, R.; Proia, P. Fighting the Consequences of the COVID-19 Pandemic: Mindfulness, Exercise, and Nutrition Practices to Reduce Eating Disorders and Promote Sustainability. Sustainability 2023, 15, 2120. [Google Scholar] [CrossRef]
- Consentino, B.B.; Virga, G.; La Placa, G.G.; Sabatino, L.; Rouphael, Y.; Ntatsi, G.; Iapichino, G.; La Bella, S.; Mauro, R.P.; D’Anna, F.; et al. Celery (Apium graveolens L.) Performances as Subjected to Different Sources of Protein Hydrolysates. Plants 2020, 9, 1633. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, L. Morphological and agronomical characterization of eggplant genetic resources from the Sicily area. J. Food Agric. Environ. 2013, 1111, 401–404. [Google Scholar]
- Sabatino, L.; Consentino, B.B.; Ntatsi, G.; La Bella, S.; Baldassano, S.; Rouphael, Y. Stand-Alone or Combinatorial Effects of Grafting and Microbial and Non-Microbial Derived Compounds on Vigour, Yield and Nutritive and Functional Quality of Greenhouse Eggplant. Plants 2022, 11, 1175. [Google Scholar] [CrossRef]
- Buturi, C.V.; Sabatino, L.; Mauro, R.P.; Navarro-León, E.; Blasco, B.; Leonardi, C.; Giuffrida, F. Iron Biofortification of Greenhouse Soilless Lettuce: An Effective Agronomic Tool to Improve the Dietary Mineral Intake. Agronomy 2022, 12, 1793. [Google Scholar] [CrossRef]
- Sabatino, L.; Di Gaudio, F.; Consentino, B.B.; Rouphael, Y.; El-Nakhel, C.; La Bella, S.; Vasto, S.; Mauro, R.P.; D’Anna, F.; Iapichino, G.; et al. Iodine Biofortification Counters Micronutrient Deficiency and Improve Functional Quality of Open Field Grown Curly Endive. Horticulturae 2021, 7, 58. [Google Scholar] [CrossRef]
- Sabatino, L.; Consentino, B.B.; Rouphael, Y.; De Pasquale, C.; Iapichino, G.; D’Anna, F.; La Bella, S. Protein Hydrolysates and Mo-Biofortification Interactively Modulate Plant Performance and Quality of ‘Canasta’ Lettuce Grown in a Protected Environment. Agronomy 2021, 11, 1023. [Google Scholar] [CrossRef]
- La Bella, S.; Consentino, B.B.; Rouphael, Y.; Ntatsi, G.; De Pasquale, C.; Iapichino, G.; Sabatino, L. Impact of Ecklonia maxima Seaweed Extract and Mo Foliar Treatments on Biofortification, Spinach Yield, Quality and NUE. Plants 2021, 10, 1139. [Google Scholar] [CrossRef]
- Sabatino, L.; La Bella, S.; Ntatsi, G.; Iapichino, G.; D’Anna, F.; De Pasquale, C.; Consentino, B.B.; Rouphael, Y. Selenium biofortification and grafting modulate plant performance and functional features of cherry tomato grown in a soilless system. Sci. Hortic. 2021, 285, 110095. [Google Scholar] [CrossRef]
- Sabatino, L.; D’Anna, F.; Iapichino, G.; Moncada, A.; D’Anna, E.; De Pasquale, C. Interactive Effects of Genotype and Molybdenum Supply on Yield and Overall Fruit Quality of Tomato. Front. Plant Sci. 2018, 9, 1922. [Google Scholar] [CrossRef]
- Biesalski Hans, K.; Jana, T. Micronutrients in the life cycle: Requirements and sufficient supply. NFS J. 2018, 11, 1–11. [Google Scholar] [CrossRef]
- Consentino, B.B.; Ciriello, M.; Sabatino, L.; Vultaggio, L.; Baldassano, S.; Vasto, S.; Rouphael, Y.; La Bella, S.; De Pascale, S. Current Acquaintance on Agronomic Biofortification to Modulate the Yield and Functional Value of Vegetable Crops: A Review. Horticulturae 2023, 9, 219. [Google Scholar] [CrossRef]
- Baldassano, S.; Accardi, G.; Aiello, A.; Buscemi, S.; Di Miceli, G.; Galimberti, D.; Candore, G.; Ruisi, P.; Caruso, C.; Vasto, S. Fibres as functional foods and the effects on gut hormones: The example of β-glucans in a single arm pilot study. J. Funct. Foods 2018, 47, 264–269. [Google Scholar] [CrossRef]
- Reiss, J.; Hahnewald, R. Molybdenum cofactor deficiency: Mutations in GPHN, MOCS1, and MOCS2. Hum. Mutat. 2011, 32, 10–18. [Google Scholar] [CrossRef]
- Novotny, J.A. Molybdenum Nutriture in Humans. J. Evid.-Based Complement. Altern. Med. 2011, 16, 164–168. [Google Scholar] [CrossRef]
- Otten, J.; Hellwig, J.; Meyers, L. (Eds.) Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; National Academies Press: Washington, DC, USA, 2007; Volume 85, p. 924. [Google Scholar]
- Hays, S.M.; Macey, K.; Poddalgoda, D.; Lu, M.; Nong, A.; Aylward, L.L. Biomonitoring Equivalents for molybdenum. Regul Toxicol Pharm. 2016, 77, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Baldassano, S.; Polizzi, M.R.; Sabatino, L.; Caldarella, R.; Macaluso, A.; Alongi, A.; Caldara, G.F.; Ferrantelli, V.; Vasto, S. A New Potential Dietary Approach to Supply Micronutrients to Physically Active People through Consumption of Biofortified Vegetables. Nutrients 2022, 14, 2971. [Google Scholar] [CrossRef] [PubMed]
- Vasto, S.; Di Gaudio, F.; Raso, M.; Sabatino, L.; Caldarella, R.; De Pasquale, C.; Di Rosa, L.; Baldassano, S. Impact on Glucose Homeostasis: Is Food Biofortified with Molybdenum a Workable Solution? A Two-Arm Study. Nutrients 2022, 14, 1351. [Google Scholar] [PubMed]
- Vasto, S.; Amato, A.; Proia, P.; Baldassano, S. Is the Secret in the Gut? SuperJump Activity Improves Bone Remodeling and Glucose Homeostasis by GLP-1 and GIP Peptides in Eumenorrheic Women. Biology 2022, 11, 296. [Google Scholar] [CrossRef] [PubMed]
- Amato, A.; Proia, P.; Caldara, G.F.; Alongi, A.; Ferrantelli, V.; Baldassano, S. Analysis of Body Perception, Preworkout Meal Habits and Bone Resorption in Child Gymnasts. Int. J. Environ. Res. Public Health 2021, 18, 2184. [Google Scholar] [CrossRef]
- Schiellerup, S.P.; Skov-Jeppesen, K.; Windeløv, J.A.; Svane, M.S.; Holst, J.J.; Hartmann, B.; Rosenkilde, M.M. Gut Hormones and Their Effect on Bone Metabolism. Potential Drug Therapies in Future Osteoporosis Treatment. Front. Endocrinol. 2019, 10, 75. [Google Scholar] [CrossRef] [PubMed]
- Baldassano, S.; Di Gaudio, F.; Sabatino, L.; Caldarella, R.; De Pasquale, C.; Di Rosa, L.; Nuzzo, D.; Picone, P.; Vasto, S. Biofortification: Effect of Iodine Fortified Food in the Healthy Population, Double-Arm Nutritional Study. Front. Nutr. 2022, 9, 426. [Google Scholar] [CrossRef] [PubMed]
- Vasto, S.; Amato, A.; Proia, P.; Caldarella, R.; Cortis, C.; Baldassano, S. Dare to Jump: The Effect of New High Impact Activity SuperJump on Bone Remodeling. A New Tool to Be Fit During COVID-19 Home Confinement. Biol. Sport 2022, 39, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Khandare, A.L.; Suresh, P.; Kumar, P.U.; Lakshmaiah, N.; Manjula, N.; Rao, G.S. Beneficial effect of copper supplementation on deposition of fluoride in bone in fluoride- and molybdenum-fed rabbits. Calcif. Tissue Int. 2005, 77, 233–238. [Google Scholar] [CrossRef]
- EFSA. Scientific Opinion on Dietary Reference Values for molybdenum. EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). EFSA J. 2013, 11, 3333. [Google Scholar] [CrossRef]
- Medeiros, D.M. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements edited by JJ Otten, JP Hellwig, and LD Meyers, 2006, 560 pages, hardcover, $44.96. The National Academies Press, Washington, DC. Am. J. Clin. Nutr. 2007, 85, 924. [Google Scholar] [CrossRef]
- Liu, N.; Guan, Y.; Li, B.; Yao, S. Biomonitorization of concentrations of 28 elements in serum and urine among workers exposed to indium compounds. PLoS ONE 2021, 16, e0246943. [Google Scholar] [CrossRef]
- Novotny, J.A.; Turnlund, J.R. Molybdenum intake influences molybdenum kinetics in men. J. Nutr. 2007, 137, 37–42. [Google Scholar] [CrossRef]
- Killilea, D.W.; Killilea, A.N. Mineral requirements for mitochondrial function: A connection to redox balance and cellular differentiation. Free Radic. Biol. Med. 2022, 182, 182–191. [Google Scholar] [CrossRef]
- Ames, B.N.; Wakimoto, P. Are vitamin and mineral deficiencies a major cancer risk? Nat. Rev. Cancer 2002, 2, 694–704. [Google Scholar] [CrossRef]
- Nieves, J.W. Osteoporosis: The role of micronutrients. Am. J. Clin. Nutr. 2005, 81, 1232s–1239s. [Google Scholar] [CrossRef] [PubMed]
- Martiniakova, M.; Babikova, M.; Mondockova, V.; Blahova, J.; Kovacova, V.; Omelka, R. The Role of Macronutrients, Micronutrients and Flavonoid Polyphenols in the Prevention and Treatment of Osteoporosis. Nutrients 2022, 14, 523. [Google Scholar] [CrossRef] [PubMed]
- Khundmiri, S.J.; Murray, R.D.; Lederer, E. PTH and Vitamin D. Compr. Physiol. 2016, 6, 561–601. [Google Scholar] [CrossRef] [PubMed]
- Baldassano, S.; Gasbjerg, L.S.; Kizilkaya, H.S.; Rosenkilde, M.M.; Holst, J.J.; Hartmann, B. Increased Body Weight and Fat Mass After Subchronic GIP Receptor Antagonist, but Not GLP-2 Receptor Antagonist, Administration in Rats. Front. Endocrinol. 2019, 10, 492. [Google Scholar] [CrossRef]
- Wang, F.S.; Wu, R.W.; Chen, Y.S.; Ko, J.Y.; Jahr, H.; Lian, W.S. Biophysical Modulation of the Mitochondrial Metabolism and Redox in Bone Homeostasis and Osteoporosis: How Biophysics Converts into Bioenergetics. Antioxidants 2021, 10, 1394. [Google Scholar] [CrossRef]
- Dobson, P.F.; Dennis, E.P.; Hipps, D.; Reeve, A.; Laude, A.; Bradshaw, C.; Stamp, C.; Smith, A.; Deehan, D.J.; Turnbull, D.M.; et al. Mitochondrial dysfunction impairs osteogenesis, increases osteoclast activity, and accelerates age related bone loss. Sci. Rep. 2020, 10, 11643. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).