
Vitamin D and Its Role on the Fatigue Mitigation: A Narrative Review
 ,
,  ,
,  , and
, and 
{kind=link}
{kind=link}
Abstract
1. The Fatigue
2. Vitamin D
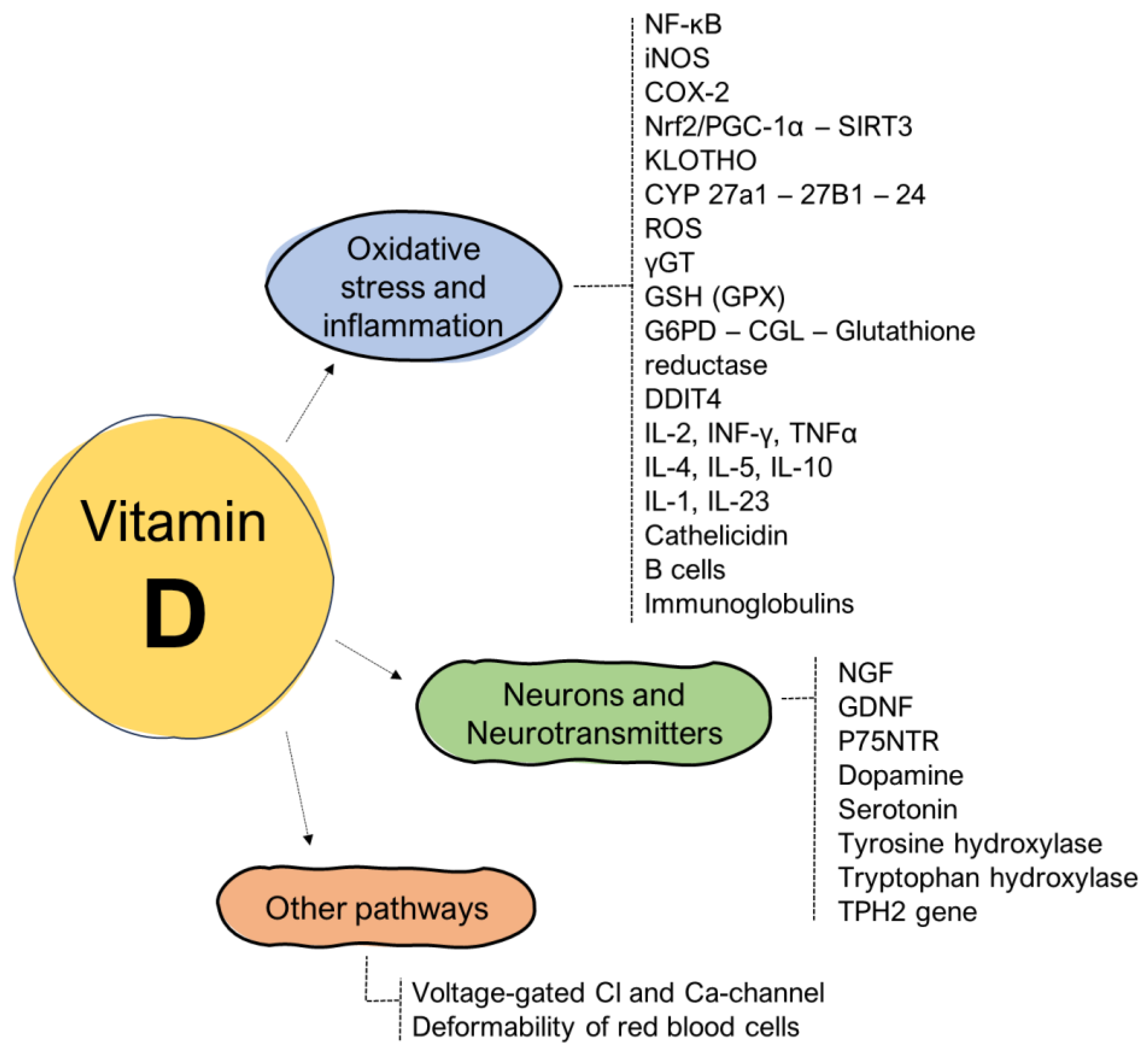
2.1. Vitamin D’s Impact on the Cytokines: Oxidative Stress and Inflammation
2.2. Vitamin D’s Interaction with Neurotransmitters
2.3. Vitamin D’s Impact on Other Molecular Pathways
3. Hypovitaminosis D: Causes, Symptoms, and Impact on Fatigue
3.1. The Point of View of Fibromyalgia
3.2. The Point of View of Multiple Sclerosis
3.3. The Point of View of Rheumatological Diseases
3.4. The Point of View of Myasthenia Gravis
3.5. The Point of View of Elderly Age
3.6. The Point of View of Cancer
3.7. The Point of View of Chronic Fatigue Syndrome
3.8. The Point of View of Parkinson’s Disease
3.9. The Point of View of Neuropsychiatric Diseases
3.10. The Point of View of Musculoskeletal Disorders
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gandevia, S.C. Spinal and supraspinal factors in human muscle fatigue. Physiol. Rev. 2001, 81, 1725–1789. [Google Scholar] [CrossRef] [PubMed]
- Engberg, I.; Segerstedt, J.; Waller, G.; Wennberg, P.; Eliasson, M. Fatigue in the general population-associations to age, sex, socioeconomic status, physical activity, sitting time and self-rated health: The northern Sweden MONICA study 2014. BMC Public Health 2017, 17, 654. [Google Scholar] [CrossRef] [PubMed]
- Behrens, M.; Gube, M.; Chaabene, H.; Prieske, O.; Zenon, A.; Broscheid, K.C.; Schega, L.; Husmann, F.; Weippert, M. Fatigue and human performance: An updated framework. Sports Med. 2023, 53, 7–31. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, A.; Behan, P.O. Fatigue in neurological disorders. Lancet 2004, 363, 978–988. [Google Scholar] [CrossRef]
- Zielinski, M.R.; Systrom, D.M.; Rose, N.R. Fatigue, sleep, and autoimmune and related disorders. Front. Immunol. 2019, 10, 1827. [Google Scholar] [CrossRef]
- Cardwell, G.; Bornman, J.F.; James, A.P.; Black, L.J. A review of mushrooms as a potential source of dietary vitamin D. Nutrients 2018, 10, 1498. [Google Scholar] [CrossRef]
- Gombart, A.F. Vitamin D. Micronutrient Information Center, Linus Pauling Institute, Oregon State University, Corvallis, 11 February 2021. Available online: https://lpi.oregonstate.edu/mic/vitamins/vitamin-D (accessed on 12 September 2023).
- Benedik, E. Sources of vitamin D for Humans. Int. J. Vitam. Nutr. Res. 2022, 92, 118–125. [Google Scholar] [CrossRef]
- Sintzel, M.B.; Rametta, M.; Reder, A.T. Vitamin D and multiple sclerosis: A comprehensive review. Neurol. Ther. 2018, 7, 59–85. [Google Scholar] [CrossRef]
- Bikle, D.D. Vitamin D metabolism, mechanism of action, and clinical applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef]
- Norman, A.W. From vitamin D to hormone D: Fundamentals of the vitamin D endocrine system essential for good health. Am. J. Clin. Nutr. 2008, 88, 491S–499S. [Google Scholar] [CrossRef]
- Webb, A.R.; DeCosta, B.R.; Holick, M.F. Sunlight regulates the skin production of vitamin D3 by causing its photodegradation. J. Clin. Endocrinol. Metab. 1989, 68, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Chun, R.F.; Hernandez, I.; Pereira, R.; Swinkles, L.; Huijs, T.; Zhou, R.; Liu, N.Q.; Shieh, A.; Guemes, M.; Mallya, S.M.; et al. Differential responses to vitamin D2 and vitamin D3 are associated with variations in free 25-hydroxyvitamin D. Endocrinology 2016, 157, 3420–3430. [Google Scholar] [CrossRef] [PubMed]
- Pike, J.W.; Meyer, M.B. The vitamin D receptor: New paradigms for the regulation of gene expression by 1,25-Dihydoxyvitamin D3. Endocrinol. Metab. Clin. N. Am. 2010, 39, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Bischoff-Ferrari, H.; Willett, W. Vitamin D and health: Mouse and human perspectives. J. Bone Miner. Res. 2009, 23, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Mizwicki, M.T.; Norman, A.W. Vitamin D Sterol Conformational Dynamics/VDR and Non-Genomic Actions. In Vitamin D, 3rd ed.; Feldman, D., Pike, J.W., Adams, J.S., Eds.; Academic Press: New York, NY, USA, 2011; pp. 271–297. [Google Scholar]
- Lee, J.S.; Kim, H.G.; Lee, D.S.; Son, C.G. Oxidative stress is a convincing contributor to idiopathic chronic fatigue. Sci. Rep. 2018, 8, 12890. [Google Scholar] [CrossRef] [PubMed]
- Chudapongse, P.; Lowchareonkul, S. The in vitro effects of vitamin D on oxidative phosphorylation and adenosine triphosphatase activity by mitochondria of rat liver. Biochem. Pharmacol. 1975, 24, 2127–2132. [Google Scholar] [CrossRef] [PubMed]
- Hoeck, A.D. Vitamin D3 deficiency results in dysfunctions of immunity with severe fatigue and depression in a variety of diseases. In Vivo 2014, 28, 133–145. [Google Scholar]
- Sinha, A.; Hollingsworth, K.G.; Ball, S.; Cheetham, T. Improving the vitamin D status of vitamin D deficient adults is associated with improved mitochondrial oxidative function in skeletal muscle. J. Clin. Endocrinol. Metab. 2013, 98, E509–E513. [Google Scholar] [CrossRef]
- Maes, M. Inflammatory and oxidative and nitrosative stress pathways underpinning chronic fatigue, somatization and psychosomatic symptoms. Curr. Opin. Psychiatry 2009, 22, 75–83. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Vitamin D deficiency: Effects on oxidative stress, epigenetics, gene regulation, and aging. Biology 2019, 8, 30. [Google Scholar] [CrossRef]
- Berridge, M.J. Vitamin D cell signaling in Health and Disease. Biochem. Biophys. Res. Commun. 2015, 460, 53–71. [Google Scholar] [CrossRef] [PubMed]
- Marcus, J.M.; Andrabi, S.A. SIRT3 regulation under cellular stress: Making sense of the ups and downs. Front. Neurosci. 2018, 12, 799. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K.N.; Mele, J.; Hayes, J.D.; Buffenstein, R. Nrf2, a guardian of healthspan and gatekeeper of species longevity. Integr. Comp. Biol. 2010, 50, 829–843. [Google Scholar] [CrossRef]
- Kim, A.; Koo, J.H.; Lee, J.M.; Joo, M.S.; Kim, T.H.; Kim, H.; Jun, D.W.; Kim, S.G. NRF2-mediated SIRT3 induction protects hepatocytes from ER stress-induced liver injury. FASEB J. 2022, 36, e22170. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Clark, J.D.; Pastor, J.V.; Gurnani, P.; Nandi, A.; Kurosu, H.; Miyoshi, M.; Ogawa, Y.; Castrillon, D.H.; Rosenblatt, K.P.; et al. Regulation of Oxidative Stress by the Anti-aging Hormone Klotho. J. Biol. Chem. 2005, 280, 38029–38034. [Google Scholar] [CrossRef] [PubMed]
- Ricca, C.; Aillon, A.; Bergandi, L.; Alotto, D.; Castagnoli, C.; Silvagno, F. The vitamin D receptor is required for mitochondrial function and cellular health. Int. J. Mol. Sci. 2018, 19, 1672. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Hyde, A.S.; Simpson, M.A.; Barycki, J.J. Emerging adjustment paradigms in glutathione metabolic. Adv. Cancer Res. 2014, 122, 69–101. [Google Scholar]
- Carlberg, C. Nutrigenomics of vitamin D. Nutrients 2019, 11, 676. [Google Scholar] [CrossRef]
- Koivisto, O.; Hanel, A.; Carlberg, C. Key vitamin D target genes with functions in the immune system. Nutrients 2020, 12, 1140. [Google Scholar] [CrossRef]
- Nguyen, M.H.; Bryant, K.; O’Neill, S.G. Vitamin D in SLE: A role in pathogenesis and fatigue? A review of the literature. Lupus 2018, 27, 2003–2011. [Google Scholar] [CrossRef]
- Carlberg, C. Vitamin D signaling in the context of innate immune: Focus on human monocitis. Front. Immunol. 2019, 10, 2211. [Google Scholar] [CrossRef] [PubMed]
- Skrobot, A.; Demkow, U.; Wachowska, M. Immunomodulatory role of vitamin A: A review. Adv. Exp. Med. Biol. 2018, 1108, 13–23. [Google Scholar] [PubMed]
- Ao, T.; Kikuta, J.; Ishii, M. The effects of vitamin D on immune system and inflammatory diseases. Biomolecules 2021, 11, 1624. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M. Vitamin D and autoimmune rheumatic diseases. Rheumatology 2009, 48, 210–212. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dobryakova, E.; Genova, H.M.; DeLuca, J.; Wylie, G.R. The dopamine imbalance hypothesis of fatigue in multiple sclerosis and other neurological disorders. Front. Neurol. 2015, 6, 52. [Google Scholar] [CrossRef]
- Gezen-Ak, D.; Dursun, E.; Yilmazer, S. The effect of vitamin D treatment on nerve growth factor (NGF) release from hippocampal neurons. Nöro Psikiyatr. Arşivi 2014, 51, 157. [Google Scholar] [CrossRef] [PubMed]
- Riaz, S.; Malcangio, M.; Miller, M.; Tomlinson, D.R. A vitamin D3 derivative (CB1093) induces nerve growth factor and prevents neurotrophic deficits in streptozotocin-diabetic rats. Diabetologia 1999, 42, 1308–1313. [Google Scholar] [CrossRef] [PubMed]
- Dechant, G.; Barde, Y.A. The neurotrophin receptor p75NTR: Novel functions and implications for diseases of the nervous system. Nat. Neurosci. 2002, 5, 1131–1136. [Google Scholar] [CrossRef]
- Eyles, D.; Brown, J.; Mackay-Sim, A.; McGrath, J.; Feron, F. Vitamin D3 and brain development. Neuroscience 2003, 118, 641–653. [Google Scholar] [CrossRef]
- Cordeiro, L.M.S.; Rabelo, P.C.R.; Moraes, M.M.; Teixeira-Coelho, F.; Coimbra, C.C.; Wanner, S.P.; Soares, D.D. Physical exercise-induced fatigue: The role of serotonergic and dopaminergic systems. Braz. J. Med. Biol. 2017, 50, e6432. [Google Scholar] [CrossRef]
- Cui, X.; Gooch, H.; Groves, N.J.; Sah, P.; Burne, T.H.; Eyles, D.W.; McGrath, J.J. Vitamin D and the brain: Key questions for future research. J. Steroid Biochem. Mol. Biol. 2015, 148, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Weissenborn, K.; Ennen, J.C.; Bokemeyer, M.; Ahl, B.; Wurster, U.; Tillmann, H.; Trebst, C.; Hecker, H.; Berding, G. Monoaminergic neurotransmission is altered in hepatitis C virus infected patients with chronic fatigue and cognitive impairment. BMJ 2006, 55, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Kostić, V.S.; Tomić, A.; Ječmenica-Lukić, M. The pathophysiology of fatigue in Parkinson’s disease and its pragmatic management. Mov. Disord. Clin. Pract. 2016, 3, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Pertile, R.A.N.; Brigden, R.; Raman, V.; Cui, X.; Du, Z.; Eyles, D. Vitamin D: A potent regulator of dopaminergic neuron differentiation and function. J. Neurochem. 2023, 166, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Orme, R.P.; Middleditch, C.; Waite, L.; Fricker, R.A. The role of vitamin D3 in the development and neuroprotection of midbrain dopamine neurons. Vitam. Horm. 2016, 100, 273–297. [Google Scholar] [PubMed]
- Seyedi, M.; Gholami, F.; Samadi, M.; Djalali, M.; Effatpanah, M.; Yekaninejad, M.S.; Hashemi, R.; Abdolahi, M.; Chamari, M.; Honarvar, N.M. The effect of vitamin D3 supplementation on serum BDNF, dopamine, and serotonin in children with attention-deficit/hyperactivity disorder. CNS Neurol. Disord. Drug Targets 2019, 18, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Zawadzka, K.; Matwiej, K.; Sokołowski, G.; Trofimiuk-Müldner, M.; Skalniak, A.; Hubalewska-Dydejczyk, A. Vitamin D status and its associations with clinical and laboratory parameters in patients with Addison’s disease. Folia Medica Cracoviensia 2021, 61, 65–78. [Google Scholar] [CrossRef] [PubMed]
- Eyles, D.W.; Burne, T.H.; McGrath, J.J. Vitamin D, effects on brain development, adult brain function and the links between low levels of vitamin D and neuropsychiatric disease. Front. Neuroendocrinol. 2013, 34, 47–64. [Google Scholar] [CrossRef]
- Kaneko, I.; Sabir, M.S.; Dussik, C.M.; Whitfield, G.K.; Karrys, A.; Hsieh, J.C.; Haussier, M.R.; Meyer, M.B.; Pike, J.W.; Jurutka, P.W. 1, 25-Dihydroxyvitamin D regulates expression of the tryptophan hydroxylase 2 and leptin genes: Implication for behavioral influences of vitamin D. FASEB J. 2015, 29, 4023–4035. [Google Scholar] [CrossRef]
- Yamamoto, S.; Ouchi, Y.; Onoe, H.; Yoshikawa, E.; Tsukada, H.; Takahashi, H.; Iwase, M.; Yamaguti, K.; Kuratsune, H.; Watanabe, Y. Reduction of serotonin transporters of patients with chronic fatigue syndrome. Neuroreport 2004, 15, 2571–2574. [Google Scholar] [CrossRef]
- Patrick, R.P.; Ames, B.N. Vitamin D and the omega-3 fatty acids control serotonin synthesis and action, part 2: Relevance for ADHD, bipolar disorder, schizophrenia, and impulsive behavior. FASEB J. 2015, 29, 2207–2222. [Google Scholar] [CrossRef]
- Pratiwi, S.E.; Sukmawati, F. Vitamin D and Serotonin’s Role in Neuropsychiatric Disorders. J. Studi Gend. Dan. Anak 2020, 114, 114–128. [Google Scholar]
- Brewer, L.D.; Thibault, V.; Chen, K.C.; Langub, M.C.; Landfield, P.W.; Porter, N.M. Vitamin D hormone confers neuroprotection in parallel with downregulation of L-type calcium channel expression in hippocampal neurons. J. Neurosci. 2001, 21, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Menegaz, D.; Mizwicki, M.T.; Barrientos-Duran, A.; Chen, N.; Henry, H.L.; Norman, A.W. Vitamin D receptor (VDR) regulation of voltage-gated chloride channels by ligands preferring a VDR-alternative pocket (VDR-AP). Mol. Endocrinol. 2011, 25, 1289–1300. [Google Scholar] [CrossRef] [PubMed]
- Zanello, L.P.; Norman, A.W. Stimulation by 1α, 25 (OH) 2-vitamin D3 of whole cell chloride currents in osteoblastic ROS 17/2.8 cells: A structure-function study. J. Biol. Chem. 1997, 272, 22617–22622. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pennisi, M.; Malaguarnera, G.; Di Bartolo, G.; Lanza, G.; Bella, R.; Chisari, E.M.; Cauli, O.; Vicari, E.; Malaguarnera, M. Decrease in serum vitamin D level of older patients with fatigue. Nutrients 2019, 11, 2531. [Google Scholar] [CrossRef]
- Entezari-Maleki, T.; Talasaz, A.H.; Salarifar, M.; Hadjibabaie, M.; Javadi, M.R.; Bozorgi, A.; Jenab, Y.; Boroumand, M.A.; Gholami, K. Plasma vitamin D status and its correlation with risk factors of thrombosis, P-selectin and hs-CRP level in patients with venous thromboembolism; the first study of Iranian population. Iran. J. Pharm. Res. IJPR 2014, 13, 319. [Google Scholar] [PubMed]
- De Metrio, M.; Milazzo, V.; Rubino, M.; Cabiati, A.; Moltrasio, M.; Marana, I.; Campodonico, J.; Cosentino, N.; Veglia, F.; Bonomi, A.; et al. Vitamin D plasma levels and in-hospital and 1-year outcomes in acute coronary syndromes: A prospective study. Medicine 2015, 94, e857. [Google Scholar] [CrossRef]
- Tsiaras, W.G.; Weinstock, A.M. Factors affecting vitamin D status. Acta Derm. Venereol. 2011, 91, 115–124. [Google Scholar] [CrossRef]
- Pilz, S.; Marz, W.; Wellnitz, B.; Seelhorst, U.; Fahrleitner-Pammer, A.; Dimai, H.P.; Boehm, B.O.; Dobnig, H. Association of vitamin D deficiency with heart failure and sudden cardiac death in a large cross-sectional study of patients referred for coronary angiography. J. Clin. Endocrinol. Metab. 2008, 93, 3927–3935. [Google Scholar] [CrossRef]
- Cohen, M.C.; Offiah, A.; Sprigg, A.; Al-Adnani, M. Vitamin D deficiency and sudden unexpected death in infancy and childhood: A cohort study. Pediatr. Dev. Pathol. 2013, 16, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.Q.; Reddy, P.S.; Kimler, B.F.; Sharma, P.; Baxa, S.E.; O’Dea, A.P.; Klemp, J.R.; Fabian, C.J. Effect of vitamin D supplementation on serum 25-hydroxy vitamin D levels, joint pain, and fatigue in women starting adjuvant letrozole treatment for breast cancer. Breast Cancer Res. Treat. 2010, 119, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Knutsen, K.V.; Brekke, M.; Gjelstad, S.; Lagerløv, P. Vitamin D status in patients with musculoskeletal pain, fatigue and headache: A cross-sectional descriptive study in a multi-ethnic general practice in Norway. Scand. J. Prim. Health Care 2010, 28, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Bilal, A.; Khan, S.; Iqbal, M.I.; Qureshi, F.S.; Fazal, M.O.; Shaheen, M.; Iqbal, S. Effect of vitamin D replacement in patients of fibromyalgia. Ann. Punjab Med. Coll. (APMC) 2009, 3, 51–58. [Google Scholar]
- Daniel, D.; Pirotta, M.V. Fibromyalgia: Should we be testing and treating for vitamin D deficiency? Aust. Fam. Physician 2011, 40, 712–716. [Google Scholar] [PubMed]
- Solmaz, D.; Avci, O.; Yalcin, B.C.; Kara, S.P.; Oran, M. AB0944 Vitamin D Deficiency Might. Contribute Fatigue and Disease Activity in Patients with Fibromyalgia. Ann. Rheum. Dis. 2015, 74, 1215. [Google Scholar]
- Lombardo, M.; Feraco, A.; Ottaviani, M.; Rizzo, G.; Camajani, E.; Caprio, M.; Armani, A. The efficacy of vitamin D supplementation in the treatment of fibromyalgia syndrome and chronic musculoskeletal pain. Nutrients 2022, 14, 3010. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef]
- Knippenberg, S.; Damoiseaux, J.; Bol, Y.; Hupperts, R.; Taylor, B.V.; Ponsonby, A.L.; Dwyer, T.; Simpson, S.; Van Der Mei, I.A.F. Higher levels of reported sun exposure, and not vitamin D status, are associated with less depressive symptoms and fatigue in multiple sclerosis. Acta Neurol. Scand. 2014, 129, 123–131. [Google Scholar] [CrossRef]
- Beckmann, Y.; Türe, S.; Duman, S.U. Vitamin D deficiency and its association with fatigue and quality of life in multiple sclerosis patients. EPMA J. 2020, 11, 65–72. [Google Scholar] [CrossRef]
- López-Muñoz, P.; Torres-Costoso, A.I.; Fernández-Rodríguez, R.; Guzmán-Pavón, M.J.; de Arenas-Arroyo, S.N.; Basco-López, J.Á.; Reina-Gutiérrez, S. Effect of Vitamin D Supplementation on Fatigue in Multiple Sclerosis: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2861. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Irastorza, G.; Gordo, S.; Olivares, N.; Egurbide, M.V.; Aguirre, C. Changes in vitamin D levels in patients with systemic lupus erythematosus: Effects on fatigue, disease activity, and damage. Arthritis Care Res. 2010, 62, 1160–1165. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Sherman, A.; Monari-Sparks, M.J.; Schweiker, O.; Hunter, K. Correction of low vitamin D improves fatigue: Effect of correction of low vitamin D in fatigue study (EViDiF Study). N. Am. J. Med. Sci. 2014, 6, 396. [Google Scholar] [CrossRef] [PubMed]
- Jelsness-Jørgensen, L.P.; Grovle, L.; Haugen, A.J. Association between vitamin D and fatigue in patients with rheumatoid arthritis: A cross-sectional study. BMJ 2020, 10, e034935. [Google Scholar] [CrossRef] [PubMed]
- Askmark, H.; Haggard, A.; Nygren, I.; Punga, A.R. Vitamin D deficiency in patients with myasthenia gravis and improvement of fatigue after supplementation of vitamin D3: A pilot study. Eur. J. Neurol. 2012, 19, 1554–1560. [Google Scholar] [CrossRef] [PubMed]
- Cadegiani, A. Remission of severe Myasthenia gravis after massive dose vitamin D treatment. Am. J. Case Rep. 2016, 17, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Huang, H.; Chen, X.; Chen, Y.; Zeng, X.; Lin, F.; Chen, X. Causal effect of vitamin D on myasthenia gravis: A two-sample Mendelian randomization study. Front. Nutr. 2023, 10, 1171830. [Google Scholar] [CrossRef]
- Al-Eisa, E.S.; Alghadir, A.H.; Gabr, S.A. Correlation between vitamin D levels and muscle fatigue risk factors based on physical activity in healthy older adults. Clin. Interv. Aging 2016, 11, 513–522. [Google Scholar]
- Zheng, Z.; Xu, W.; Wang, F.; Qii, Y.; Xue, Q. Association between vitamin D3 levels and frailty in the elderly: A large sample cross-sectional study. Front. Nutr. 2022, 9, 980908. [Google Scholar] [CrossRef]
- Dev, R.; Del Fabbro, E.; Schwartz, G.G.; Hui, D.; Palla, S.L.; Gutierrez, N.; Bruera, E. Preliminary report: Vitamin D deficiency in advanced cancer patients with symptoms of fatigue or anorexia. Oncologist 2011, 16, 1637–1641. [Google Scholar] [CrossRef] [PubMed]
- Głąbska, D.; Kołota, A.; Lachowicz, K.; Skolmowska, D.; Stachoń, M.; Guzek, D. Vitamin D Supplementation and Mental Health in Multiple Sclerosis Patients: A Systematic Review. Nutrients 2021, 13, 4207. [Google Scholar] [PubMed]
- Yancey, J.R.; Thomas, S.M. Chronic fatigue syndrome: Diagnosis and treatment. AFP 2012, 86, 741–746. [Google Scholar]
- Moss-Morris, R.; Deary, V.; Castellet, B. Chronic fatigue syndrome. Handb. Clin. Neurol. 2013, 110, 303–314. [Google Scholar]
- Earl, K.E.; Sakellariou, G.K.; Sinclair, M.; Fenech, M.; Croden, F.; Owens, D.J.; Tang, J.; Miller, A.; Lawton, C.; Dye, L.; et al. Vitamin D status in chronic fatigue syndrome/myalgic encephalomyelitis: A cohort study from the North-West of England. BMJ Open 2017, 7, e015296. [Google Scholar] [CrossRef] [PubMed]
- Berkovitz, S.; Ambler, G.; Jenkins, M.; Thurgood, S. Serum 25-hydroxy vitamin D levels in chronic fatigue syndrome: A retrospective survey. Int. J. Vitam. Nutr. Res. 2009, 79, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Havdahl, A.; Mitchell, R.; Paternoster, L.; Davey Smith, G. Investigating causality in the association between vitamin D status and self-reported tiredness. Sci. Rep. 2019, 9, 2880. [Google Scholar] [CrossRef] [PubMed]
- Herlofson, K.; Kluger, B.M. Fatigue in Parkinson’s disease. J. Neurol. Sci. 2017, 374, 38–41. [Google Scholar] [CrossRef]
- Wang, L.; Evatt, M.L.; Maldonado, L.G.; Perry, W.R.; Ritchie, J.C.; Beecham, G.W.; Martin, E.R.; Haines, J.L.; Pericak-Vance, M.A.; Vance, J.M.; et al. Vitamin D from different sources is inversely associated with Parkinson disease. Mov. Disord. 2015, 30, 560–566. [Google Scholar] [CrossRef]
- Ding, H.; Dhima, K.; Lockhart, K.C.; Locascio, J.J.; Hoesing, A.N.; Duong, K.; Trisini-Lipsanopoulos, A.; Hayes, M.T.; Sohur, U.S.; Wills, A.M.; et al. Unrecognized vitamin D3 deficiency is common in Parkinson disease: Harvard Biomarker Study. Neurology 2013, 81, 1531–1537. [Google Scholar] [CrossRef]
- Pignolo, A.; Mastrilli, S.; Davì, C.; Arnao, V.; Aridon, P.; dos Santos Mendes, F.A.; Gagliardo, C.; D’Amelio, M. Vitamin D and Parkinson’s disease. Nutrients 2022, 14, 1220. [Google Scholar] [CrossRef]
- Fullard, M.E.; Duda, J.E. A review of the relationship between vitamin D and Parkinson disease symptoms. Front. Neurol. 2020, 11, 454. [Google Scholar] [CrossRef]
- Roy, N.M.; Al-Harthi, L.; Sampat, N.; Al-Mujaini, R.; Mahadevan, S.; Al Adawi, S.; Essa, M.M.; Al Subhi, L.; Al-Balushi, B.; Qoronfleh, M.W.; et al. Impact of vitamin D on neurocognitive function in dementia, depression, schizophrenia and ADHD. Front. Biosci.-Landmark 2020, 26, 566–611. [Google Scholar] [CrossRef] [PubMed]
- Krisanova, N.; Pozdnyakova, N.; Pastukhov, A.; Dudarenko, M.; Maksymchuk, O.; Parkhomets, P.; Sivko, R.; Borisova, T. Vitamin D3 deficiency in puberty rats causes presynaptic malfunctioning through alterations in exocytotic release and uptake of glutamate/GABA and expression of EAAC-1/GAT-3 transporters. Food Chem. Toxicol. 2019, 123, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Portis, S.A.; Zitman, I.H. A Mechanism of Fatigue in Neuropsychiatric Patients: A Preliminary Report. JAMA 1943, 121, 569–573. [Google Scholar] [CrossRef]
- Rylander, M.; Verhulst, S. Vitamin D insufficiency in psychiatric inpatients. J. Psychiatr. Pract. 2013, 19, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Józefowicz, O.; Rabe-Jablonska, J.; Wozniacka, A.; Strzelecki, D. Analysis of vitamin D status in major depression. J. Psychiatr. Pract. 2014, 20, 329–337. [Google Scholar] [CrossRef]
- Mayne, P.E.; Burne, T.H. Vitamin D in synaptic plasticity, cognitive function, and neuropsychiatric illness. Trends Neurosci. 2019, 42, 293–306. [Google Scholar] [CrossRef]
- Wintermeyer, E.; Ihle, C.; Ehnert, S.; Stöckle, U.; Ochs, G.; De Zwart, P.; Flesch, I.; Bahrs, C.; Nussler, A.K. Crucial role of vitamin D in the musculoskeletal system. Nutrients 2016, 8, 319. [Google Scholar] [CrossRef]
- Atherton, K.; Berry, D.J.; Parsons, T.; Macfarlane, G.J.; Power, C.; Hyppönen, E. Vitamin D and chronic widespread pain in a white middle-aged British population: Evidence from a cross-sectional population survey. Ann. Rheum. Dis. 2009, 68, 817–822. [Google Scholar] [CrossRef]
- MacFarlane, G.J.; Palmer, B.; Roy, D.; Afzal, C.; Silman, A.J.; O’neill, T. An excess of widespread pain among South Asians: Are low levels of vitamin D implicated? Ann. Rheum. Dis. 2005, 64, 1217–1219. [Google Scholar] [CrossRef]
- McBeth, J.; Pye, S.R.; O’Neill, T.W.; Macfarlane, G.J.; Tajar, A.; Bartfai, G.; Boonen, S.; Bouillon, R.; Casanueva, F.; Finn, J.D.; et al. Musculoskeletal pain is associated with very low levels of vitamin D in men: Results from the European Male Ageing Study. Ann. Rheum. Dis. 2010, 69, 1448–1452. [Google Scholar] [CrossRef] [PubMed]
- Goyal, V.; Agrawal, M. Effect of supplementation of vitamin D and calcium on patients suffering from chronic non-specific musculoskeletal pain: A pre-post study. J. Fam. Med. Prim. Care 2021, 10, 1839–1844. [Google Scholar] [CrossRef] [PubMed]
- Fishbain, D.A.; Cole, B.; Cutler, R.B.; Lewis, J.; Rosomoff, H.L.; Fosomoff, R.S. Is pain fatiguing? A structured evidence-based review. Pain Med. 2003, 4, 51–62. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Molfetta, I.V.; Bordoni, L.; Gabbianelli, R.; Sagratini, G.; Alessandroni, L. Vitamin D and Its Role on the Fatigue Mitigation: A Narrative Review. Nutrients 2024, 16, 221. https://doi.org/10.3390/nu16020221
Di Molfetta IV, Bordoni L, Gabbianelli R, Sagratini G, Alessandroni L. Vitamin D and Its Role on the Fatigue Mitigation: A Narrative Review. Nutrients. 2024; 16(2):221. https://doi.org/10.3390/nu16020221
Chicago/Turabian StyleDi Molfetta, Ippolita Valentina, Laura Bordoni, Rosita Gabbianelli, Gianni Sagratini, and Laura Alessandroni. 2024. "Vitamin D and Its Role on the Fatigue Mitigation: A Narrative Review" Nutrients 16, no. 2: 221. https://doi.org/10.3390/nu16020221
APA StyleDi Molfetta, I. V., Bordoni, L., Gabbianelli, R., Sagratini, G., & Alessandroni, L. (2024). Vitamin D and Its Role on the Fatigue Mitigation: A Narrative Review. Nutrients, 16(2), 221. https://doi.org/10.3390/nu16020221