Abstract
Maternal dietary factors have been suggested as possible contributing influences for congenital anomalies (CAs). We aimed to assess the association between vitamin D supplementation or vitamin D status (s-25OHD) during pregnancy and CAs in the offspring. A comprehensive literature search was conducted in the three electronic databases: PubMed, Embase, and Cochrane Library. Included studies were critically appraised using appropriate tools (risk of bias 2, ROBINS-I). A protocol was registered in the International Prospective Register of Systematic Reviews (CRD42019127131). A meta-analysis of four randomised controlled trials (RCTs) including 3931 participants showed no effect of vitamin D supplementation on CAs, a relative risk of 0.76 (95% CI 0.45; 1.30), with moderate certainty in the effect estimates by GRADE assessment. Of the nine identified observational studies, six were excluded due to a critical risk of bias in accordance with ROBINS-I. Among the included observational studies, two studies found no association, whereas one case-control study identified an association between s-25OHD < 20 nmol/L and neural tube defects, with an adjusted odds ratio of 2.34 (95% CI: 1.07; 5.07). Interpretation of the results should be cautious given the low prevalence of CAs, RCTs with onset of supplementation after organogenesis, and low-quality observational studies.
1. Introduction
Structural congenital anomalies (CAs) occur during intrauterine life, may present in different organ systems, and vary in complexity. Globally, an estimated 6% of infants are born with CAs, and the most common forms of CAs are congenital heart disease (CHD) or neural tube defects (NTDs) [1,2]. CAs are a major cause of infant morbidity and long-term disability and are a leading cause of infant mortality globally. Known causes include gene defects and chromosomal abnormalities, including trisomy 13 and 18. Still, many CAs occur without a known cause [2]. Several environmental and potentially modifiable factors have been suggested as potential risk factors for CAs, including maternal illnesses, drugs, pollution, and maternal malnutrition [1]. For instance, a case-control study from 2016 found a reduced occurrence of selected CHDs in the offspring with increased maternal diet quality [3]. Early folic acid supplementation has specifically been shown to protect against NTDs and thus is advised to women planning pregnancy [4]. Additionally, a Dutch case-control study from 2018 found that a compromised maternal vitamin D status (serum 25-hydroxyvitamin D; s-25OHD) was associated with a higher prevalence of CHD in offspring [5]. However, this study used post-pregnancy s-25OHD concentrations as a proxy for exposure during early pregnancy [5]. s-25OHD is the primary circulating form of vitamin D and is used to determine vitamin D status. The s-25OHD concentrations do not differ between pregnant and non-pregnant women, whereas the active form of vitamin D (1,25(OH)2D) increases substantially in pregnancy [6]. During pregnancy, the supply of vitamin D in the foetus completely depends on maternal concentrations of vitamin D, and concentrations in the neonate, cord, and mother are closely correlated [7,8].
A critical window for intervention in relation to the prevention of CAs might be in early pregnancy when the foetal organ systems start developing [9]. The objective of the present systematic review and meta-analysis was to synthesise and critically appraise the literature for studies that examined the association between exposure to vitamin D status during pregnancy and the risk of CAs in the offspring.
2. Methods
Before conducting the present systematic review, we developed a protocol based on Preferred Reporting Items for Systematic Review and Meta-analysis Protocols (PRISMA-P) [10], which we registered at the International Prospective Register of Systematic Reviews (PROSPERO) (registration number: CRD42019127131, 14 May 2019). The present systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [11].
2.1. Alterations to Protocol
Quality assessment of randomised controlled trials (RCTs) was performed using Cochrane Risk of Bias 2 (RoB 2) [12] and not Cochrane Risk of Bias (RoB) [13] as stated in the protocol. We found the updated tool the better choice.
2.2. Eligibility Criteria
Studies in English on the association between vitamin D exposure during foetal life and the development of CAs in offspring were eligible for inclusion. The eligibility criteria were structured as Population, Intervention (exposure), Comparison, and Outcome (PICO). The population of interest was healthy pregnant women without any disease prior to pregnancy (e.g., diabetes mellitus) or any diseases developed in pregnancy (e.g., gestational diabetes, pre-eclampsia). Premature offspring or offspring with chromosomal abnormalities were excluded as we expected these to have a different aetiology. The exposure of interest was measured maternal vitamin D status (s-25OHD) in the blood/serum of the mother, cord, or offspring in the period leading up to pregnancy, during pregnancy, or shortly following birth, or exposure to vitamin D via supplementation in a randomised controlled setting. The outcome of interest was CAs in the offspring, including anomalies of the nervous system, circulatory system, respiratory system, digestive system, genital organs, urinary system, and musculoskeletal system, as well as malformations of the eye, ear, face and neck, cleft lip, and cleft palate.
2.3. Information Sources
PubMed, Embase, and Cochrane Library were searched for relevant studies. The comprehensive literature search was performed in August 2019 (with no restriction on date) and again on 15 June 2020 (dates restricted to 2019–2020).
2.4. Search
Search terms were identified by the authors of the present systematic review for the aspects of “fetal life” and “vitamin D”. All search terms were entered as free text as well as Medical Subject Headings (MeSH terms). The electronic search was limited to studies on humans by applying the filter “human” in the electronic databases. The search strategy was conducted by KCW after guidance from a librarian specialised in literature searches and was cross-checked by MNH (Table S1)
2.5. Study Selection
All identified studies were exported to Endnote and subsequently imported to the software programme Covidence, and duplicates were removed. The selection process was managed in the Covidence software by three reviewers (MNH, FT, and KCW). Initially, studies were assessed for inclusion based on title and abstract by independent votes of two reviewers. At this stage, studies were included based on relevant population and intervention, i.e., healthy pregnant women including their offspring and measured vitamin D or vitamin D supplementation in an RCT setting. Subsequently, full texts were retrieved, and studies were screened and included based on the outcome of independent votes of two reviewers. Disagreements during the selection process were resolved by discussion among the three reviewers (MNH, FT, and KCW).
2.6. Data Collection
One author extracted relevant data from the included studies (KCW), and the extracted data were double-checked by either MNH or FT. The journal article, Supplementary Materials provided in the journal article, trial protocol/registration, and personal communication with study authors were used as sources to inform data extraction. We emailed the corresponding author of potentially relevant studies for clarification or to resolve other uncertainties. The deadline for a reply from the study authors was kept open during the conduction of the review.
2.7. Data Items
Relevant study data included the following: study author, country, year of publication, study design, size of the study population, source of the study population (in- and exclusion criteria), baseline characteristics, assessment of exposure, trimester of exposure (if specified), confounding factors considered, outcomes and method of assessment, analysis methods, and key results, as well as reported conflicts of interest and trial registration.
2.8. Summary Measures and Synthesis of Results
Results of the included RCTs were synthesised in a meta-analysis with random effect inverse variance analyses to generate pooled effect estimates expressed as relative risk and corresponding 95% confidence interval (CI). Heterogeneity was quantified using I2 statistics, with an I2 value greater than 50% considered as substantial heterogeneity.
Additional planned analyses, i.e., funnel plots, dose-response analyses, subgroup analysis by risk of bias, and types of anomalies, were deemed inappropriate due to a lack of studies.
All Analyses Were Performed in Revman Version 5.4 (Cochrane, London, UK). A meta-analysis of observational studies was planned but deemed limited due to the unavailability of eligible studies. Therefore, a narrative synthesis was conducted. In accordance with the guideline in the Risk of Bias In Non-Randomised Studies of Intervention (ROBINS-I) tool [14], we excluded studies that were assessed to have a critical risk of bias from the synthesis.
2.9. Certainty Assessment (GRADE)
Certainty assessments in the effect estimates were evaluated using the Grading Recommendations Assessment, Development, and Evaluation (GRADE) method, with the four possible quality ratings: high, moderate, low, and very low. Downgrading was performed using the standard definition of risk of bias, inconsistency, indirectness, imprecision, and publication bias. The overall certainty in the evidence was based on the lowest quality of the primary outcome.
2.10. Risk of Bias in Individual Studies
Risk of bias was assessed by two reviewers independently (MHN and KCW) by applying the Cochrane Risk of Bias 2 (RoB 2) tool [15] and the ROBINS-I tool [14] in RCTs and observational studies, respectively. Discrepancies were resolved through discussion. According to ROBINS-I [14], confounder domains and co-interventions should be specified at the protocol stage. Confounders were found by constructing and analysing a directed acyclic graph, including maternal age, body mass index (BMI), smoking, socio-economic status, ethnicity, parity, and alcohol consumption. Possible co-interventions that individuals might receive after the initiation of the exposure if interest could be multivitamin use or counselling from a trained dietician. This may be initiated if inadequate vitamin D status is detected during pregnancy.
3. Results
The comprehensive literature search yielded a vast number of unique records (18,938 records). After the removal of duplicates, all records were screened by title and abstract, resulting in 2338 records that were retrieved and assessed in full. The full-text assessment led to the exclusion of 2325 records, and a total of 13 studies were included in the review (Figure 1). Detailed reasons for the exclusion of the 2325 studies can be presented upon request. The complete search strategy can be seen in Table S1.
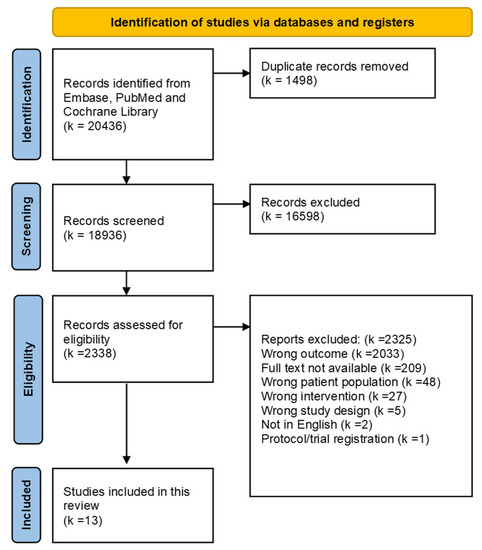
Figure 1.
Flow chart.
3.1. Study Characteristics
Four RCTs [16,17,18,19] and nine observational studies [20,21,22,23,24,25,26,27,28] were included in the review. The RCTs were published between 2016 and 2018 and originated from the USA [18], Canada [19], the UK [17], and Denmark [16], and varied in study population size from 623 to 1298 included pregnant women. The intervention was supplementation with vitamin D ranging from a daily supplement of 800 IU to weekly supplements of 28,000 IU. The primary outcomes of the four included RCTs were persistent wheeze, bone health, asthma and recurrent wheeze, and infant growth. Roth et al., included congenital malformations as an outcome [19], while the remaining three RCTs included congenital malformations as a safety measure [16,17,18].
The observational studies were published between 2014 and 2018. Five of the nine studies were conducted in Turkey [22,24,25,26,28]. The remaining studies were from Spain [20], Egypt [27], Tunisia [23], and China [21] and varied from small case-control studies of 60 participants to cohort studies of 1953 participants. Vitamin D status (s-25OHD) was assessed in maternal blood during gestational weeks 11–25, except for one study that assessed vitamin D status in mothers and offspring shortly after birth [26]. One study did not specify when vitamin D status (s-25OHD) was assessed [27]. The primary outcome of the observational studies were malformations, NTDs, CHD, and congenital diaphragmatic hernia (see Table 1, Table 2 and Table S2).

Table 1.
Characteristics of included RCTs.
Table 2.
Characteristics of included observational studies.
3.2. Risk of Bias within Studies
Risk of bias was assessed for all included studies and presented separately for RCTs and observational studies (see Figure S1a,b).
The four included RCTs were all assessed to be at some concern of bias. The judgement was driven by domain 5, “Bias in selection of the reported result”, according to which, all studies were judged as having some concerns due to missing a pre-specified analysis plan. Chawes et al., 2016 [16] and Litonjua et al., 2016 [18] both had missing information concerning allocation sequence concealment and were judged to be at some concerns of risk of bias in domain 1, “Bias arising from the randomisation process”. See Figure S1a.
All nine observational studies were assessed to have a serious or critical risk of bias, with the most problematic domain in ROBINS-I being domain 1 “Bias due to confounding”. Six observational studies did not adjust analyses for any confounders and were subsequently excluded from the synthesis in accordance with guidelines from ROBINS-I [14]. Three observational studies adjusted for some confounders and were rated at serious risk of bias [21,23,26]. See Figure S1b.
3.3. Vitamin D and Congenital Anomalies
The meta-analysis of the four RCTs (n = 3931) that reported on CAs showed no difference in the risk of CAs between vitamin D supplementation and placebo (RR: 0.76, 95% CI: 0.45, 1.30) (Figure 2). There was substantial heterogeneity (I2 = 54%, p = 0.09), and a sensitivity analysis showed that by removing the study by Roth et al., 2018 [19], the heterogeneity was reduced to I2 = 0%. The certainty of the effect estimates was moderate due to imprecision (wide confidence intervals). We did not assess risk of publication bias due to the low number of included studies. We found discrepancies in the reporting of CAs in the Supplementary Materials and the clinical trial’s registration in the study by Litonjua et al., 2016 [18]. We extracted the data from the peer-reviewed Supplementary Materials. This did not substantially affect the overall effect estimate of the meta-analysis.
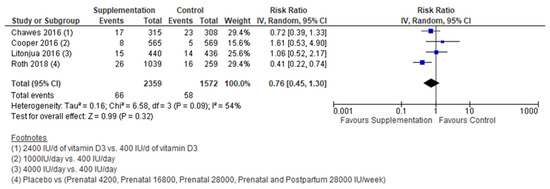
Figure 2.
Meta-analysis of RCTs [16,17,18,19].
The three included observational studies investigated the association between vitamin D status and CHD, congenital malformations, and NTD, respectively [21,23,26] (see Table 3). Further, the studies differed in terms of the timing of s-25OHD assessment, from 11–25 weeks of gestation, shortly after birth or not reported, and the selection of confounding factors. Only one study found a significant association; Nasri et al., 2016 [23] found decreased concentrations of vitamin D to be associated with an increased risk of neural tube defects, with an adjusted odds ratio of 2.34 95% CI (1.07; 5.07) and a p-value 0.035. Of note, the cases and controls were matched by folate supplementation in the study.
Table 3.
Key findings of the observational studies (excluding the studies rated as having critical risk of bias, as recommended by ROBINS-I).
We did not conduct a GRADE assessment for the observational studies as we were not able to pool the estimates.
4. Discussion
4.1. Summary of the Evidence
Maternal nutrition and supplement use during pregnancy are important for foetal development, and certain nutrients have been linked to the development of CAs, i.e., folic acid, for the prevention of NTDs [29]. This systematic review showed that, with overall moderate certainty in our findings, supplementation with vitamin D up to 4000 IU/day during pregnancy was not associated with differences in the occurrence of CA, though the RR in the meta-analysis pointed towards being in favour of supplementation. Although there were some variations in baseline characteristics, vitamin D dose, intervention duration, and outcome definition of the included RCTs, the evidence from the systematic review and meta-analysis was based on well-conducted and methodologically strong RCTs. A caveat to our results is that the included RCTs were not designed to answer our research question, and CAs were included in most of the RCTs as safety measures. CAs are rare events, particularly when considering the individual types of anomalies, and our meta-analysis may be underpowered. Further, the inclusion of participants in the RCTs was after the first trimester and, thereby, after the initial organ formation and what we consider to be the critical window of exposure. Due to limitations imposed by the scientific ethical committee, Cooper et al., 2016 only included women with concentrations of vitamin D between 25 and 100 nmol/L and thereby excluded women with low concentrations of vitamin D [17]. This may have prevented any beneficial effect materialising due to sufficient concentrations of vitamin D already at baseline for all participants [30]. In fact, secondary analyses completed by Litonjua and colleagues revealed that initial concentrations of vitamin D among the participants affected the overall effect of the intervention [31].
The null results on vitamin D supplementation during pregnancy on offspring risk of CAs were also reported by previous reviews by Bi et al., 2018 and by Liu et al., 2022 [32,33]. Bi et al., 2018 did not include results from Roth et al., 2018 [19]. Neither of the two systematic reviews included observational studies, nor were CAs the primary objective of the reviews [32,33].
One of the included observational studies showed that vitamin D deficiency (<30 nmol/L) in the mother was associated with an increased risk of NTD in the foetus [23]. A similar result was found in two other observational studies that examined NTDs as an outcome; however, they are here excluded due to critical risk of bias [22,28]. Sources of vitamin D, e.g., fatty fish, are part of a healthy diet, and maternal vitamin D status may also be considered an indicator of the general nutritional status of the mother during pregnancy. Possible interactions between nutrients, e.g., folic acid and vitamin D, may be hypothesised and should be tested for in future studies.
Regarding other CAs, two of the included observational studies showed no association between s-25OHD and CHD and malformations, respectively [21,26]. This is in accordance with findings from two studies with malformations as the outcome that we excluded due to their critical risk of bias in accordance with the ROBINS-I [20,24]. In contrast, the excluded study with a critical risk of bias by Mokhtar et al., 2018 showed that maternal vitamin D deficiency (s-25OHD < 25 nmol/L) was associated with an increased risk of CHD in offspring [27].
Another study we excluded due to a critical risk of bias found that maternal serum vitamin D was significantly lower in pregnancies complicated by congenital diaphragmatic hernias than in healthy pregnancies [25]. The lack of appropriate confounder control invalidates the trust in the associations found in the excluded studies.
4.2. Strengths and Limitations of the Included Studies
The four included RCTs had sufficient quality to be included, together reaching a total participant number of 3931. By GRADE assessment, the certainty reached a moderate level given the wide confidence intervals. None of the RCTs had CAs as their primary endpoint, which is probably related to the low prevalence of CAs, making a single RCT on CA as a primary outcome non-feasible. The onset of the intervention varied between gestation weeks 11 and 25, i.e., the second trimester of pregnancy, which is after the critical period of organ formation early in pregnancy [16,17,18,19]. Only one RCT excluded known foetal anomalies before randomisation [18].
Reporting adverse events may be performed very differently across studies [34]. This has implications for the validity of the current review, as we cannot be sure that all CAs were identified. Further, the method of detection may vary and introduce heterogeneity between the RCTs. CAs were an a priori safety measure; however, the method of measurement of CAs was not stated, which gives rise to concerns about underreporting of less obvious CAs. Based on these limitations, we are careful to make conclusions about the association between vitamin D and CAs from the current level I (RCT) evidence.
The three included observational studies were at serious risk of bias, primarily due to incomplete confounder control but also due to the selection of participants, e.g., two of the studies restricted the inclusion of pregnant women to those giving live births and measurement of vitamin D status was performed at different time points and with different methods of detection. Nasri et al., 2016 included pregnant women before elective termination [23]. Furthermore, the case-control match by folate supplementation was not specified in detail which could call into question the quality of matching of this important nutrient regarding NTD.
4.3. Strengths and Limitations of the Review
The comprehensive literature search is a strength of the present systematic review. We searched for and included studies in which the aim was to assess the association between vitamin D status during pregnancy and CA in the offspring and those that examined vitamin D supplementation during pregnancy and other outcomes with CAs as a safety measure or secondary outcome. We successfully captured both the former and the latter.
Publications based on the same study population were only included with one publication. One study did not report CA as an outcome; however, it stated that one child died with a CA. We were not able to obtain contact with the author to clarify if CAs were included as an outcome and thereby routinely reported for all study subjects or only for deaths [35]. This study was not included in the present systematic review. RCTs without any CAs may not have reported their findings and thus were not included in the present systematic review.
CA is a composite outcome covering potentially very different conditions, and a limitation of this review is the lack of possibility to conduct subgroup analyses on types of anomalies, severity, or dose–response relationships. We were furthermore not able to perform meta-regressions or subgroup analyses to test the cause of the substantial heterogeneity due to the scarcity of studies. Heterogeneity was most likely due to differences in populations, interventions, comparisons, and outcomes.
5. Conclusions
This review provides an overview of the results from the available literature on vitamin D status and CAs, and the results from the meta-analysis of RCTs suggested no association between vitamin D and CAs, with moderate certainty in our findings. However, few and small studies prevented us from providing a firm conclusion on the association. Unlike for many other and more frequent outcomes, the most feasible study design to investigate the present research question is the observational study design due to the low prevalence of CAs and the recruitment of participants, as well as that the initiation of supplementation often takes place after organogenesis. However, most current observational studies lacked sufficient control of confounders.
Future studies in this area should consider including pregnancies before termination of pregnancy to avoid selection bias, and optimally, women of reproductive age should be included prior to pregnancy. Additionally, future studies should be of sufficient size and include relevant confounders.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu15092125/s1, Table S1: Search terms and strategy; Table S2: Study identification; Figure S1: (a) Risk of bias assessment of included RCTs according to Cochranes Risk of Bias tool 2; (b) Risk of bias assessment of included observational studies according to ROBINS-I.
Author Contributions
Conceptualization: all authors. Methodology: K.C.W., F.T. and M.N.H. Writing the original draft: K.C.W. Critically reviewing and editing: all authors. All authors have read and agreed to the published version of the manuscript.
Funding
The Danish Children’s Heart Foundation (18-R110-A5181-26045) supported the project. The Parker Institute, Bispebjerg and Frederiksberg Hospital is supported by a core grant from the Oak Foundation (OCAY-18-774-OFIL).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are openly available in the respective studies included in the systematic review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. Congenital Anomalies. Available online: https://www.who.int/health-topics/congenital-anomalies#tab=tab_1 (accessed on 16 February 2022).
- Sarmah, S.; Muralidharan, P.; Marrs, J.A. Common congenital anomalies: Environmental causes and prevention with folic acid containing multivitamins. Birth Defects Res. C Embryo Today 2016, 108, 274–286. [Google Scholar] [CrossRef] [PubMed]
- Botto, L.D.; Krikov, S.; Carmichae, S.L.; Munger, R.G.; Shaw, G.M.; Feldkamp, M.L. Lower rate of selected congenital heart defects with better maternal diet quality: A population-based study. Arch. Dis. Child Fetal Neonatal Ed. 2016, 101, F43–F49. [Google Scholar] [CrossRef] [PubMed]
- Imbard, A.; Benoist, J.F.; Blom, H.J. Neural Tube Defects, Folic Acid and Methylation. Int. J. Environ. Res. Public Health 2013, 10, 4352. [Google Scholar] [CrossRef] [PubMed]
- Koster, M.P.H.; van Duijn, L.; Krul-Poel, Y.H.M.; Laven, J.S.; Helbing, W.A.; Simsek, S.; Steegers-Theunissen, R.P.M. A compromised maternal vitamin D status is associated with congenital heart defects in offspring. Early Hum. Dev. 2018, 117, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Wagner, C.L.; Castracane, V.D. Understanding vitamin D metabolism in pregnancy: From physiology to pathophysiology and clinical outcomes. Metabolism 2018, 86, 112–123. [Google Scholar] [CrossRef]
- Rabbani, S.; Afaq, S.; Fazid, S.; Khattak, M.I.; Yousafzai, Y.M.; Habib, S.H.; Lowe, N.; Ul-Haq, Z. Correlation between maternal and neonatal blood Vitamin D level: Study from Pakistan. Matern. Child Nutr. 2021, 17, e13028. [Google Scholar] [CrossRef]
- VioStreym, S.; Kristine Moller, U.; Rejnmark, L.; Heickendorff, L.; Mosekilde, L.; Vestergaard, P. Maternal and infant vitamin D status during the first 9 months of infant life-a cohort study. Eur. J. Clin. Nutr. 2013, 67, 1022–1028. [Google Scholar] [CrossRef]
- Donovan, M.F.; Cascella, M. Embryology, Weeks 6–8. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2021; Bookshelf ID: NBK563181. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Risk of Bias Tools-Current Version of RoB 2. Available online: https://sites.google.com/site/riskofbiastool/welcome/rob-2-0-tool/current-version-of-rob-2 (accessed on 29 April 2022).
- Chawes, B.L.; Bønnelykke, K.; Stokholm, J.; Vissing, N.H.; Bjarnadóttir, E.; Schoos, A.-M.M.; Wolsk, H.M.; Pedersen, T.M.; Vinding, R.K.; Thorsteinsdóttir, S.; et al. Effect of Vitamin D 3 Supplementation During Pregnancy on Risk of Persistent Wheeze in the Offspring A Randomized Clinical Trial. JAMA 2016, 315, 353–361. [Google Scholar] [CrossRef]
- Cooper, C.; Harvey, N.C.; Bishop, N.J.; Kennedy, S.; Papageorghiou, A.T.; Schoenmakers, I.; Fraser, R.; Gandhi, S.V.; Carr, A.; D’Angelo, S.; et al. Maternal gestational vitamin D supplementation and off spring bone health (MAVIDOS): A multicentre, double-blind, randomised placebo-controlled trial. Lancet Diabetes Endocrinol. 2016, 4, 393–402. [Google Scholar] [CrossRef]
- Litonjua, A.A.; Carey, V.J.; Laranjo, N.; Harshfield, B.J.; Mcelrath, T.F.; O’Connor, G.T.; Sandel, M.; Iverson, R.E., Jr.; Lee-Paritz, A.; Strunk, R.C.; et al. Effect of Prenatal Supplementation with Vitamin D on Asthma or Recurrent Wheezing in Offspring by Age 3 Years The VDAART Randomized Clinical Trial. JAMA 2016, 315, 362–370. [Google Scholar] [CrossRef]
- Roth, D.E.; Morris, S.K.; Zlotkin, S.; Gernand, A.D.; Ahmed, T.; Shanta, S.S.; Papp, E.; Korsiak, J.; Shi, J.; Islam, M.M.; et al. Vitamin D Supplementation in Pregnancy and Lactation and Infant Growth. N. Engl. J. Med. 2018, 379, 1174–1177. [Google Scholar] [CrossRef]
- Fernández-Alonso, A.M.; Dionis-Sánchez, E.C.; Chedraui, P.; González-Salmerón, M.D.; Pérez-López, F.R. First-trimester maternal serum 25-hydroxyvitamin D3 status and pregnancy outcome. Int. J. Gynecol. Obstet. 2012, 116, 6–9. [Google Scholar] [CrossRef]
- Zhou, J.; Su, L.; Liu, M.; Liu, Y.; Cao, X.; Wang, Z.; Xiao, H. Associations between 25-hydroxyvitamin D levels and pregnancy outcomes: A prospective observational study in southern China. Eur. J. Clin. Nutr. 2014, 68, 925–930. [Google Scholar] [CrossRef]
- Daglar, K.; Tokmak, A.; Kirbas, A.; Guzel, A.I.; Erkenekli, K.; Yucel, A.; Uygur, D. Maternal serum vitamin D levels in pregnancies complicated by neural tube defects. J. Matern. Fetal Neonatal Med. 2016, 29, 298–302. [Google Scholar] [CrossRef]
- Nasri, K.; Ben Fradj, M.K.; Feki, M.; Kaabechi, N.; Sahraoui, M.; Masmoudi, A.; Marrakchi, R.; Gaigi, S.S. Maternal 25-hydroxyvitamin D level and the occurrence of neural tube defects in Tunisia. Int. J. Gynecol. Obstet. 2016, 134, 131–134. [Google Scholar] [CrossRef]
- Ates, S.; Sevket, O.; Ozcan, P.; Ozkal, F.; Kaya, M.O.; Dane, B. Vitamin D status in the first-trimester: Effects of Vitamin D deficiency on pregnancy outcomes. Afr. Health Sci. 2016, 16, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Turkmen, G.G.; Timur, H.; Tokmak, A.; Yilmaz, Z.; Kirbas, A.; Daglar, K.; Sanhal, C.Y.; Uygur, D. Levels of serum vitamin D and calcium in pregnancies complicated with fetal congenital diaphragmatic hernia and normal pregnancies. J. Matern. Fetal Neonatal Med. 2017, 30, 990–994. [Google Scholar] [CrossRef] [PubMed]
- Dilli, D.; Doğan, N.N.; Örün, U.A.; Koç, M.; Zenciroğlu, A.; Karademir, S.; Akduman, H. Maternal and neonatal micronutrient levels in newborns with CHD. Cardiol. Young 2018, 28, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Mokhtar, W.A.; Fawzy, A.; Allam, R.M.; Amer, R.M.; Hamed, M.S. Maternal vitamin D level and vitamin D receptor gene polymorphism as a risk factor for congenital heart diseases in offspring; An Egyptian case-control study. Genes Dis. 2018, 6, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Sirinoglu, H.A.; Pakay, K.; Aksoy, M.; Turan Bakırci, I.; Ozkaya, E.; Sanverdi, I. Comparison of serum folate, 25-OH vitamin D, and calcium levels between pregnants with and without fetal anomaly of neural tube origin. J. Matern. Fetal Neonatal Med. 2018, 31, 1490–1493. [Google Scholar] [CrossRef] [PubMed]
- Wald, N.; Sneddon, J.; Densem, J.; Frost, C.; Stone, R. Prevention of neural tube defects: Results of the Medical Research Council Vitamin Study. Lancet 1991, 338, 131–137. [Google Scholar] [CrossRef]
- Giustina, A.; Bouillon, R.; Binkley, N.; Sempos, C.; Adler, R.A.; Bollerslev, J.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Heijboer, A.; et al. Controversies in Vitamin D: A Statement from the Third International Conference. JBMR Plus 2020, 4, e10417. [Google Scholar] [CrossRef]
- Wolsk, H.M.; Harshfield, B.J.; Laranjo, N.; Carey, V.J.; O’Connor, G.; Sandel, M.; Strunk, R.C.; Bacharier, L.B.; Zeiger, R.S.; Schatz, M.; et al. Vitamin D supplementation in pregnancy, prenatal 25(OH)D levels, race, and subsequent asthma or recurrent wheeze in offspring: Secondary analyses from the Vitamin D Antenatal Asthma Reduction Trial. J. Allergy Clin. Immunol. 2017, 140, 1423–1429.e5. [Google Scholar] [CrossRef]
- Bi, W.G.; Nuyt, A.M.; Weiler, H.; Leduc, L.; Santamaria, C.; Wei, S.Q. Association between Vitamin D Supplementation during Pregnancy and Offspring Growth, Morbidity, and Mortality: A Systematic Review and Meta-analysis. JAMA Pediatr. 2018, 172, 635–645. [Google Scholar] [CrossRef]
- Liu, Y.; Ding, C.; Xu, R.; Wang, K.; Zhang, D.; Pang, W.; Tu, W.; Chen, Y. Effects of vitamin D supplementation during pregnancy on offspring health at birth: A meta-analysis of randomized controlled trails. Clin. Nutr. 2022, 41, 1532–1540. [Google Scholar] [CrossRef]
- Peryer, G.; Golder, S.; Junqueira, D.R.; Vohra, S.; Loke, Y.K. Chapter 19: Adverse effects | Cochrane Training. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Version 6.3; Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 20 April 2022).
- Goldring, S.T.; Griffiths, C.J.; Martineau, A.R.; Robinson, S.; Yu, C.; Poulton, S.; Kirkby, J.C.; Stocks, J.; Hooper, R.; Shaheen, S.O.; et al. Prenatal Vitamin D Supplementation and Child Respiratory Health: A Randomised Controlled Trial. PLoS ONE 2013, 8, e66627. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).