
Importance of an Ongoing Nutritional Counselling Intervention on Eating Habits of Newly Diagnosed Children with Celiac Disease

 , , , , and
, , , , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Participants and Recruitment Centers
2.2. Data Collection
2.3. Intervention Design
2.4. Anthropometric Measurements
2.5. Calculation of Energy Expenditure
2.6. Biochemical Data
2.7. Dietary Data
2.8. Statistical Analysis
3. Results
3.1. Anthropometric Parameters during the First Year of a GFD in Children and Adolescents with CD
3.2. Food Frequency Consumption of Foods among Children and Adolescents with CD
3.3. Mediterranean Diet Quality Index According to the KIDMED Questionnaire in Children and Adolescents with CD
3.4. Food Consumption According to the NOVA System in Children and Adolescents with CD
3.5. GFP Contribution to Total Energy Intake in Children and Adolescents with CD
3.6. Energy, Macronutrient, Fiber, and Cholesterol Intakes of Children and Adolescents with CD
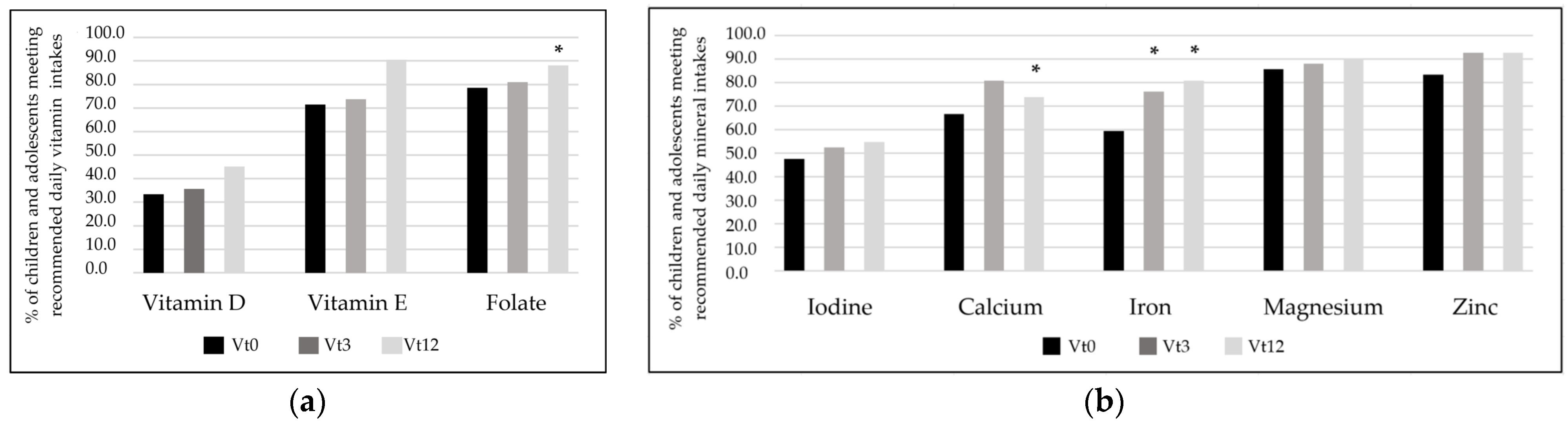
3.7. Micronutrient Intakes of Children and Adolescents with CD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Itzlinger, A.; Branchi, F.; Elli, L.; Schumann, M. Gluten-Free Diet in Celiac Disease-Forever and for All? Nutrients 2018, 10, 1796. [Google Scholar] [CrossRef]
- Gujral, N.; Freeman, H.J.; Thomson, A.B. Celiac disease: Prevalence, diagnosis, pathogenesis and treatment. World J. Gastroenterol. 2012, 18, 6036–6059. [Google Scholar] [CrossRef] [PubMed]
- Riznik, P.; De Leo, L.; Dolinsek, J.; Gyimesi, J.; Klemenak, M.; Koletzko, B.; Koletzko, S.; Korponay-Szabó, I.R.; Krencnik, T.; Not, T.; et al. Clinical Presentation in Children With Coeliac Disease in Central Europe. J. Pediatr. Gastroenterol. Nutr. 2021, 72, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac disease: A comprehensive current review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Rubio-Tapia, A. Epidemiology, Presentation, and Diagnosis of Celiac Disease. Gastroenterology 2021, 160, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Lindfors, K.; Ciacci, C.; Kurppa, K.; Lundin, K.E.A.; Makharia, G.K.; Mearin, M.L.; Murray, J.A.; Verdu, E.F.; Kaukinen, K. Coeliac disease. Nat. Rev. Dis. Primers 2019, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836.e822. [Google Scholar] [CrossRef] [PubMed]
- Di Nardo, G.; Villa, M.P.; Conti, L.; Ranucci, G.; Pacchiarotti, C.; Principessa, L.; Raucci, U.; Parisi, P. Nutritional Deficiencies in Children with Celiac Disease Resulting from a Gluten-Free Diet: A Systematic Review. Nutrients 2019, 11, 1588. [Google Scholar] [CrossRef]
- Roberts, S.E.; Morrison-Rees, S.; Thapar, N.; Benninga, M.A.; Borrelli, O.; Broekaert, I.; Dolinsek, J.; Martin-de-Carpi, J.; Mas, E.; Miele, E.; et al. Systematic review and meta-analysis: The incidence and prevalence of paediatric coeliac disease across Europe. Aliment. Pharmacol. Ther. 2021, 54, 109–128. [Google Scholar] [CrossRef]
- Mustalahti, K.; Catassi, C.; Reunanen, A.; Fabiani, E.; Heier, M.; McMillan, S.; Murray, L.; Metzger, M.H.; Gasparin, M.; Bravi, E.; et al. The prevalence of celiac disease in Europe: Results of a centralized, international mass screening project. Ann. Med. 2010, 42, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Sahin, Y. Celiac disease in children: A review of the literature. World J. Clin. Pediatr. 2021, 10, 53–71. [Google Scholar] [CrossRef] [PubMed]
- Kupper, C. Dietary guidelines and implementation for celiac disease. Gastroenterology 2005, 128, S121–S127. [Google Scholar] [CrossRef] [PubMed]
- Nasr, I.; Leffler, D.A.; Ciclitira, P.J. Management of celiac disease. Gastrointest. Endosc. Clin. N. Am. 2012, 22, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Commission Regulation (EC) No. 41/2009 of January 2009 concerning the composition and labelling of foodstuffs suitable for people intolerant to gluten. Off. J. Eur. Union 2009, L16, 3–5.
- Thompson, T. The Gluten-Free Labeling Rule: What Registered Dietitian Nutritionists Need to Know to Help Clients with Gluten-Related Disorders. J. Acad. Nutr. Diet. 2015, 115, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Sánchez, M.I.; Causada-Calo, N.; Bercik, P.; Ford, A.C.; Murray, J.A.; Armstrong, D.; Semrad, C.; Kupfer, S.S.; Alaedini, A.; Moayyedi, P.; et al. Safety of Adding Oats to a Gluten-Free Diet for Patients With Celiac Disease: Systematic Review and Meta-analysis of Clinical and Observational Studies. Gastroenterology 2017, 153, 395–409.e393. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.; Kaur, A.; Chopra, C.S. Gluten-Free Products for Celiac Susceptible People. Front. Nutr. 2018, 5, 116. [Google Scholar] [CrossRef]
- Zhang, M.; Jia, R.; Ma, M.; Yang, T.; Sun, Q.; Li, M. Versatile wheat gluten: Functional properties and application in the food-related industry. Crit. Rev. Food Sci. Nutr. 2023, 63, 10444–10460. [Google Scholar] [CrossRef]
- EU Law—EUR-Lex. Available online: https://eur-lex.europa.eu/homepage.html (accessed on 12 May 2024).
- Naik, R.D.; Seidner, D.L.; Adams, D.W. Nutritional Consideration in Celiac Disease and Nonceliac Gluten Sensitivity. Gastroenterol. Clin. N. Am. 2018, 47, 139–154. [Google Scholar] [CrossRef]
- Larretxi, I.; Simon, E.; Benjumea, L.; Miranda, J.; Bustamante, M.A.; Lasa, A.; Eizaguirre, F.J.; Churruca, I. Gluten-free-rendered products contribute to imbalanced diets in children and adolescents with celiac disease. Eur. J. Nutr. 2019, 58, 775–783. [Google Scholar] [CrossRef]
- Freeman, H.J. Dietary compliance in celiac disease. World J. Gastroenterol. 2017, 23, 2635–2639. [Google Scholar] [CrossRef]
- Cichewicz, A.B.; Mearns, E.S.; Taylor, A.; Boulanger, T.; Gerber, M.; Leffler, D.A.; Drahos, J.; Sanders, D.S.; Thomas Craig, K.J.; Lebwohl, B. Diagnosis and Treatment Patterns in Celiac Disease. Dig. Dis. Sci. 2019, 64, 2095–2106. [Google Scholar] [CrossRef]
- Ballestero Fernández, C.; Varela-Moreiras, G.; Úbeda, N.; Alonso-Aperte, E. Nutritional Status in Spanish Children and Adolescents with Celiac Disease on a Gluten Free Diet Compared to Non-Celiac Disease Controls. Nutrients 2019, 11, 2329. [Google Scholar] [CrossRef] [PubMed]
- Sue, A.; Dehlsen, K.; Ooi, C.Y. Paediatric Patients with Coeliac Disease on a Gluten-Free Diet: Nutritional Adequacy and Macro- and Micronutrient Imbalances. Curr. Gastroenterol. Rep. 2018, 20, 2. [Google Scholar] [CrossRef]
- Suárez-González, M.; Bousoño-García, C.; Jiménez-Treviño, S.; Díaz-Martín, J.J. Gluten-Free Diet: Nutritional Strategies to Improve Eating Habits in Children with Celiac Disease: A Prospective, Single-arm Intervention Study. Nutrients 2021, 13, 1108. [Google Scholar] [CrossRef]
- Lasa, A.; Fernandez Gil, P.; Bustamante, M.; Miranda, J. Nutritional and Sensorial Aspects of Gluten-Free Products. In Nutritional and Analytical Approaches of Gluten-Free Diet in Celiac Disease; Sringer: Cham, Switzerland, 2017; pp. 59–78. [Google Scholar]
- Simón, E.; Molero-Luis, M.; Fueyo-Díaz, R.; Costas-Batlle, C.; Crespo-Escobar, P.; Montoro-Huguet, M.A. The Gluten-Free Diet for Celiac Disease: Critical Insights to Better Understand Clinical Outcomes. Nutrients 2023, 15, 4013. [Google Scholar] [CrossRef] [PubMed]
- Costas-Batlle, C.; Trott, N.; Jeanes, Y.; Seamark, L.; Gardiner, C. A dietitian-led coeliac service helps to identify and reduce involuntary gluten ingestion with subsequent reduction in the frequency of repeat endoscopies. J. Hum. Nutr. Diet. 2023, 36, 1751–1759. [Google Scholar] [CrossRef] [PubMed]
- Perez-Junkera, G.; Vázquez-Polo, M.; Eizagirre, F.J.; Benjumea, L.; Tutau, C.; Esteban, B.; Miranda, J.; Larretxi, I.; Navarro, V.; Churruca, I.; et al. Application of a Platform for Gluten-Free Diet Evaluation and Dietary Advice: From Theory to Practice. Sensors 2022, 22, 732. [Google Scholar] [CrossRef]
- Shepherd, S.J.; Gibson, P.R. Nutritional inadequacies of the gluten-free diet in both recently-diagnosed and long-term patients with coeliac disease. J. Hum. Nutr. Diet. 2013, 26, 349–358. [Google Scholar] [CrossRef]
- Hsu, M.S.H.; Rouf, A.; Allman-Farinelli, M. Effectiveness and Behavioral Mechanisms of Social Media Interventions for Positive Nutrition Behaviors in Adolescents: A Systematic Review. J. Adolesc. Health 2018, 63, 531–545. [Google Scholar] [CrossRef] [PubMed]
- Sobradillo, B.; Aguirre, A.; Aresti, U.; Bilbao, A.; Fernández-Ramos, C.; Lizárraga, A.; Lorenzo, H.; Madariaga, L.; Rica, I.; Ruiz, I.; et al. Curvas y Tablas de Crecimiento. Estudios Longitudinal y Transversal; Fundación Faustino Orbegozo: Bilbao, Spain, 2004; pp. 1–31. [Google Scholar]
- SEGHNP (Sociedad Española de Gastroenterología, Hepatología y Nutrición Pediátrica). Aplicación Nutricional. Available online: https://www.seghnp.org/nutricional/ (accessed on 1 September 2020).
- Russolillo, G.; Marques, I. Food Portion Sizes Album; Imagen Comunicación Multimedia: Madrid, Spain, 2008; p. 186. [Google Scholar]
- FESNAD. Dietary reference intakes (DRI) for Spanish population, 2010. Act Dietética 2010, 14, 196–197. [Google Scholar]
- SENC. Objetivos nutricionales para la población española. Consenso de la Sociedad Española de Nutrición. Rev. Esp. Nutri. Comunitaria 2011, 17, 178–199. [Google Scholar]
- Monteiro, C.; Cannon, G.; Lawrence, M.; Louzada, M.L.; Machado, P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy, 2019. [Google Scholar]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Gładyś, K.; Dardzińska, J.; Guzek, M.; Adrych, K.; Kochan, Z.; Małgorzewicz, S. Expanded Role of a Dietitian in Monitoring a Gluten-Free Diet in Patients with Celiac Disease: Implications for Clinical Practice. Nutrients 2021, 13, 1859. [Google Scholar] [CrossRef] [PubMed]
- Lionetti, E.; Catassi, C. New clues in celiac disease epidemiology, pathogenesis, clinical manifestations, and treatment. Int. Rev. Immunol. 2011, 30, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Bascuñán, K.A.; Vespa, M.C.; Araya, M. Celiac disease: Understanding the gluten-free diet. Eur. J. Nutr. 2017, 56, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Melini, V.; Melini, F. Gluten-Free Diet: Gaps and Needs for a Healthier Diet. Nutrients 2019, 11, 170. [Google Scholar] [CrossRef]
- Penagini, F.; Dilillo, D.; Meneghin, F.; Mameli, C.; Fabiano, V.; Zuccotti, G.V. Gluten-free diet in children: An approach to a nutritionally adequate and balanced diet. Nutrients 2013, 5, 4553–4565. [Google Scholar] [CrossRef]
- Lionetti, E.; Antonucci, N.; Marinelli, M.; Bartolomei, B.; Franceschini, E.; Gatti, S.; Catassi, G.N.; Verma, A.K.; Monachesi, C.; Catassi, C. Nutritional Status, Dietary Intake, and Adherence to the Mediterranean Diet of Children with Celiac Disease on a Gluten-Free Diet: A Case-Control Prospective Study. Nutrients 2020, 12, 143. [Google Scholar] [CrossRef]
- Gessaroli, M.; Frazzoni, L.; Sikandar, U.; Bronzetti, G.; Pession, A.; Zagari, R.M.; Fuccio, L.; Forchielli, M.L. Nutrient intakes in adult and pediatric coeliac disease patients on gluten-free diet: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2023, 77, 784–793. [Google Scholar] [CrossRef] [PubMed]
- James, S.P. National Institutes of Health Consensus Development Conference Statement on Celiac Disease, June 28-30, 2004. Gastroenterology 2005, 128, S1–S9. [Google Scholar] [CrossRef] [PubMed]
- Robinson, G.H.J.; Balk, J.; Domoney, C. Improving pulse crops as a source of protein, starch and micronutrients. Nutr. Bull. 2019, 44, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Suárez-González, M.; Bousoño García, C.; Jiménez Treviño, S.; Iglesias Cabo, T.; Díaz Martín, J.J. Influence of nutrition education in paediatric coeliac disease: Impact of the role of the registered dietitian: A prospective, single-arm intervention study. J. Hum. Nutr. Diet. 2020, 33, 775–785. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of ultra-processed foods and health status: A systematic review and meta-analysis. Br. J. Nutr. 2021, 125, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Cordova, R.; Viallon, V.; Fontvieille, E.; Peruchet-Noray, L.; Jansana, A.; Wagner, K.H.; Kyrø, C.; Tjønneland, A.; Katzke, V.; Bajracharya, R.; et al. Consumption of ultra-processed foods and risk of multimorbidity of cancer and cardiometabolic diseases: A multinational cohort study. Lancet Reg. Health Eur. 2023, 35, 100771. [Google Scholar] [CrossRef]
- Srour, B.; Kordahi, M.C.; Bonazzi, E.; Deschasaux-Tanguy, M.; Touvier, M.; Chassaing, B. Ultra-processed foods and human health: From epidemiological evidence to mechanistic insights. Lancet Gastroenterol. Hepatol. 2022, 7, 1128–1140. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef]
- Tristan Asensi, M.; Pagliai, G.; Lotti, S.; Corrao, A.; Colombini, B.; Giangrandi, I.; Sofi, F.; Dinu, M. Adherence to the Mediterranean Diet and Ultra-Processed Foods Consumption in a Group of Italian Patients with Celiac Disease. Nutrients 2023, 15, 938. [Google Scholar] [CrossRef]
- Anania, C.; Pacifico, L.; Olivero, F.; Perla, F.M.; Chiesa, C. Cardiometabolic risk factors in children with celiac disease on a gluten-free diet. World J. Clin. Pediatr. 2017, 6, 143–148. [Google Scholar] [CrossRef]
- Norsa, L.; Shamir, R.; Zevit, N.; Verduci, E.; Hartman, C.; Ghisleni, D.; Riva, E.; Giovannini, M. Cardiovascular disease risk factor profiles in children with celiac disease on gluten-free diets. World J. Gastroenterol. 2013, 19, 5658–5664. [Google Scholar] [CrossRef]
- Calcaterra, V.; Cena, H.; Rossi, V.; Santero, S.; Bianchi, A.; Zuccotti, G. Ultra-Processed Food, Reward System and Childhood Obesity. Children 2023, 10, 804. [Google Scholar] [CrossRef]
- Cadenhead, J.W.; Martínez-Steele, E.; Contento, I.; Kushi, L.H.; Lee, A.R.; Nguyen, T.T.T.; Lebwohl, B.; Green, P.H.R.; Wolf, R.L. Diet quality, ultra-processed food consumption, and quality of life in a cross-sectional cohort of adults and teens with celiac disease. J. Hum. Nutr. Diet. 2023, 36, 1144–1158. [Google Scholar] [CrossRef]
- González, M.P.; Ballestero-Fernández, C.; Fajardo, V.; Achón, M.; García-González, Á.; Alonso-Aperte, E.; Úbeda, N. Gluten-Free Product Contribution to Energy and Macronutrient Intakes in Spanish Children and Adolescents with Celiac Disease. Foods 2022, 11, 3790. [Google Scholar] [CrossRef]
- Zuccotti, G.; Fabiano, V.; Dilillo, D.; Picca, M.; Cravidi, C.; Brambilla, P. Intakes of nutrients in Italian children with celiac disease and the role of commercially available gluten-free products. J. Hum. Nutr. Diet. 2013, 26, 436–444. [Google Scholar] [CrossRef]
- Bardella, M.T.; Fredella, C.; Prampolini, L.; Molteni, N.; Giunta, A.M.; Bianchi, P.A. Body composition and dietary intakes in adult celiac disease patients consuming a strict gluten-free diet. Am. J. Clin. Nutr. 2000, 72, 937–939. [Google Scholar] [CrossRef]
- Ohlund, K.; Olsson, C.; Hernell, O.; Ohlund, I. Dietary shortcomings in children on a gluten-free diet. J. Hum. Nutr. Diet. 2010, 23, 294–300. [Google Scholar] [CrossRef]
- Vici, G.; Belli, L.; Biondi, M.; Polzonetti, V. Gluten free diet and nutrient deficiencies: A review. Clin. Nutr. 2016, 35, 1236–1241. [Google Scholar] [CrossRef]
- Martín-Masot, R.; Jiménez-Muñoz, M.; Herrador-López, M.; Flor-Alemany, M.; Navas-López, V.M.; Nestares, T. The Importance of an Early Evaluation after Establishing a Gluten-Free Diet in Children with Celiac Disease. Nutrients 2023, 15, 1761. [Google Scholar] [CrossRef]
- Mariani, P.; Viti, M.G.; Montouri, M.; La Vecchia, A.; Cipolletta, E.; Calvani, L.; Bonamico, M. The Gluten-Free Diet: A Nutritional Risk Factor for Adolescents with Celiac Disease? J. Pediatr. Gastroenterol. Nutr. 1998, 27, 519–523. [Google Scholar]
- Forchielli, M.L.; Fernicola, P.; Diani, L.; Scrivo, B.; Salfi, N.C.; Pessina, A.C.; Lima, M.; Conti, V.; Pession, A. Gluten-Free Diet and Lipid Profile in Children With Celiac Disease: Comparison With General Population Standards. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 224–229. [Google Scholar] [CrossRef]
- Wild, D.; Robins, G.G.; Burley, V.J.; Howdle, P.D. Evidence of high sugar intake, and low fibre and mineral intake, in the gluten-free diet. Aliment. Pharmacol. Ther. 2010, 32, 573–581. [Google Scholar] [CrossRef]
- Theethira, T.G.; Dennis, M. Celiac disease and the gluten-free diet: Consequences and recommendations for improvement. Dig. Dis. 2015, 33, 175–182. [Google Scholar] [CrossRef]
- Babio, N.; Alcázar, M.; Castillejo, G.; Recasens, M.; Martínez-Cerezo, F.; Gutiérrez-Pensado, V.; Masip, G.; Vaqué, C.; Vila-Martí, A.; Torres-Moreno, M.; et al. Patients With Celiac Disease Reported Higher Consumption of Added Sugar and Total Fat Than Healthy Individuals. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 63–69. [Google Scholar] [CrossRef]
- Larretxi, I.; Txurruka, I.; Navarro, V.; Lasa, A.; Bustamante, M.Á.; Fernández-Gil, M.D.P.; Simón, E.; Miranda, J. Micronutrient Analysis of Gluten-Free Products: Their Low Content Is Not Involved in Gluten-Free Diet Imbalance in a Cohort of Celiac Children and Adolescent. Foods 2019, 8, 321. [Google Scholar] [CrossRef]
- Mager, D.R.; Liu, A.; Marcon, M.; Harms, K.; Brill, H.; Mileski, H.; Dowhaniuk, J.; Nasser, R.; Carroll, M.W.; Persad, R.; et al. Diet patterns in an ethnically diverse pediatric population with celiac disease and chronic gastrointestinal complaints. Clin. Nutr. ESPEN 2019, 30, 73–80. [Google Scholar] [CrossRef]
- Pearce, E.N.; Lazarus, J.H.; Moreno-Reyes, R.; Zimmermann, M.B. Consequences of iodine deficiency and excess in pregnant women: An overview of current knowns and unknowns. Am. J. Clin. Nutr. 2016, 104 (Suppl. S3), 918S–923S. [Google Scholar] [CrossRef]
- Delvecchio, M.; Bizzoco, F.; Lapolla, R.; Gentile, A.; Carrozza, C.; Barone, M.; Simonetti, S.; Giordano, P.; Dargenio, V.N.; Cristofori, F.; et al. Iodine Absorption in Celiac Children: A Longitudinal Pilot Study. Nutrients 2021, 13, 808. [Google Scholar] [CrossRef]
- Gobbetti, M.; Pontonio, E.; Filannino, P.; Rizzello, C.G.; De Angelis, M.; Di Cagno, R. How to improve the gluten-free diet: The state of the art from a food science perspective. Food Res. Int. 2018, 110, 22–32. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Children and Adolescents | p Value | |||||||
|---|---|---|---|---|---|---|---|---|
| Recommended Daily Portion Intake * | Vt0 | Vt3 | Vt12 | Vt0 vs. Vt3 | Vt0 vs. Vt12 | Vt3 vs. Vt12 | ||
| Daily consumption | Dairy | 2–4 | 1.9 ± 0.4 | 2.3 ± 0.6 | 2.4 ± 0.5 | <0.001 | <0.001 | NS |
| BRI | 36% | 14% | 26% | |||||
| RI | 64% | 86% | 74% | |||||
| ARI | 0% | 0% | 0% | |||||
| Cereals | 4–6 | 3.3 ± 0.8 | 4 ± 0.8 | 4 ± 1.9 | <0.001 | 0.001 | NS | |
| BRI | 60% | 26% | 33% | |||||
| RI | 40% | 74% | 67% | |||||
| ARI | 0% | 0% | 0% | |||||
| Vegetables | 2 | 0.6 ± 0.4 | 0.9 ± 0.2 | 1 ± 0.5 | <0.001 | <0.001 | NS | |
| BRI | 95% | 86% | 81% | |||||
| RI | 5% | 14% | 19% | |||||
| ARI | 0% | 0% | 0% | |||||
| Fruits | 3 | 1.7 ± 0.6 | 2.1 ± 0.6 | 1.8 ± 0.6 | <0.05 | <0.05 | NS | |
| BRI | 90% | 83% | 83% | |||||
| RI | 10% | 17% | 17% | |||||
| ARI | 0% | 0% | 0% | |||||
| Oils | 3–6 | 3 ± 0.5 | 3.3 ± 0.7 | 3.4 ± 0.6 | <0.05 | <0.05 | NS | |
| BRI | 26% | 10% | 5% | |||||
| RI | 74% | 90% | 95% | |||||
| ARI | 0% | 0% | 0% | |||||
| Weekly consumption | Meat | 3–4 | 4.4 ± 1.8 | 4 ± 1.8 | 4.2 ± 1.3 | <0.05 | NS | NS |
| BRI | 2% | 10% | 2% | |||||
| RI | 45% | 57% | 45% | |||||
| ARI | 53% | 33% | 53% | |||||
| Fish | 3–4 | 3 ± 2 | 3.1 ± 1.7 | 3.1 ± 1.9 | NS | NS | NS | |
| BRI | 41% | 36% | 40% | |||||
| RI | 38% | 48% | 46% | |||||
| ARI | 21% | 16% | 14% | |||||
| Eggs | 3–4 | 3.1 ± 0.5 | 3 ± 0.4 | 3 ± 0.4 | NS | NS | NS | |
| BRI | 10% | 12% | 12% | |||||
| RI | 71% | 81% | 69% | |||||
| ARI | 19% | 7% | 19% | |||||
| Legumes | 2–4 | 2.2 ± 1.2 | 2.4 ± 1.1 | 2.7 ± 1 | <0.05 | <0.05 | <0.05 | |
| BRI | 33% | 24% | 19% | |||||
| RI | 67% | 76% | 74% | |||||
| ARI | 0% | 0% | 7% | |||||
| Nuts | 3–7 | 1.5 ± 2.1 | 2.6 ± 2.1 | 2.4 ± 2.3 | <0.001 | <0.05 | NS | |
| BRI | 67% | 36% | 50% | |||||
| RI | 33% | 62% | 48% | |||||
| ARI | 0% | 2% | 2% | |||||
| Pastries | 4.7 ± 3 | 4.1 ± 3.5 | 3.9 ± 3.9 | NS | NS | NS | ||
| Sausages | 3.3 ± 2 | 2.1 ± 1.7 | 2.5 ± 1.2 | <0.05 | 0.056 | NS | ||
| Children and Adolescents | p Value | |||||
|---|---|---|---|---|---|---|
| Vt0 | Vt3 | Vt12 | Vt0 vs. Vt3 | Vt0 vs. Vt12 | ||
| Total punctuation | 6.5 ± 2.1 | 7.9 ± 1.4 | 7.7 ± 2.1 | <0.001 | <0.001 | |
| KIDMED index score | Poor (≤3) | 10% | 0% | 2% | ||
| Average (4–7) | 55% | 38% | 43% | |||
| Good (≥8) | 35% | 62% | 55% | |||
| Children and Adolescents | p Value | |||||
|---|---|---|---|---|---|---|
| Vt0 | Vt3 | Vt12 | Vt0 vs. Vt3 | Vt0 vs. Vt12 | Vt3 vs. Vt12 | |
| G1 | 6.6 ± 2 | 7.2 ± 2 | 7.1 ± 1.9 | <0.05 | <0.05 | NS |
| G2 | 2.7 ± 0.7 | 2.9 ± 1.1 | 2.7 ± 0.9 | NS | NS | NS |
| G3 | 0.7 ± 0.4 | 0.7 ± 0.5 | 0.9 ± 0.7 | NS | <0.05 | <0.05 |
| G4 | 4.5 ± 1.3 | 4 ± 1.5 | 3.8 ± 1.5 | <0.05 | <0.05 | NS |
| Children and Adolescents | p Value | |||||
|---|---|---|---|---|---|---|
| Vt0 | Vt3 | Vt12 | Vt0 vs. Vt3 | Vt0 vs. Vt12 | Vt3 vs. Vt12 | |
| GFP | 2.5 ± 0.9 | 2.3 ± 0.9 | 2.3 ± 0.9 | NS | <0.05 | NS |
| Ultraprocessed dairy products | 0.8 ± 0.6 | 0.6 ± 0.6 | 0.5 ± 0.5 | NS | 0.06 | NS |
| Snacks | 0.1 ± 0.2 | 0.1 ± 0.2 | 0.2 ± 0.2 | NS | NS | NS |
| Candy and chocolates | 0.3 ± 0.4 | 0.2 ± 0.3 | 0.3 ± 0.4 | <0.05 | NS | NS |
| Sausages | 0.6 ± 0.5 | 0.4 ± 0.4 | 0.5 ± 0.4 | NS | NS | NS |
| Other ultraprocesed foods (soft drinks, juices, ultra processed foods and sauces) | 0.2 ± 0.2 | 0.1 ± 0.2 | 0.1 ± 0.2 | NS | NS | NS |
| Children and Adolescents | p Value | ||||||
|---|---|---|---|---|---|---|---|
| Recommended Intake * | Vt0 | Vt3 | Vt12 | Vt0 vs. Vt3 | Vt0 vs. Vt12 | Vt3 vs. Vt12 | |
| Energy intake (kcal) | ±20% of EE | 1508.4 ± 175.1 | 1678.1 ± 253 | 1710.1 15 ± 207.9 | <0.001 | <0.001 | NS |
| <80% | 40% | 36% | 38% | ||||
| 80–120% | 48% | 50% | 45% | ||||
| >120% | 12% | 14% | 17% | ||||
| Protein (%) | 10–15 | 16.2 ± 2.2 | 15.7 ± 2 | 16.7 ± 2.1 | NS | NS | NS |
| <10% | 0% | 0% | 0% | ||||
| 10–15% | 24% | 43% | 26% | ||||
| >15% | 76% | 57% | 74% | ||||
| Lipids (%) | 30–35 | 38 ± 3.9 | 37.3 ± 5.2 | 37.1 ± 4.4 | NS | NS | NS |
| <30% | 7% | 9% | 5% | ||||
| 30–35% | 17% | 29% | 24% | ||||
| >35% | 76% | 62% | 71% | ||||
| Saturated fats (%) | <10 | 11.4 ± 2.1 | 10.5 ± 2.6 | 11.4 ± 2.4 | NS | NS | NS |
| <10% | 33% | 48% | 36% | ||||
| ≥10% | 67% | 52% | 64% | ||||
| Monounsaturated fats (%) | ≥20 | 15.1 ± 2.6 | 14.5 ± 3.6 | 15.1 ± 3.4 | NS | NS | NS |
| <20% | 90.5% | 83% | 90% | ||||
| ≥20% | 9.5% | 17% | 10% | ||||
| Polyunsaturated fats (%) | ≥4 | 4.1 ± 0.8 | 4.2 ± 1.5 | 4.2 ± 1 | NS | NS | NS |
| <4% | 45% | 55% | 38% | ||||
| ≥4% | 55% | 45% | 62% | ||||
| Carbohydrates (%) | 50–60 | 45.7 ± 4.1 | 47 ± 5.6 | 46.2 ± 4.5 | <0.05 | NS | NS |
| <50% | 83% | 67% | 74% | ||||
| 50–60% | 17% | 33% | 26% | ||||
| >60% | 0% | 0% | 0% | ||||
| Simple sugars (%) | <10 | 12.5 ± 3.4 | 11.8 ± 4.4 | 12.9 ± 3.7 | NS | NS | <0.05 |
| <10% | 29% | 29% | 21% | ||||
| ≥10% | 71% | 71% | 79% | ||||
| Fibre (g) | g/day | 18.1 ± 6.4 | 20.5 ± 8.3 | 21.9 ± 6.7 | NS | <0.05 | NS |
| <10 g/1000 kcal | 29% | 26% | 21% | ||||
| 10–14 g/1000 kcal | 52% | 57% | 48% | ||||
| >14 g/1000 kcal | 19% | 17% | 31% | ||||
| Cholesterol (mg) | <300 | 240 ± 93.3 | 280 ± 83.2 | 272.89 ± 80.2 | NS | <0.05 | NS |
| <300 | 36% | 55% | 52% | ||||
| ≥300 | 64% | 45% | 48% | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perez-Junkera, G.; Simón, E.; Calvo, A.E.; García Casales, Z.; Oliver Goicolea, P.; Serrano-Vela, J.I.; Larretxi, I.; Lasa, A. Importance of an Ongoing Nutritional Counselling Intervention on Eating Habits of Newly Diagnosed Children with Celiac Disease. Nutrients 2024, 16, 2418. https://doi.org/10.3390/nu16152418
Perez-Junkera G, Simón E, Calvo AE, García Casales Z, Oliver Goicolea P, Serrano-Vela JI, Larretxi I, Lasa A. Importance of an Ongoing Nutritional Counselling Intervention on Eating Habits of Newly Diagnosed Children with Celiac Disease. Nutrients. 2024; 16(15):2418. https://doi.org/10.3390/nu16152418
Chicago/Turabian StylePerez-Junkera, Gesala, Edurne Simón, Ariane Erika Calvo, Zuriñe García Casales, Pablo Oliver Goicolea, Juan Ignacio Serrano-Vela, Idoia Larretxi, and Arrate Lasa. 2024. "Importance of an Ongoing Nutritional Counselling Intervention on Eating Habits of Newly Diagnosed Children with Celiac Disease" Nutrients 16, no. 15: 2418. https://doi.org/10.3390/nu16152418
APA StylePerez-Junkera, G., Simón, E., Calvo, A. E., García Casales, Z., Oliver Goicolea, P., Serrano-Vela, J. I., Larretxi, I., & Lasa, A. (2024). Importance of an Ongoing Nutritional Counselling Intervention on Eating Habits of Newly Diagnosed Children with Celiac Disease. Nutrients, 16(15), 2418. https://doi.org/10.3390/nu16152418