
Branched-Chain and Aromatic Amino Acids, Type 2 Diabetes, and Cardiometabolic Risk Factors among Puerto Rican Adults
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. T2D Assessment
2.3. Metabolomic Profiling
2.4. Cardiometabolic Markers
2.4.1. Measures of Glycemia
2.4.2. Measures of Dyslipidemia and Inflammation
2.4.3. Body Composition Measures
2.5. Assessment of Covariates
2.6. Statistical Analysis
3. Results
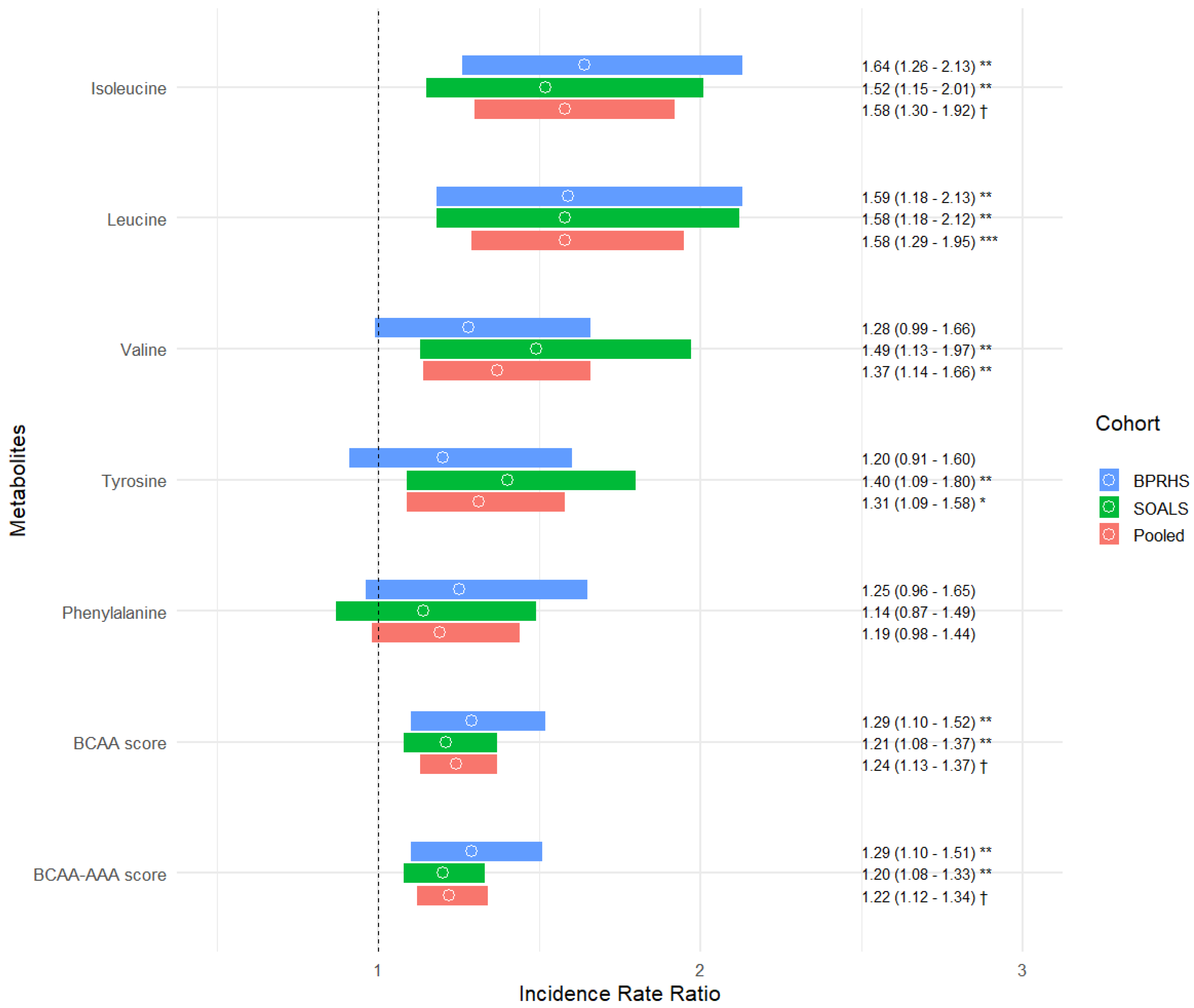
3.1. BCAAs, AAAs, and Prevalent and Incident T2D
3.2. BCAAs, AAAs, and Baseline Cardiometabolic Risk Factors
3.3. BCAAs, AAAs, and Longitudinal Changes in Cardiometabolic Risk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report Website. Available online: https://www.cdc.gov/diabetes/php/data-research/?CDC_AAref_Val=https://www.cdc.gov/diabetes/data/statistics-report/index.html (accessed on 15 July 2024).
- Koyama, A.K.; Bullard, K.M.; Onufrak, S.; Xu, F.; Saelee, R.; Miyamoto, Y.; Pavkov, M.E. Risk Factors Amenable to Primary Prevention of Type 2 Diabetes Among Disaggregated Racial and Ethnic Subgroups in the U.S. Diabetes Care 2023, 46, 2112–2119. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Gao, H.-Y.; Fan, Z.-Y.; He, Y.; Yan, Y.-X. Metabolomics Signatures in Type 2 Diabetes: A Systematic Review and Integrative Analysis. J. Clin. Endocrinol. Metab. 2020, 105, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Han, Q.; Liu, Y.; Sun, C.; Gang, X.; Wang, G. The Relationship between Branched-Chain Amino Acid Related Metabolomic Signature and Insulin Resistance: A Systematic Review. J. Diabetes Res. 2016, 2016, 2794591. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Yang, Z.; Wang, L.; Han, Y.; Peng, C.; Yan, C.; Yan, D. Metabolite Biomarkers of Type 2 Diabetes Mellitus and Pre-Diabetes: A Systematic Review and Meta-Analysis. BMC Endocr. Disord. 2020, 20, 174. [Google Scholar] [CrossRef] [PubMed]
- Morze, J.; Wittenbecher, C.; Schwingshackl, L.; Danielewicz, A.; Rynkiewicz, A.; Hu, F.B.; Guasch-Ferre, M. Metabolomics and Type 2 Diabetes Risk: An Updated Systematic Review and Meta-Analysis of Prospective Cohort Studies. Diabetes Care 2022, 45, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferré, M.; Hruby, A.; Toledo, E.; Clish, C.B.; Martínez-González, M.A.; Salas-Salvadó, J.; Hu, F.B. Metabolomics in Prediabetes and Diabetes: A Systematic Review and Meta-Analysis. Diabetes Care 2016, 39, 833–846. [Google Scholar] [CrossRef] [PubMed]
- Chai, J.C.; Chen, G.C.; Yu, B.; Xing, J.; Li, J.; Khambaty, T.; Perreira, K.M.; Perera, M.J.; Vidot, D.C.; Castaneda, S.F.; et al. Serum Metabolomics of Incident Diabetes and Glycemic Changes in a Population With High Diabetes Burden: The Hispanic Community Health Study/Study of Latinos. Diabetes 2022, 71, 1338–1349. [Google Scholar] [CrossRef] [PubMed]
- Rivas-Tumanyan, S.; Pacheco, L.S.; Haslam, D.E.; Liang, L.; Tucker, K.L.; Joshipura, K.J.; Bhupathiraju, S.N. Novel Plasma Metabolomic Markers Associated with Diabetes Progression in Older Puerto Ricans. Metabolites 2022, 12, 513. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Wang, S.; Wu, Y.; Guo, Y.; Wang, X. Baseline Serum BCAAs Are Related to the Improvement in Insulin Resistance in Obese People After a Weight Loss Intervention. Diabetes Metab. Syndr. Obes. 2023, 16, 179–186. [Google Scholar] [CrossRef]
- Zhao, H.; Shen, J.; Djukovic, D.; Daniel-MacDougall, C.; Gu, H.; Wu, X.; Chow, W.-H. Metabolomics-identified Metabolites Associated with Body Mass Index and Prospective Weight Gain among Mexican American Women. Obes. Sci. Pract. 2016, 2, 309–317. [Google Scholar] [CrossRef]
- Tucker, K.L.; Mattei, J.; Noel, S.E.; Collado, B.M.; Mendez, J.; Nelson, J.; Griffith, J.; Ordovas, J.M.; Falcon, L.M. The Boston Puerto Rican Health Study, a Longitudinal Cohort Study on Health Disparities in Puerto Rican Adults: Challenges and Opportunities. BMC Public Health 2010, 10, 107. [Google Scholar] [CrossRef] [PubMed]
- Pérez, C.M.; Muñoz, F.; Andriankaja, O.M.; Ritchie, C.S.; Martínez, S.; Vergara, J.; Vivaldi, J.; López, L.; Campos, M.; Joshipura, K.J. Cross-Sectional Associations of Impaired Glucose Metabolism Measures with Bleeding on Probing and Periodontitis. J. Clin. Periodontol. 2017, 44, 142–149. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Standards of Medical Care in Diabetes--2011. Diabetes Care 2011, 34, S11–S61. [CrossRef] [PubMed]
- Evans, A.M.; DeHaven, C.D.; Barrett, T.; Mitchell, M.; Milgram, E. Integrated, Nontargeted Ultrahigh Performance Liquid Chromatography/Electrospray Ionization Tandem Mass Spectrometry Platform for the Identification and Relative Quantification of the Small-Molecule Complement of Biological Systems. Anal. Chem. 2009, 81, 6656–6667. [Google Scholar] [CrossRef] [PubMed]
- Haslam, D.E.; Liang, L.; Wang, D.D.; Kelly, R.S.; Wittenbecher, C.; Pérez, C.M.; Martínez, M.; Lee, C.-H.; Clish, C.B.; Wong, D.T.W.; et al. Associations of Network-Derived Metabolite Clusters with Prevalent Type 2 Diabetes among Adults of Puerto Rican Descent. BMJ Open Diabetes Res. Care 2021, 9, e002298. [Google Scholar] [CrossRef] [PubMed]
- Andriankaja, O.M.; Joshipura, K.; Muñoz, F.; Dye, B.A.; Hu, F.B.; Pérez, C.M. Impact of Impaired Glucose Metabolism on Periodontitis Progression over Three Years. Dent. J. 2022, 10, 10. [Google Scholar] [CrossRef]
- Joshipura, K.J.; Muñoz-Torres, F.J.; Dye, B.A.; Leroux, B.G.; Ramírez-Vick, M.; Pérez, C.M. Longitudinal Association between Periodontitis and Development of Diabetes. Diabetes Res. Clin. Pract. 2018, 141, 284–293. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey (NHANES): Anthropometry Procedures Manual; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2007; pp. 15–16. [Google Scholar]
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.; Hill, M.N.; Jones, D.W.; Kurtz, T.; Sheps, S.G.; Roccella, E.J. Recommendations for Blood Pressure Measurement in Humans and Experimental Animals. Circulation 2005, 111, 697–716. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385. [Google Scholar] [CrossRef] [PubMed]
- Bhupathiraju, S.N.; Lichtenstein, A.H.; Dawson-Hughes, B.; Hannan, M.T.; Tucker, K.L. Adherence to the 2006 American Heart Association Diet and Lifestyle Recommendations for Cardiovascular Disease Risk Reduction Is Associated with Bone Health in Older Puerto Ricans. Am. J. Clin. Nutr. 2013, 98, 1309–1316. [Google Scholar] [CrossRef] [PubMed]
- Tucker, K.L.; Bianchi, L.A.; Maras, J.; Bermudez, O.I. Adaptation of a Food Frequency Questionnaire to Assess Diets of Puerto Rican and Non-Hispanic Adults. Am. J. Epidemiol. 1998, 148, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Bhupathiraju, S.N.; Guasch-Ferré, M.; Gadgil, M.D.; Newgard, C.B.; Bain, J.R.; Muehlbauer, M.J.; Ilkayeva, O.R.; Scholtens, D.M.; Hu, F.B.; Kanaya, A.M.; et al. Dietary Patterns among Asian Indians Living in the United States Have Distinct Metabolomic Profiles That Are Associated with Cardiometabolic Risk. J. Nutr. 2018, 148, 1150–1159. [Google Scholar] [CrossRef] [PubMed]
- Cook RD Detection of Influential Observation in Linear Regression. Technometrics 1977, 19, 15–18. [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Yekutieli, D. The Control of the False Discovery Rate in Multiple Testing under Dependency. Ann. Stat. 2001, 29, 1165–1188. [Google Scholar] [CrossRef]
- Lotta, L.A.; Scott, R.A.; Sharp, S.J.; Burgess, S.; Luan, J.; Tillin, T.; Schmidt, A.F.; Imamura, F.; Stewart, I.D.; Perry, J.R.B.; et al. Genetic Predisposition to an Impaired Metabolism of the Branched-Chain Amino Acids and Risk of Type 2 Diabetes: A Mendelian Randomisation Analysis. PLoS Med. 2016, 13, e1002179. [Google Scholar] [CrossRef]
- Porcu, E.; Gilardi, F.; Darrous, L.; Yengo, L.; Bararpour, N.; Gasser, M.; Marques-Vidal, P.; Froguel, P.; Waeber, G.; Thomas, A.; et al. Triangulating Evidence from Longitudinal and Mendelian Randomization Studies of Metabolomic Biomarkers for Type 2 Diabetes. Sci. Rep. 2021, 11, 6197. [Google Scholar] [CrossRef]
- Moon, J.; Kim, O.; Jo, G.; Shin, M.-J. Alterations in Circulating Amino Acid Metabolite Ratio Associated with Arginase Activity Are Potential Indicators of Metabolic Syndrome: The Korean Genome and Epidemiology Study. Nutrients 2017, 9, 740. [Google Scholar] [CrossRef] [PubMed]
- Melnik, B.C. Leucine Signaling in the Pathogenesis of Type 2 Diabetes and Obesity. World J. Diabetes 2012, 3, 38. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.; Krssak, M.; Bernroider, E.; Anderwald, C.; Brehm, A.; Meyerspeer, M.; Nowotny, P.; Roth, E.; Waldhausl, W.; Roden, M. Mechanism of Amino Acid-Induced Skeletal Muscle Insulin Resistance in Humans. Diabetes 2002, 51, 599–605. [Google Scholar] [CrossRef] [PubMed]
- De Bandt, J.P.; Coumoul, X.; Barouki, R. Branched-Chain Amino Acids and Insulin Resistance, from Protein Supply to Diet-Induced Obesity. Nutrients 2022, 15, 68. [Google Scholar] [CrossRef] [PubMed]
- Stančáková, A.; Civelek, M.; Saleem, N.K.; Soininen, P.; Kangas, A.J.; Cederberg, H.; Paananen, J.; Pihlajamäki, J.; Bonnycastle, L.L.; Morken, M.A.; et al. Hyperglycemia and a Common Variant of GCKR Are Associated with the Levels of Eight Amino Acids in 9,369 Finnish Men. Diabetes 2012, 61, 1895–1902. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, H.K.; Gudmundsdottir, V.; Nielsen, H.B.; Hyotylainen, T.; Nielsen, T.; Jensen, B.A.H.; Forslund, K.; Hildebrand, F.; Prifti, E.; Falony, G.; et al. Human Gut Microbes Impact Host Serum Metabolome and Insulin Sensitivity. Nature 2016, 535, 376–381. [Google Scholar] [CrossRef]
- Ejtahed, H.-S.; Angoorani, P.; Soroush, A.-R.; Hasani-Ranjbar, S.; Siadat, S.-D.; Larijani, B. Gut Microbiota-Derived Metabolites in Obesity: A Systematic Review. Biosci. Microbiota. Food Health 2020, 39, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Hamaya, R.; Mora, S.; Lawler, P.R.; Cook, N.R.; Ridker, P.M.; Buring, J.E.; Lee, I.M.; Manson, J.E.; Tobias, D.K. Association of Plasma Branched-Chain Amino Acid With Biomarkers of Inflammation and Lipid Metabolism in Women. Circ. Genom. Precis. Med. 2021, 14, E003330. [Google Scholar] [CrossRef]
- Moore, S.C.; Matthews, C.E.; Sampson, J.N.; Stolzenberg-Solomon, R.Z.; Zheng, W.; Cai, Q.; Tan, Y.T.; Chow, W.-H.; Ji, B.-T.; Liu, D.K.; et al. Human Metabolic Correlates of Body Mass Index. Metabolomics 2014, 10, 259–269. [Google Scholar] [CrossRef]
- Newgard, C.B.; An, J.; Bain, J.R.; Muehlbauer, M.J.; Stevens, R.D.; Lien, L.F.; Haqq, A.M.; Shah, S.H.; Arlotto, M.; Slentz, C.A.; et al. A Branched-Chain Amino Acid-Related Metabolic Signature That Differentiates Obese and Lean Humans and Contributes to Insulin Resistance. Cell Metab. 2009, 9, 311–326. [Google Scholar] [CrossRef]
- Hamaya, R.; Mora, S.; Lawler, P.R.; Cook, N.R.; Buring, J.E.; Lee, I.M.; Manson, J.E.; Tobias, D.K. Association of Modifiable Lifestyle Factors with Plasma Branched-Chain Amino Acid Metabolites in Women. J. Nutr. 2022, 152, 1515–1524. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| BPRHS (n = 670) | SOALS (n = 999) | |
|---|---|---|
| Mean (±SD) or n (%) | Mean (±SD) or n (%) | |
| Age, years | 57.2 (±7.41) | 50.7 (±6.77) |
| Female | 502 (74.9) | 729 (73.0) |
| Total income, USD/dollars | 18,003 (±18,221) | - |
| <20,000 | - | 543 (54.4) |
| 20,000–49,999 | - | 338 (33.8) |
| ≥50,000 | - | 118 (11.8) |
| Education | ||
| No schooling–7th to 8th grade | 336 (50.2) | 113 (11.3) |
| 9th–12th grade | 237 (35.4) | 439 (43.9) |
| Some college or more | 97 (14.5) | 447 (44.7) |
| Smoking status | ||
| Never | 315 (47.0) | 639 (64.0) |
| Past | 204 (30.5) | 179 (17.9) |
| Current | 151 (22.5) | 181 (18.1) |
| Alcohol consumption | ||
| Never/abstainer | 203 (30.3) | 442 (44.2) |
| Past | 197 (29.4) | 113 (11.3) |
| Current | 270 (40.3) | 444 (44.4) |
| Multivitamin supplement use, yes | 134 (20.0) | - |
| Statin or lipid-lowering medication use, yes | 295 (44.0) | 85 (8.51) |
| Hypertension medication use, yes | 376 (56.1) | 267 (26.7) |
| BMI, kg/m2 | 32.2 (±6.67) | 33.3 (±6.17) |
| Waist circumference, cm | 102 (±14.9) | 106 (±14.0) |
| LDL cholesterol, mg/dL | 108 (±34.4) | 123 (±32.7) |
| HDL cholesterol, mg/dL | 45.2 (±12.4) | 48.1 (±13.1) |
| Triglycerides, mg/dL | 162 (±112) | 149 (±83.7) |
| Glucose, mg/dL | 120 (±50.2) | 95.8 (±20.2) |
| Hemoglobin A1c, % | 7.00 (±1.78) | 5.80 (±0.62) |
| HOMA-IR | 6.06 (±9.99) | 2.62 (±1.83) |
| Insulin, mcU/mL | 18.8 (±26.2) | 10.8 (±6.83) |
| C-reactive protein, mg/L | 6.36 (±8.83) | 5.92 (±6.32) |
| Type 2 diabetes, yes | 354 (52.84) | 75 (7.51) |
| Systolic blood pressure, mmHg | 136 (±18.8) | 129 (±17.1) |
| Diastolic blood pressure, mmHg | 81.5 (±10.7) | 80.9 (±9.67) |
| Physical activity | 31.4 (±4.40) | 22.0 (±39.7) |
| Alcohol, g/d | 4.05 (±15.4) | 2.36 (±5.82) |
| AHA diet score | 8.70 (±2.04) | - |
| Psychosocial stress score | 23.4 (±9.67) | - |
| Cultural acculturation score | 22.6 (±21.2) | - |
| 2 YEAR CHANGES IN GLYCEMIC MEASURES | ||||
| Metabolite | Δ HOMA-IR | Δ Insulin, mcU/mL | Δ Glucose, mg/dL | Δ HbA1c, % |
| Isoleucine | 0.07 (−0.03; 0.17) | 0.28 (0.03; 0.54) | 0.89 (0.22; 1.56) | 0.02 (−0.001; 0.04) |
| Leucine | 0.09 (−0.008; 0.19) | 0.37 (0.11; 0.63) * | 0.78 (0.09; 1.46) | 0.02 (−0.004; 0.04) |
| Valine | 0.09 (−0.003; 0.19) | 0.43 (0.17; 0.68) ** | 0.67 (0.02; 1.33) | 0.01 (−0.01; 0.03) |
| Phenylalanine | 0.04 (−0.05; 0.14) | 0.24 (−0.01; 0.48) | 0.01 (−0.63; 0.65) | 0.01 (−0.01; 0.03) |
| Tyrosine | 0.13 (0.04; 0.22) * | 0.37 (0.12; 0.61) * | 0.36 (−0.28; 1.00) | 0.01 (−0.01; 0.03) |
| BCAA score a | 0.04 (−0.001; 0.08) | 0.18 (0.06; 0.30) * | 0.36 (0.06; 0.67) | 0.01 (−0.003; 0.02) |
| BCAA-AAA score b | 0.04 (0.01; 0.08) | 0.19 (0.08; 0.30) ** | 0.30 (0.03; 0.58) | 0.01 (−0.003; 0.01) |
| 2 YEAR CHANGES IN DYSLIPIDEMIA AND INFLAMMATION MEASURES | ||||
| Metabolite | Δ HDL−C, mg/dL | Δ LDL−C, mg/dL | Δ Triglycerides, mg/dL | Δ CRP, mg/L |
| Isoleucine | −0.19 (−0.41; 0.03) | −0.03 (−0.78; 0.73) | 1.62 (−0.22; 3.46) | −0.05 (−0.24; 0.14) |
| Leucine | −0.28 (−0.51; −0.05) | −0.13 (−0.90; 0.65) | 1.62 (−0.27; 3.51) | −0.08 (−0.28; 0.11) |
| Valine | −0.24 (−0.46; −0.02) | 0.02 (−0.74; 0.77) | 1.31 (−0.5; 3.13) | 0.01 (−0.17; 0.20) |
| Phenylalanine | −0.21 (−0.42; 0.01) | −0.24 (−0.97; 0.50) | 0.33 (−1.43; 2.09) | −0.11 (−0.30; 0.08) |
| Tyrosine | 0.04 (−0.18; 0.25) | −0.26 (−0.99; 0.48) | −0.18 (−1.95; 1.58) | −0.07 (−0.25; 0.11) |
| BCAA score a | −0.15 (−0.27; −0.03) | 0.01 (−0.38; 0.40) | 0.90 (−0.03; 1.83) | −0.01 (−0.11; 0.08) |
| BCAA-AAA score b | −0.14 (−0.25; −0.03) | −0.02 (−0.38; 0.34) | 0.77 (−0.09; 1.63) | −0.01 (−0.10; 0.07) |
| 2 YEAR CHANGES IN ANTHROPOMETRIC MEASURES | ||||
| Metabolite | Δ Waist Circumference, cm | Δ BMI | Δ Weight, kg | |
| Isoleucine | 0.10 (−0.20; 0.39) | −0.09 (−0.17; −0.01) | −0.15 (−0.38; 0.09) | |
| Leucine | 0.16 (−0.14; 0.47) | −0.08 (−0.16; 0.005) | −0.07 (−0.31; 0.18) | |
| Valine | 0.15 (−0.14; 0.44) | −0.03 (−0.11; 0.05) | 0.05 (−0.18; 0.29) | |
| Phenylalanine | 0.37 (0.08; 0.65) | −0.06 (−0.14; 0.02) | −0.04 (−0.27; 0.19) | |
| Tyrosine | 0.30 (0.02; 0.58) | −0.02 (−0.10; 0.06) | −0.12 (−0.35; 0.12) | |
| BCAA score a | 0.08 (−0.06; 0.22) | −0.04 (−0.08; 0.0002) | −0.04 (−0.18; 0.09) | |
| BCAA-AAA score b | 0.09 (−0.04; 0.22) | −0.04 (−0.08; −0.001) | −0.05 (−0.18; 0.08) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivas-Tumanyan, S.; Pacheco, L.S.; Haslam, D.E.; Morou-Bermudez, E.; Liang, L.; Tucker, K.L.; Joshipura, K.J.; Bhupathiraju, S.N. Branched-Chain and Aromatic Amino Acids, Type 2 Diabetes, and Cardiometabolic Risk Factors among Puerto Rican Adults. Nutrients 2024, 16, 2562. https://doi.org/10.3390/nu16152562
Rivas-Tumanyan S, Pacheco LS, Haslam DE, Morou-Bermudez E, Liang L, Tucker KL, Joshipura KJ, Bhupathiraju SN. Branched-Chain and Aromatic Amino Acids, Type 2 Diabetes, and Cardiometabolic Risk Factors among Puerto Rican Adults. Nutrients. 2024; 16(15):2562. https://doi.org/10.3390/nu16152562
Chicago/Turabian StyleRivas-Tumanyan, Sona, Lorena S. Pacheco, Danelle E. Haslam, Evangelia Morou-Bermudez, Liming Liang, Katherine L. Tucker, Kaumudi J. Joshipura, and Shilpa N. Bhupathiraju. 2024. "Branched-Chain and Aromatic Amino Acids, Type 2 Diabetes, and Cardiometabolic Risk Factors among Puerto Rican Adults" Nutrients 16, no. 15: 2562. https://doi.org/10.3390/nu16152562