
Introduction of Complementary Foods and the Risk of Sensitization and Allergy in Children up to Three Years of Age


Abstract
:1. Introduction
2. Materials and Methods
- -
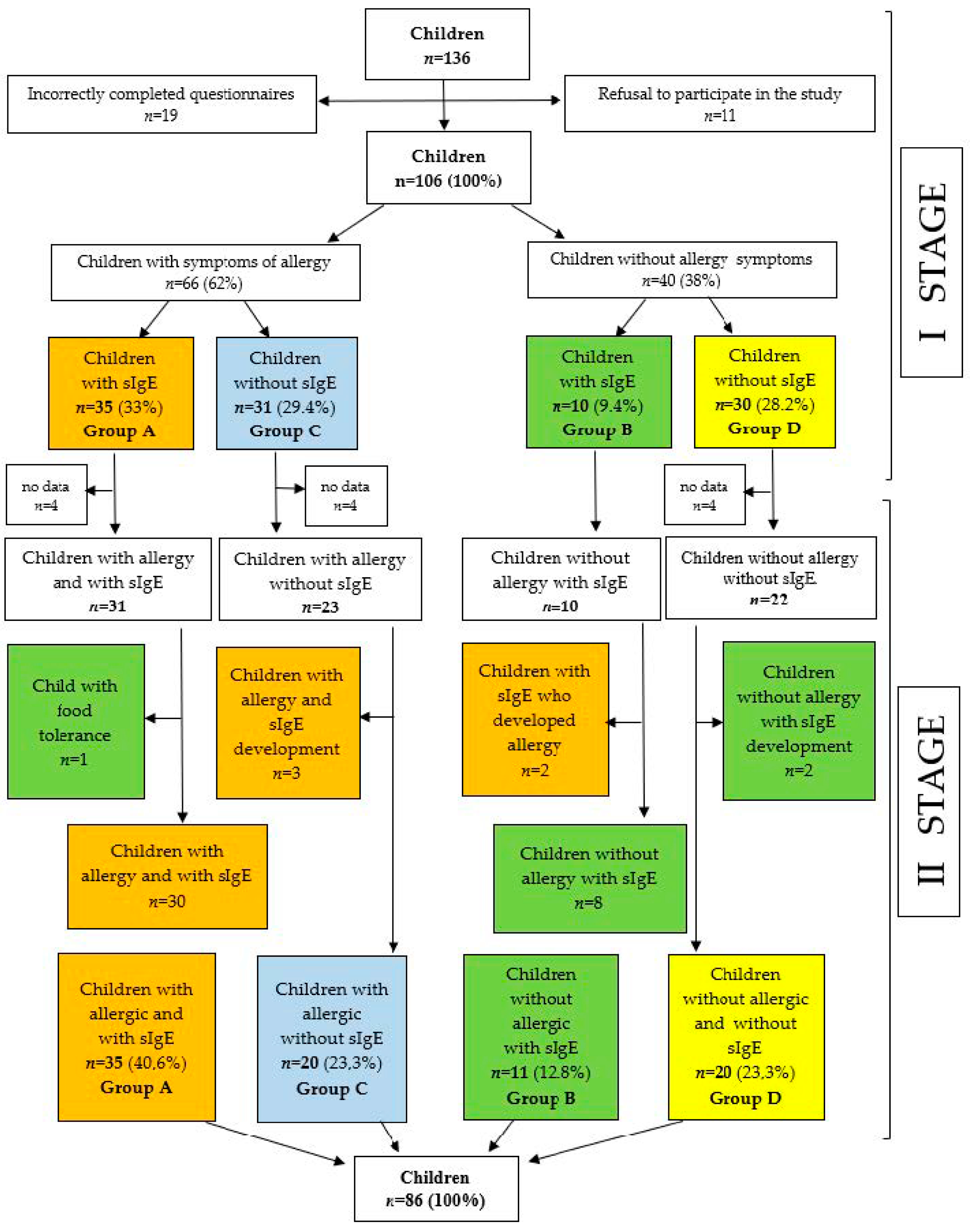
- Group A: children with allergic symptoms and concomitant sensitization (i.e., children with IgE-mediated allergy);
- -
- Group B: children without allergic symptoms, with concomitant sensitization sensitized children);
- -
- Group C: children with allergic symptoms, without concomitant sensitization (i.e., children with non-IgE-mediated allergy);
- -
- Group D: children without allergic symptoms and without concomitant sensitization (i.e., healthy children).
2.1. Statistical Analysis
2.2. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Platts-Mills, T.A.E. The allergy epidemics: 1870–2010. J. Allergy Clin. Immunol. 2015, 136, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Wypych, T.P.; Marsland, B.J. Diet Hypotheses in Light of the Microbiota Revolution: New Perspectives. Nutrients 2017, 9, 537. [Google Scholar] [CrossRef] [PubMed]
- Kuśmierek, M.; Sardecka, I.; Łoś-Rycharska, E.; Krogulska, A. The impact of immunomodulatory factors from maternal diet during pregnancy on cow’s milk allergy in offspring—A pilot study in the paediatric population of the Kuyavian—Pomeranian Voivodship. Allergol. Immunopathol. 2019, 47, 570–578. [Google Scholar] [CrossRef]
- El-Gamal, Y.; Elmasry, O.; El-Ghoneimy, D.; Cunha, S.; Chivinge, J.; Robinson, Z.; Boyle, R.J. Immunomodulatory effects of food. Egypt. J. Pediatr. Allergy Immunol. 2011, 9, 3–13. [Google Scholar]
- Garcia-Larsen, V.; Ierodiakonou, D.; Jarrold, K.; Cunha, S.; Chivinge, J.; Robinson, Z.; Geoghegan, N.; Ruparelia, A.; Devani, P.; Trivella, M.; et al. Diet during pregnancy and infancy and risk of allergic or autoimmune disease: A systematic review and meta-analysis. PLoS Med. 2018, 15, e1002507. [Google Scholar] [CrossRef] [PubMed]
- Muraro, A.; Werfel, T.; Hoffmann-Sommergruber, K.; Roberts, G.; Beyer, K.; Bindslev-Jensen, C.; Cardona, V.; Dubois, A.; Dutoit, G.; Eigenmann, P.; et al. EAACI food allergy and anaphylaxis guidelines: Diagnosis and maagement of food allergy. Allergy 2014, 69, 1008–1025. [Google Scholar] [CrossRef]
- Kaczmarski, M.; Wasilewska, J.; Jarocka-Cyrta, E.; Cudowska, B.; Żur, E.; Matuszewska, E.; Jastrzębska-Piotrowska, J. Polish statement on food allergy in children and adolescents. Post. Dermatol. Alergol. 2011, 28, 331–367. [Google Scholar]
- Fiocchi, A.; Brozek, J.; Schünemann, H.; Bahna, S.L.; Von Berg, A.; Beyer, K.; Bozzola, M.; Bradsher, J.; Compalati, E.; Ebisawa, M.; et al. World Allergy Organization (WAO) Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA) Guidelines. Pediatr. Allergy Immunol. 2010, 21, 1–125. [Google Scholar] [CrossRef]
- Caffarelli, C.; Di Mauro, D.; Mastrorilli, C.; Bottau, P.; Cipriani, F.; Ricci, G. Solid Food Introduction and the Development of Food Allergies. Nutrients 2018, 10, 1790. [Google Scholar] [CrossRef]
- Agostoni, C.; Decsi, T.; Fewtrell, M.; Goulet, O.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; van Goudoever, J. Complementary Feeding: A Commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 99–110. [Google Scholar] [CrossRef]
- Katz, Y.; Rajuan, N.; Goldberg, M.R.; Eisenberg, E.; Heyman, E.; Cohen, A.; Leshno, M. Early exposure to cow’s milk protein is protective against IgE-mediated cow’s milk protein allergy. J. Allergy Clin. Immunol. 2010, 126, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Fleischer, D.M.; Chan, E.S.; Venter, C.; Spergel, J.M.; Abrams, E.M.; Stukus, D.; Groetch, M.; Shaker, M.; Greenhawt, M. A Consensus Approach to the Primary Prevention of Food Allergy Through Ntrtion: Guidance from the American Academy of Allergy, Asthma, and Immunology; American College of Allergy, Asthma, and Immunology; and the Canadian Society for Allergy and Clinical Immunology. J. Allergy Clin. Immunol. Pract. 2021, 9, 22–43.e4. [Google Scholar] [CrossRef] [PubMed]
- Halken, S.; Muraro, A.; Silva, D.; Khaleva, E.; Angier, E.; Arasi, S.; Arshad, H.; Bahnson, H.T.; Beyer, K.; Boyle, R.; et al. EAACI guideline: Preventing the development of food allergy in infants and young children (2020 update). Pediatr. Allergy Immunol. 2021, 32, 843–858. [Google Scholar] [CrossRef] [PubMed]
- Hanifin, J.M.; Rajka, G. Diagnostic features of atopic dermatitis. Acta Derm. Venereol. 1980, 92, 44–47. [Google Scholar] [CrossRef]
- Kaczmarski, M.; Cudowska, B.; Bandzul, K.; Witkowska, T.; Parfieniuk, W.l. The prevalence of food allergy in infants in north-east Poland. Nowa Pediatr. 1999, 4, 26–28. [Google Scholar]
- Tham, E.H.; Lee, B.W.; Chan, Y.H.; Loo, E.X.L.; Toh, J.Y.; Goh, A.; Teoh, O.H.; Yap, F.; Tan, K.H.; Godfrey, K.M.; et al. Low Food Allergy Prevalence Despite Delayed Introduction of Allergenic Foods—Data from the GUSTO Cohort. J. Allergy Clin. Immunol. Pract. 2018, 6, 466–475. [Google Scholar] [CrossRef]
- de Silva, D.; Halken, S.; Singh, C.; Muraro, A.; Angier, E.; Arasi, S.; Arshad, H.; Beyer, K.; Boyle, R.; Du Toit, G.; et al. Preventing food allergy in infancy and childhood: Systematic review of randomised controlled trials. Pediatr. Allergy Immunol. 2020, 31, 813–826. [Google Scholar] [CrossRef]
- Sakihara, T.; Otsuji, K.; Arakaki, Y.; Hamada, K.; Sugiura, S.; Ito, K. Early Discontinuation of Cow’s Milk Protein Ingestion Is Associated with the Devoment of Cow’s Milk Allergy. J. Allergy Clin. Immunol. Pract. 2022, 10, 172–179. [Google Scholar] [CrossRef]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Mis, N.F.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef]
- Kull, I.; Bergstrom, A.; Lilja, G.; Pershagen, G.; Wickman, M. Fish consumption during the first year of life and development of allergic diseases during childhood. Allergy 2006, 61, 1009–1015. [Google Scholar] [CrossRef]
- Maslin, K.; Galvin, A.D.; Shepherd, S. A qualitative study of mothers’ perceptions of weaning and the use of commercial infant food in the United Kingdom. Matern. Paediatr. Nutr. 2015, 1, 103. [Google Scholar] [CrossRef]
- Andrusaityte, S.; Grazuleviciene, R.; Petraviciene, I. Effect of Diet and Maternal Education on Allergies Among Preschool Chidren: A Case-Control Study. Environ. Res. 2017, 159, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, B.; Novak, N. Effects of Daily Food Processing on Allergenicity. Crit. Rev. Food Sci. Nutr. 2019, 59, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Vissers, Y.M.; Blanc, F.; Skov, P.S.; Johnson, P.E.; Rigby, N.M.; Przybylski-Nicaise, L.; Bernard, H.; Wal, J.-M.; Ballmer-Weber, B.; Zuidmeer-Jongejan, L.; et al. Effect of heating and glycation on the allergenicity of 2S albumins (Ara h 2/6) from peanut. PLoS ONE 2011, 6, e23998. [Google Scholar] [CrossRef]
- European Nut Association. Available online: http://www.groundnuts.eu/europe (accessed on 20 December 2022).
- Beyer, K.; Morrow, E.; Li, X.M.; Bardina, L.; Bannon, G.A.; Burks, A.W.; Sampson, H.A. Effects of cooking methods on peanut allergenicity. J. Allergy Clin. Immunol. 2001, 107, 1077–1081. [Google Scholar] [CrossRef]
- Tao, T.; Bernardo, B.K.; Eldi, P.; Chegeni, N.; Wiese, M.; Colella, A.; Kral, A.; Hayball, J.; Smith, W.; Forsyth, K.; et al. Extended boiling of peanut progressively reduces IgE allergenicity while retaining T cell reactivity. Clin. Exp. Allergy 2016, 46, 1004–1014. [Google Scholar] [CrossRef]
- Hourihane, J.O.; Bedwani, S.J.; Dean, T.P.; Warner, J.O. Randomised, double blind, crossover challenge study of allergenicity of peanut oils in subjects allergic to peanuts. BMJ 1997, 314, 1084–1088. [Google Scholar] [CrossRef]
- Blom, W.M.; Kruizinga, A.G.; Rubingh, C.M.; Remington, B.C.; Crevel, R.W.; Houben, G.F. Assessing food allergy risks from residual peanut protein in higly refined vegetable oil. Food Chem. Toxicol. 2017, 106 Pt A, 306–313. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Parameter | Total n = 86 (100%) | Group A n = 35 (40.6%) | Group B n = 11 (12.8%) | Group C n = 20 (23.3%) | Group D n = 20 (23.3%) | p | |
|---|---|---|---|---|---|---|---|
| The course of pregnancy, n (%) | |||||||
| 80 (93.1) | 33 (94.2) | 11 (100) | 19 (95) | 17 (85) | >0.05 | |
| 6 (6.9) | 2 (5.7) | 0 (0) | 1 (5) | 3 (15) | ||
| Type of delivery, n (%) | >0.05 | ||||||
| 55 (63.9) | 23 (65.7) | 7 (63.6) | 11 (55) | 14 (70) | ||
| 31 (36.1) | 12 (34.3) | 4 (36.4) | 9 (45) | 6 (30) | ||
| Duration of pregnancy, Hbd | >0.05 | ||||||
| median (Q1–Q3) | 39 (38–40) | 39 (38–41) | 40 (39.5–40) | 38.5 (36–40) | 39 (38–40) | ||
| Birth weight (grams) | >0.05 | ||||||
| mean ± SD | 3256 ± 591.9 | 3376 ± 586.2 | 3330 ± 495.5 | 3096 ± 742.9 | 3177 ± 550.5 | ||
| Points on the Apgar scale | >0.05 | ||||||
| median (Q1–Q3) | 10 (10–10) | 10 (10–10) | 10 (10–10) | 10 (8.5–10) | 10 (10–10) | ||
| Age of the child, month | >0.05 | ||||||
| mean ± SD | 31.9 ± 3.5 | 31.9 ± 3.8 | 32.5 ± 3.2 | 31.9 ± 3.2 | 31.9 ± 3.2 | ||
| Sex, n (%) | >0.05 | ||||||
| 50 (58.1) | 23 (65.7) | 5 (45.5) | 8 (40) | 14 (70) | ||
| 36 (41.9) | 12 (34.3) | 6 (54.5) | 12 (60) | 6 (30) | ||
| Having siblings, n (%) | >0.05 | ||||||
| 39 (45.3) | 18 (51.4) | 6 (54.5) | 14 (70) | 9 (45) | ||
| 47 (54.7) | 17 (48.6) | 5 (45.5) | 6 (30) | 11 (55) | ||
| Number of children in the family, n (%) | >0.05 | ||||||
| 47(54.6) | 18 (51.4) | 6 (54.5) | 14 (70) | 9 (45) | ||
| 28 (32.6) | 13 (37.1) | 2 (18.2) | 4 (20) | 9 (45) | ||
| 7 (8.1) | 3 (8.6) | 2 (18.2) | 2 (10) | 0 (0) | ||
| 4 (4.7) | 1 (2.9) | 1 (9.1) | 0 (0) | 2 (10) | ||
| Order of birth, n (%) | >0.05 | ||||||
| 49 (57.0) | 19 (54.3) | 7 (63.6) | 14 (70) | 9 (45) | ||
| 26 (30.2) | 12 (34.3) | 1 (9.1) | 4 (20) | 9 (45) | ||
| 7 (8.1) | 3 (8.6) | 2 (18.2) | 2 (10) | 0 (0) | ||
| 4 (4.7) | 1 (2.9) | 1 (9.1) | 0 (0) | 2 (10) | ||
| Place of living, n (%) | 0.05 | ||||||
| 24 (43.6) | 13 (37.1) | 2 (18.2) | 5 (25) | 11 (55) | ||
| 14 (25.4) | 12 (34.3) | 2 (18.2) | 6 (30) | 2 (10) | ||
| 17 (31.0) | 10 (28.6) | 7 (62.6) | 9 (45) | 7 (35) | ||
| Parent age, years | >0.05 | ||||||
| 30.3 ± 4.9 | 30.7 ± 4.6 | 29.8 ± 5.5 | 33.2 ± 5.2 | 29.6 ± 5.6 | ||
| 32.7 ± 4.6 | 32.8 ± 4.6 | 32.8 ± 6.2 | 35.9 ± 6.1 | 32.5 ± 4.6 | ||
| Parent’s education, n (%) | >0.05 | ||||||
| mother | |||||||
| 5 (9.1) | 0 (0) | 3 (27.3) | 1 (5) | 5 (25) | ||
| 12 (21.8) | 10 (28.6) | 2 (18.2) | 1 (5) | 2 (10) | ||
| 38 (69.1) | 25 (71.4) | 6 (54.5) | 18 (90) | 13 (65) | ||
| father | >0.05 | ||||||
| 10 (18.2) | 6 (17.1) | 4 (36.4) | 2 (10) | 4 (20) | ||
| 14 (25.4) | 9 (25.7) | 3 (27.3) | 5 (25) | 5 (25) | ||
| 31 (5.4) | 20 (57.1) | 4 (36.4) | 13 (65) | 11 (55) | ||
| Family history of atopy | 59 (68.6) | 28 (80) | 5 (45.5) | 15 (75) | 11 (55) | 0.0002 | |
| Allergies in family members | >0.05 | ||||||
| 18 (20.9) | 10 (28.6) | 1 (9.1) | 3 (15) | 4 (20) | ||
| 26 (30.2) | 13 (37.1) | 3 (27.3) | 5 (25) | 5 (25) | ||
| 17 (19.8) | 8 (22.9) | 0 (0) | 7 (35) | 2 (10) | ||
| 12 (13.9) | 5 (14.3) | 3 (23.3) | 2 (10) | 2 (10) | ||
| Type of allergy in the family | >0.05 | ||||||
| 29 (33.7) | 13 (37.1) | 4 (36.4) | 7 (35) | 5 (25) | ||
| 23 (26.7) | 13 (37.1) | 0 (0) | 7 (35) | 3 (15) | ||
| 49 (57) | 27 (77.1) | 4 (36.4) | 10 (50) | 8 (40) | ||
| Time of Introducing Complementary Foods | Group A + C n = 55 (100%) | Group B + D n = 31 (100%) | p | Group A n = 35 (100%) | Group D n = 20 (100%) | p | Group A + B n = 46 (100%) | Group C + D n = 40 (100%) | p |
|---|---|---|---|---|---|---|---|---|---|
| Egg white | 0.89 | 1.00 | 0.53 | ||||||
| ≤3 m | 3 (5.5) | 2 (6.5) | 3 (8.6) | 1 (5) | 4 (8.7) | 1 (2.5) | |||
| 4–6 m | 5 (9.1) | 2 (6.5) | 3 (8.6) | 1 (5) | 4 (8.7) | 3 (7.5) | |||
| 7–12 m | 47 (85.5) | 27 (87.1) | 29 (82.9) | 18 (90) | 38 (82.6) | 36 (90) | |||
| Milk | 0.64 | 0.82 | 0.63 | ||||||
| ≤3 m | 4 (7.4) | 1 (3.3) | 3 (8.8) | 1 (5.3) | 3 (6.7) | 2 (5.1) | |||
| 4–6 m | 15 (27.8) | 11 (36.7) | 9 (26.5) | 4 (21.1) | 16 (35.6) | 10 (25.6) | |||
| 7–12 m | 35 (64.8) | 18 (60) | 22 (64.7) | 14 (73.7) | 26 (57.8) | 27 (69.2) | |||
| Peanuts | 0.66 | 1.00 | 1.00 | ||||||
| ≤3 m | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| 4–6 m | 2 (13.3) | 4 (23.5) | 2 (18.2) | 4 (25) | 2 (16.7) | 4 (20) | |||
| 7–12 m | 13 (86.7) | 13(76.5) | 9 (81.8) | 12 (75) | 10 (83.3) | 16 (80) | |||
| Wheat | 0.59 | 0.09 | 0.06 | ||||||
| ≤3 m | 2 (3.7) | 1 (3.3) | 2 (5.7) | 1 (5.3) | 2 (4.3) | 1 (2.6) | |||
| 4–6 m | 11 (20.4) | 10 (33.3) | 4 (11.4) | 7 (36.8) | 7 (15.2) | 14 (36.8) | |||
| 7–12 m | 41 (75.9) | 19 (63.3) | 29 (82.9) | 11 (57.9) | 37 (80.4) | 23 (60.5) | |||
| Soybean | 1.00 | 0.56 | 0.26 | ||||||
| ≤3 m | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| 4–6 m | 2 (28.6) | 4 (33.3) | 2 (50) | 3 (27.3) | 3 (60) | 3 (21.4) | |||
| 7–12 m | 5 (71.4) | 8 (66.7) | 2 (50) | 8 (72.7) | 2 (40) | 11 (78.6) | |||
| Fish | 0.42 | 0.43 | 0.21 | ||||||
| ≤3 m | 5 (9.3) | 1 (3.3) | 2 (5.9) | 1 (5.3) | 2 (4.4) | 4 (10.3) | |||
| 4–6 m | 11 (20.4) | 9 (30) | 5 (14.7) | 6 (31.6) | 8 (17.8) | 12 (30.8) | |||
| 7–12 m | 38 (70.4) | 20(66.7) | 27 (79.4) | 12 (63.2) | 35 (77.8) | 23 (59) | |||
| Tree nuts | 1.00 | 1.00 | 0.62 | ||||||
| ≤3 m | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| 4–6 m | 2 (22.2) | 2 (16.7) | 2 (25) | 2 (16.7) | 2 (25) | 2 (15.4) | |||
| 7–12 m | 7 (77.8) | 10 (83.3) | 6 (75) | 10 (83.3) | 6 (75) | 11 (84.6) | |||
| Shellfish | >0.05 | >0.05 | >0.05 | ||||||
| ≤3 m | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| 4–6 m | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| 7–12 m | 2 (100) | 4 (100) | 2 (100) | 4 (100) | 2 (100) | 4 (100) |
| Frequency and Form of Food Supply | Groups A + C n = 55 (100%) | Groups B + D n = 31 (100%) | p | Group A n = 35 (100%) | Group D n = 20 (100%) | p | Groups A + B n = 46 (100%) | Groups C + D n = 40 (100%) | p |
|---|---|---|---|---|---|---|---|---|---|
| Frequency of egg white supply, n (%) | 0.083 | 0.15 | 0.845 | ||||||
| 1–2x/day | 20 (37) | 5 (16.1) | 11 (32.4) | 2 (10) | 14 (31.1) | 11 (27.5) | |||
| 1–3x/week | 27 (50) | 23 (74.2) | 18 (52.9) | 16 (80) | 25 (55.6) | 25 (62.5) | |||
| 1–3x/month | 7 (13) | 3 (9.7) | 5 (14.7) | 2 (10) | 6 (13.3) | 4 (10) | |||
| Form of egg protein supply, n (%) | 0.066 | 0.189 | 0.484 | ||||||
| raw | 1 (1.8) | 3 (9.7) | 1 (2.9) | 2 (10) | 2 (4.3) | 2 (5) | |||
| boiled | 49 (89.1) | 28 (90.3) | 30 (85.7) | 18 (90) | 40 (87) | 37 (92.5) | |||
| baked | 5 (9.1) | 0 (0) | 4 (11.4) | 0 (0) | 4 (8.7) | 1 (2.5) | |||
| Frequency of milk supply, n (%) | 0.715 | 0.248 | 0.269 | ||||||
| 1–2x/day | 37 (68.5) | 18 (60) | 23 (67.6) | 9 (47.4) | 32 (71.1) | 23 (59) | |||
| 1–3x/week | 13 (24.1) | 10 (33.3) | 7 (20.6) | 8 (42.1) | 9 (20) | 14 (35.9) | |||
| 1–3x/month | 4 (7.4) | 2 (6.7) | 4 (11.8) | 2 (105) | 4 (8.9) | 2 (5.1) | |||
| Form of milk supply, n (%) | 0.024 | 0.15 | 1.00 | ||||||
| raw | 9 (16.7) | 0 (0) | 5 (14.7) | 0 (0) | 5 (11.1) | 4 (10.5) | |||
| boiled | 45 (83.3) | 29 (100) | 29 (85.3) | 18 (100) | 40 (88.9) | 34 (89.5) | |||
| baked | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| Frequency of peanuts supply, n (%) | >0.05 | >0.05 | >0.05 | ||||||
| 1–2x/day | 1 (6.7) | 0 (0) | 1 (9.1) | 0 (0) | 1 (8.3) | 0 (0) | |||
| 1–3x/week | 2 (13.3) | 1 (5.9) | 2 (18.2) | 0 (0) | 3 (25) | 0 (0) | |||
| 1–3x/month | 12 (80) | 16 (94.1) | 8 (72.7) | 16 (100) | 8 (66.7) | 20 (100) | |||
| Form of peanuts supply, n (%) | 0.07 | 0.028 | 0.108 | ||||||
| raw | 7 (46.7) | 7 (41.2) | 6 (54.5) | 7 (43.8) | 6 (50) | 8 (40) | |||
| boiled | 5 (33.3) | 9 (52.9) | 3 (27.3) | 9 (56.2) | 4 (33.3) | 10 (50) | |||
| baked | 3 (20) | 1 (5.9) | 2 (18.2) | 0 (0) | 2 (16.7) | 2 (10) | |||
| Frequency of wheat supply, n (%) | >0.05 | 0.267 | >0.05 | ||||||
| 1–2x/day | 32 (60.4) | 15 (50) | 20 (58.8) | 8 (42.1) | 27 (60) | 20 (52.6) | |||
| 1–3x/week | 20 (37.7) | 14 (46.7) | 14 (41.2) | 11 (57.9) | 17 (37.8) | 17 (44.7) | |||
| 1–3x/month | 1 (1.9) | 1 (3.3) | 0 (0) | 0 (0) | 1 (2.2) | 1 (2.6) | |||
| Form of wheat supply, n (%) | >0.05 | >0.05 | >0.05 | ||||||
| boiled | 26 (49) | 7 (23.3) | 15 (44.1) | 3 (15.8) | 19 (42.2) | 15 (39.5) | |||
| baked | 27 (51) | 23 (76.7) | 19 (55.9) | 16 (84.2) | 26 (57.8) | 23 (60.5) | |||
| Frequency of soy supply, n (%) | >0.05 | >0.05 | >0.05 | ||||||
| 1–2x/day | 0 (0) | 2 (16.7) | 0 (0) | 2 (18.2) | 0 (0) | 2 (14.3) | |||
| 1–3x/week | 1 (14.3) | 7 (58.3) | 0 (0) | 7 (63.6) | 0 (0) | 8 (57.1) | |||
| 1–3x/month | 6 (85.7) | 3 (25) | 4 (100) | 2 (18.2) | 5 (100) | 4 (28.6) | |||
| Form of soy supply, n (%) | 0.074 | 0.56 | 1.00 | ||||||
| boiled | 5 (71.4) | 3 (25) | 2 (50) | 3 (27.3) | 2 (40) | 6 (42.9) | |||
| baked | 2 (28.6) | 9 (75) | 2 (50) | 8 (72.7) | 3 (60) | 8 (57.1) | |||
| Frequency of fish supply, n (%) | 0.009 | 0.251 | 0.943 | ||||||
| 1–2x/day | 8 (14.8) | 2 (6.7) | 4 (11.8) | 1 (5.3) | 5 (11.1) | 5 (12.8) | |||
| 1–3x/week | 43 (79.6) | 19 (63.3) | 28 (82.4) | 14 (73.7) | 33 (73.3) | 29 (74.4) | |||
| 1–3x/month | 3 (5.6) | 9 (30) | 2 (5.9) | 4 (21.1) | 7 (15.6) | 5 (12.8) | |||
| Form of fish supply, n (%) | 0.155 | 0.496 | 0.787 | ||||||
| boiled | 46 (85.2) | 21 (70) | 28 (82.4) | 14 (73.7) | 35 (77.8) | 32 (82.1) | |||
| baked | 8 (14.8) | 9 (30) | 6 (17.6) | 5 (26.3) | 10 (22.2) | 7 (17.9) | |||
| Frequency of tree nuts supply n (%) | >0.05 | >0.05 | >0.05 | ||||||
| 1–2x/day | 2 (22.2) | 0 (0) | 2 (25) | 0 (0) | 2 (25) | 0 (0) | |||
| 1–3x/week | 2 (22.2) | 6 (50) | 2 (25) | 6 (50) | 2 (25) | 6 (46.2) | |||
| 1–3x/month | 5 (55.6) | 6 (50) | 4 (50) | 6 (50) | 4 (50) | 7 (53.8) | |||
| Form of tree nuts supply n (%) | >0.05 | >0.05 | >0.05 | ||||||
| raw | 7 (77.8) | 8 (66.7) | 6 (75) | 8 (66.7) | 6 (75) | 9 (69.2) | |||
| boiled | 2 (22.2) | 0 (0) | 2 (25) | 0 (0) | 2 (25) | 0 (0) | |||
| baked | 0 (0) | 4 (33.3) | 0 (0) | 4 (33.3) | 0 (0) | 4 (30.8) | |||
| Frequency of shellfish supply n (%) | >0.05 | >0.05 | >0.05 | ||||||
| 1–2x/day | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| 1–3x/week | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| 1–3x/month | 2 (100) | 4 (100) | 2 (100) | 4 (100) | 2 (100) | 4 (100) | |||
| Form of shellfish supply n (%) | 1.00 | 1.00 | 1.00 | ||||||
| boiled | 2 (100) | 3 (75) | 2 (100) | 3 (75) | 2 (100) | 3 (75) | |||
| baked | 0 (0) | 1 (25) | 0 (0) | 1 (25) | 0 (0) | 1 (25) |
| Parameter | Model I | Model II | ||
|---|---|---|---|---|
| OR (95%CI) | p | aOR (95%CI) | p | |
| Family history of inhalant allergy yes vs. no | 3.25 (1.3–8.14) | 0.012 | ||
| The occurrence of AD in the family yes vs. no | 5.3 (1.4–19.8) | 0.012 | 17.6 (1.9–159.6) | 0.011 |
| The frequency of egg white supply 1–3x/week vs. 1–2x/day | 0.29 (0.1–0.91) | 0.033 | ||
| Frequency of fish supply 1–3x/month vs. 1–2x/day | 0.08 (0.01–0.63) | 0.016 | ||
| Frequency of supply of gluten-free products 1–3x/week vs. 1–2x/day | 0.34 (0.13–0.9) | 0.03 | ||
| Using ready-made products yes vs. no | 9.49 (3.27–27.59) | <0.001 | 11.5 (2.7–49.7) | 0.001 |
| Variety of diet (number of product groups) | ||||
| 6 months 5–6 vs. 0–4 | 0.22 (0.08–0.62) | 0.004 | 0.17 (0.04–0.71) | 0.015 |
| 6 months ≥7 vs. 0–4 | 0.1 (0.02–0.45) | 0.003 | 0.08 (0.01–0.58) | 0.012 |
| 12 months ≥8 vs. 5–7 | 0.18 (0.07–0.48) | 0.001 | 0.14 (0.03–0.57) | 0.006 |
| Parameter | Model I | Model II | ||
|---|---|---|---|---|
| OR (95%CI) | p | aOR (95%CI) | p | |
| Family history of food allergy yes vs. no | 3.51 (1.1–11.15) | 0.034 | ||
| Family history of inhalant allergy yes vs. no | 6.32 (2.13–18.73) | 0.001 | 5.65 (1.43–22.22) | 0.001 |
| The occurrence of AD in the family yes vs. no | 5.3 (1.4–20.03) | 0.014 | ||
| Exclusive breastfeeding time | 0.81 (0.7–0.95) | 0.009 | 0.82 (0.69–0.99) | 0.008 |
| Time to introduce foods in the form of lumps 7.5 months vs. 8 months | 1.49 (1.02–2.16) | 0.038 | ||
| Time to introduce solid foods 10 months vs. 11 months | 1.33 (1.04–1.71 | 0.025 | ||
| Variety of diet (number of product groups) | ||||
| 6 months 5–6 vs. 0–4 | 0.16 (0.05–0.54) | 0.003 | ||
| 6 months ≥7 vs. 0–4 | 0.06 (0.01–0.42) | 0.005 | 0.16 (0.04–0.67) | 0.003 |
| 12 months ≥8 vs. 5–7 | 0.11 (0.03–0.34) | <0.001 | 0.15 (0.01–1.67) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chęsy, M.; Krogulska, A. Introduction of Complementary Foods and the Risk of Sensitization and Allergy in Children up to Three Years of Age. Nutrients 2023, 15, 2054. https://doi.org/10.3390/nu15092054
Chęsy M, Krogulska A. Introduction of Complementary Foods and the Risk of Sensitization and Allergy in Children up to Three Years of Age. Nutrients. 2023; 15(9):2054. https://doi.org/10.3390/nu15092054
Chicago/Turabian StyleChęsy, Magdalena, and Aneta Krogulska. 2023. "Introduction of Complementary Foods and the Risk of Sensitization and Allergy in Children up to Three Years of Age" Nutrients 15, no. 9: 2054. https://doi.org/10.3390/nu15092054