Abstract
Human milk (HM) of mothers infected with or vaccinated against SARS-CoV-2 contains specific immunoglobulins, which may protect their offspring against infection or severe disease. The time frame and duration after infection or vaccination, during which these immunoglobulins are detected in HM, as well as the major factors that influence their levels, have not been fully elucidated. This systematic review aimed to collect the existing literature and describe the immune response, specifically regarding the immunoglobulins in HM after COVID-19 disease or vaccination in non-immune women. We conducted a systematic search of PubMed and Scopus databases to identify studies published up until 19 March 2023. In total, 975 articles were screened, and out of which 75 were identified as being relevant and were finally included in this review. Infection by SARS-CoV-2 virus primarily induces an IgA immune response in HM, while vaccination predominantly elevates IgG levels. These immunoglobulins give HM a neutralizing capacity against SARS-CoV-2, highlighting the importance of breastfeeding during the pandemic. The mode of immune acquisition (infection or vaccination) and immunoglobulin levels in maternal serum are factors that seem to influence immunoglobulin levels in HM. Further studies are required to determine the impact of other factors, such as infection severity, lactation period, parity, maternal age and BMI on immunoglobulin level in HM.
1. Introduction
The global COVID-19 pandemic has resulted in more than 6.85 million deaths worldwide with about 0.1% of incidents occurring in neonates and children under 5 years [1,2]. The widespread availability of vaccines has played a crucial role in controlling transmission rates and reducing morbidity and mortality. The Center for Disease Control and Prevention (CDC) recommends vaccination for individuals aged 6 months and older, including neonates and non-vaccinated infants [3].
Younger or unvaccinated infants are defenseless against SARS-CoV-2 virus. Breastfeeding could be a protective factor against severe infection for these infants. Human milk (HM) contains various bioactive nutrients, such as immunoglobulins that block the penetration of microorganisms into the endothelium [4]. Initial concerns regarding the safety of breastfeeding during maternal infection led to previous recommendations for infected women to avoid breastfeeding. However, since June 23, 2020, the World Health Organization (WHO) strongly recommends breastfeeding, as the benefits outweigh the potential risks [5]. Recent studies indicate that maternal vaccination against SARS-CoV-2 virus reduces the risk of hospitalization in infants by approximately 60% [6].
SARS-CoV-2 virus is a single-stranded RNA virus, and its RNA is enveloped to a nucleocapsid. Its genome encodes four structural proteins: N(Nucleocapsid), M(Membrane), S(Spike) and E(Envelope) proteins [7]. The N protein is found in the virus core, and it forms complexes with viral RNA. It is also found in infected cells, so it is a common target for antigen tests [8,9]. The other three proteins are found in the viral envelope. The S protein interacts with the Angiotensin-converting enzyme 2(ACE2) receptor and mediates SARS-CoV-2 to be inserted into the host’s cells. The S protein consists of two subunits: the S1 subunit which contains an exposed receptor-binding domain (RBD), the part of the S protein that binds to the ACE2 receptor, and the S2 subunit for membrane fusion [10]. Tests that are used to evaluate the immune response after the vaccination target S protein or a subunit of it. Serology tests that are used in cases of COVID-19 disease, can target the N protein as well.
Nicolaidou V. et al., in a recent systematic review, reported that the HM of vaccinated lactating women contains neutralizing immunoglobulins against SARS-CoV-2 [11]. The presence of specific antibodies against the virus in the HM of vaccinated women has also been confirmed by another recent meta-analysis by Whited and Cervantes [12]. COVID-19 disease leads to an immune response in maternal organisms as well, and neutralizing antibodies are detected in their HM [13]. However, the duration that these antibodies remain in detectable levels, the time frame in which the immune response begins to wane, the factors that influence their levels in HM and the differences in the immune response between infected women and those who are vaccinated still remain unclear. We conducted a systematic review of the current literature from the beginning of the pandemic until March 19, 2023, in order to synthesize the current knowledge regarding the presence of antibodies against SARS-CoV-2 in HM after COVID-19 disease or vaccination, among non-previously immune pregnant or lactating women.
2. Materials and Methods
In order to perform this systematic review, we followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines’ (PRISMA) recommendation (presented as Supplementary Material) [14]. The systematic review was not registered in Prospero. We searched the Pubmed and Scopus databases from 1 December 2019 to 19 March 2023. We searched the existing literature only written in the English language.
The keywords used for the literature search were as follows: “SARS-CoV-2”, “Covid 19”, “novel coronavirus”, “Immunoglobulin*”, “antibody”, “IgG”, “IgA”, “secretory IgA”, “sIgA”, “immunological”, “immune system”, “immunogenicity”, “immunology”, “milk transferred antibody”, “breast milk”, “maternal milk”, “human milk”, “breastmilk”, “colostrum”, “breastfeeding”, “donor milk”, “lactating women” and “lactation”, combined with Boolean logical operators (AND, OR).
Additionally, we searched all of the references of the relevant studies and of previous corresponding systematic reviews in order to confirm the study saturation.
2.1. Study Eligibility Criteria
All selected studies examined the immunological response in the HM of pregnant or lactating women after COVID-19 disease or vaccination. After the duplicates were deleted, two investigators (M.D. and R.S.) independently checked the titles and abstracts of the retrieved papers, and consequently studied the full texts to decide which of them were eligible for the review. Any disagreements between the two researchers were analyzed and resolved by a third researcher (Z.I.).
Studies included in the present review met the following eligibility criteria: (1) women vaccinated against or infected by SARS-CoV-2 virus during pregnancy or lactating period were the study population, (2) there was no history of previously confirmed COVID-19 disease or vaccination, (3) current COVID-19 disease was confirmed via a PCR positive test, serology test or other laboratory method and (4) data on HM-specific immunoglobulins against SARS-CoV-2 were described in the studies that were included in the review as well. Irrelevant or non-original studies, case reports or studies with indecisive data were excluded from this review, as well as studies in any language other than English.
2.2. Data Extraction
The 2 researchers (M.D. and R.S.) separately studied the eligible studies and extracted useful data in an electronical database (Microsoft Excel). Complete information included the name of the first author, date of publication, country of origin, duration and population of the study, diagnosis method or vaccine type, time of HM collection, studied immunoglobulins and main outcomes or results of the study. Any disagreement between the two researchers was analyzed and resolved by a third researcher (Z.I.). Finally, the selected studies were examined again by another investigator (N.I) to check for eligibility and for duplication, and the extracted data were checked for their accuracy.
3. Results
A total of 975 articles were initially retrieved. After excluding duplicates and articles with titles and abstracts not related to our review object, 122 studies were selected for their full text to be studied. In these studies, the full text was comprehensively studied and 75 studies finally met the eligibility criteria. The searching and selection processes are depicted in a PRISMA graph (Figure 1).
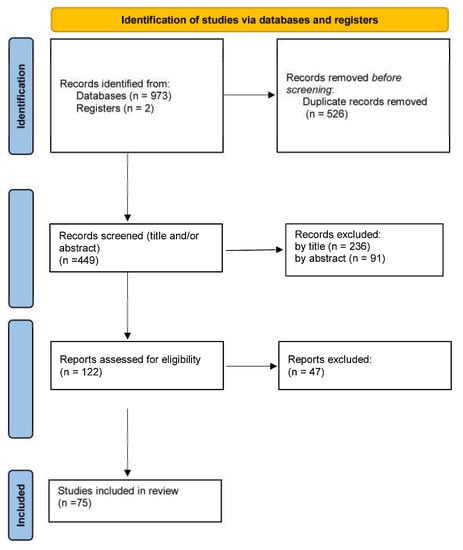
Figure 1.
Flow chart of the study selection process.
Seventeen studies out of the total included women infected for the first time during pregnancy (Table 1) [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26]. Another 17 studies examined women infected for the first time during lactation (Table 2) [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43]. Six more studies included vaccinated pregnant women not previously immunized (Table 3) [22,25,27,29,44,45]. Finally, 40 studies examined vaccinated lactating women not previously immunized (Table 4) [22,25,32,38,42,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80]. Ten studies included more than one participant group, and therefore they have been put into more than one table [22,25,27,29,32,38,42,44,46,47].

Table 1.
Characteristics of included studies referring to first-time-infected pregnant women.
Table 2.
Characteristics of included studies referring to first-time-infected lactating women.
Table 3.
Characteristics of included studies referring to vaccinated pregnant women not previously infected or vaccinated.
Table 4.
Characteristics of included studies referring to vaccinated lactating women not previously infected or vaccinated.
In total, 874 infected pregnant women, 537 infected lactating women, 196 vaccinated pregnant women and 1450 vaccinated lactating women were included in this systematic review. In the case of pregnant women, all samples were collected postpartum and most of them were collected within the 1st week postpartum. In some cases, samples were collected later, even 6 months after delivery in one study [27]. HM samples from lactating women were collected in variable time-points, with the longest being 6–10 months post infection or vaccination [43,51,54,56,62]. All studies detected specific immunoglobulins against SARS-CoV-2. Infection mainly induces the production of specific IgA antibodies [17,30,31,32,33,34,35,36,37,38,39,40,41,42,43,46,47,83,84,85,86], while vaccination mostly elicits the IgG response [22,25,27,29,32,38,42,44,46,47]. From the included studies, it seems that maternal age and BMI do not influence antibody titers. Yet, the general immune response of the mother and consequently the titers of some immunoglobulins in HM and maternal serum seem to correlate with the levels of other immunoglobulins in HM [16,21].
SARS-CoV-2 virus was not detected in HM samples in any study [18,20,24,30,36,38,40], and no study reported severe side effects after vaccination [42,53,63,65,66,72].
4. Discussion
Breastfeeding is the best dietary choice for infants [4]. HM contains specific immunoglobulins that are produced in response to exposure of the mother to pathogens. These immunoglobulins maintain their structural integrity in the infant’s stomach, bind to intestinal mucus and prevent pathogens from entering the bloodstream [89,90,91]. The presence of specific immunoglobulins against SARS-CoV-2 in the HM of infected or vaccinated mothers could potentially shield neonates and infants from future infections or even from severe disease.
4.1. Post Infection Immune Response
This systematic review affirms that specific immunoglobulins against SARS-CoV-2 virus were detected in the HΜ of women who were infected during pregnancy or lactation. These immunoglobulins were mainly IgA, and specifically secretory IgA antibodies, and less IgM and IgG were found [17,20,25,28,32,35,36,43,82], which is compatible with the known proportion of antibody isotypes in human milk [92]. They also primarily (80%) targeted the RBD domain of the S1 subunit [17].
4.1.1. Anti-SARS-CoV-2 IgA Immunoglobulins
IgA titers in HM increase one week after infection, and these titers are even higher 2 weeks post COVID-19 disease [40]. Many studies indicate that they remain high in HM and detectable even 2–3 months after infection [27,31,34,35,38,39,40,42,43,83,85,86]. Pace RM et al. reported that IgA remained positive in 77% of 64 lactating women 2 months after infection [40]. Junker HG et al. found that HM conversion was observed after a median of 15 days and IgA levels peaked after 35 days. After 70 days, however, IgA was detectable only in 33% of HM samples [42]. Conti MG et al. reported that IgA was detectable in all HM samples of 28 lactating women even 2 months after delivery [23]. These women had been infected during pregnancy, which indicates that IgA may persist for a longer period of time. Indeed, other studies confirm their persistence in HM even 5–10 months post COVID-19 disease [34,39,43]. Fox A. et al. reported that all of the 28 tested women in their study had detectable IgA in HM 4–10 months after infection and 43% of them had even higher titers than what they had at 1 month after the infection [43]. The presence of specific IgA against SARS-CoV-2 in HM is optimal for infants. According to a recent cross-sectional study in Brazil, the titers of IgA in the HM of women infected during pregnancy were negatively correlated with the presence of clinical symptoms in their neonates [83].
Various factors influence anti-SARS-CoV-2 IgA levels in HM. The concentration of specific IgA immunoglobulins in HM is positively correlated with the levels of total IgA, IgM and IgG titers in HM [21]. Additionally, levels of specific IgG in maternal serum are also significantly correlated with IgA levels in HM [16]. However, this is not the case for IgA titers in serum. There is no reported association between IgA titers in HM and maternal serum [25,35,47]. This is logical as IgA in HM after natural infection is not of serum origin, but of muscular origin [93].
As for the time from infection, the data are conflicting. Some report a negative correlation with antibody titers [21,23], while others report a positive correlation [37]. Infection induces a humoral response and antibody titers begin to rise. After an unknown period of time, they reach a peak, and then they begin to wane over time [94]. Therefore, contradicting results in the studies may be due to different time-points of sample collection.
Additionally, not all types of antibodies have the same response over time. Bobik T.V. et al. tested sIgA against specific epitopes of SARS-CoV-2 virus (N protein, linear NTD, RBD-SD1 and RBD) and reported that the levels of sIgA against N-protein and against linear NTD and RBD-SD1 were higher in women that were infected during the third trimester compared to women infected during the first and second trimesters. Regarding sIgA against RBD, they found that their levels were similar, independent of the trimester of pregnancy when infection occurred [19]. No correlation between time of infection during pregnancy and anti-RBD antibodies was reported by Szczygioł, P. et al. either [28]. This indicates that this kind of antibody is more stable over time. Interestingly, Wachman EM et al. reported that anti-RBD IgA titers were not stable but significantly higher in women infected during the first or second trimester of pregnancy [84].
The severity of COVID-19 disease is another factor, but its impact on antibody titers has not yet been clarified. Pace, R.M et al. reported higher concentrations of antibodies in the HM of women with symptomatic COVID-19 disease than in the HM of asymptomatic women; yet, the difference was not significantly important [40]. In other relevant studies, no association between the two parameters has been found [28,83]. Probably, the severity of the disease has a positive impact on antibody levels. Many other studies on the general population have reported that antibody titers are higher in people with severe/moderate COVID-19 disease [94]. More studies are required to reach safe conclusions. From the existing data in the literature, no correlation has been found between IgA levels in HM and maternal age or infant gender [35,37].
4.1.2. Anti-SARS-CoV-2 IgM Immunoglobulins
IgM immunoglobulins are the second most abundant antibodies in HM, and yet their titers are significantly lower than IgA titers. In a prospective study, Decenti EC detected anti-SARS-CoV-2 antibodies in only 7.5% of milk samples [26]. Specific IgM against 2 SARS-CoV-2 was mainly detected in samples collected 10–40 days after infection, and after that, their levels declined [20,21]. In a relevant study by Luo QQ et al., a positive correlation between IgM levels in HM and maternal serum was found [24]. The presence of IgM antibodies against infectious diseases in HM can provide passive immunity to infants, while simultaneously hindering the entry and transportation of viruses, such as HIV, to the infant [95,96]. Given these findings, it is plausible that breastfeeding by SARS-CoV-2-infected mothers offers postpartum protection to the infant through antibodies, reducing the risk of viral transmission.
4.1.3. Anti-SARS-CoV-2 IgG Immunoglobulins
HM contains low titers of IgG immunoglobulins, and in some studies they were not even detectable [20,24]. Decenti, E. C. et al. studied HM samples from 141 women, and they detected IgG only in 3% of the study population [26]. Bauerl et al. reported low IgG titers in HM, with an increase in these titers from Day 40 to Day 205 after COVID-19 disease [21]. Pullen KM et al. detected IgG in a low concentration, but they did not observe any significant change in the titers over time (the mean time of sample collection was 66 days post infection). They also claimed that IgG was functionally attenuated compared to IgA and IgM [35]. In another 2 studies, low titers of IgG 0–3 months after delivery were reported [23,81]. Contrarily to the previous studies, Fox. A. et al. reported that they detected anti-S IgG antibodies in 75% of participants, with 13% of them being present in high titers [43]. The factors that influence their titers in HM are not all clear, but there is a positive correlation between IgG titers in HM and serum [29,35,47].
4.2. Post Vaccination Immune Response
The vaccination of pregnant or lactating women against SARS-CoV-2 also induces the secretion of specific anti-spike antibodies in HM. However, there are some differences in this immune response compared to the one after natural infection. First of all, vaccination mainly induces an IgG response and less of an IgA response [22,25,32,38,42,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79]. After mRNA vaccination, a 10-fold and 100-fold increase in IgA and IgG titers was observed, respectively [47]. Vaccination induces no significant increase in secretory antibodies’ titers. IgA seems to be almost exclusively of systemic and not mucosal origin [55]. Pietrasanta et al. measured two subtypes of specific anti-S IgA antibodies, IgA1, which has systemic origin, and IgA2, which is mainly detected in mucosal secretions, and they observed that the antibodies were mainly IgA1 [53]. These differences in immune response are probably due to the intramuscular route of vaccine administration [50,67].
4.2.1. Anti-SARS-CoV-2 IgG Immunoglobulins
IgG titers were detected in 87–100% of women post vaccination [50,62,65,66,72,77]. Only in one study was a moderate IgG immune response (43% of women) observed [73]. IgG titers in HM increase after each dose [38,47,50,52,55,63,67,71,74,75]. The peak of anti-S1-IgG titers occurs about 1–2 weeks after the 2nd dose and after that they wane [48,51,52,53,56,62,65,66,71]. A recent longitudinal study reported that IgG antibodies’ half lives in HM are about 2 months [45]. In other relevant studies, no significant difference in IgG titers was observed between 30 and 60 days post vaccination [57,80]. Even IgG levels wane over time, but remain in detectable levels 2 [57], 3 [38,53,72] and 6 months post vaccination [49,73]. Contrarily with total IgG levels, secretory IgG antibodies continuously increase even 6 months after the first dose of mRNA vaccines [54]. The main IgG subclasses in HM after 2 doses of mRNA-based vaccines are IgG1 and IgG3, which are the main subclasses of IgG that emerge after viral infections [45,97]. Interestingly, Agostinis C. et al., in a recent study, demonstrated that the presence of anti-S IgG in the HM of vaccinated lactating women is capable of activating in vitro the complement [80]. All of these data indicate that vaccinated mothers are capable of providing protective antibodies to their offspring for a long time after their primary vaccination.
As for the factors influencing antibody levels in HM, numerous studies have confirmed a significant positive correlation between IgG titers in HM and maternal serum [25,29,45,47,48,51,56,62,63,64,69,75,77,79,80]. A positive correlation between the lactation period and the total antibody titers was also reported in a study by Trofin F. et al. (lactating period between 3 and 36 months) [57]. However, this was not confirmed in other studies during the lactation period between 1.5 and 23 months [50,73]. A negative correlation was reported with parity [57], while no correlation was confirmed between IgG levels and maternal age or BMI [57,69,74].
4.2.2. Anti-SARS-CoV-2 IgA Immunoglobulins
IgA immunoglobulins in detectable levels are present in 75–95% of vaccinated women at 2 weeks after the 2nd dose [42,63,65,66,74]. In a prospective study, though, detectable levels were present in just 36% of women post vaccination [73]. Yet, it is not clear if IgA rises mainly after the 1st dose, without any additional increase after the 2nd dose [38,47,63,67,73,74], or whether their titers present a biphasic model after vaccination [42,52,55,65,66,70,71]. Many studies indicate waning IgA titers about one month after the 1st vaccine dose [44,49,51,56]. Contrarily, Juncker HG et al. reported that IgA titers peaked 2 weeks after the 1st dose, and then they waned until the 2nd dose, when they finally reached a second peak 5 days after vaccination [70]. Ricciardi et al. studied secretory IgA and they observed peak titers at 3 weeks after the 2nd dose, while their concentration significantly decreased at 6 months post vaccination [54]. Perez SE et al. detected IgA antibodies in about 50% and 25% of samples at 1 and 3 months post vaccination, respectively [62]. Finally, Narayanaswamy et al. observed no difference in anti-RBD IgA median titers before and after vaccination [50].
A positive correlation was found between IgA titers in HM and IgG titers in maternal serum [51,62,69,74]. A positive correlation may also exist between the IgA titers in HM and the IgA titers in maternal serum [25,47,64]; however, this finding is not supported by all studies [74]. The lactation period is also another factor which has an impact on IgA titers, and is not clearly defined by the included studies. A positive impact (lactation period between 3 and 36 months) [57] was reported in one study, while in others, either a negative (lactation period <18 months) [63] or no impact (lactation period 1.5–23 months for infants) [50] was reported. A negative correlation was found between antibody concentration and parity [57], and there was no correlation with maternal age [57,74].
4.2.3. Anti-SARS-CoV-2 IgM immunoglobulins
Vaccination does not significantly influence IgM levels in HM. In the majority of studies, they are not even detectable [50,51,64,69,73,79], and in others they are just poorly detected [62,74].
4.3. Differences in Immune Response after Infection or Vaccination
Higher IgG titers were observed in the HM of vaccinated women compared to those who were previously infected with SARS-CoV-2 [22,25,32]. In the case of IgA, the data are ambiguous, with some studies reporting higher antibody titers after vaccination [27], some reporting lower [52] and some reporting no significant difference after vaccination or infection [42]. As has already been mentioned, infection mainly induces IgA and, to a lesser extent, the IgM immune response, while vaccination primarily stimulates the production of IgG antibodies. IgA and IgG are found mainly in secretory form and they are released by mammary tissue to HM. After a natural infection with SARS-CoV-2, B-cells stimulated in the lymphoid tissues of the respiratory tract migrate to the mammary gland and release secretory antibodies into HM [93]. Contrarily, post vaccination antiSARS-CoV-2 antibodies in HM are derived from maternal serum [11]. Secretory IgA antibodies are attached to the gastrointestinal tract of breastfeeding infants, where they bind with local microorganisms and block their penetration [4]. On the other hand, IgG antibodies produced post vaccination have been found to be capable of activating the complement. Therefore, infants can benefit from both types of antibodies in different ways [80].
As for the type of immunoglobulins, vaccination induces anti-spike protein antibodies. Infection, on the other hand, mainly induces the anti-N protein. A relative study by Bobik T.V. et al. reported significantly lower levels of the anti-RBD antibody compared to anti-N antibodies in the HM of lactating women infected during the third trimester [19]. L.Bode et al., in a recent study, reported that IgA antibodies in the HM of infected women are mainly directed against the N protein (about 43%) and less against the S protein (about 24%), and there was heterogeneity in the type and quantity of antibodies.
4.4. Differences in Immune Response According to Vaccine Type
No difference between detected antibody titers was described in women vaccinated with Moderna or Pfizer/BioNtech vaccines [32,52,57,63,68,88]. Only in one study of Gray KJ et al. were higher IgA titers detected in the Moderna group after the 2nd dose [67]. However, compared to the adenovirus-vectored vaccines, mRNA vaccines induce higher titers of antibodies [52,58,61]. Yang X. et al. reported that IgG and IgA levels were detectable in 86–100% and 52–71%, respectively, in mRNA-vaccinated women, and in 33–38% and 17–23%, respectively, in the adenovirus-vector-vaccinated women [58]. The Moderna vaccine also induces significantly higher titers of secretory antibodies compared with the rest of the vaccines [58]. Yet, six months post vaccination, no significant difference in antibody titers was observed among three types of vaccines [88].
4.5. Neutralizing Capacity
Although specific antibodies against SARS-CoV-2 are present in HM after COVID-19 disease or vaccination, it is essential to clarify whether these antibodies have neutralizing capacity. A neutralizing antibody binds with the viral surface and blocks its replication cycle, and so it protects the subject from subsequent infection [98]. Both infection [18,27,30,32,36,43,44,82] and vaccination [22,27,32,44,50,51,53,56,62,71,76,77] induce the production of neutralizing antibodies in HM, more intense, though, post infection [38,44].
In a study of 38 infected lactating women, no correlation between specific anti-SARS-CoV-2 antibody levels and the neutralization capacity of the HM was observed [31]. However, this is not in line with what other studies support. The neutralizing capacity against SARS-CoV-2 seems to be greater in the HM of infected women compared to the pre-pandemic controls, and it also seems to be positively correlated with antibody titers [18,27,30,32,36,43,44,82]. In a relevant study, 62% of the samples had neutralizing antibodies in vitro. Contrarily, the samples collected from the pre-pandemic controls had no neutralizing capacity [36]. Pace RM et al. reported that the HM neutralizing capacity post infection is significantly correlated with anti-RBD antibody levels [30].
Antibody titers also seem to influence the neutralizing capacity of the HM of vaccinated women [44,62]. As for variants, vaccination seems to be more beneficial against the Wuhan-Hu-1 strain and less against the Beta, Gamma and Delta variants. The binding capacity of antibodies is reduced by 30% to these strains [49]. In another study, less of a neutralizing capacity was reported against the Beta variant compared to D614G, Alpha and Gamma [50].
Our systematic review has some limitations. SARS-CoV-2 is a new virus. In the early stages of the pandemic, many studies were conducted with small sample sizes and lacked inclusion criteria. Furthermore, most of the tests used were homemade ELISA assays, which lacked standardization in terms of measurement units. Due to the great heterogeneity of the studies included, not only regarding the type of laboratory test, but also the differences in the timing of sampling between studies and study subjects (pregnant or lactating women), a meta-analysis was not deemed appropriate and instead we focused on presenting a systematic review of the available literature.
5. Conclusions
Infection with SARS-CoV-2 and vaccination against the virus elicit a maternal immune response in breastfeeding mothers with a short period of 1–2 weeks. Consequently, these mothers can transmit specific immunoglobulins with neutralizing capacity to their infants via HM. Therefore, it is recommended that breastfeeding is encouraged in mothers infected or vaccinated, as their HM can provide infants with specific antibodies even months after infection or vaccination.
Infection primarily induces an IgA-mediated immune response, while vaccination mainly elevates IgG immunoglobulins. Our data suggest that both IgA and IgG immunoglobulins contribute to the neutralizing capacity of HM, indicating clinical benefits for infants who receive HM from vaccinated or infected women. However, further studies are required to determine whether factors such as infection severity, lactation period, parity, maternal age and BMI have an impact on the levels of immunoglobulins in HM.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu15081905/s1, Supplement: PRISMA 2020 check list.
Author Contributions
Conceptualization, M.D., R.S., Z.I. and N.I.; methodology, R.S. and M.D.; data curation, M.D., A.P., R.S., T.B., G.K., N.I. and Z.I.; investigation, R.S. and N.I.; writing—original draft preparation, M.D., R.S. and N.I.; writing—review and editing, M.D., T.B., R.S., N.I. and Z.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 7 February 2023).
- Newborn Mortality. Available online: https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-child-mortality-report-2021 (accessed on 7 February 2023).
- COVID-19 Vaccination for Children|CDC. Available online: https://www.cdc.gov/vaccines/covid-19/planning/children.html (accessed on 7 February 2023).
- Dimitroglou, M.; Iliodromiti, Z.; Christou, E.; Volaki, P.; Petropoulou, C.; Sokou, R.; Boutsikou, T.; Iacovidou, N. Human Breast Milk: The Key Role in the Maturation of Immune, Gastrointestinal and Central Nervous Systems: A Narrative Review. Diagnostics 2022, 12, 2208. [Google Scholar] [CrossRef] [PubMed]
- Clinical Management of COVID-19: Interim Guidance, 27 May 2020. Available online: https://apps.who.int/iris/handle/10665/332196 (accessed on 14 November 2022).
- Halasa, N.B.; Olson, S.M.; Staat, M.A.; Newhams, M.M.; Price, A.M.; Boom, J.A.; Sahni, L.C.; Cameron, M.A.; Pannaraj, P.S.; Bline, K.E.; et al. Effectiveness of Maternal Vaccination with MRNA COVID-19 Vaccine during Pregnancy against COVID-19-Associated Hospitalization in Infants Aged. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Yang, C.; Xu, X.-F.; Xu, W.; Liu, S.-W. Structural and Functional Properties of SARS-CoV-2 Spike Protein: Potential Antivirus Drug Development for COVID-19. Acta Pharmacol. Sin. 2020, 41, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Lu, S.; Corbett, K.D. Structural Basis for SARS-CoV-2 Nucleocapsid Protein Recognition by Single-Domain Antibodies. Front. Immunol. 2021, 12, 719037. [Google Scholar] [CrossRef]
- Batra, M.; Tian, R.; Zhang, C.; Clarence, E.; Sacher, C.S.; Miranda, J.N.; De La Fuente, J.R.O.; Mathew, M.; Green, D.; Patel, S.; et al. Role of IgG against N-Protein of SARS-COV2 in COVID-19 Clinical Outcomes. Sci. Rep. 2021, 11, 3455. [Google Scholar] [CrossRef]
- Cafaro, A.; Sangster, M.; Yuan, M.; Shah, P.; Canziani, G.A.; Carter, E.P.; Chaiken, I. The Case for S2: The Potential Benefits of the S2 Subunit of the SARS-CoV-2 Spike Protein as an Immunogen in Fighting the COVID-19 Pandemic. Front. Immunol. 2021, 1, 637651. [Google Scholar] [CrossRef]
- Nicolaidou, V.; Georgiou, R.; Christofidou, M.; Felekkis, K.; Pieri, M.; Papaneophytou, C. Detection of SARS-CoV-2-Specific Antibodies in Human Breast Milk and Their Neutralizing Capacity after COVID-19 Vaccination: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 2957. [Google Scholar] [CrossRef]
- Whited, N.; Cervantes, J. Antibodies against SARS-CoV-2 in Human Breast Milk after Vaccination: A Systematic Review and Meta-Analysis. Breastfeed. Med. 2022, 17, 475–483. [Google Scholar] [CrossRef]
- Low, J.M.; Low, Y.W.; Zhong, Y.; Lee, C.Y.C.; Chan, M.; Ng, N.B.H.; Amin, Z.; Ng, Y.P.M. Titres and Neutralising Capacity of SARS-CoV-2-Specific Antibodies in Human Milk: A Systematic Review. Arch. Dis. Child. Fetal Neonatal Ed. 2022, 107, F1–F7. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Narayanaswamy, V.; Pentecost, B.; Alfandari, D.; Chin, E.; Minor, K.; Kastrinakis, A.; Lieberman, T.; Arcaro, K.F.; Leftwich, H. Humoral and Cell-Mediated Immune Response in Colostrum from Women Diagnosed Positive for SARS-CoV-2. Breastfeed. Med. 2021, 16, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Larcade, R.; DeShea, L.; Lang, G.A.; Caballero, M.T.; Ferretti, A.; Beasley, W.H.; Tipple, T.E.; Vain, N.; Prudent, L.; Lang, M.L.; et al. Maternal-Fetal Immunologic Response to SARS-CoV-2 Infection in a Symptomatic Vulnerable Population: A Prospective Cohort. J. Infect. Dis. 2021, 225, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Fox, A.; Marino, J.; Amanat, F.; Krammer, F.; Hahn-Holbrook, J.; Zolla-Pazner, S.; Powell, R.L. Robust and Specific Secretory IgA against SARS-CoV-2 Detected in Human Milk. iScience 2020, 23, 101735. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Wang, S.; Zeng, W.; Chen, S.; Wu, J.; Lin, X.; Liu, Y.; Sun, Z.; Feng, L. Clinical and Immunologic Features among COVID-19-Affected Mother-Infant Pairs: Antibodies to SARS-CoV-2 Detected in Breast Milk. New Microbes New Infect. 2020, 37, 100752. [Google Scholar] [CrossRef] [PubMed]
- Bobik, T.V.; Kostin, N.N.; Skryabin, G.A.; Tsabai, P.N.; Simonova, M.A.; Knorre, V.D.; Mokrushina, Y.A.; Smirnov, I.V.; Kosolapova, J.A.; Vtorushina, V.V.; et al. Epitope-Specific Response of Human Milk Immunoglobulins in COVID-19 Recovered Women. Pathogens 2021, 10, 705. [Google Scholar] [CrossRef]
- Peng, S.; Zhu, H.; Yang, L.; Cao, L.; Huang, X.; Dynes, M.; Narayan, A.; Xia, J.; Chen, Y.; Zhang, P.; et al. A Study of Breastfeeding Practices, SARS-CoV-2 and Its Antibodies in the Breast Milk of Mothers Confirmed with COVID-19. Lancet Reg. Health -West. Pacific 2020, 4, 100045. [Google Scholar] [CrossRef]
- Bäuerl, C.; Randazzo, W.; Sánchez, G.; Selma-Royo, M.; García Verdevio, E.; Martínez, L.; Parra-Llorca, A.; Lerin, C.; Fumadó, V.; Crovetto, F.; et al. SARS-CoV-2 RNA and Antibody Detection in Breast Milk from a Prospective Multicentre Study in Spain. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 107, 216–221. [Google Scholar] [CrossRef]
- Collier, A.R.Y.; McMahan, K.; Yu, J.; Tostanoski, L.H.; Aguayo, R.; Ansel, J.; Chandrashekar, A.; Patel, S.; Apraku Bondzie, E.; Sellers, D.; et al. Immunogenicity of COVID-19 MRNA Vaccines in Pregnant and Lactating Women. JAMA 2021, 325, 2370–2380. [Google Scholar] [CrossRef]
- Conti, M.G.; Terreri, S.; Piano Mortari, E.; Albano, C.; Natale, F.; Boscarino, G.; Zacco, G.; Palomba, P.; Cascioli, S.; Corrente, F.; et al. Immune Response of Neonates Born to Mothers Infected with SARS-CoV-2. JAMA Netw. Open 2021, 4, e2132563. [Google Scholar] [CrossRef]
- Luo, Q.Q.; Xia, L.; Yao, D.J.; Wu, M.; Wang, H.B.; Luo, M.H.; Jiang, X.; Chen, H. Breastfeeding in Mothers with COVID-19: Insights from Laboratory Tests and Follow-up from Early Outbreak of the Pandemic in China. J. Women’s Health 2021, 30, 1546–1555. [Google Scholar] [CrossRef]
- Conti, M.G.; Terreri, S.; Terrin, G.; Natale, F.; Pietrasanta, C.; Salvatori, G.; Brunelli, R.; Midulla, F.; Papaevangelou, V.; Carsetti, R.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 Infection versus Vaccination in Pregnancy: Implications for Maternal and Infant Immunity. Clin. Infect. Dis. 2022, 75, S37–S45. [Google Scholar] [CrossRef] [PubMed]
- Decenti, E.C.; Salvatore, M.A.; Mancon, A.; Portella, G.; Rocca, A.; Vocale, C.; Donati, S. A Large Series of Molecular and Serological Specimens to Evaluate Mother-to-Child SARS-CoV-2 Transmission: A Prospective Study from the Italian Obstetric Surveillance System. Int. J. Infect. Dis. 2022, 126, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Olearo, F.; Radmanesh, L.S.; Felber, N.; von Possel, R.; Emmerich, P.; Pekarek, N.; Pfefferle, S.; Nörz, D.; Hansen, G.; Diemert, A.; et al. Anti-SARS-CoV-2 Antibodies in Breast Milk during Lactation after Infection or Vaccination: A Cohort Study. J. Reprod. Immunol. 2022, 153, 103685. [Google Scholar] [CrossRef]
- Szczygioł, P.; Łukianowski, B.; Kościelska-Kasprzak, K.; Jakuszko, K.; Bartoszek, D.; Krajewska, M.; Królak-Olejnik, B. Antibodies in the Breastmilk of COVID-19 Recovered Women. BMC Pregnancy Childbirth 2022, 22, 635. [Google Scholar] [CrossRef] [PubMed]
- Nir, O.; Schwartz, A.; Toussia-Cohen, S.; Leibovitch, L.; Strauss, T.; Asraf, K.; Doolman, R.; Sharabi, S.; Cohen, C.; Lustig, Y.; et al. Maternal-Neonatal Transfer of SARS-CoV-2 Immunoglobulin G Antibodies among Parturient Women Treated with BNT162b2 Messenger RNA Vaccine during Pregnancy. Am. J. Obstet. Gynecol. MFM 2022, 4, 100492. [Google Scholar] [CrossRef]
- Pace, R.M.; Williams, J.E.; Järvinen, K.M.; Belfort, M.B.; Pace, C.D.; Lackey, K.A.; Gogel, A.C.; Nguyen-Contant, P.; Kanagaiah, P.; Fitzgerald, T.; et al. COVID-19 and Human Milk: SARS-CoV-2, Antibodies, and Neutralizing Capacity. medRxiv Prepr. Serv. Health Sci. 2020, 12. [Google Scholar] [CrossRef]
- van Keulen, B.J.; Romijn, M.; Bondt, A.; Dingess, K.A.; Kontopodi, E.; van der Straten, K.; Den Boer, M.A.; Burger, J.A.; Poniman, M.; Bosch, B.J.; et al. Human Milk from Previously COVID-19-Infected Mothers: The Effect of Pasteurization on Specific Antibodies and Neutralization Capacity. Nutrients 2021, 13, 1645. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; Hakansson, A.P.; Hall, S.; Lavangnananda, S.; Fels, S.; Medo, E. Functional Antibodies against SARS-CoV-2 Receptor Binding Domain Variants with Mutations N501Y or E484K in Human Milk from COVID-19-Vaccinated, -Recovered, and -Unvaccinated Women. Breastfeed. Med. 2022, 17, 163–172. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; DaPra, C.; Fels, S.; Medo, E. Receptor-Binding Domain Severe Acute Respiratory Syndrome Coronavirus 2-Specific Antibodies in Human Milk from Mothers with Coronavirus Disease 2019 Polymerase Chain Reaction or with Symptoms Suggestive of Coronavirus Disease 2019. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 125–128. [Google Scholar] [CrossRef]
- Juncker, H.G.; Romijn, M.; Loth, V.N.; Ruhé, E.J.M.; Bakker, S.; Kleinendorst, S.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; et al. Antibodies against SARS-CoV-2 in Human Milk: Milk Conversion Rates in the Netherlands. J. Hum. Lact. 2021, 37, 469–476. [Google Scholar] [CrossRef]
- Pullen, K.M.; Atyeo, C.; Collier, A.R.Y.; Gray, K.J.; Belfort, M.B.; Lauffenburger, D.A.; Edlow, A.G.; Alter, G. Selective Functional Antibody Transfer into the Breastmilk after SARS-CoV-2 Infection. Cell Rep. 2021, 37, 109959. [Google Scholar] [CrossRef]
- Pace, R.M.; Williams, J.E.; Järvinen, K.M.; Belfort, M.B.; Pace, C.D.W.; Lackey, K.A.; Gogel, A.C.; Nguyen-Contant, P.; Kanagaiah, P.; Fitzgerald, T.; et al. Characterization of SARS-CoV-2 RNA, Antibodies, and Neutralizing Capacity in Milk Produced by Women with COVID-19. MBio 2021, 12, e03192-20. [Google Scholar] [CrossRef] [PubMed]
- Demers-Mathieu, V.; Dapra, C.; Medo, E. Comparison of Severe Acute Respiratory Syndrome Coronavirus 2-Specific Antibodies’ Binding Capacity between Human Milk and Serum from Coronavirus Disease 2019-Recovered Women. Breastfeed. Med. 2021, 16, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Young, B.E.; Seppo, A.E.; Diaz, N.; Rosen-Carole, C.; Nowak-Wegrzyn, A.; Cruz Vasquez, J.M.; Ferri-Huerta, R.; Nguyen-Contant, P.; Fitzgerald, T.; Sangster, M.Y.; et al. Association of Human Milk Antibody Induction, Persistence, and Neutralizing Capacity with SARS-CoV-2 Infection vs. MRNA Vaccination. JAMA Pediatr. 2021, 176, 159. [Google Scholar] [CrossRef] [PubMed]
- Juncker, H.G.; Romijn, M.; Loth, V.N.; Caniels, T.G.; de Groot, C.J.M.; Pajkrt, D.; van Gils, M.J.; van Goudoever, J.B.; van Keulen, B.J. Human Milk Antibodies against SARS-CoV-2: A Longitudinal Follow-up Study. J. Hum. Lact. 2021, 37, 485–491. [Google Scholar] [CrossRef]
- Pace, R.M.; Williams, J.E.; Järvinen, K.M.; Meehan, C.L.; Martin, M.A.; Ley, S.H.; Barbosa-Leiker, C.; Andres, A.; Yeruva, L.; Belfort, M.B.; et al. Milk from Women Diagnosed with COVID-19 Does Not Contain SARS-CoV-2 RNA but Has Persistent Levels of SARS-CoV-2-Specific IgA Antibodies. Front. Immunol. 2021, 12, 801797. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; Dapra, C.; Mathijssen, G.; Sela, D.A.; Järvinen, K.M.; Seppo, A.; Fels, S.; Medo, E. Human Milk Antibodies against S1 and S2 Subunits from SARS-CoV-2, HCoV-OC43, and HCoV-229E in Mothers with a Confirmed COVID-19 PCR, Viral SYMPTOMS, and Unexposed Mothers. Int. J. Mol. Sci. 2021, 22, 1749. [Google Scholar] [CrossRef]
- Juncker, H.G.; Mulleners, S.J.; van Gils, M.J.; Bijl, T.P.L.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; van Keulen, B.J. Comparison of SARS-CoV-2-Specific Antibodies in Human Milk after MRNA-Based COVID-19 Vaccination and Infection. Vaccines 2021, 9, 1475. [Google Scholar] [CrossRef]
- Fox, A.; Marino, J.; Amanat, F.; Oguntuyo, K.Y.; Hahn-Holbrook, J.; Lee, B.; Zolla-Pazner, S.; Powell, R.L. The IgA in Milk Induced by SARS-CoV-2 Infection Is Comprised of Mainly Secretory Antibody That Is Neutralizing and Highly Durable over Time. PLoS ONE 2022, 17, e0249723. [Google Scholar] [CrossRef]
- Leung, H.Y.H.; Leung, B.W.; Gil, M.M.; Rolle, V.; Moungmaithong, S.; Wang, C.C.; Poon, L.C. SARS-CoV-2-specific Antibodies and Neutralization Capacity in Breast Milk Following Infection vs. Vaccination. Ultrasound Obstet. Gynecol. 2022, 60, 425. [Google Scholar] [CrossRef]
- Marshall, N.E.; Blanton, M.B.; Doratt, B.M.; Malherbe, D.C.; Rincon, M.; True, H.; Mcdonald, T.; Beauregard, C.; Adatorwovor, R.; Messaoudi, I. SARS-CoV-2 Vaccine Booster Elicits Robust Prolonged Maternal Antibody Responses and Passive Transfer via the Placenta and Breastmilk. bioRxiv 2022, 11, 518385. [Google Scholar] [CrossRef] [PubMed]
- Longueira, Y.; Ojeda, D.S.; Battistelli, R.B.A.; Sanchez, L.; Oviedo Rouco, S.; Albano, D.; Guevara, E.; Valls, V.; Pando, M.A.; Gamarnik, A.V. SARS-CoV-2-Specific IgG and IgA Response in Maternal Blood and Breastmilk of Vaccinated Naïve and Convalescent Lactating Participants. Front. Immunol. 2022, 13, 5514. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Young, B.E.; Li, D.; Seppo, A.E.; Zhou, Q.; Wiltse, A.; Nowak-Wegrzyn, A.; Murphy, K.; Widrick, K.; Diaz, N.; et al. Broad cross-Reactive IgA and IgG against Human Coronaviruses in Milk Induced by COVID-19 Vaccination and Infection. medRxiv Prepr. Serv. Health Sci. 2022, 10, 980. [Google Scholar] [CrossRef] [PubMed]
- Esteve-Palau, E.; Gonzalez-Cuevas, A.; Guerrero, M.E.; Garcia-Terol, C.; Alvarez, M.C.; Garcia, G.; Moreno, E.; Medina, F.; Casadevall, D.; Diaz-Brito, V. Quantification and Progress over Time of Specific Antibodies against Severe Acute Respiratory Syndrome Coronavirus 2 in Breast Milk of Lactating Women Vaccinated with BNT162b2 Pfizer-BioNTech Coronavirus Disease 2019 Vaccine (LacCOVID). Open Forum Infect. Dis. 2022, 9, ofac239. [Google Scholar] [CrossRef]
- Low, J.M.; Gu, Y.; Ng, M.S.F.; Wang, L.W.; Amin, Z.; Zhong, Y.; Macary, P.A. Human Milk Antibodies after BNT162b2 Vaccination Exhibit Reduced Binding against SARS-CoV-2 Variants of Concern. Vaccines 2022, 10, 225. [Google Scholar] [CrossRef]
- Narayanaswamy, V.; Pentecost, B.T.; Schoen, C.N.; Alfandari, D.; Schneider, S.S.; Baker, R.; Arcaro, K.F. Neutralizing Antibodies and Cytokines in Breast Milk after Coronavirus Disease 2019 (COVID-19) MRNA Vaccination. Obstet. Gynecol. 2022, 139, 181–191. [Google Scholar] [CrossRef]
- Bender, J.M.; Lee, Y.; Cheng, W.A.; Marentes Ruiz, C.J.; Pannaraj, P.S. Coronavirus Disease 2019 Vaccine Booster Effects Are Seen in Human Milk Antibody Response. Front. Nutr. 2022, 9, 898849. [Google Scholar] [CrossRef]
- Selma-Royo, M.; Bäuerl, C.; Mena-Tudela, D.; Aguilar-Camprubí, L.; Pérez-Cano, F.J.; Parra-Llorca, A.; Lerin, C.; Martínez-Costa, C.; Collado, M.C. Anti-SARS-CoV-2 IgA and IgG in Human Milk after Vaccination Is Dependent on Vaccine Type and Previous SARS-CoV-2 Exposure: A Longitudinal Study. Genome Med. 2022, 14, 42. [Google Scholar] [CrossRef]
- Pietrasanta, C.; Darwich, A.; Ronchi, A.; Crippa, B.; Spada, E.; Mosca, F.; Pugni, L.; Rescigno, M. Humoral Response to Anti-SARS-CoV-2 Vaccine in Breastfeeding Mothers and Mother-to-Infant Antibody Transfer through Breast Milk. NPJ Vaccines 2022, 7, 63. [Google Scholar] [CrossRef]
- Ricciardi, A.; Zelini, P.; Cassaniti, I.; Avanzini, M.A.; Colaneri, M.; De Silvestri, A.; Baldanti, F.; Bruno, R. Serum and Breastmilk SARS-CoV-2 Specific Antibodies Following BNT162b2 Vaccine: Prolonged Protection from SARS-CoV-2 in Newborns and Older Children. Int. J. Infect. Dis. 2022, 122, 905. [Google Scholar] [CrossRef]
- Pieri, M.; Maniori, M.A.; Shahabian, L.; Kanaan, E.; Paphiti-Demetriou, I.; Pipis, S.; Felekkis, K.; Nicolaidou, V.; Papaneophytou, C. Survival of Vaccine-Induced Human Milk SARS-CoV-2 IgG, IgA and SIgA Immunoglobulins across Simulated Human Infant Gastrointestinal Digestion. Nutrients 2022, 14, 3368. [Google Scholar] [CrossRef] [PubMed]
- Stafford, L.; Valcarce, V.; Henry, M.; Neu, J.; Parker, L.; Martina, M.; Vicuna, V.; Gowen, T.; Cato, E.; Kosik, I.; et al. Detection of SARS-CoV-2 IgA and IgG in Human Milk and Breastfeeding Infant Stool 6 Months after Maternal COVID-19 Vaccination. J. Perinatol. 2023, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Trofin, F.; Nastase, E.V.; Iancu, L.S.; Constantinescu, D.; Cianga, C.M.; Lunca, C.; Ursu, R.G.; Cianga, P.; Dorneanu, O.S. Anti-RBD IgA and IgG Response and Transmission in Breast Milk of Anti-SARS-CoV-2 Vaccinated Mothers. Pathogens 2022, 11, 286. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Fox, A.; Decarlo, C.; Norris, C.; Griffin, S.; Wedekind, S.; Flanagan, J.M.; Shenker, N.; Powell, R.L. Comparative Profiles of SARS-CoV-2 Spike-Specific Human Milk Antibodies Elicited by MRNA-and Adenovirus-Based COVID-19 Vaccines. In Breastfeeding Medicine; Mary Ann Liebert, Inc.: New York, NY, USA, 2022; Volume 17, pp. 638–646. [Google Scholar] [CrossRef]
- Guida, M.; Terracciano, D.; Cennamo, M.; Aiello, F.; La Civita, E.; Esposito, G.; Gargiulo, V.; Maruotti, G.M.; Portella, G.; Sarno, L. COVID-19 Vaccine MRNABNT162b2 Elicits Human Antibody Response in Milk of Breastfeeding Women. Vaccines 2021, 9, 785. [Google Scholar] [CrossRef] [PubMed]
- Valcarce, V.; Stafford, L.S.; Neu, J.; Cacho, N.; Parker, L.; Mueller, M.; Burchfield, D.J.; Li, N.; Larkin, J. Detection of SARS-CoV-2-Specific IgA in the Human Milk of COVID-19 Vaccinated Lactating Health Care Workers. Breastfeed. Med. 2021, 16, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Lechosa-Muñiz, C.; Paz-Zulueta, M.; Mendez-Legaza, J.M.; Irure-Ventura, J.; González, R.C.; Montes, J.C.; López-Hoyos, M.; Llorca, J.; Cabero-Pérez, M.J. Induction of SARS-CoV-2-Specific IgG and IgA in Serum and Milk with Different SARS-CoV-2 Vaccines in Breastfeeding Women: A cross-Sectional Study in Northern Spain. Int. J. Environ. Res. Public Health 2021, 18, 8831. [Google Scholar] [CrossRef] [PubMed]
- Perez, S.E.; Luna Centeno, L.D.; Cheng, W.A.; Marentes Ruiz, C.J.; Lee, Y.; Congrave-Wilson, Z.; Powell, R.L.; Stellwagen, L.; Pannaraj, P.S. Human Milk SARS-CoV-2 Antibodies up to 6 Months after Vaccination. Pediatrics 2022, 149, e2021054260. [Google Scholar] [CrossRef]
- Golan, Y.; Prahl, M.; Cassidy, A.G.; Gay, C.; Wu, A.H.B.; Jigmeddagva, U.; Lin, C.Y.; Gonzalez, V.J.; Basilio, E.; Warrier, L.; et al. COVID-19 MRNA Vaccination in Lactation: Assessment of Adverse Events and Vaccine Related Antibodies in Mother-Infant Dyads. Front. Immunol. 2021, 12, 4596. [Google Scholar] [CrossRef] [PubMed]
- Jakuszko, K.; Kościelska-Kasprzak, K.; Żabińska, M.; Bartoszek, D.; Poznański, P.; Rukasz, D.; Kłak, R.; Królak-Olejnik, B.; Krajewska, M. Immune Response to Vaccination against COVID-19 in Breastfeeding Health Workers. Vaccines 2021, 9, 663. [Google Scholar] [CrossRef]
- Perl, S.H.; Uzan-Yulzari, A.; Klainer, H.; Asiskovich, L.; Youngster, M.; Rinott, E.; Youngster, I. SARS-CoV-2-Specific Antibodies in Breast Milk after COVID-19 Vaccination of Breastfeeding Women. JAMA 2021, 325, 2013–2014. [Google Scholar] [CrossRef]
- Low, J.M.; Gu, Y.; Ng, M.S.F.; Amin, Z.; Lee, L.Y.; Ng, Y.P.M.; Shunmuganathan, B.D.; Niu, Y.; Gupta, R.; Tambyah, P.A.; et al. Codominant IgG and IgA Expression with Minimal Vaccine MRNA in Milk of BNT162b2 Vaccinees. NPJ Vaccines 2021, 6, 105. [Google Scholar] [CrossRef] [PubMed]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. COVID-19 Vaccine Response in Pregnant and Lactating Women: A Cohort Study. medRxiv 2021, preprint. [Google Scholar] [CrossRef]
- Baird, J.K.; Jensen, S.M.; Urba, W.J.; Fox, B.A.; Baird, J.R. SARS-CoV-2 Antibodies Detected in Mother’s Milk Post-Vaccination. J. Hum. Lact. 2021, 37, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, D.S.R.; Perez, M.M.L.; Perez, M.C.; Hernandez, M.I.S.; Pulido, S.M.; Villacampa, L.P.; Vilar, A.M.F.; Falero, M.R.; Carretero, P.G.; Millan, B.R.; et al. SARS-CoV-2 Antibodies in Breast Milk after Vaccination. Pediatrics 2021, 148, e2021052286. [Google Scholar] [CrossRef]
- Juncker, H.G.; Mulleners, S.J.; van Gils, M.J.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; van Keulen, B.J. The Levels of SARS-CoV-2 Specific Antibodies in Human Milk Following Vaccination. J. Hum. Lact. 2021, 37, 477–484. [Google Scholar] [CrossRef]
- Rosenberg-Friedman, M.; Kigel, A.; Bahar, Y.; Werbner, M.; Alter, J.; Yogev, Y.; Dror, Y.; Lubetzky, R.; Dessau, M.; Gal-Tanamy, M.; et al. BNT162b2 MRNA Vaccine Elicited Antibody Response in Blood and Milk of Breastfeeding Women. Nat. Commun. 2021, 12, 6222. [Google Scholar] [CrossRef]
- Scrimin, F.; Campisciano, G.; Comar, M.; Ragazzon, C.; Davanzo, R.; Quadrifoglio, M.; Giangreco, M.; Stabile, G.; Ricci, G. IgG and IgA Antibodies Post SARS-CoV-2 Vaccine in the Breast Milk and Sera of Breastfeeding Women. Vaccines 2022, 10, 125. [Google Scholar] [CrossRef]
- Charepe, N.; Gonçalves, J.; Juliano, A.M.; Lopes, D.G.; Canhão, H.; Soares, H.; Serrano, E.F. COVID-19 MRNA Vaccine and Antibody Response in Lactating Women: A Prospective Cohort Study. BMC Pregnancy Childbirth 2021, 21, 632. [Google Scholar] [CrossRef]
- Gonçalves, J.; Juliano, A.M.; Charepe, N.; Alenquer, M.; Athayde, D.; Ferreira, F.; Archer, M.; Amorim, M.J.; Serrano, F.; Soares, H. Secretory IgA and T Cells Targeting SARS-CoV-2 Spike Protein Are Transferred to the Breastmilk upon MRNA Vaccination. Cell Rep. Med. 2021, 2, 100468. [Google Scholar] [CrossRef]
- Esteve-Palau, E.; Gonzalez-Cuevas, A.; Guerrero, M.E.; Garcia-Terol, C.; Alvarez, M.C.; Casadevall, D.; Diaz-Brito, V. Quantification of Specific Antibodies against SARS-CoV-2 in Breast Milk of Lactating Women Vaccinated with an MRNA Vaccine. JAMA Netw. Open 2021, 4, e2120575. [Google Scholar] [CrossRef]
- Yeo, K.T.; Chia, W.N.; Tan, C.W.; Ong, C.; Yeo, J.G.; Zhang, J.; Poh, S.L.; Lim, A.J.M.; Sim, K.H.Z.; Sutamam, N.; et al. Neutralizing Activity and SARS-CoV-2 Vaccine MRNA Persistence in Serum and Breastmilk after BNT162b2 Vaccination in Lactating Women. Front. Immunol. 2022, 12, 5793. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.; Nir, O.; Toussia-Cohen, S.; Leibovich, L.; Strauss, T.; Asraf, K.; Doolman, R.; Sharabi, S.; Cohen, C.; Levin, E.G.; et al. Presence of SARS-CoV-2 Antibodies in Lactating Women and Their Infants Following BNT162b2 Messenger RNA Vaccine. Am. J. Obstet. Gynecol. 2021, 225, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.C.; Carter, E.B.; Raghuraman, N.; Nolan, L.S.; Gong, Q.; Lewis, A.N.; Good, M. Anti–Severe Acute Respiratory Syndrome Coronavirus 2 Antibodies Induced in Breast Milk after Pfizer-BioNTech/BNT162b2 Vaccination. Am. J. Obstet. Gynecol. 2021, 225, 101–103. [Google Scholar] [CrossRef] [PubMed]
- Scaggs Huang, F. Are SARS-CoV-2 Antibodies Detectable in Human Milk after Vaccination against COVID-19? J. Pediatric Infect. Dis. Soc. 2022, 11, 126. [Google Scholar] [CrossRef]
- Agostinis, C.; Toffoli, M.; Balduit, A.; Mangogna, A.; Yasmin, H.; Ragazzon, C.; Pegoraro, S.; Campisciano, G.; Stabile, G.; Zito, G.; et al. Anti-Spike Antibodies Present in the Milk of SARS-CoV-2 Vaccinated Mothers Are Complement-Activating. Int. J. Mol. Sci. 2023, 24, 4395. [Google Scholar] [CrossRef]
- Gu, Y.; Low, J.M.; Tan, J.S.Y.; Ng, M.S.F.; Ng, L.F.P.; Shunmuganathan, B.; Gupta, R.; MacAry, P.A.; Amin, Z.; Lee, L.Y.; et al. Immune and Pathophysiologic Profiling of Antenatal Coronavirus Disease 2019 in the GIFT Cohort: A Singaporean Case-Control Study. Front. Pediatr. 2022, 10, 949756. [Google Scholar] [CrossRef]
- Martin-Vicente, M.; Carrasco, I.; Muñoz-Gomez, M.J.; Lobo, A.H.; Mas, V.; Vigil-Vázquez, S.; Vázquez, M.; Manzanares, A.; Cano, O.; Alonso, R.; et al. Antibody Levels to SARS-CoV-2 Spike Protein in Mothers and Children from Delivery to Six Months Later. Birth 2022. [Google Scholar] [CrossRef]
- Dutra, L.V.; Silva, M.H.; Lebrão, C.W.; Affonso-Fonseca, F.L.; Suano-Souza, F.I. Impact of the Presence Anti-SARS-CoV-2 IgA in the Colostrum of Women Infected by COVID-19 During the Pregnancy in Neonatal Clinical Outcomes: A cross-Sectional Study. Matern. Child Health J. 2023, 27, 737. [Google Scholar] [CrossRef]
- Wachman, E.M.; Snyder-Cappione, J.; Devera, J.; Boateng, J.; Dhole, Y.; Clarke, K.; Yuen, R.R.; Parker, S.E.; Hunnewell, J.; Ferraro, R.; et al. Maternal, Infant, and Breast Milk Antibody Response Following COVID-19 Infection in Early versus Late Gestation. Pediatr. Infect. Dis. J. 2023, 42, e70–e76. [Google Scholar] [CrossRef]
- Calabretto, M.; D’Alisa, R.; Faraone, S.; Mazzuti, L.; Pecorini, F.; Turriziani, O. Detection of SARS-CoV-2 RNA and Antibodies in Breast Milk of Infected Mothers. J. Med. Virol. 2023, 95, e28142. [Google Scholar] [CrossRef]
- Narayanaswamy, V.; Pentecost, B.T.; Telfer, J.C.; Burnside, A.S.; Schneider, S.S.; Alfandari, D.; Baker, R.L.; Saiju, A.; Nodiff, S.; Arcaro, K.F. Durable Antibody and Effector Memory T Cell Responses in Breastmilk from Women with SARS-CoV-2. Front. Immunol. 2022, 13, 985226. [Google Scholar] [CrossRef] [PubMed]
- Bode, L.; Bertrand, K.; Najera, J.A.; Furst, A.; Honerkamp-Smith, G.; Shandling, A.D.; Chambers, C.D.; Camerini, D.; Campo, J.J. Characterization of SARS-CoV-2 Antibodies in Human Milk from 21 Women with Confirmed COVID-19 Infection. Pediatr. Res. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lechosa-Muñiz, C.; Paz-Zulueta, M.; Irure-Ventura, J.; Mendez-Legaza, J.M.; Cuesta González, R.; Gómez-Acebo, I.; López-Hoyos, M.; Llorca, J.; Cabero-Pérez, M.J. Development of SARS-CoV-2 Specific IgG and IgA Antibodies in Serum and Milk with Different SARS-CoV-2 Vaccines in Lactating Women. Int. Breastfeed. J. 2023, 18, 3. [Google Scholar] [CrossRef] [PubMed]
- Demers-Mathieu, V.; Huston, R.K.; Markell, A.M.; McCulley, E.A.; Martin, R.L.; Dallas, D.C. Antenatal Influenza A-Specific IgA, IgM, and IgG Antibodies in Mother’s Own Breast Milk and Donor Breast Milk, and Gastric Contents and Stools from Preterm Infants. Nutrients 2019, 11, 1567. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; Underwood, M.A.; Beverly, R.L.; Dallas, D.C. Survival of Immunoglobulins from Human Milk to Preterm Infant Gastric Samples at 1, 2, and 3 Hours Postprandial. Neonatology 2018, 114, 242. [Google Scholar] [CrossRef]
- Thai, J.D.; Gregory, K.E. Bioactive Factors in Human Breast Milk Attenuate Intestinal Inflammation during Early Life. Nutrients 2020, 12, 581. [Google Scholar] [CrossRef]
- Hurley, W.L.; Theil, P.K. Perspectives on Immunoglobulins in Colostrum and Milk. Nutrients 2011, 3, 442–474. [Google Scholar] [CrossRef]
- Goldman, A.S.; Chheda, S.; Keeney, S.E.; Schmalstieg, F.C. Immunology of Human Milk and Host Immunity. Fetal Neonatal Physiol. 2020, 2011, 1690–1701. [Google Scholar] [CrossRef]
- Yaugel-Novoa, M.; Bourlet, T.; Paul, S. Role of the Humoral Immune Response during COVID-19: Guilty or Not Guilty? Mucosal Immunol. 2022, 15, 1170–1180. [Google Scholar] [CrossRef]
- Michaud, E.; Mastrandrea, C.; Rochereau, N.; Paul, S. Human Secretory IgM: An Elusive Player in Mucosal Immunity. Trends Immunol. 2020, 41, 141–156. [Google Scholar] [CrossRef]
- Van de Perre, P.; Simonon, A.; Karita, E.; Butera, J.B.; Hitimana, D.G.; Mukamabano, B.; Van Goethem, C.; Lepage, P.; Dabis, F.; Msellati, P. Infective and Anti-Infective Properties of Breastmilk from HIV-1-Infected Women. Lancet 1993, 341, 914–918. [Google Scholar] [CrossRef] [PubMed]
- Vidarsson, G.; Dekkers, G.; Rispens, T. IgG Subclasses and Allotypes: From Structure to Effector Functions. Front. Immunol. 2014, 5, 520. [Google Scholar] [CrossRef] [PubMed]
- Morales-Núñez, J.J.; Muñoz-Valle, J.F.; Torres-Hernández, P.C.; Hernández-Bello, J. Overview of Neutralizing Antibodies and Their Potential in COVID-19. Vaccines 2021, 9, 1376. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).