
Impact of Preoperative Immunonutrition on Oxidative Stress and Gut Barrier Function in Surgical Patients with Crohn’s Disease

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient’s Enrollment and Sample Collections
2.2. Markers of Oxidative Stress
2.3. RT-PCR
2.4. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Casanova, M.J.; Chaparro, M.; Molina, B.; Merino, O.; Batanero, R.; Dueñas-Sadornil, C.; Robledo, P.; Garcia-Albert, A.M.; Gómez-Sánchez, M.B.; Calvet, X.; et al. Prevalence of Malnutrition and Nutritional Characteristics of Patients With Inflammatory Bowel Disease. J. Crohn’s Colitis 2017, 11, 1430–1439. [Google Scholar] [CrossRef]
- Agin, M.; Yucel, A.; Gumus, M.; Yuksekkaya, H.A.; Tumgor, G. The Effect of Enteral Nutrition Support Rich in TGF-β in the Treatment of Inflammatory Bowel Disease in Childhood. Medicina 2019, 55, 620. [Google Scholar] [CrossRef] [PubMed]
- Ruemmele, F.M.; Roy, C.C.; Levy, E.; Seidman, E.G. Nutrition as primary therapy in pediatric Crohn’s disease: Fact or fantasy? J. Pediatr. 2000, 136, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Fell, J.M.; Paintin, M.; Arnaud-Battandier, F.; Beattie, R.M.; Hollis, A.; Kitching, P.; Donnet-Hughes, A.; MacDonald, T.T.; Walker-Smith, J.A. Mucosal healing and a fall in mucosal pro-inflammatory cytokine mRNA induced by a specific oral polymeric diet in paediatric Crohn’s disease. Aliment. Pharmacol. Ther. 2000, 14, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Grimble, R.F. Immunonutrition. Curr. Opin. Gastroenterol. 2005, 21, 216–222. [Google Scholar] [CrossRef]
- Weimann, A.; Wobith, M. ESPEN Guidelines on Clinical nutrition in surgery—Special issues to be revisited. Eur. J. Surg. Oncol. 2022, in press. [CrossRef]
- Wagner, I.J.; Rombeau, J.L. Nutritional support of surgical patients with inflammatory bowel disease. Surg. Clin. N. Am. 2011, 91, 787–803. [Google Scholar] [CrossRef]
- Xu, J.; Sun, X.; Xin, Q.; Cheng, Y.; Zhan, Z.; Zhang, J.; Wu, J. Effect of immunonutrition on colorectal cancer patients undergoing surgery: A meta-analysis. Int. J. Color. Dis. 2018, 33, 273–283. [Google Scholar] [CrossRef]
- McClave, S.A.; Martindale, R.G.; Maxwell, J.P. Immunonutrition and Colorectal Surgery. Dis. Colon Rectum 2017, 60, 3–4. [Google Scholar] [CrossRef]
- Zhu, H.; Li, Y.R. Oxidative stress and redox signaling mechanisms of inflammatory bowel disease: Updated experimental and clinical evidence. Exp. Biol. Med. 2012, 237, 474–480. [Google Scholar] [CrossRef]
- Christman, J.W.; Blackwell, T.S.; Juurlink, B.H. Redox regulation of nuclear factor kappa B: Therapeutic potential for attenuating inflammatory responses. Brain Pathol. 2000, 10, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Krzystek-Korpacka, M.; Neubauer, K.; Berdowska, I.; Boehm, D.; Zielinski, B.; Petryszyn, P.; Terlecki, G.; Paradowski, L.; Gamian, A. Enhanced formation of advanced oxidation protein products in IBD. Inflamm. Bowel Dis. 2008, 14, 794–802. [Google Scholar] [CrossRef]
- Luceri, C.; Bigagli, E.; Agostiniani, S.; Giudici, F.; Zambonin, D.; Scaringi, S.; Ficari, F.; Lodovici, M.; Malentacchi, C. Analysis of Oxidative Stress-Related Markers in Crohn’s Disease Patients at Surgery and Correlations with Clinical Findings. Antioxidants 2019, 8, 378. [Google Scholar] [CrossRef]
- Ciccocioppo, R.; Vanoli, A.; Klersy, C.; Imbesi, V.; Boccaccio, V.; Manca, R.; Betti, E.; Cangemi, G.C.; Strada, E.; Besio, R.; et al. Role of the advanced glycation end products receptor in Crohn’s disease inflammation. World J. Gastroenterol. 2013, 19, 8269–8281. [Google Scholar] [CrossRef] [PubMed]
- Xie, F.; Sun, S.; Xu, A.; Zheng, S.; Xue, M.; Wu, P.; Zeng, J.H.; Bai, L. Advanced oxidation protein products induce intestine epithelial cell death through a redox-dependent., c-jun N-terminal kinase and poly (ADP-ribose) polymerase-1-mediated pathway. Cell Death Dis. 2014, 5, e1006. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Qian, J.; Zhang, Q.; Hu, Y.; Sun, D.; Jiang, L. Advanced glycation end products increased placental vascular permeability of human BeWo cells via RAGE/NF-kB signaling pathway. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 250, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. Educational and Clinical Practice Committee, European Society of Parenteral and Enteral Nutrition (ESPEN). ESPEN guidelines for nutrition screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Grass, F.; Pache, B.; Martin, D.; Hahnloser, D.; Demartines, N.; Hübner, M. Preoperative Nutritional Conditioning of Crohn’s Patients-Systematic Review of Current Evidence and Practice. Nutrients. 2017, 9, 562. [Google Scholar] [CrossRef] [PubMed]
- Cerantola, Y.; Grass, F.; Cristaudi, A.; Demartines, N.; Schäfer, M.; Hübner, M. Perioperative nutrition in abdominal surgery: Recommendations and reality. Gastroenterol. Res. Pract. 2011, 2011, 739347. [Google Scholar] [CrossRef] [PubMed]
- Cerantola, Y.; Hübner, M.; Grass, F.; Demartines, N.; Schäfer, M. Immunonutrition in gastrointestinal surgery. Br. J. Surg. 2011, 98, 37–48. [Google Scholar] [CrossRef]
- Moya, P.; Miranda, E.; Soriano-Irigaray, L.; Arroyo, A.; Aguilar, M.D.; Bellón, M.; Muñoz, J.L.; Candela, F.; Calpena, R. Perioperative immunonutrition in normo-nourished patients undergoing laparoscopic colorectal resection. Surg. Endosc. 2016, 30, 4946–4953. [Google Scholar] [CrossRef]
- Kellow, N.J.; Coughlan, M.T. Effect of diet-derived advanced glycation end products on inflammation. Nutr. Rev. 2015, 73, 737–759. [Google Scholar] [CrossRef]
- Bigagli, E.; Luceri, C.; Dicembrini, I.; Tatti, L.; Scavone, F.; Giovannelli, L.; Mannucci, E.; Lodovici, M. Effect of Dipeptidyl-Peptidase 4 Inhibitors on Circulating Oxidative Stress Biomarkers in Patients with Type 2 Diabetes Mellitus. Antioxidants 2020, 9, 233. [Google Scholar] [CrossRef]
- Nowotny, K.; Jung, T.; Höhn, A.; Weber, D.; Grune, T. Advanced glycation end products and oxidative stress in type 2 diabetes mellitus. Biomolecules 2015, 5, 194–222. [Google Scholar] [CrossRef]
- Rojas, A.; Delgado-López, F.; González, I.; Pérez-Castro, R.; Romero, J.; Rojas, I. The receptor for advanced glycation end-products: A complex signaling scenario for a promiscuous receptor. Cell. Signal. 2013, 25, 609–614. [Google Scholar] [CrossRef]
- Ibrahim, Z.A.; Armour, C.L.; Phipps, S.; Sukkar, M.B. RAGE and TLRs: Relatives., friends or neighbours? Mol. Immunol. 2013, 56, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Body-Malapel, M.; Djouina, M.; Waxin, C.; Langlois, A.; Gower-Rousseau, C.; Zerbib, P.; Schmidt, A.M.; Desreumaux, P.; Boulanger, E.; Vignal, C. The RAGE signaling pathway is involved in intestinal inflammation and represents a promising therapeutic target for Inflammatory Bowel Diseases. Mucosal Immunol. 2019, 12, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Snelson, M.; Lucut, E.; Coughlan, M.T. The Role of AGE-RAGE Signalling as a Modulator of Gut Permeability in Diabetes. Int. J. Mol. Sci. 2022, 23, 1766. [Google Scholar] [CrossRef] [PubMed]
- Qu, W.; Yuan, X.; Zhao, J.; Zhang, Y.; Hu, J.; Wang, J.; Li, J. Dietary advanced glycation end products modify gut microbial composition and partially increase colon permeability in rats. Mol. Nutr. Food Res. 2017, 6, 1700118. [Google Scholar] [CrossRef] [PubMed]
- Sido, B.; Seel, C.; Hochlehnert, A.; Breitkreutz, R.; Dröge, W. Low intestinal glutamine level and low glutaminase activity in Crohn’s disease: A rational for glutamine supplementation? Dig. Dis. Sci. 2006, 51, 2170–2179. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Yang, Y.; Sun, S.; Dai, Z.; Ren, F.; Wu, Z. Insights into diet-associated oxidative pathomechanisms in inflammatory bowel disease and protective effects of functional amino acids. Nutr. Rev. 2022, 81, 95–113. [Google Scholar] [CrossRef] [PubMed]
- Crespo, I.; San-Miguel, B.; Prause, C.; Marroni, N.; Cuevas, M.J.; González-Gallego, J.; Tuñón, M.J. Glutamine treatment attenuates endoplasmic reticulum stress and apoptosis in TNBS-induced colitis. PLoS ONE 2012, 7, e50407. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, C.; Wu, G.; Sun, Y.; Wang, B.; He, B.; Dai, Z.; Wu, Z. Glutamine enhances tight junction protein expression and modulates corticotropin-releasing factor signaling in the jejunum of weanling piglets. J. Nutr. 2015, 145, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Wu, Z.; Ji, Y.; Sun, K.; Dai, Z.; Wu, G. L-Glutamine Enhances Tight Junction Integrity by Activating CaMK Kinase 2-AMP-Activated Protein Kinase Signaling in Intestinal Porcine Epithelial Cells. J. Nutr. 2016, 146, 501–508. [Google Scholar] [CrossRef]
- Singh, K.; Gobert, A.P.; Coburn, L.A.; Barry, D.P.; Allaman, M.; Asim, M.; Luis, P.B.; Schneider, C.; Milne, G.L.; Boone, H.H.; et al. Dietary Arginine Regulates Severity of Experimental Colitis and Affects the Colonic Microbiome. Front. Cell. Infect. Microbiol. 2019, 9, 66. [Google Scholar] [CrossRef]
- Rao, J.N.; Liu, L.; Zou, T.; Marasa, B.S.; Boneva, D.; Wang, S.R.; Malone, D.L.; Turner, D.J.; Wang, J.Y. Polyamines are required for phospholipase C-gamma1 expression promoting intestinal epithelial restitution after wounding. Am. J. Physiol. Gastrointest. Liver Physiol. 2007, 292, G335–G343. [Google Scholar] [CrossRef] [PubMed]
- Lecleire, S.; Hassan, A.; Marion-Letellier, R.; Antonietti, M.; Savoye, G.; Bôle-Feysot, C.; Lerebours, E.; Ducrotté, P.; Déchelotte, P.; Coëffier, M. Combined glutamine and arginine decrease proinflammatory cytokine production by biopsies from Crohn’s patients in association with changes in nuclear factor-kappaB and p38 mitogen-activated protein kinase pathways. J. Nutr. 2008, 138, 2481–2486. [Google Scholar] [CrossRef] [PubMed]
- Drover, J.W.; Dhaliwal, R.; Weitzel, L.; Wischmeyer, P.E.; Ochoa, J.B.; Heyland, D.K. Perioperative use of arginine-supplemented diets: A systematic review of the evidence. J. Am. Coll. Surg. 2011, 212, 385–399. [Google Scholar] [CrossRef] [PubMed]
- Lev-Tzion, R.; Griffiths, A.M.; Leder, O.; Turner, D. Omega 3 fatty acids (fish oil) for maintenance of remission in Crohn’s disease. Cochrane Database Syst. Rev. 2014, 2014, CD006320. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Forbes, A.; Escher, J.; Hébuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; et al. ESPEN guideline: Clinical nutrition in inflammatory bowel disease. Clin. Nutr. 2017, 36, 321–347. [Google Scholar] [CrossRef] [Green Version]
- Barbalho, S.M.; Goulart Rde, A.; Quesada, K.; Bechara, M.D.; de Carvalho Ade, C. Inflammatory bowel disease: Can omega-3 fatty acids really help? Ann. Gastroenterol. 2016, 29, 37–43. [Google Scholar]
- Beguin, P.; Errachid, A.; Larondelle, Y.; Schneider, Y.J. Effect of polyunsaturated fatty acids on tight junctions in a model of the human intestinal epithelium under normal and inflammatory conditions. Food Funct. 2013, 4, 923–931. [Google Scholar] [CrossRef]
- Zhao, J.; Shi, P.; Sun, Y.; Sun, J.; Dong, J.N.; Wang, H.G.; Zuo, L.G.; Gong, J.F.; Li, Y.; Gu, L.L.; et al. DHA protects against experimental colitis in IL-10-deficient mice associated with the modulation of intestinal epithelial barrier function. Br. J. Nutr. 2015, 114, 181–188. [Google Scholar] [CrossRef]
- Tanaka, M.; Lee, K.; Martinez-Augustin, O.; He, Y.; Sanderson, I.R.; Walker, W.A. Exogenous nucleotides alter the proliferation, differentiation and apoptosis of human small intestinal epithelium. J. Nutr. 1996, 126, 424–433. [Google Scholar] [CrossRef]
- Hess, J.R.; Greenberg, N.A. The role of nucleotides in the immune and gastrointestinal systems: Potential clinical applications. Nutr. Clin. Pract. 2012, 27, 281–294. [Google Scholar] [CrossRef]
- Heerasing, N.; Thompson, B.; Hendy, P.; Heap, G.A.; Walker, G.; Bethune, R.; Mansfield, S.; Calvert, C.; Kennedy, N.A.; Ahmad, T.; et al. Exclusive enteral nutrition provides an effective bridge to safer interval elective surgery for adults with Crohn’s disease. Aliment. Pharmacol. Ther. 2017, 45, 660–669. [Google Scholar] [CrossRef]
- Beaupel, N.; Brouquet, A.; Abdalla, S.; Carbonnel, F.; Penna, C.; Benoist, S. Preoperative oral polymeric diet enriched with transforming growth factor-beta 2 (Modulen) could decrease postoperative morbidity after surgery for complicated ileocolonic Crohn’s disease. Scand. J. Gastroenterol. 2017, 52, 5–10. [Google Scholar] [CrossRef]
- Waitzberg, D.L.; Saito, H.; Plank, L.D.; Jamieson, G.G.; Jagannath, P.; Hwang, T.L.; Mijares, J.M.; Bihari, D. Postsurgical infections are reduced with specialized nutrition support. World J. Surg. 2006, 30, 1592–1604. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Controls | Immunonutrition | p | |
|---|---|---|---|
| n | 8 | 8 | |
| Age, years | 49.0 ± 5.1 | 50.5 ± 4.3 | 0.8270 |
| Gender M, n (%) | 5 (62.5%) | 4 (50.0%) | >0.999 |
| Smokers/former smoker, n (%) | 5 (62.5%) | 4 (50.0%) | >0.999 |
| BMI, kg/m2 | 23.1 ± 1.43 | 20.92 ± 1.1 | 0.2484 |
| Disease duration, yrs | 18.2 ± 3.2 | 12.3 ± 3.5 | 0.2274 |
| Familial IBD, n (%) | 0 | 2 (25.0%) | 0.4667 |
| Disease location ileal, n (%) | 8 (100%) | 8 (100%) | >0.999 |
| Disease behavior | >0.999 | ||
| Stricturing | 4 | 4 | |
| Fistulizing | 4 | 4 | |
| Nutritional risk, n(%) | >0.999 | ||
| 1–2 | 3 (37.5%) | 4 (50.0%) | |
| 3–4 | 5 (62.5%) | 4 (50.0%) | |
| Surgical recurrence n (%) | 5 (71.4%) | 2 (28.6%) | 0.3147 |
| Δ diagnosis-surgery, years | 7.4 ± 2.6 | 3.1 ± 1.6 | 0.4437 |
| Abdominal fistulae, n (%) | 2 (25.0%) | 5(62.5%) | 0.3147 |
| Preoperative therapy, n (%) | |||
| corticosteroids | 3 (37.5%) | 3 (37.5%) | >0.999 |
| 5-ASA | 3 (37.5%) | 2(25%) | >0.999 |
| CDAI | 250 (250–300) | 300 (250–350) | 0.1189 |
| Type of Surgery | >0.999 | ||
| open | 1 | 1 | |
| laparoscopy | 7 | 7 |
| Controls | Immunonutrition | p | |
|---|---|---|---|
| n | 8 | 8 | |
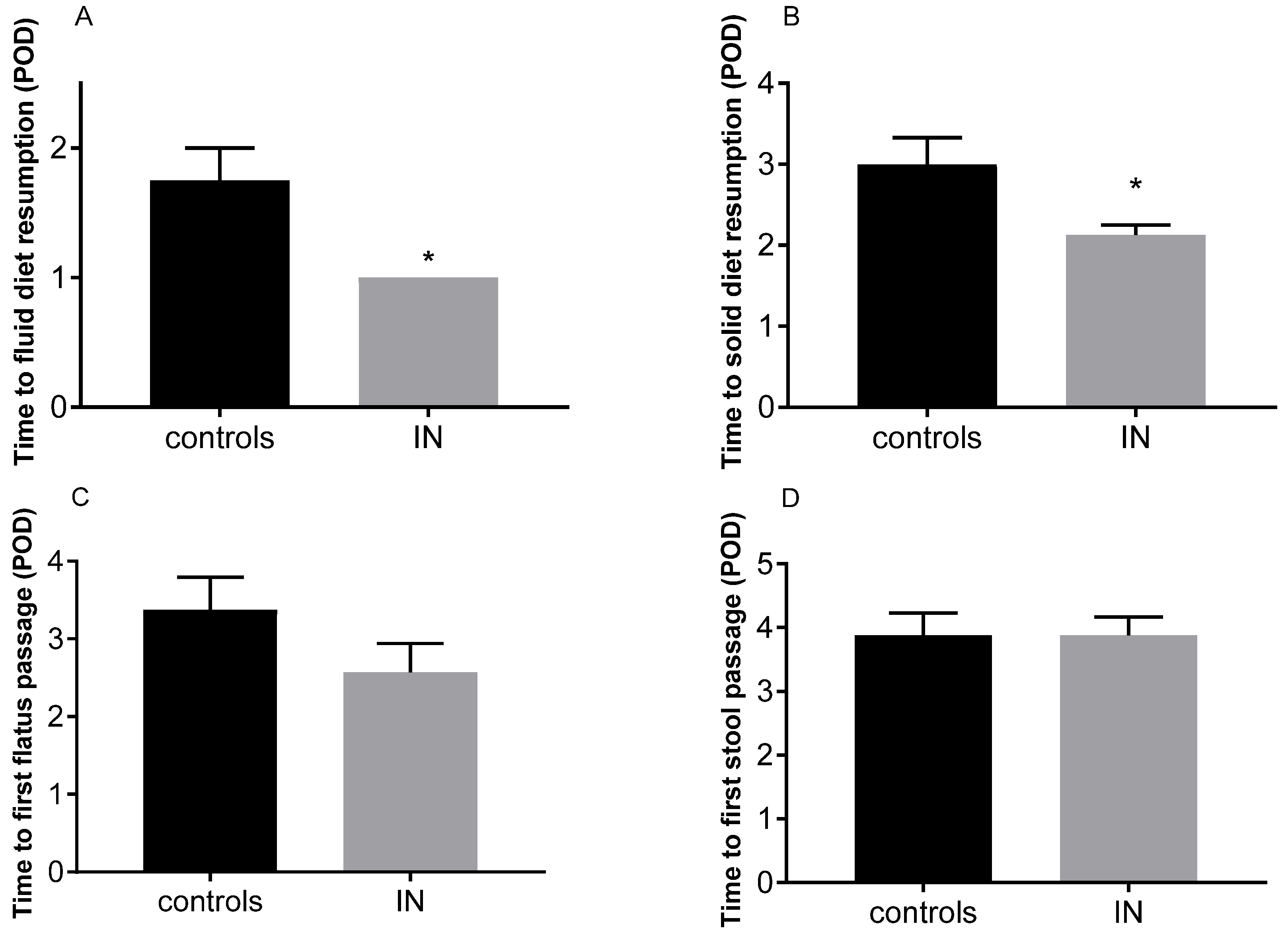
| POD discharge, days | 5 (5–6) | 6 (5.2–6.7) | 0.2071 |
| Days of first flatus passage | 4 (2–4) | 3 (2–3.75) | 0.2890 |
| Days of first stool | 4(3.25–4.75) | 4(3–4.75) | >0.999 |
| Oral fluid nutrition n (%) | 0.0256 | ||
| POD1 | 3 (37.5%) | 8 (100%) | |
| POD2–3 | 5 (62.5%) | 0 | |
| Oral solid nutrition, n (%) | 0.0286 | ||
| POD2 | 2 (25.0%) | 7 (87.5%) | |
| POD3 | 2 (25.0%) | 1 (12.5%) | |
| POD4 | 4 (50.0%) | 0 |
| Oxidative Markers | Controls | Immunonutrition | p |
|---|---|---|---|
| n | 8 | 8 | |
| Plasma samples | |||
| AGEs, UA/mg of proteins | 7.89 ± 1.46 | 7.56 ± 0.91 | 0.8560 |
| AOPPs, µmol/mg of proteins | 1.51 ± 0.38 | 1.55 ± 0.19 | 0.9095 |
| Mucosal samples | |||
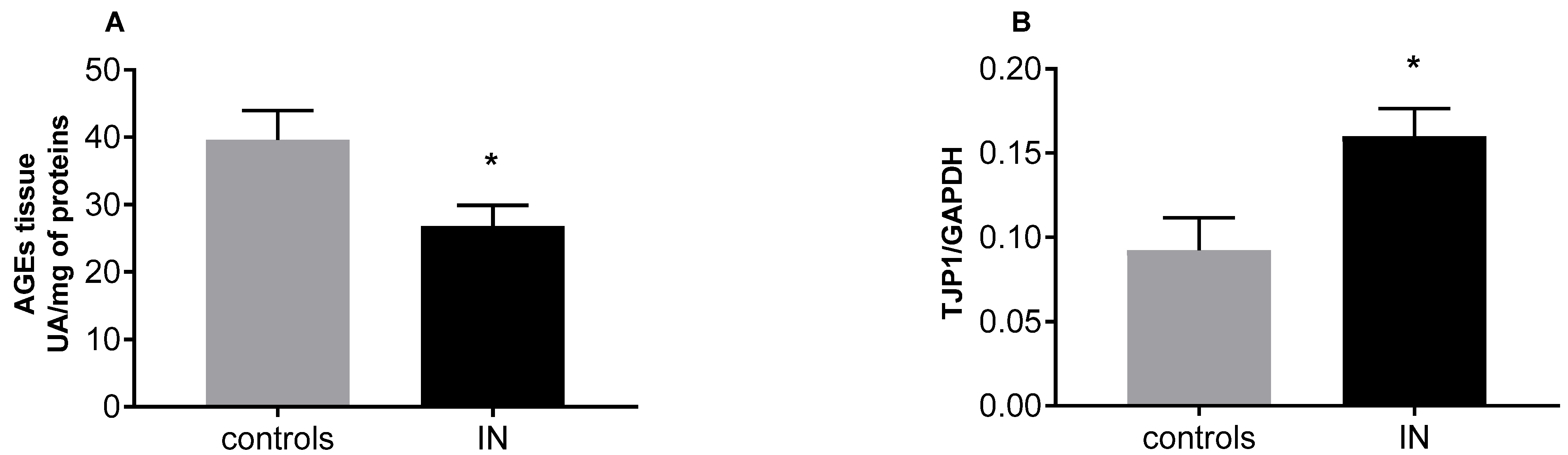
| AGEs, UA/mg of proteins | 39.59 ± 4.41 | 26.83 ± 3.06 | 0.0321 |
| AOPPs, µmol/mg of proteins | 22.74 ± 6.18 | 25.15 ± 5.55 | 0.7753 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bigagli, E.; D’Ambrosio, M.; Cinci, L.; Fiorindi, C.; Agostiniani, S.; Bruscoli, E.; Nannoni, A.; Lodovici, M.; Scaringi, S.; Giudici, F.; et al. Impact of Preoperative Immunonutrition on Oxidative Stress and Gut Barrier Function in Surgical Patients with Crohn’s Disease. Nutrients 2023, 15, 882. https://doi.org/10.3390/nu15040882
Bigagli E, D’Ambrosio M, Cinci L, Fiorindi C, Agostiniani S, Bruscoli E, Nannoni A, Lodovici M, Scaringi S, Giudici F, et al. Impact of Preoperative Immunonutrition on Oxidative Stress and Gut Barrier Function in Surgical Patients with Crohn’s Disease. Nutrients. 2023; 15(4):882. https://doi.org/10.3390/nu15040882
Chicago/Turabian StyleBigagli, Elisabetta, Mario D’Ambrosio, Lorenzo Cinci, Camilla Fiorindi, Sara Agostiniani, Elisa Bruscoli, Anita Nannoni, Maura Lodovici, Stefano Scaringi, Francesco Giudici, and et al. 2023. "Impact of Preoperative Immunonutrition on Oxidative Stress and Gut Barrier Function in Surgical Patients with Crohn’s Disease" Nutrients 15, no. 4: 882. https://doi.org/10.3390/nu15040882