
Development and Evaluation of the Reliability of a Semi-Quantitative Food Frequency Questionnaire to Assess the Intake in the Serbian Population
 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Methodology
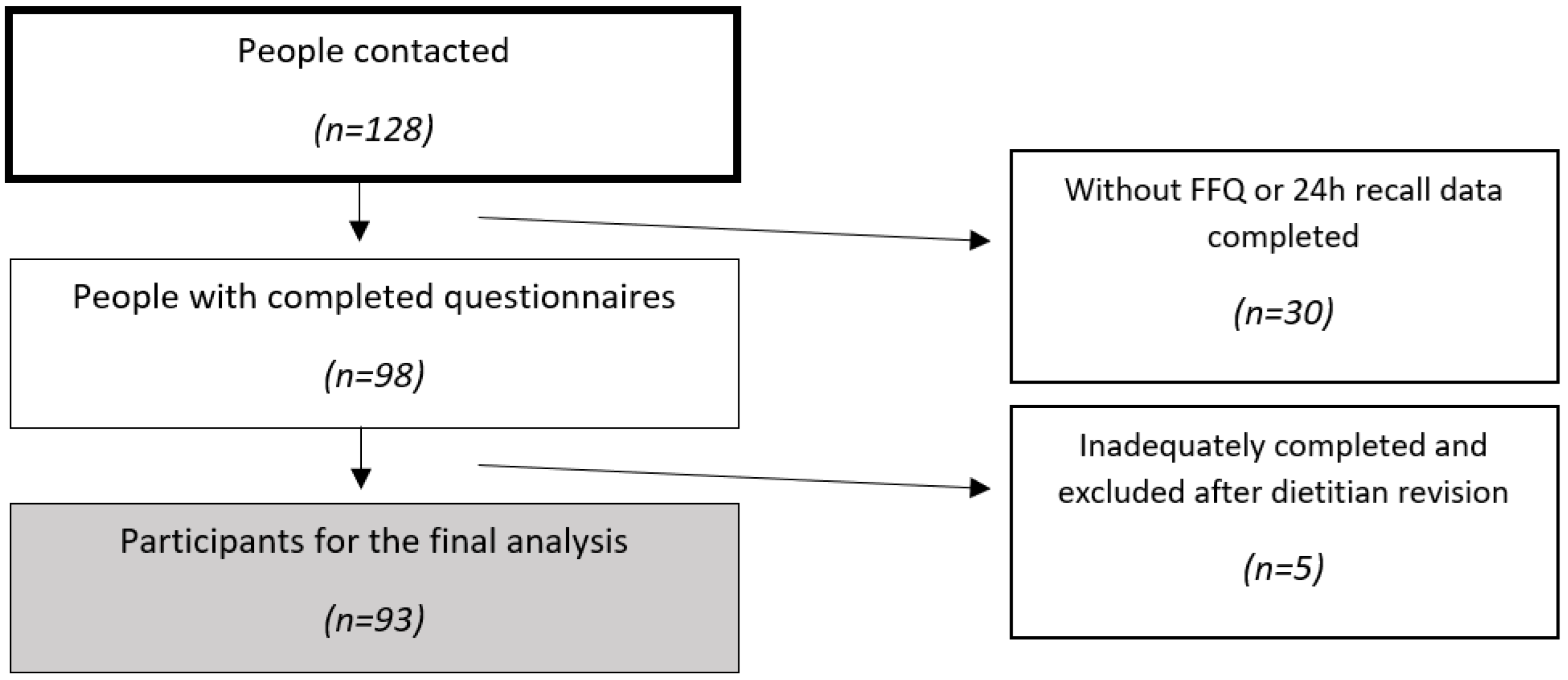
2.1. Participants, Recruitment, and Ethics
2.2. Food Frequency Questionnaire Development
2.3. Food Frequency Questionnaire Validation
2.4. General Data and Anthropometric Measurements
2.5. Statistics
3. Results
4. Discussion
5. Strengths and Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Food and Agriculture Organization of the United Nations. Dietary Assessment. A Resource Guide to Method Selection and Application in Low Resource Settings. Available online: https://www.fao.org/3/i9940en/I9940EN.pdf (accessed on 25 August 2023).
- Bailey, R.L. Overview of dietary assessment methods for measuring intakes of foods, beverages, and dietary supplements in research studies. Curr. Opin. Biotechnol. 2021, 70, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Naska, A.; Lagiou, A.; Lagiou, P. Dietary assessment methods in epidemiological research: Current state of the art and future prospects. F1000Research 2017, 6, 926. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.A.; Landry, D.; Little, J.; Minelli, C. Systematic review of statistical approaches to quantify, or correct for, measurement error in a continuous exposure in nutritional epidemiology. BMC. Med. Res. Methodol. 2017, 17, 146. [Google Scholar] [CrossRef] [PubMed]
- Rakic, L.; Djokic, D.; Drakulovic, M.; Pejic, A.; Radojicic, Z.; Marinkovic, M. Risk factors associated with anemia among Serbian non-pregnant women 20 to 49 years old. A cross-sectional study. Hippokratia 2013, 17, 47–54. [Google Scholar] [PubMed]
- Stosovic, D.; Vasiljevic, N.; Jovanovic, V.; Cirkovic, A.; Paunovic, K.; Davidovic, D. Dietary habits of older adults in Serbia: Findings from the National Health Survey. Front. Public Health 2021, 9, 610873. [Google Scholar] [CrossRef] [PubMed]
- Statistical Office of the Republic of Serbia. The 2019 Serbian National Health Survey. Available online: https://www.stat.gov.rs/en-us/vesti/20210429-istrazivanje-zdravlja-stan/ (accessed on 23 August 2023).
- Milešević, J.; Vranić, D.; Gurinović, M.; Korićanac, V.; Borović, B.; Zeković, M.; Glibetić, M. The intake of phosphorus and nitrites through meat products: A health risk assessment of children aged 1 to 9 years old in Serbia. Nutrients 2022, 14, 242. [Google Scholar] [CrossRef] [PubMed]
- Milešević, J.; Slobodan, L.; Vranić, D.; Zeković, M.; Borović, B.; Glibetić, M.; Milićević, D. Dietary intake of salt from meat products in Serbian population. Int. J. Environ. Res. Public Health 2023, 20, 4192. [Google Scholar] [CrossRef] [PubMed]
- Janković, S.; Stošić, M.; Miljaković, E.A.; Ćurčić, M.; Ćosić, D.D.; Đorđević, A.B.; Antonijević, B. Cadmium dietary exposure assessment in the adult population and pre-school children in the Republic of Serbia. Food Addit. Contam. Part A Chem. Anal. Control. Expo. Risk. Assess. 2023, 40, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Djekic-Ivankovic, M.; Weiler, H.A.; Nikolic, M.; Kadvan, A.; Gurinovic, M.; Mandic, L.M.; Glibetic, M. Validity of an FFQ assessing the vitamin D intake of young Serbian women living in a region without food fortification: The method of triads model. Public Health Nutr. 2016, 19, 437–445. [Google Scholar] [CrossRef]
- Zekovic, M.; Djekic-Ivankovic, M.; Nikolic, M.; Gurinovic, M.; Krajnovic, D.; Glibetic, M. Validity of the food frequency questionnaire assessing the folate intake in women of reproductive age living in a country without food fortification: Application of the method of triads. Nutrients 2017, 9, 128. [Google Scholar] [CrossRef]
- Udovicki, B.; Keskic, T.; Aleksic, B.; Smigic, N.; Rajkovic, A. Second order probabilistic assessment of chronic dietary exposure to aflatoxin M1 in Serbia. Food Chem. Toxicol. 2023, 178, 113906. [Google Scholar] [CrossRef] [PubMed]
- Samuelson, G. Dietary habits and nutritional status in adolescents over Europe: An overview of current studies in the Nordic countries. Eur. J. Clin. Nutr. 2000, 54S1, S21–S28. [Google Scholar] [CrossRef] [PubMed]
- Kiani, A.K.; Medori, M.C.; Bonetti, G.; Aquilanti, B.; Velluti, V.; Matera, G.; Bertelli, M. Modern vision of the Mediterranean diet. J. Prev. Med. Hyg. 2022, 63, 2–3. [Google Scholar]
- Boylan, S.; Welch, A.; Pikhart, H.; Malyutina, S.; Pajak, A.; Kubinova, R.; Bobak, M. Dietary habits in three Central and Eastern European countries: The HAPIEE study. BMC. Public Health 2009, 9, 439. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.; Machado, P.; Santos, T.; Sievert, K.; Backholer, K.; Hadjikakou, M.; Lawrence, M. Ultra-processed foods and the nutrition transition: Global, regional and national trends, food systems transformations and political economy drivers. Obes. Rev. 2020, 21, 12. [Google Scholar] [CrossRef] [PubMed]
- Poobalan, A.S.; Aucott, L.S.; Clarke, A.; Smith, W.C.S. Diet behaviour among young people in transition to adulthood (18–25 year olds): A mixed method study. Health Psychol. Behav. Med. 2014, 2, 909–928. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Pêgo, C.; Nissensohn, M.; Kavouras, S.A.; Babio, N.; Serra-Majem, L.; Águila, A.M.; Salas-Salvadó, J. Relative validity and repeatability in a Spanish population with metabolic syndrome from the PREDIMED-PLUS study. Nutrients 2016, 8, 475. [Google Scholar] [CrossRef] [PubMed]
- de la Fuente-Arrillaga, C.; Ruiz, Z.V.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef]
- Fundación Iberoamericana de Nutrición. EvalFINUT 2.0. Available online: https://www.finut.org/evalfinut/ (accessed on 24 August 2023).
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: Oxford, UK, 2013; pp. 70–95. [Google Scholar]
- Block, G.; Wakimoto, P.; Jensen, C.; Mandel, S.; Green, R.R. Validation of a food frequency questionnaire for Hispanics. Prev. Chronic. Dis. 2006, 3, 3. [Google Scholar]
- Tijerina, A.; Tur, J.A. Development and validation of a semiquantitative food frequency questionnaire to assess dietary intake in 40-65-year-old Mexican women. Ann. Nutr. Metab. 2020, 76, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1231S. [Google Scholar] [CrossRef] [PubMed]
- Decarli, A.; Franceschi, S.; Ferraroni, M.; Gnagnarella, P.; Parpinel, M.T.; La Vecchia, C.; Giacosa, A. Validation of a food-frequency questionnaire to assess dietary intakes in cancer studies in Italy: Results for specific nutrients. Ann. Epidemiol. 1996, 6, 110–118. [Google Scholar] [CrossRef] [PubMed]
- El Kinany, K.; Garcia-Larsen, V.; Khalis, M.; Deoula, M.M.S.; Benslimane, A.; Ibrahim, A.; El Rhazi, K. Adaptation and validation of a food frequency questionnaire (FFQ) to assess dietary intake in Moroccan adults. Nutr. J. 2018, 17, 61. [Google Scholar] [CrossRef] [PubMed]
- van Dongen, M.C.; Wijckmans-Duysens, N.E.G.; den Biggelaar, L.J.; Ocké, M.C.; Meijboom, S.; Brants, H.A.; de Vries, J.H.; Feskens, E.J.; Bueno-de-Mesquita, H.B.; Geelen, A.; et al. The Maastricht FFQ: Development and validation of a comprehensive food frequency questionnaire for the Maastricht study. Nutrition 2019, 62, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Tenório, M.C.D.S.; Wanderley, T.M.; Macedo, I.A.; Vanderlei, A.L.A.; Souza, B.G.; de Ataide-Silva, T.; de Oliveira, A.C.M. Validation and reproducibility of a FFQ focused on pregnant women living in Northeastern Brazil. Public Health Nutr. 2021, 24, 5769–5776. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Ruelas, É.; Bernal-Orozco, M.F.; Macedo-Ojeda, G.; Márquez-Sandoval, Y.F.; Altamirano-Martínez, M.B.; Vizmanos, B. Validation of semiquantitative FFQ administered to adults: A systematic review. Public Health Nutr. 2021, 24, 3399–3418. [Google Scholar] [CrossRef]
- Davidović Cvetko, E.; Drenjančević, I.; Jukić, I.; Stupin, A.; Šušnjara, P.; Vulin, M.; Stanojević, L. Cross-cultural adaptation and reproducibility of the EPIC-Norfolk food frequency questionnaire in young people living in Croatia. Croat. Med. J. 2024, 65, 20–29. [Google Scholar] [CrossRef]
- Rabić, D.; Sindik, J.; Missoni, S. Development and validation of a self-administered food frequency questionnaire to assess habitual dietary intake and quality of diet in healthy adults in the Republic of Croatia. Coll. Antropol. 2014, 38, 1017–1026. [Google Scholar]
- Močić Pavić, A.; Sila, S.; Niseteo, T.; Hojsak, I.; Kolaček, S. Development and Validation of a Food Frequency Questionnaire for Population of Adolescents in Croatia. Food Technol. Biotechnol. 2021, 59, 74–81. [Google Scholar] [CrossRef]
- Bountziouka, V.; Bathrellou, E.; Giotopoulou, A.; Katsagoni, C.; Bonou, M.; Vallianou, N.; Panagiotakos, D.B. Development, repeatability and validity regarding energy and macronutrient intake of a semi-quantitative food frequency questionnaire: Methodological considerations. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 659–667. [Google Scholar] [CrossRef]
- Gurinović, M.; Nikolić, M.; Zeković, M.; Milešević, J.; Kadvan, A.; Ranić, M.; Glibetić, M. Implementation of Harmonized Food Consumption Data Collection in the Balkan Region According to the EFSA EU Menu Methodology Standards. Front. Nutr. 2022, 8, 809328. [Google Scholar] [CrossRef]
- Beaton, G.H.; Milner, J.; McGuire, V.; Feather, T.E.; Little, J.A. Source of variance in 24 h dietary recall data: Implications for nutrition study design and interpretation. Carbohydrate sources, vitamins, and minerals. Am. J. Clin. Nutr. 1983, 37, 986–995. [Google Scholar] [PubMed]
- Ortiz-Andrellucchi, A.; Doreste-Alonso, J.; Henríquez-Sánchez, P.; Cetin, I.; Serra-Majem, L. Dietary assessment methods for micronutrient intake in pregnant women: A systematic review. Br. J. Nutr. 2009, 101, 1. [Google Scholar] [CrossRef]
- Ajabnoor, S.M.; Jambi, H.; Bahijri, S. Development and validation of a food frequency questionnaire in adult Saudi subjects in Jeddah city. BMC. Public Health 2024, 24, 9. [Google Scholar] [CrossRef]
- Carlsen, M.H.; Lillegaard, I.T.; Karlsen, A.; Blomhoff, R.; Drevon, C.A.; Andersen, L.F. Evaluation of energy and dietary intake estimates from a food frequency questionnaire using independent energy expenditure measurement and weighed food records. Nutr. J. 2010, 9, 37. [Google Scholar] [CrossRef]
- Beck, K.L.; Houston, Z.L.; McNaughton, S.A.; Kruger, R. Development and evaluation of a food frequency questionnaire to assess nutrient intakes of adult women in New Zealand. Nutr. Diet. 2020, 77, 253–259. [Google Scholar] [CrossRef]
- Vega-Salas, M.J.; Curi-Quinto, K.; Hidalgo-Aréstegui, A.; Meza-Carbajal, K.; Lago-Berrocal, N.; Arias, L.; Vimaleswaran, K.S. Development of an online food frequency questionnaire and estimation of misreporting of energy intake during the COVID-19 pandemic among young adults in Peru. Front. Nutr. 2022, 9, 949330. [Google Scholar] [CrossRef]
- Henriksen, H.B.; Knudsen, M.D.; Hjartåker, A.; Blomhoff, R.; Carlsen, M.H. Digital food frequency questionnaire assessing adherence to the Norwegian food-based dietary guidelines and other national lifestyle recommendations: Instrument validation study. J. Med. Internet. Res. 2024, 26, e53442. [Google Scholar] [CrossRef] [PubMed]
- Troeschel, A.N.; Hartman, T.J.; Flanders, W.D.; Wang, Y.; Hodge, R.A.; McCullough, L.E.; Mitchell, D.C.; Sampson, L.; Patel, A.V.; McCullough, M.L. The American Cancer Society Cancer Prevention Study-3 FFQ has reasonable validity and reproducibility for food groups and a diet quality score. J. Nutr. 2020, 150, 1566–1578. [Google Scholar] [CrossRef] [PubMed]
- Macdiarmid, J.; Blundell, J. Assessing dietary intake: Who, what and why of under-reporting. Nutr. Res. Rev. 1998, 11, 231–253. [Google Scholar] [CrossRef]
- Castell, G.S.; Serra-Majem, L.; Ribas-Barba, L. ¿Qué y cuánto comemos? El método recuerdo de 24 h. Rev. Esp. Nutr. Comunitaria 2015, 2, 42–44. [Google Scholar]
- Arija, V.; Abellana, R.; Ribot, B.; Ramón, J.M. Sesgos y ajustes en la valoración nutricional de las encuestas alimentarias. Rev. Esp. Nutr. Comunitaria 2015, 21, 112–117. [Google Scholar]
- Lee, H.; Kang, M.; Song, W.O.; Shim, J.E.; Paik, H.Y. Gender analysis in the development and validation of FFQ: A systematic review. Br. J. Nutr. 2016, 115, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Saravia, L.; Miguel-Berges, M.L.; Iglesia, I.; Nascimento-Ferreira, M.V.; Perdomo, G.; Bove, I.; Moreno, L.A. Relative validity of FFQ to assess food items, energy, macronutrient and micronutrient intake in children and adolescents: A systematic review with meta-analysis. Br. J. Nutr. 2021, 125, 792–818. [Google Scholar] [CrossRef]
- Tabacchi, G.; Amodio, E.; Di Pasquale, M.; Bianco, A.; Jemni, M.; Mammina, C. Validation and reproducibility of dietary assessment methods in adolescents: A systematic literature review. Public Health Nutr. 2014, 17, 2700–2714. [Google Scholar] [CrossRef]
- EUROSTAT. Overweight and Obesity—BMI Statistics. 2019. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Overweight_and_obesity_-_BMI_statistics#Obesity_in_the_EU:_gender_differences (accessed on 26 July 2024).
- Statistical Office of the Republic of Serbia. Demographic Yearbook 2022. Belgrade: Statistical Office of the Republic of Serbia. 2023. Available online: https://publikacije.stat.gov.rs/G2023/PdfE/G202314020.pdf (accessed on 26 July 2024).


{kind=link}
{kind=link}
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| n (%) | |
|---|---|
| Sex | |
| Men | 39 (41.9%) |
| Women | 54 (58.1%) |
| mean (±SD) | |
| Age (years) | 24.3 (±2.6) |
| Weight (kg) | 71.7 (±18.5) |
| Height (m) | 1.72 (0.2) |
| BMI (kg/m2) | 23.6 (±4.0) |
| n (%) | |
| Underweight (<18.5) | 7 (7.5) |
| Normal weight (18.5–24.9) | 51 (54.8) |
| Overweight (25–29.9) | 29 (31.2) |
| Obesity (≥30) | 6 (6.5) |
| Nutrient | FFQ Mean (± SD) | 24 hR * Mean (±SD) |
|---|---|---|
| Energy (kcal) | 2824.5 (1347.3) | 2288.4 (554.1) |
| Water (ml) | 1361.3 (329.3) | 1041.3 (474.0) |
| Protein (g) | 114.4 (44.4) | 102.5 (29.1) |
| Carbohydrates (g) | 294.7 (156.9) | 228.8 (72.6) |
| Fiber (g) | 33.2 (17.5) | 21.6 (9.1) |
| Fat (g) | 121.5 (67.4) | 103.9 (31.4) |
| Saturated (g) | 43.1 (24.8) | 37.5 (13.2) |
| Monounsaturated (g) | 44.8 (26.8) | 34.3 (11.1) |
| Polyunsaturated (g) | 20.7 (12.1) | 22.9 (10.2) |
| Cholesterol (mg) | 468.6 (241.6) | 479.1 (217.4) |
| Calcium (mg) | 1055.8 (475.1) | 883.3 (367.3) |
| Sodium (mg) | 3134.3 (1679.1) | 2523.7 (961.8) |
| Phosphorous (mg) | 1947.3 (783.0) | 1543.6 (496.6) |
| Vitamin B12 (µg) | 8.4 (4.3) | 8.1 (5.3) |
| Vitamin C (mg) | 207.5 (135.3) | 99.7 (67.4) |
| Vitamin D (µg) | 5.5 (4.1) | 5.9 (6.5) |
| Nutrient | Validation FFQ vs. 24 hR | |||
|---|---|---|---|---|
| Pearson Correlation Coefficient | ICC | |||
| Unadjusted b | Energy-Adjusted c | Unadjusted | Energy-Adjusted | |
| Energy (kcal) | 0.24 * | 0.13 * | ||
| Water (ml) | 0.13 | 0.07 | 0.84 | 0.13 |
| Protein (g) | 0.08 | 0.11 | 0.09 | 0.21 |
| Carbohydrates (g) | 0.32 ** | 0.23 * | 0.34 ** | 0.37 * |
| Fiber (g) | 0.08 | 0.14 | 0.01 | 0.25 |
| Fat (g) | 0.14 | 0.01 | 0.09 | 0.01 |
| Saturated (g) | 0.11 | 0.04 | 0.15 | 0.08 |
| Monounsaturated (g) | 0.16 | 0.16 | 0.24 | 0.28 |
| Polyunsaturated (g) | 0.11 | 0.04 | 0.13 | 0.08 |
| Cholesterol (mg) | 0.26 * | 0.33 * | 0.22 ** | 0.50 ** |
| Calcium (mg) | 0.07 | 0.08 | 0.07 | 0.15 |
| Sodium (mg) | 0.22 * | −0.08 | 0.01 | −0.17 |
| Phosphorous (mg) | 0.05 | 0.01 | 0.05 | 0.01 |
| Vitamin B12 (µg) | 0.25 * | 0.23 * | 0.38 * | 0.37 * |
| Vitamin C (mg) | 0.19 | 0.22 * | 0.25 * | 0.36 * |
| Vitamin D (µg) | 0.17 | 0.24 * | 0.29 | 0.49 * |
| Nutrients | Q1-24 hR and Q5-FFQ2 | Q5-24 hR and Q1-FFQ | Classified in FFQ within 1 Quintile in 24 hR |
|---|---|---|---|
| Energy (kcal) | 3.2 | 4.3 | 57.1 |
| Water (ml) | 3.2 | 3.2 | 55.9 |
| Protein (g) | 5.3 | 3.2 | 58.1 |
| Carbohydrates (g) | 2.1 | 1.1 | 66.6 |
| Fiber (g) | 5.3 | 5.3 | 49.4 |
| Fat (g) | 0.0 | 6.4 | 58.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, S.; Vidović, B.; Tijerina, A.; Tur, J.A.; Bouzas, C. Development and Evaluation of the Reliability of a Semi-Quantitative Food Frequency Questionnaire to Assess the Intake in the Serbian Population. Nutrients 2024, 16, 2490. https://doi.org/10.3390/nu16152490
Garcia S, Vidović B, Tijerina A, Tur JA, Bouzas C. Development and Evaluation of the Reliability of a Semi-Quantitative Food Frequency Questionnaire to Assess the Intake in the Serbian Population. Nutrients. 2024; 16(15):2490. https://doi.org/10.3390/nu16152490
Chicago/Turabian StyleGarcia, Silvia, Bojana Vidović, Alexandra Tijerina, Josep A. Tur, and Cristina Bouzas. 2024. "Development and Evaluation of the Reliability of a Semi-Quantitative Food Frequency Questionnaire to Assess the Intake in the Serbian Population" Nutrients 16, no. 15: 2490. https://doi.org/10.3390/nu16152490
APA StyleGarcia, S., Vidović, B., Tijerina, A., Tur, J. A., & Bouzas, C. (2024). Development and Evaluation of the Reliability of a Semi-Quantitative Food Frequency Questionnaire to Assess the Intake in the Serbian Population. Nutrients, 16(15), 2490. https://doi.org/10.3390/nu16152490