

Post-Transplant Diabetes Mellitus in Kidney-Transplanted Patients: Related Factors and Impact on Long-Term Outcome
 , , , , ,
, , , , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
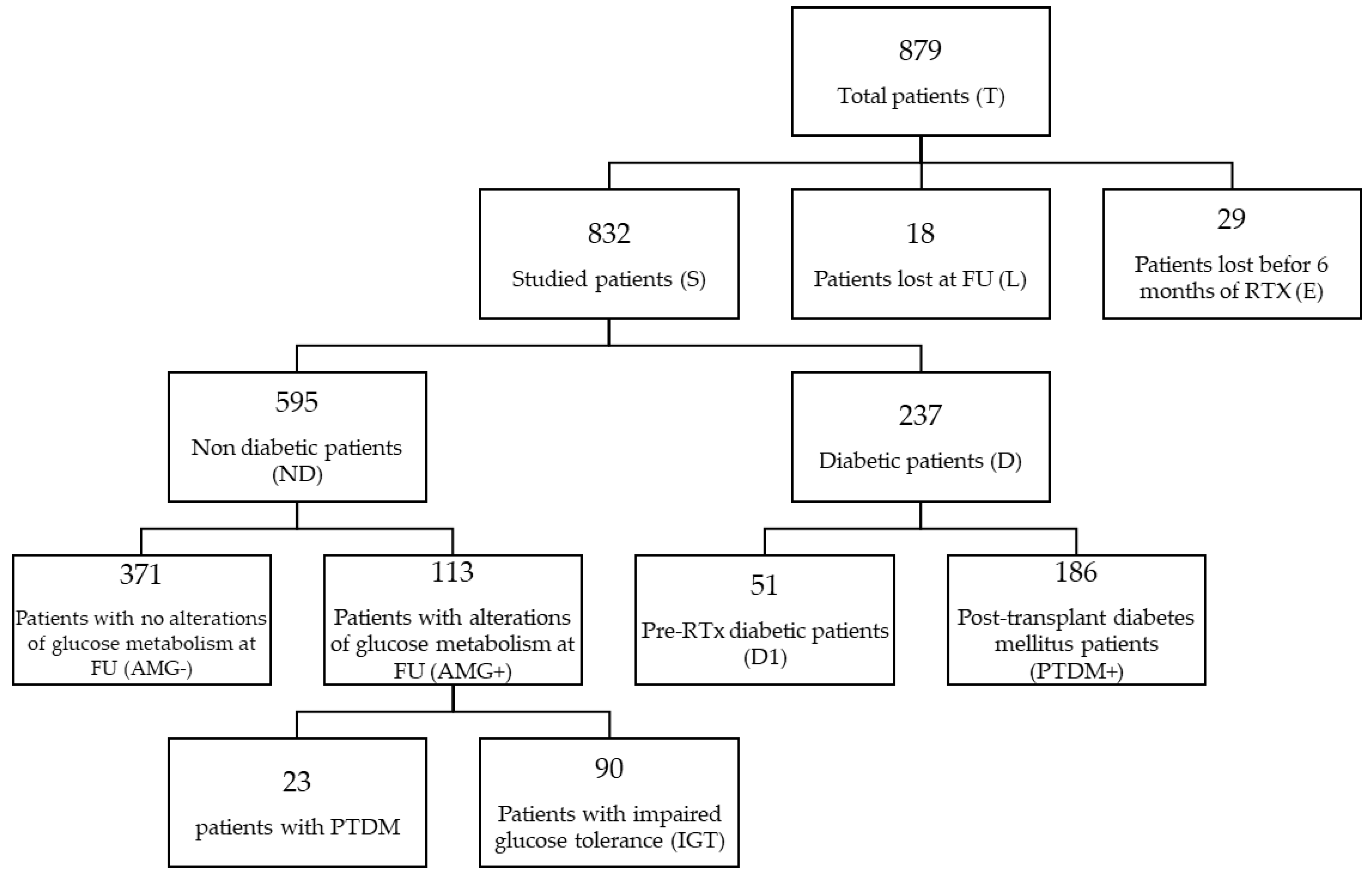
2.1. Study Design
- -
- Collection of pathological and pharmacological history and complete physical examination, at the time of inclusion in the study (T1);
- -
- Detection of clinical and biochemical parameters at 1, 6, and 12 months (T1, T6, and T12, respectively) after transplantation;
- -
- Specific biochemical determinations of glucose metabolism (glycemia, glycated hemoglobin, and insulin) and concerning mineral metabolism, in particular parathyroid hormone (PTH), calcium (Ca), phosphorus (P), and native and active vitamin D levels (25OH and 1-25OH) at T1, T6, and T12;
- -
- The collection of data concerning induction and maintenance of immunosuppressive therapy (at T1 and T12) and antihypertensive, antidiabetic, lipid, and vitamin D treatments, as well as the calculation of cumulative doses of steroid therapy at T1, T6, and T12;
2.2. Measurements and Definitions
- -
- Normoglycemic patients (AMG−);
- -
- Patients with alterations in glucose metabolism (AMG+):
- -
- IFG (Impaired Fasting Glucose): fasting blood glucose between 100 and 125 mg/dL;
- -
- IGT (Impaired Glucose Tolerance): blood glucose between 140 and 199 mg/dL at 120′ from the load;
- -
- A novel diagnosis of diabetes: blood glucose after loading >200 mg/dL.
2.3. Follow-Up
2.4. Statistical Analyses
3. Results
3.1. Characteristics of the Cohort Studied and Comparison between Groups
3.2. Comparison between D and ND Patients
3.3. Comparison between PTDM and ND Patients
3.4. OGTT Analysis: Comparison between AMG+ and AMG−
3.5. Differences in Glucose Metabolism Parameters among the Groups
3.6. Impact of Glucose Metabolism Alterations on Long-Term Clinical Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shivaswamy, V.; Boerner, B.; Larsen, J. Post-Transplant Diabetes Mellitus: Causes, Treatment, and Impact on Outcomes. Endocr Rev. 2016, 37, 37–61. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cosio, F.G.; Kudva, Y.; van der Velde, M.; Larson, T.S.; Textor, S.C.; Griffin, M.D.; Stegall, M.D. New onset hyperglycemia and diabetes are associated with increased cardiovascular risk after kidney transplantation. Kidney Int. 2005, 67, 2415–2421. [Google Scholar] [CrossRef] [PubMed]
- Aleid, H.; Alhuraiji, A.; Alqaraawi, A.; Abdulbaki, A.; Altalhi, M.; Shoukri, M.; Abdelmoneim, E.; Ali, T. New-onset diabetes after kidney transplantation: Incidence, risk factors, and outcomes. Saudi J. Kidney Dis. Transpl. 2016, 27, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Sharif, A.; Hecking, M.; de Vries, A.P.; Porrini, E.; Hornum, M.; Rasoul-Rockenschaub, S.; Berlakovich, G.; Krebs, M.; Kautzky-Willer, A.; Schernthaner, G.; et al. Proceedings from an international consensus meeting on posttransplantation diabetes mellitus: Recommendations and future directions. Am. J. Transplant. 2014, 14, 1992–2000. [Google Scholar] [CrossRef] [PubMed]
- Du, Q.; Li, T.; Yi, X.; Song, S.; Kang, J.; Jiang, Y. Prevalence of new-onset diabetes mellitus after kidney transplantation: A systematic review and meta-analysis. Acta Diabetol. 2024. [Google Scholar] [CrossRef] [PubMed]
- Chakkera, H.A.; Weil, E.J.; Castro, J.; Heilman, R.L.; Reddy, K.S.; Mazur, M.J.; Hamawi, K.; Mulligan, D.C.; Moss, A.A.; Mekeel, K.L.; et al. Hyperglycemia during the immediate period after kidney transplantation. Clin. J. Am. Soc. Nephrol. 2009, 4, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Jenssen, T.; Hartmann, A. Post-transplant diabetes mellitus in patients with solid organ transplants. Nat. Rev. Endocrinol. 2019, 15, 172–188. [Google Scholar] [CrossRef] [PubMed]
- Alfieri, C.; Favi, E.; Campioli, E.; Cicero, E.; Molinari, P.; Campise, M.; Gandolfo, M.T.; Regalia, A.; Cresseri, D.; Messa, P.; et al. Prevalence and Risk Factors of Abnormal Glucose Metabolism and New-Onset Diabetes Mellitus after Kidney Transplantation: A Single-Center Retrospective Observational Cohort Study. Medicina 2022, 58, 1608. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44 (Suppl. 1), S1–S232. [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F.; Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Lentine, K.L.; Smith, J.M.; Hart, A.; Miller, J.; Skeans, M.A.; Larkin, L.; Robinson, A.; Gauntt, K.; Israni, A.K.; Hirose, R.; et al. OPTN/SRTR 2020 Annual Data Report: Kidney. Am. J. Transplant. 2022, 22 (Suppl. 2), 21–136. [Google Scholar] [CrossRef] [PubMed]
- Malik, R.F.; Jia, Y.; Mansour, S.G.; Reese, P.P.; Hall, I.E.; Alasfar, S.; Doshi, M.D.; Akalin, E.; Bromberg, J.S.; Harhay, M.N.; et al. Post-transplant Diabetes Mellitus in Kidney Transplant Recipients: A Multicenter Study. Kidney360 2021, 2, 1296–1307. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, J.; Xu, L.; Wei, X.; Li, X.; Cai, M. Incidence and Risk Factors of Posttransplantation Diabetes Mellitus in Living Donor Kidney Transplantation: A Single-Center Retrospective Study in China. Transplant. Proc. 2018, 50, 3381–3385. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.; Grden, A.; Skare, T.; Jaworski, P.; Nisihara, R. Risk factors for new-onset diabetes mellitus after kidney transplantation (NODAT): A Brazilian single center study. Arch. Endocrinol. Metab. 2018, 62, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Paek, J.H.; Kang, S.S.; Park, W.Y.; Jin, K.; Park, S.B.; Han, S.; Kim, C.D.; Ro, H.; Lee, S.; Jung, C.W.; et al. Incidence of Post-transplantation Diabetes Mellitus Within 1 Year After Kidney Transplantation and Related Factors in Korean Cohort Study. Transplant. Proc. 2019, 51, 2714–2717. [Google Scholar] [CrossRef] [PubMed]
- Cosio, F.G.; Pesavento, T.E.; Kim, S.; Osei, K.; Henry, M.; Ferguson, R.M. Patient survival after renal transplantation: IV. Impact of post-transplant diabetes. Kidney Int. 2002, 62, 1440–1446. [Google Scholar] [CrossRef] [PubMed]
- Bayer, N.D.; Cochetti, P.T.; Anil Kumar, M.S.; Teal, V.; Huan, Y.; Doria, C.; Bloom, R.D.; Rosas, S.E. Association of metabolic syndrome with development of new-onset diabetes after transplantation. Transplantation 2010, 90, 861–866. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Israni, A.K.; Snyder, J.J.; Skeans, M.A.; Kasiske, B.L.; PORT Investigators. Clinical diagnosis of metabolic syndrome: Predicting new-onset diabetes, coronary heart disease, and allograft failure late after kidney transplant. Transpl. Int. 2012, 25, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Dedinská, I.; Laca, Ľ.; Miklušica, J.; Rosenberger, J.; Žilinská, Z.; Galajda, P.; Mokáň, M. Waist circumference as an independent risk factor for NODAT. Ann. Transplant. 2015, 20, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Heldal, T.F.; Ueland, T.; Jenssen, T.; Hartmann, A.; Reisaeter, A.V.; Aukrust, P.; Michelsen, A.; Åsberg, A. Inflammatory and related biomarkers are associated with post-transplant diabetes mellitus in kidney recipients: A retrospective study. Transpl. Int. 2018, 31, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Spoto, B.; Pisano, A.; Zoccali, C. Insulin resistance in chronic kidney disease: A systematic review. Am. J. Physiol. Renal. Physiol. 2016, 311, F1087–F1108. [Google Scholar] [CrossRef] [PubMed]
- Hecking, M.; Sharif, A.; Eller, K.; Jenssen, T. Management of post-transplant diabetes: Immunosuppression, early prevention, and novel antidiabetics. Transpl. Int. 2021, 34, 27–48. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Song, Y.; Wang, L.; Pittas, A.G.; Del Gobbo, L.C.; Zhang, C.; Manson, J.E.; Hu, F.B. Blood 25-hydroxy vitamin D levels and incident type 2 diabetes: A meta-analysis of prospective studies. Diabetes Care 2013, 36, 1422–1428. [Google Scholar] [CrossRef] [PubMed]
- Le Fur, A.; Fournier, M.C.; Gillaizeau, F.; Masson, D.; Giral, M.; Cariou, B.; Cantarovich, D.; Dantal, J. Vitamin D deficiency is an independent risk factor for PTDM after kidney transplantation. Transpl. Int. 2016, 29, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Foroutan, F.; Friesen, E.L.; Clark, K.E.; Motaghi, S.; Zyla, R.; Lee, Y.; Kamran, R.; Ali, E.; De Snoo, M.; Orchanian-Cheff, A.; et al. Risk Factors for 1-Year Graft Loss After Kidney Transplantation: Systematic Review and Meta-Analysis. Clin. J. Am. Soc. Nephrol. 2019, 14, 1642–1650. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gaynor, J.J.; Ciancio, G.; Guerra, G.; Sageshima, J.; Hanson, L.; Roth, D.; Goldstein, M.J.; Chen, L.; Kupin, W.; Mattiazzi, A.; et al. Single-centre study of 628 adult, primary kidney transplant recipients showing no unfavourable effect of new-onset diabetes after transplant. Diabetologia 2015, 58, 334–345. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.; Culliford, A.; Phagura, N.; Evison, F.; Gallier, S.; Sharif, A. Comparing survival outcomes for kidney transplant recipients with pre-existing diabetes versus those who develop post-transplantation diabetes. Diabet. Med. 2022, 39, e14707. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | T (n = 832) | ND (n = 595) | D (n = 237) | PTDM+ (n = 186) | AMG+ (n = 113) | AMG− (n = 371) | p |
|---|---|---|---|---|---|---|---|
| Age at transplantation, years | 49 ± 13 | 47 ± 13 | 54 ± 11 | 53 ± 11 | 53 ± 12 | 46 ± 13 | * <0.001 ^ <0.001 ° <0.001 |
| Gender (females/males), % | 42.2% 57.8% | 44.5% 55.5% | 36.3% 63.7% | 43.6% 56.4% | 35.4% 64.6% | 44.2% 55.8% | * 0.030 ^ 0.149 ° 0.081 |
| Type of dialysis (no/HD/ PD), % | 8.5% 70.6% 20.9% | 8.7% 72.9% 18.4% | 8.0% 65.0% 27.0% | 8.1% 65.0% 26.9% | 5.3% 70.8% 23.9% | 9.4% 66.3% 24.3% | * 0.022 ^ 0.041 ° 0.384 |
| Dialysis vintage, months | 54 ± 52 | 55 ± 53 | 50 ± 48 | 51 ± 47 | 54 ± 47 | 51 ± 50 | * 0.163 ^ 0.365 ° 0.654 |
| Type of transplant (deceased/living), % | 83.7% 16.3% | 82.5% 17.5% | 86.9% 13.1% | 84.9% 15.1% | 88.4% 11.6% | 79.0% 21.0% | * 0.120 ^ 0.369 ° 0.027 |
| Familiar history of diabetes, % | 23.0% | 20.2% | 30.0% | 24.5% | 24.0% | 20.4% | * 0.007 ^ 0.314 ° 0.267 |
| Steroid therapy before KTx, % | 39.2% | 40.6% | 35.7% | 37.0% | 32.1% | 39.6% | * 0.222 ^ 0.423 ° 0.176 |
| Parameters | 1st Month (T1) | 6th Month (T6) | 12th Month (T12) |
|---|---|---|---|
| eGFR (mL/min) | 64.66 ± 26.71 | 63.00 ± 23.70 | 64.27 ± 23.66 |
| Creatinine (mg/dL) | 1.45 ± 0.57 | 1.64 ± 5.72 | 1.41 ± 0.45 |
| Proteinuria (g/24 h) | 0.20 [0.14-0.30] | 0.18 [0.11–0.26] | 0.17 [0.11–0.26] |
| BMI (kg/m2) | 23.42 ± 3.75 | - | 24.32 ± 3.85 |
| SBP (mmHg) | 130.62 ± 16.45 | 131.23 ± 17.52 | 129.91 ± 16.80 |
| DBP (mmHg) | 79.71 ± 10.39 | 79.94 ± 10.28 | 79.63 ± 10.21 |
| Uric acid (mg/dL) | 5.79 ± 1.59 | 6.51 ± 1.52 | 6.54 ± 1.55 |
| Hemoglobin (g/dL) | 10.98 ± 1.36 | 12.29 ± 1.48 | 12.76 ± 1.60 |
| Albumin (g/dL) | 4.14 ± 0.43 | 4.40 ± 0.36 | 4.40 ± 0.36 |
| PTH (pg/mL) | 63 [38–104] | 57 [38–94] | 55 [37–88] |
| Ca (mg/dL) | 9.74 ± 0.79 | 9.84 ± 0.72 | 9.82 ± 0.70 |
| P (mg/dL) | 2.54 ± 0.90 | 3.10 ± 0.70 | 3.13 ± 0.64 |
| Mg (mg/dL) | 1.63 ± 0.23 | 1.74 ± 0.22 | 1.71 ± 0.23 |
| Glucose (mg/dL) | 88 ± 23 | 91 ± 23 | 89 ± 23 |
| Insulinemia (μIU/mL) | 8.70 [6.30–12.15] | 8.20 [5.90–11.79] | 8.60 [5.90–11.45] |
| Glycated hemoglobin (mmol/mol) | 36.42 ± 7.69 | 39.31 ± 7.74 | 39.76 ± 8.29 |
| Alkaline phosphatase (U/L) | 88 [68–121] | 91 [67–125] | 83 [62–111] |
| Total cholesterol (mg/dL) | 212 ± 50 | 200 ± 45 | 195 ± 43 |
| HDL cholesterol (mg/dL) | 61 ± 19 | 55 ± 17 | 56 ± 17 |
| Triglycerides (mg/dL) | 165 ± 85 | 159 ± 80 | 148 ± 68 |
| CRP (mg/dL) | 0.17 [0.08–0.54] | 0.12 [0.07–0.30] | 0.13 [0.07–0.34] |
| 25OH(D) (ng/dL) | 14.43 ± 7.93 | 16.70 ± 10.04 | 19.24 ± 11.56 |
| 1-25OH(D) (ng/dL) | 38.33 ± 23.83 | 49.09 ± 20.82 | 52.44 ± 20.82 |
| Parameters | p | Odds Ratio | CI | |
|---|---|---|---|---|
| Age at transplantation | <0.001 | 1.032 | 1.016 | 1.048 |
| BMI T1 | 0.002 | 1.080 | 1.029 | 1.133 |
| Total cholesterol (mg/dL) T1 | 0.126 | 1.003 | 0.999 | 1.007 |
| Triglycerides (mg/dL) T1 | 0.010 | 1.003 | 1.001 | 1.005 |
| Hemodialysis | 0.268 | 0.688 | 0.356 | 1.332 |
| Peritoneal dialysis | 0.876 | 1.059 | 0.518 | 2.161 |
| Parameters | p | Odds Ratio | IC | |
|---|---|---|---|---|
| Age at transplantation | 0.006 | 1.034 | 1.010 | 1.059 |
| BMI T1 | 0.027 | 1.091 | 1.010 | 1.178 |
| 25-OH (ng/mL) T1 | 0.005 | 0.935 | 0.892 | 0.979 |
| Triglycerides (mg/dL) T6 | 0.021 | 1.004 | 1.001 | 1.007 |
| CRP (mg/dL) T1 | 0.380 | 1.047 | 0.945 | 1.159 |
| Type of transplant | 0.325 | 1.526 | 0.658 | 3.540 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfieri, C.; Campioli, E.; Fiorina, P.; Orsi, E.; Grancini, V.; Regalia, A.; Campise, M.; Verdesca, S.; Delfrate, N.W.; Molinari, P.; et al. Post-Transplant Diabetes Mellitus in Kidney-Transplanted Patients: Related Factors and Impact on Long-Term Outcome. Nutrients 2024, 16, 1520. https://doi.org/10.3390/nu16101520
Alfieri C, Campioli E, Fiorina P, Orsi E, Grancini V, Regalia A, Campise M, Verdesca S, Delfrate NW, Molinari P, et al. Post-Transplant Diabetes Mellitus in Kidney-Transplanted Patients: Related Factors and Impact on Long-Term Outcome. Nutrients. 2024; 16(10):1520. https://doi.org/10.3390/nu16101520
Chicago/Turabian StyleAlfieri, Carlo, Edoardo Campioli, Paolo Fiorina, Emanuela Orsi, Valeria Grancini, Anna Regalia, Mariarosaria Campise, Simona Verdesca, Nicholas Walter Delfrate, Paolo Molinari, and et al. 2024. "Post-Transplant Diabetes Mellitus in Kidney-Transplanted Patients: Related Factors and Impact on Long-Term Outcome" Nutrients 16, no. 10: 1520. https://doi.org/10.3390/nu16101520
APA StyleAlfieri, C., Campioli, E., Fiorina, P., Orsi, E., Grancini, V., Regalia, A., Campise, M., Verdesca, S., Delfrate, N. W., Molinari, P., Pisacreta, A. M., Favi, E., Messa, P., & Castellano, G. (2024). Post-Transplant Diabetes Mellitus in Kidney-Transplanted Patients: Related Factors and Impact on Long-Term Outcome. Nutrients, 16(10), 1520. https://doi.org/10.3390/nu16101520