
Feasibility of Employing mHealth in Delivering Preventive Nutrition Interventions Targeting the First 1000 Days of Life: Experiences from a Community-Based Cluster Randomised Trial in Rural Bangladesh

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
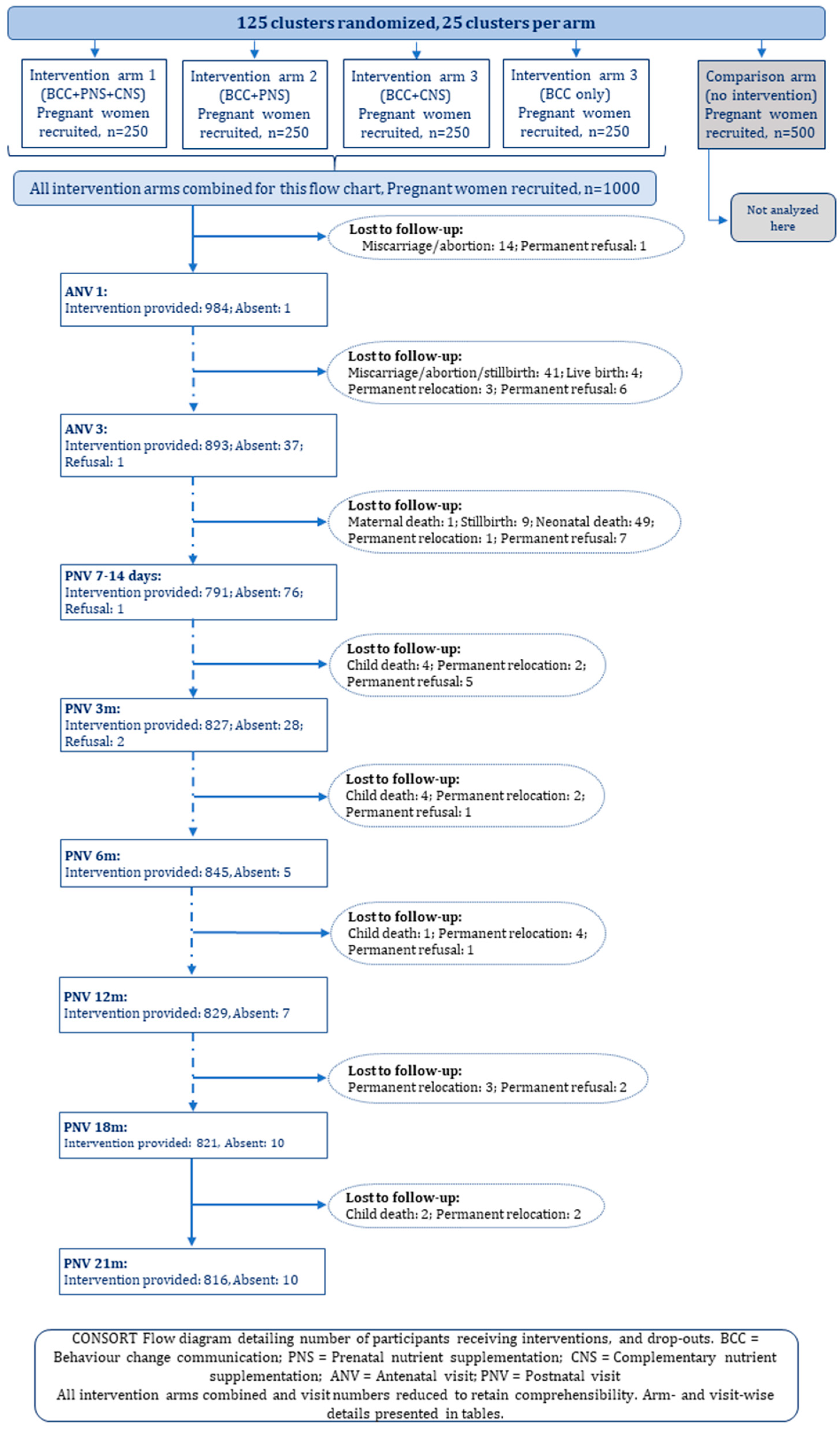
2.1. Study Design and Participants
2.2. Architecture of the Electronic Intervention System
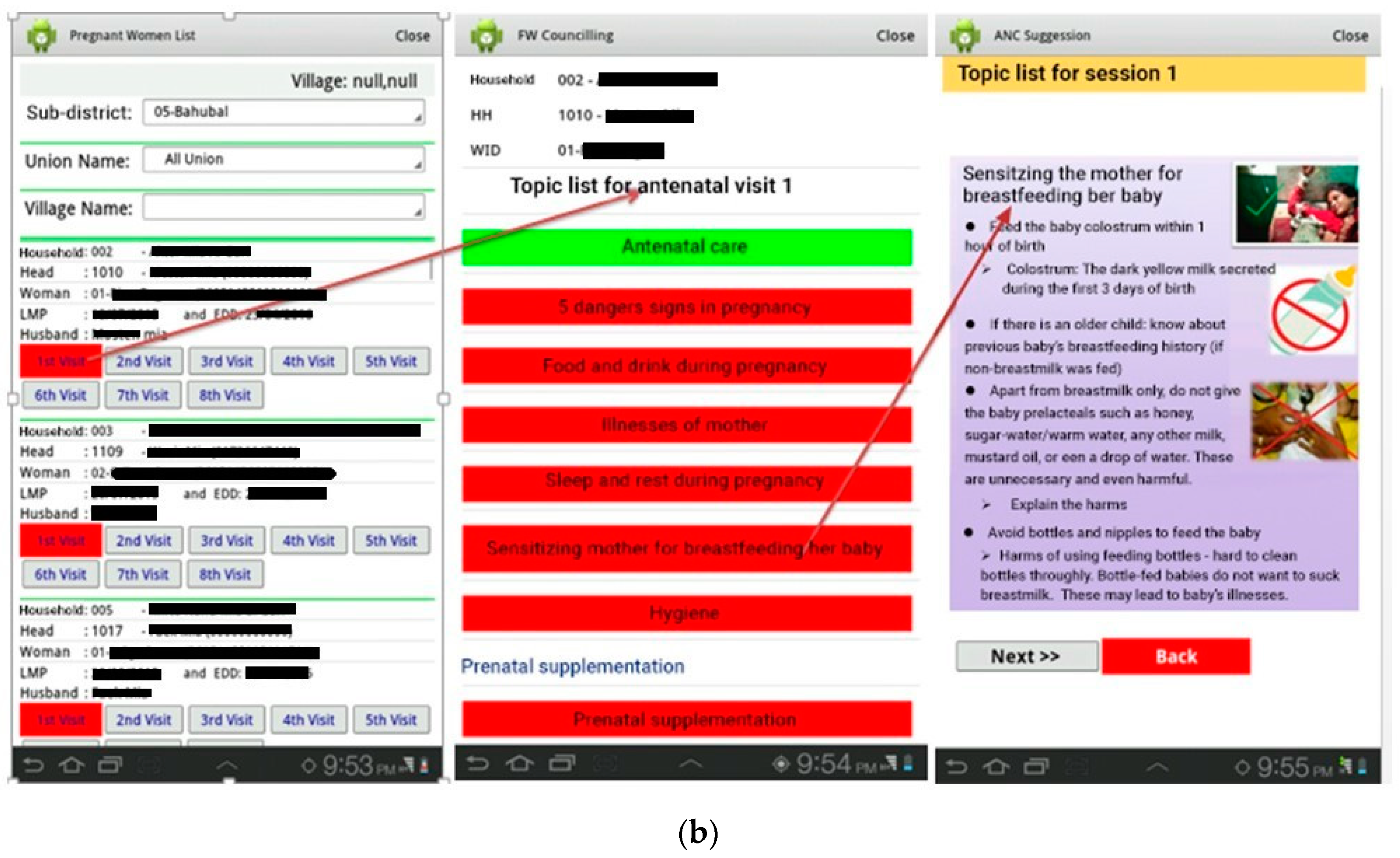
2.2.1. BCC Modules
2.2.2. LNS Inventory
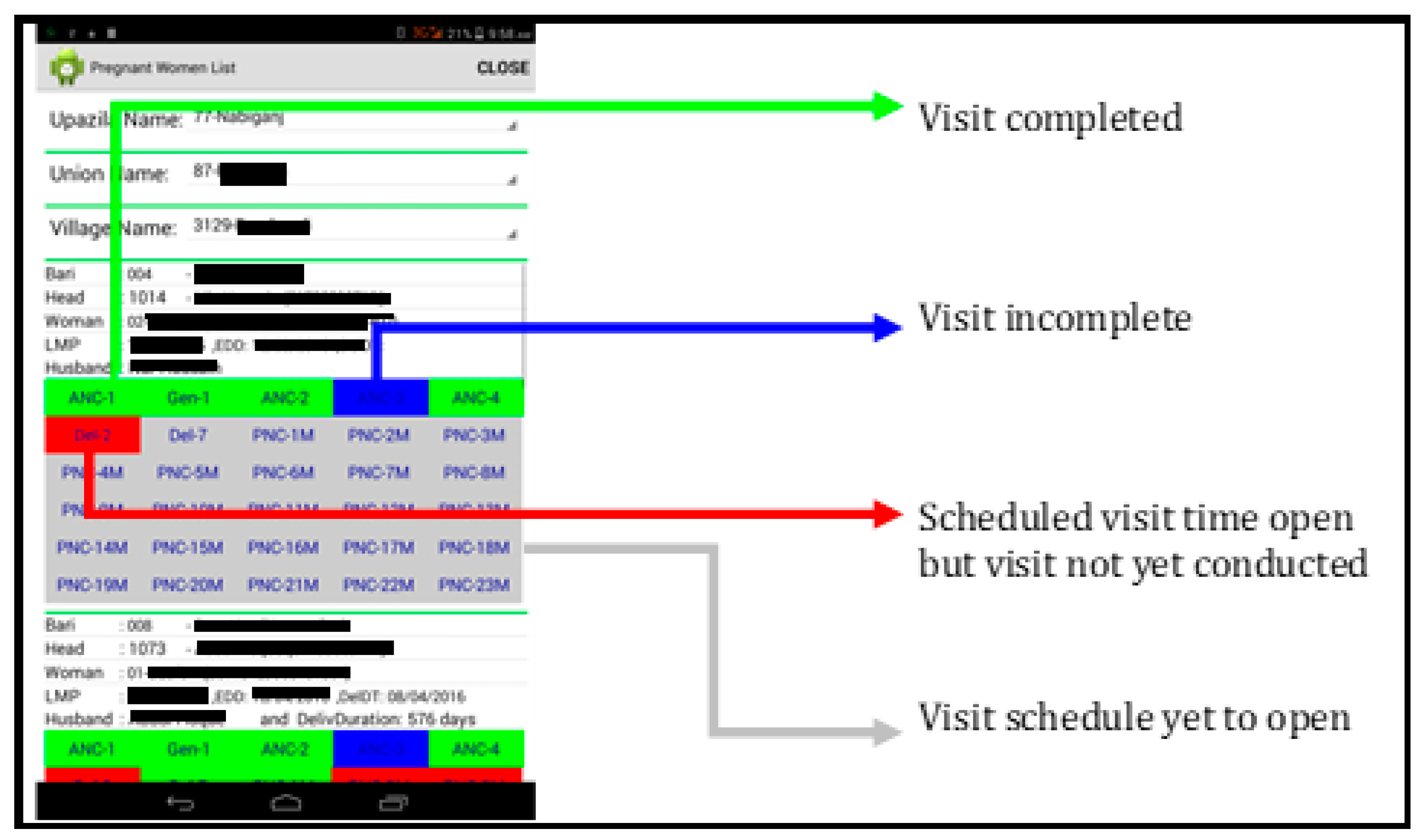
2.3. Intervention Implementation and Monitoring with the App
2.4. Data Collection
2.5. Data Management and Analysis
2.6. Ethics Approval
3. Results
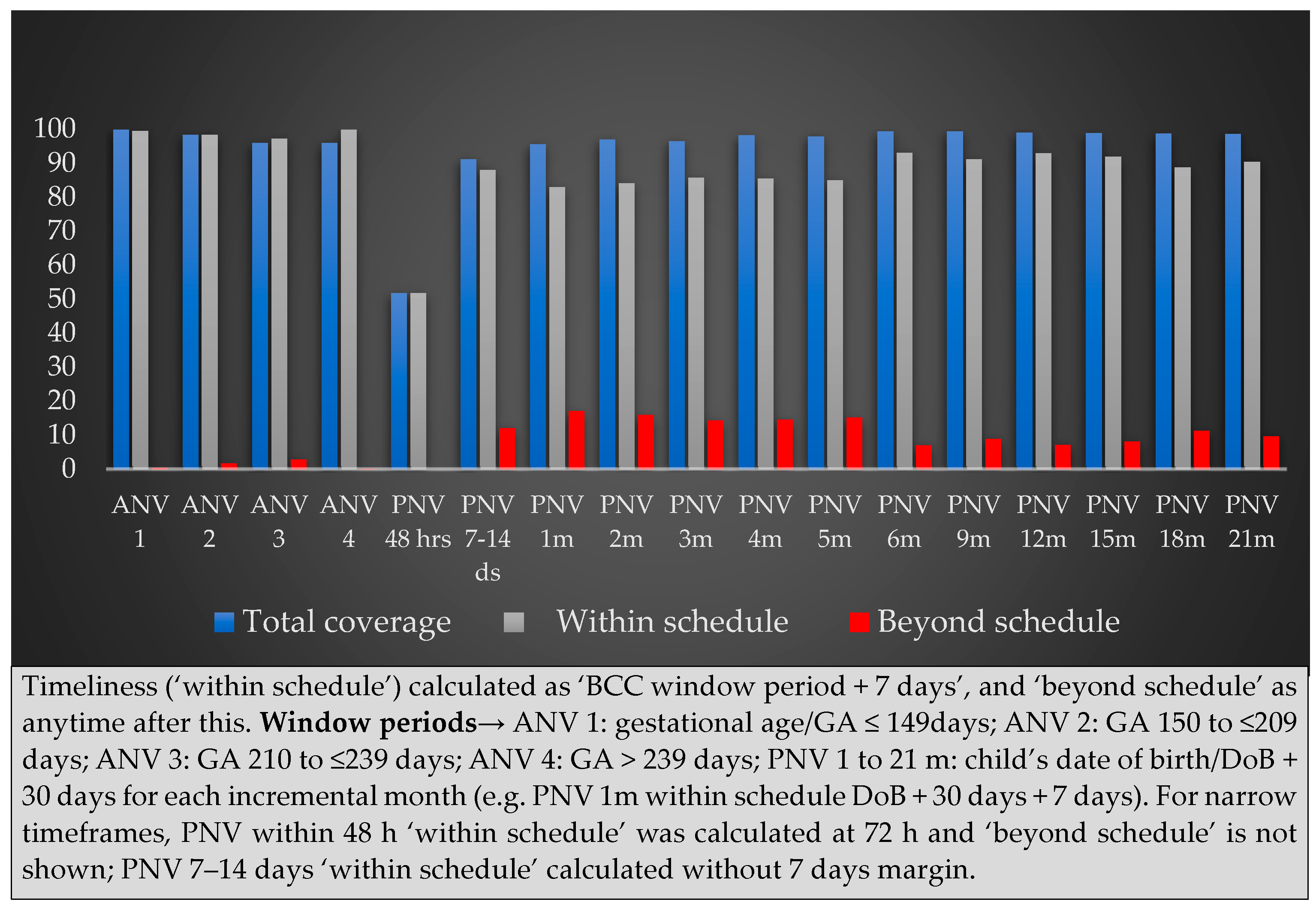
3.1. Intervention Visit Coverage: Quantitative Assessments
3.2. Benefits, Challenges and Solutions from Healthcare Providers’ Perspective: Qualitative Findings
“Mothers understand (messages) faster from pictures than verbal explanation”[IDI, CHW]
“Workload seems much less because of using the tablet”[IDI, CHW]
“I have to ensure counselling quality: I check if important messages are overlooked, or if messages are clearly relayed to mothers … I check if the Field Supervisors can properly supervise and share feedback to their assigned CHWs … I supervise both these cadres”[IDI, Intervention team supervisor]
“A mother maybe in hospital probably having a caesarean section, or the baby was in hospital with a problem, or the mother had a problem. She forgot (to notify birth), maybe she called us after five days and said that her baby was delivered but they could not inform us for this and that reason”.[IDI, CHW]
“You can work with a charged tablet. (But my tablet) charge came down to 60–50% just after one visit, and turned off when I signed into another visit”.[IDI, CHW]
“Some places have no electricity. Even if I carry the charger, I cannot use it if the family uses (low energy storage) solar power … so we always keep hard copies (of BCC messages) and use it as alternatives”.[IDI, CHW]
“Many times, it does not upload or download, (or) takes a long time … say, it keeps uploading for an hour … it takes forever to upload”[IDI, CHW]
“(We were given) simple instructions: like, take the tab to an open space, take some time and be patient. If it still doesn’t work, shut it down, wait for some time and turn it on again. Wait half an hour. If not fixed by this, wait another half an hour. If much time is gone but the problem persists, we take the tab to office”.[IDI, CHW]
“I am continuously worried if something happens to the tab, since it is an official asset”.[IDI, CHW]
“I’m always scared if the tab is lost … at work and at home … we work alone so it can be hijacked”[IDI, CHW]
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Universal Health Coverage (UHC) [Internet]. Available online: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc) (accessed on 15 April 2024).
- World Health Organization. Declaration of Alma-Ata. In Proceedings of the International Conference on Primary Health Care, Alma-Ata, USSR, 6–12 September 1978. [Google Scholar]
- Bhutta, Z.A.; Lassi, Z.S.; Pariyo, G.; Huicho, L. Global Experience of Community Health Workers for Delivery of Health Related Millennium Development Goals: A Systematic Review, Country Case Studies, and Recommendations for Integration into National Health Systems; WHO: Geneva, Switzerland, 2010; 377p. [Google Scholar]
- Gilmore, B.; McAuliffe, E. Effectiveness of community health workers delivering preventive interventions for maternal and child health in low- and middle-income countries: A systematic review. BMC Public Health 2013, 13, 847. [Google Scholar] [CrossRef] [PubMed]
- Perry, H.B.; Zulliger, R.; Rogers, M.M. Community Health Workers in Low-, Middle-, and High-Income Countries: An Overview of Their History, Recent Evolution, and Current Effectiveness. Annu. Rev. Public Health 2014, 35, 399–421. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Bhutta, Z.A. Community-based intervention packages for reducing maternal and neonatal morbidity and mortality and improving neonatal outcomes. Cochrane Database Syst. Rev. 2015, 2015, CD007754. [Google Scholar] [CrossRef]
- El Arifeen, S.; Christou, A.; Reichenbach, L.; Osman, F.A.; Azad, K.; Islam, K.S.; Ahmed, F.; Perry, H.B.; Peters, D.H. Community-based approaches and partnerships: Innovations in health-service delivery in Bangladesh. Lancet 2013, 382, 2012–2026. [Google Scholar] [CrossRef] [PubMed]
- Glenton, C.; Colvin, C.J.; Carlsen, B.; Swartz, A.; Lewin, S.; Noyes, J.; Rashidian, A. Barriers and facilitators to the implementation of lay health worker programmes to improve access to maternal and child health: Qualitative evidence synthesis. Cochrane Database Syst. Rev. 2013, 2013, CD010414. [Google Scholar] [CrossRef] [PubMed]
- Aranda-Jan, C.B.; Mohutsiwa-Dibe, N.; Loukanova, S. Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health 2014, 14, 188. [Google Scholar] [CrossRef]
- Kallander, K.; Tibenderana, J.K.; Akpogheneta, O.J.; Strachan, D.L.; Hill, Z.; ten Asbroek, A.H.; Conteh, L.; Kirkwood, B.R.; Meek, S.R. Mobile health (mHealth) approaches and lessons for increased performance and retention of community health workers in low- and middle-income countries: A review. J. Med. Internet Res. 2013, 15, e17. [Google Scholar] [CrossRef]
- World Health Organization. Global Diffusion of EHealth: Making Universal Health Coverage Achievable: Report of the Third Global Survey on EHealth; World Health Organization (WHO): Geneva, Switzerland, 2016. [Google Scholar]
- Mitchell, K.J.; Bull, S.; Kiwanuka, J.; Ybarra, M.L. Cell phone usage among adolescents in Uganda: Acceptability for relaying health information. Health Educ. Res. 2011, 26, 770–781. [Google Scholar] [CrossRef]
- Guan, V.; Zhou, C.; Wan, H.; Zhou, R.; Zhang, D.; Zhang, S.; Yang, W.; Voutharoja, B.P.; Wang, L.; Win, K.T.; et al. A Novel Mobile App for Personalized Dietary Advice Leveraging Persuasive Technology, Computer Vision, and Cloud Computing: Development and Usability Study. JMIR Form. Res. 2023, 7, e46839. [Google Scholar] [CrossRef]
- Vodopivec-Jamsek, V.; de Jongh, T.; Gurol-Urganci, I.; Atun, R.; Car, J. Mobile phone messaging for preventive health care. Cochrane Database Syst. Rev. 2012, 12, CD007457. [Google Scholar] [CrossRef]
- Feroz, A.; Perveen, S.; Aftab, W. Role of mHealth applications for improving antenatal and postnatal care in low and middle income countries: A systematic review. BMC Health Serv. Res. 2017, 17, 704. [Google Scholar] [CrossRef]
- Tang, K.; Gerling, K.; Chen, W.; Geurts, L. Information and Communication Systems to Tackle Barriers to Breastfeeding: Systematic Search and Review. J. Med. Internet Res. 2019, 21, e13947. [Google Scholar] [CrossRef]
- National Institute of Population Research and Training (NIPORT); Medical Education and Family Welfare Division; Ministry of Health and Family Welfare; ICF (NIPORT/ICF). Bangladesh Demographic and Health Survey 2017–18; NIPORT/ICF: Rockville, MD, USA, 2019. [Google Scholar]
- Labrique, A.B.; Vasudevan, L.; Kochi, E.; Fabricant, R.; Mehl, G. mHealth innovations as health system strengthening tools: 12 common applications and a visual framework. Glob. Health Sci. Pract. 2013, 1, 160–171. [Google Scholar] [CrossRef]
- Tonkin, E.; Brimblecombe, J.; Wycherley, T.P. Characteristics of Smartphone Applications for Nutrition Improvement in Community Settings: A Scoping Review. Adv. Nutr. 2017, 8, 308–322. [Google Scholar] [CrossRef]
- Iribarren, S.J.; Akande, T.O.; Kamp, K.J.; Barry, D.; Kader, Y.G.; Suelzer, E. Effectiveness of Mobile Apps to Promote Health and Manage Disease: Systematic Review and Meta-analysis of Randomized Controlled Trials. JMIR Mhealth Uhealth 2021, 9, e21563. [Google Scholar] [CrossRef]
- Chanani, S.; Wacksman, J.; Deshmukh, D.; Pantvaidya, S.; Fernandez, A.; Jayaraman, A. M-Health for Improving Screening Accuracy of Acute Malnutrition in a Community-Based Management of Acute Malnutrition Program in Mumbai Informal Settlements. Food Nutr. Bull. 2016, 37, 504–516. [Google Scholar] [CrossRef]
- Frank, T. A Mobile Health Application to Manage Acute Malnutrition; Lessons from Developing and Piloting the App in Five Countries; World Vision/Save the Children: London, UK, 2017. [Google Scholar]
- Jones, C.O.; Wasunna, B.; Sudoi, R.; Githinji, S.; Snow, R.W.; Zurovac, D. “Even if you know everything you can forget”: Health worker perceptions of mobile phone text-messaging to improve malaria case-management in Kenya. PLoS ONE 2012, 7, e38636. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed]
- Aunger, R.; Curtis, V. Behaviour Centred Design: Towards an applied science of behaviour change. Health Psychol. Rev. 2016, 10, 425–446. [Google Scholar] [CrossRef] [PubMed]
- Billah, S.M.; Ferdous, T.E.; Karim, M.A.; Dibley, M.J.; Raihana, S.; Moinuddin, M.; Choudhury, N.; Ahmed, T.; Hoque, D.M.E.; Menon, P.; et al. A community-based cluster randomised controlled trial to evaluate the effectiveness of different bundles of nutrition-specific interventions in improving mean length-for-age z score among children at 24 months of age in rural Bangladesh: Study protocol. BMC Public Health 2017, 17, 375. [Google Scholar] [CrossRef] [PubMed]
- Billah, S.M.; Ferdous, T.E.; Siddique, A.B.; Raynes-Greenow, C.; Kelly, P.; Choudhury, N.; Ahmed, T.; Gillespie, S.; Hoddinott, J.; Haider, R.; et al. The effect of electronic job aid assisted one-to-one counselling to support exclusive breastfeeding among 0–5-month-old infants in rural Bangladesh. Matern. Child Nutr. 2022, 18, e13377. [Google Scholar] [CrossRef] [PubMed]
- Billah, S.M.; Ferdous, T.E.; Kelly, P.; Raynes-Greenow, C.; Siddique, A.B.; Choudhury, N.; Ahmed, T.; Gillespie, S.; Hoddinott, J.; Menon, P.; et al. Effect of nutrition counselling with a digital job aid on child dietary diversity: Analysis of secondary outcomes from a cluster randomised controlled trial in rural Bangladesh. Matern. Child Nutr. 2022, 18, e13267. [Google Scholar] [CrossRef]
- NIPORT, Mitra and Associates, and ICF International. Bangladesh Demographic and Health Survey 2011; National Institute of Population Research and Training: Dhaka, Bangladesh; Mitra and Associates: Dhaka, Bangladesh; MEASURE DHS ICF International: Calverton, MD, USA, 2013. [Google Scholar]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E.; Lancet Nutrition Interventions Review Group, the Maternal and Child Nutrition Study Group. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. The Community Infant and Young Child Feeding Counseling Package: Key Messages Booklet; UNICEF: Hong Kong, China, 2012. [Google Scholar]
- Government of Bangladesh, Ministry of Health. Infant and Young Child Feeding Training Manual (Sub-District and Union Level); Government of Bangladesh, Ministry of Health: Dhaka, Bangladesh, 2013. [Google Scholar]
- Government of Bangladesh. Maternal and Neonatal Care Counselling Module for Community Health Workers Training Module; Government of Bangladesh: Dhaka, Bangladesh, 2011. [Google Scholar]
- Wilcox, A.B.; Gallagher, K.; Bakken, S. Security approaches in using tablet computers for primary data collection in clinical research. Egems Gener. Evid. Methods Improv. Patient Outcomes 2013, 1, 1008. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishna, K.; Dass, D.; Raj, T.; Rakesh, D.; Kishore, R.; Srinivasan, K.; Nyblade, L.; Ekstrand-Abueg, M.; Ekstrand, M.L. Development of a Novel Tablet-based Approach to Reduce HIV Stigma among Healthcare Staff in India. Perspect Health Inf Manag. 2017, 14, 1b. [Google Scholar]
- King, J.D.; Buolamwini, J.; Cromwell, E.A.; Panfel, A.; Teferi, T.; Zerihun, M.; Melak, B.; Watson, J.; Tadesse, Z.; Vienneau, D.; et al. A novel electronic data collection system for large-scale surveys of neglected tropical diseases. PLoS ONE 2013, 8, e74570. [Google Scholar] [CrossRef] [PubMed]
- Paudel, D.; Ahmed, M.; Pradhan, A.; Dangol, R.L. Successful use of tablet personal computers and wireless technologies for the 2011 Nepal Demographic and Health Survey. Glob. Health Sci. Pract. 2013, 1, 277–284. [Google Scholar] [CrossRef]
- Modi, D.; Dholakia, N.; Gopalan, R.; Venkatraman, S.; Dave, K.; Shah, S.; Desai, G.; Qazi, S.A.; Sinha, A.; Pandey, R.M.; et al. mHealth intervention “ImTeCHO” to improve delivery of maternal, neonatal, and child care services-A cluster-randomized trial in tribal areas of Gujarat, India. PLoS Med. 2019, 16, e1002939. [Google Scholar] [CrossRef]
- Aboud, F.E.; Singla, D.R. Challenges to changing health behaviours in developing countries: A critical overview. Soc. Sci. Med. 2012, 75, 589–594. [Google Scholar] [CrossRef]
- Murray, E.; Burns, J.; See, T.S.; Lai, R.; Nazareth, I. Interactive Health Communication Applications for people with chronic disease. Cochrane Database Syst. Rev. 2005, 4, CD004274. [Google Scholar] [CrossRef]
- Konig, L.; Marbach-Breitruck, E.; Engler, A.; Suhr, R. The Development and Evaluation of an e-Learning Course That Promotes Digital Health Literacy in School-age Children: Pre-Post Measurement Study. J. Med. Internet Res. 2022, 24, e37523. [Google Scholar] [CrossRef]
- Janmohamed, A.; Sohani, N.; Lassi, Z.S.; Bhutta, Z.A. The Effects of Community Home Visit and Peer Group Nutrition Intervention Delivery Platforms on Nutrition Outcomes in Low and Middle-Income Countries: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 440. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Rind, F.; Irfan, O.; Hadi, R.; Das, J.K.; Bhutta, Z.A. Impact of Infant and Young Child Feeding (IYCF) Nutrition Interventions on Breastfeeding Practices, Growth and Mortality in Low- and Middle-Income Countries: Systematic Review. Nutrients 2020, 12, 722. [Google Scholar] [CrossRef]
- Lee, S.H.; Nurmatov, U.B.; Nwaru, B.I.; Mukherjee, M.; Grant, L.; Pagliari, C. Effectiveness of mHealth interventions for maternal, newborn and child health in low- and middle-income countries: Systematic review and meta-analysis. J Glob Health 2016, 6, 010401. [Google Scholar] [CrossRef] [PubMed]
- Hasan, A.M.R.; Smith, G.; Selim, M.A.; Akter, S.; Khan, N.U.Z.; Sharmin, T.; Rasheed, S. Work and breast milk feeding: A qualitative exploration of the experience of lactating mothers working in ready made garments factories in urban Bangladesh. Int. Breastfeed. J. 2020, 15, 93. [Google Scholar] [CrossRef]
- Rasheed, S.; Frongillo, E.A.; Devine, C.M.; Alam, D.S.; Rasmussen, K.M. Maternal, infant, and household factors are associated with breast-feeding trajectories during infants’ first 6 months of life in Matlab, Bangladesh. J. Nutr. 2009, 139, 1582–1587. [Google Scholar] [CrossRef]
- Ruotsalainen, J.H.; Verbeek, J.H.; Marine, A.; Serra, C. Preventing occupational stress in healthcare workers. Cochrane Database Syst. Rev. 2015, 2015, CD002892. [Google Scholar] [CrossRef]
- Roxby, P. NHS Computer Issues Linked to Patient Harm. Available online: https://www.bbc.com/news/articles/c4nn0vl2e78o (accessed on 20 August 2024).
- Management Information System. Health Bulletin 2016; Management Information System (MIS); Directorate General of Health Services (DGHS): Dhaka, Bangladesh, 2016. [Google Scholar]
- Tosini, G.; Ferguson, I.; Tsubota, K. Effects of blue light on the circadian system and eye physiology. Mol. Vis. 2016, 22, 61–72. [Google Scholar]
- Moon, J.; Yun, J.; Yoon, Y.D.; Park, S.I.; Seo, Y.J.; Park, W.S.; Chu, H.Y.; Park, K.H.; Lee, M.Y.; Lee, C.W.; et al. Blue light effect on retinal pigment epithelial cells by display devices. Integr. Biol. 2017, 9, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Grant, K.; Goldizen, F.C.; Sly, P.D.; Brune, M.N.; Neira, M.; van den Berg, M.; Norman, R.E. Health consequences of exposure to e-waste: A systematic review. Lancet Glob. Health 2013, 1, e350–e361. [Google Scholar] [CrossRef]
- Noel-Brune, M.; Goldizen, F.C.; Neira, M.; van den Berg, M.; Lewis, N.; King, M.; Suk, W.A.; Carpenter, D.O.; Arnold, R.G.; Sly, P.D. Health effects of exposure to e-waste. Lancet Glob. Health 2013, 1, e70. [Google Scholar] [CrossRef] [PubMed]
- Fiander, M.; McGowan, J.; Grad, R.; Pluye, P.; Hannes, K.; Labrecque, M.; Roberts, N.W.; Salzwedel, D.M.; Welch, V.; Tugwell, P. Interventions to increase the use of electronic health information by healthcare practitioners to improve clinical practice and patient outcomes. Cochrane Database Syst. Rev. 2015, 2015, CD004749. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antenatal Visits (ANV) 1–4 | PNV 6–11: 6–21 Months |
|---|---|
| Diet during pregnancy: Do’s and Don’ts (food groups, homemade good food, foods/drinks/tobacco to avoid, sample 1-day menu) | Homemade nutritious food + continued BF |
| Antenatal care (ANC), and birth preparedness | 4 important food groups: animal protein, plant protein, complex carbs, fruits & veg, iron-rich foods, esp. animal sources |
| Pregnancy-related 5 danger signs and immediate care | Quantity: increases with age |
| Sleep and rest during pregnancy | 6–8 m: ½ of 250 mL bowl; twice/day |
| Sensitising the mother for breastfeeding (early initiation of BF, avoiding pre-lacteal, exclusive breastfeeding/EBF for 6 m) | 9–11 m: ½ of 250 mL bowl; thrice/day |
| Water, sanitation and hygiene (WASH) | 12–23 m: full of 250 mL bowl; thrice/day |
| Additional snacks: 1–2 times/day | |
| Additional counselling at ANV 2 | Responsive feeding |
| Anaemia: tackling through diet and hygiene | Practical demonstration of CF as needed |
| Extra care for teenage pregnancy | WASH during BF and CF |
| Preparing the mother mentally for neonatal care (drying and wrapping) | Feeding anorexic & sick infants: frequent, small feeds (BF, CF), increased food variety, avoiding junk food; caregiver’s patience |
| Additional counselling at ANV 3–4 | Vaccination, care seeking during illnesses, |
| Birth preparedness at home | Diet for lactating mothers, sample 1 day menu |
| Position and attachment for breastfeeding/BF (practical demonstration) | Family planning, WASH, sleep & rest |
| Postnatal care (PNC) | |
| Postnatal visits (PNV) 1–5: birth to 5 completed months | BF essentials continued (position & attachment, expression etc, as needed) |
| Continued: EBF for 6 m, position & attachment (hands-on demo) | |
| Rules and signs of enough BF | |
| Expression of breastmilk; care for breast problems | |
| Caring the low birth weight, sick infants | |
| PNC, vaccination, home care for mother & child | |
| Danger signs of neonate, infant and nursing mother | |
| Diet of lactating mother, sample 1-day menu | |
| Family planning, WASH, sleep & rest |
| Intervention(s) | Intervention Arms | Comparison | |||
|---|---|---|---|---|---|
| Arm 1 | Arm 2 | Arm 3 | Arm 4 | Arm 5 | |
| BCC | - | ||||
| PNS | - | - | - | ||
| CNS | - | - | - | ||
| Intervention Visits | Eligible | Conducted |
|---|---|---|
| n (%) | n (%) | |
| Antenatal visits (ANVs) [Enrolled women: 1000 in four arms combined] | ||
| ANV 1 | 985 (98.5) | 984 (99.9) |
| ANV 2 | 950 (96.4) | 934 (98.3) |
| ANV 3 | 931 (98.0) | 893 (95.9) |
| ANV 4 | 868 (93.2) | 832 (95.9) |
| Postnatal visits (PNVs) [Resultant live births: 1355 in four arms combined] | ||
| PNV within 48 h of birth | 874 (94.5) | 453 (51.8) |
| PNV within 7–14 days of birth | 868 (99.3) | 791 (91.1) |
| PNV 1 month | 864 (99.5) | 826 (95.6) |
| PNV 2 month | 858 (99.3) | 832 (97.0) |
| PNV 3 month | 857 (99.9) | 827 (96.5) |
| PNV 4 month | 852 (99.4) | 837 (98.2) |
| PNV 5 month | 852 (100.0) | 833 (97.8) |
| PNV 6 month | 850 (99.8) | 845 (99.4) |
| PNV 9 month | 844 (99.3) | 838 (99.3) |
| PNV 12 month | 837 (99.2) | 829 (99.0) |
| PNV 15 month | 834 (99.6) | 825 (98.9) |
| PNV 18 month | 832 (99.8) | 821 (98.7) |
| PNV 21 month | 828 (99.5) | 816 (98.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferdous, T.E.; Jaman, M.J.; Siddique, A.B.; Sultana, N.; Hossain, T.; Arifeen, S.E.; Billah, S.M. Feasibility of Employing mHealth in Delivering Preventive Nutrition Interventions Targeting the First 1000 Days of Life: Experiences from a Community-Based Cluster Randomised Trial in Rural Bangladesh. Nutrients 2024, 16, 3429. https://doi.org/10.3390/nu16203429
Ferdous TE, Jaman MJ, Siddique AB, Sultana N, Hossain T, Arifeen SE, Billah SM. Feasibility of Employing mHealth in Delivering Preventive Nutrition Interventions Targeting the First 1000 Days of Life: Experiences from a Community-Based Cluster Randomised Trial in Rural Bangladesh. Nutrients. 2024; 16(20):3429. https://doi.org/10.3390/nu16203429
Chicago/Turabian StyleFerdous, Tarana E, Md. Jahiduj Jaman, Abu Bakkar Siddique, Nadia Sultana, Takrib Hossain, Shams El Arifeen, and Sk Masum Billah. 2024. "Feasibility of Employing mHealth in Delivering Preventive Nutrition Interventions Targeting the First 1000 Days of Life: Experiences from a Community-Based Cluster Randomised Trial in Rural Bangladesh" Nutrients 16, no. 20: 3429. https://doi.org/10.3390/nu16203429
APA StyleFerdous, T. E., Jaman, M. J., Siddique, A. B., Sultana, N., Hossain, T., Arifeen, S. E., & Billah, S. M. (2024). Feasibility of Employing mHealth in Delivering Preventive Nutrition Interventions Targeting the First 1000 Days of Life: Experiences from a Community-Based Cluster Randomised Trial in Rural Bangladesh. Nutrients, 16(20), 3429. https://doi.org/10.3390/nu16203429