
Is Ultra-Processed Food Intake Associated with a Higher Risk of Glaucoma? A Prospective Cohort Study including 19,255 Participants from the SUN Project

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Methods
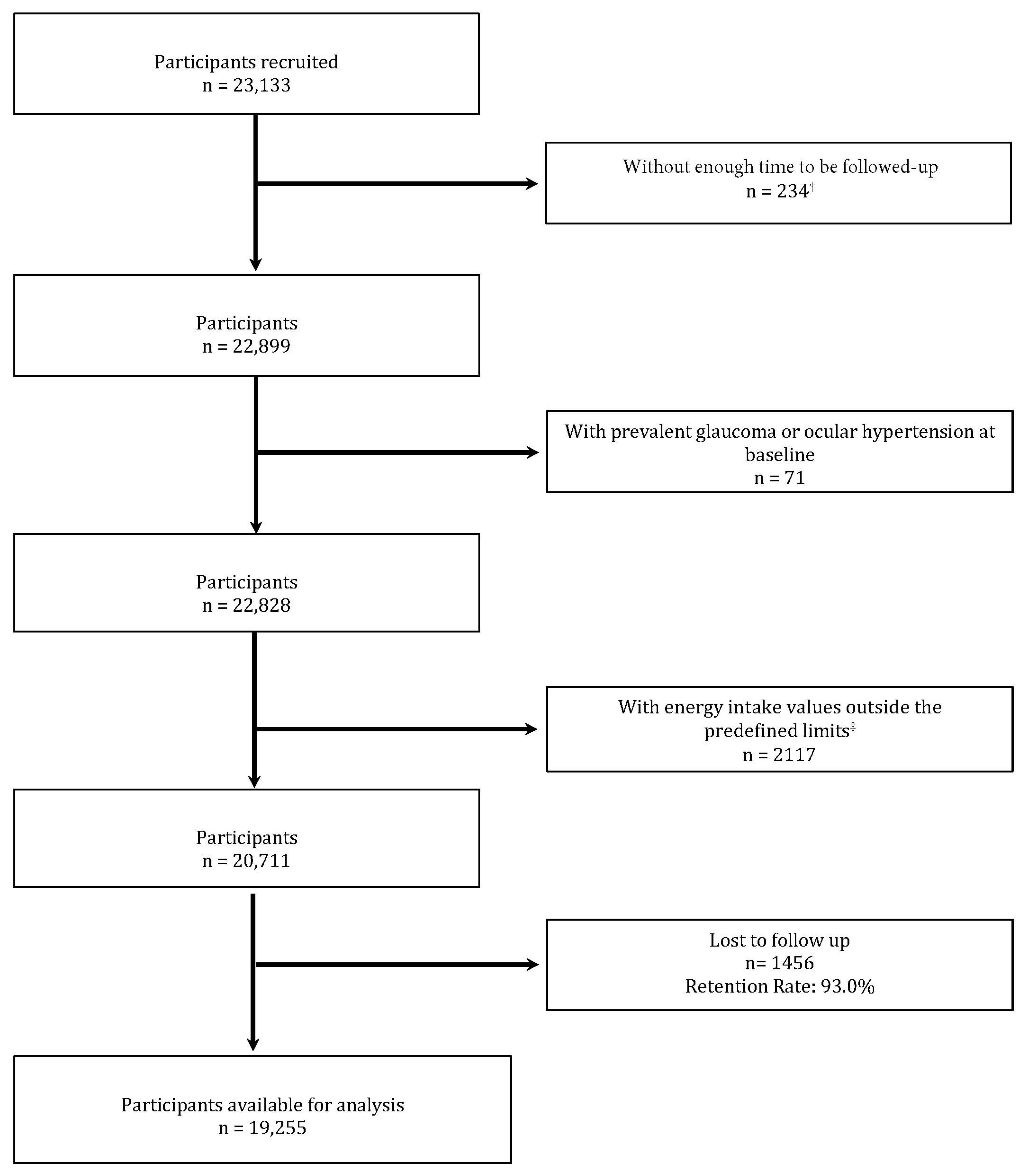
2.1. Study Design and Population
2.2. Glaucoma Incidence (Dependent Variable)
2.3. UPF Consumption (Independent Variable)

2.4. Covariates
2.5. Statistical Analysis
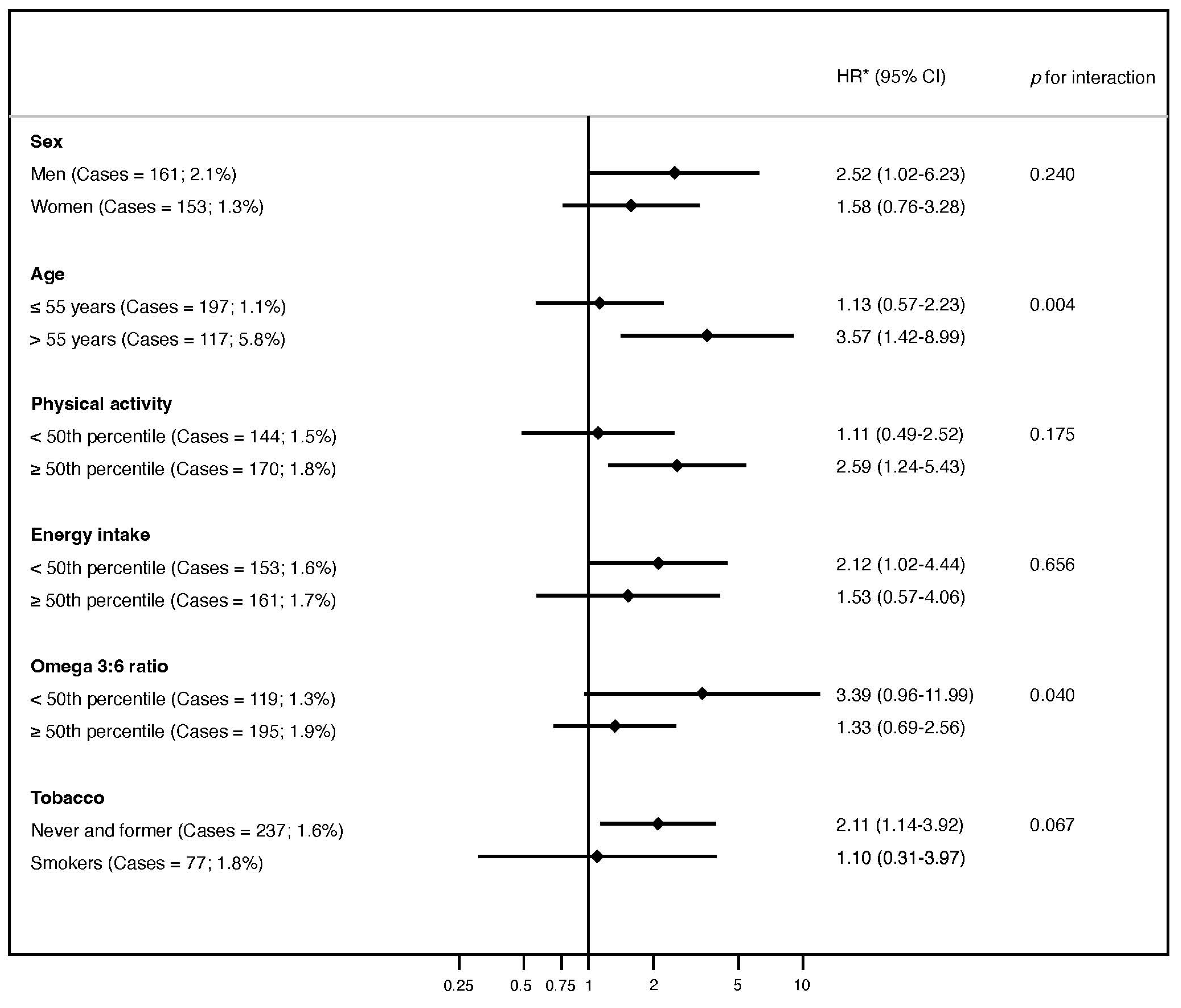
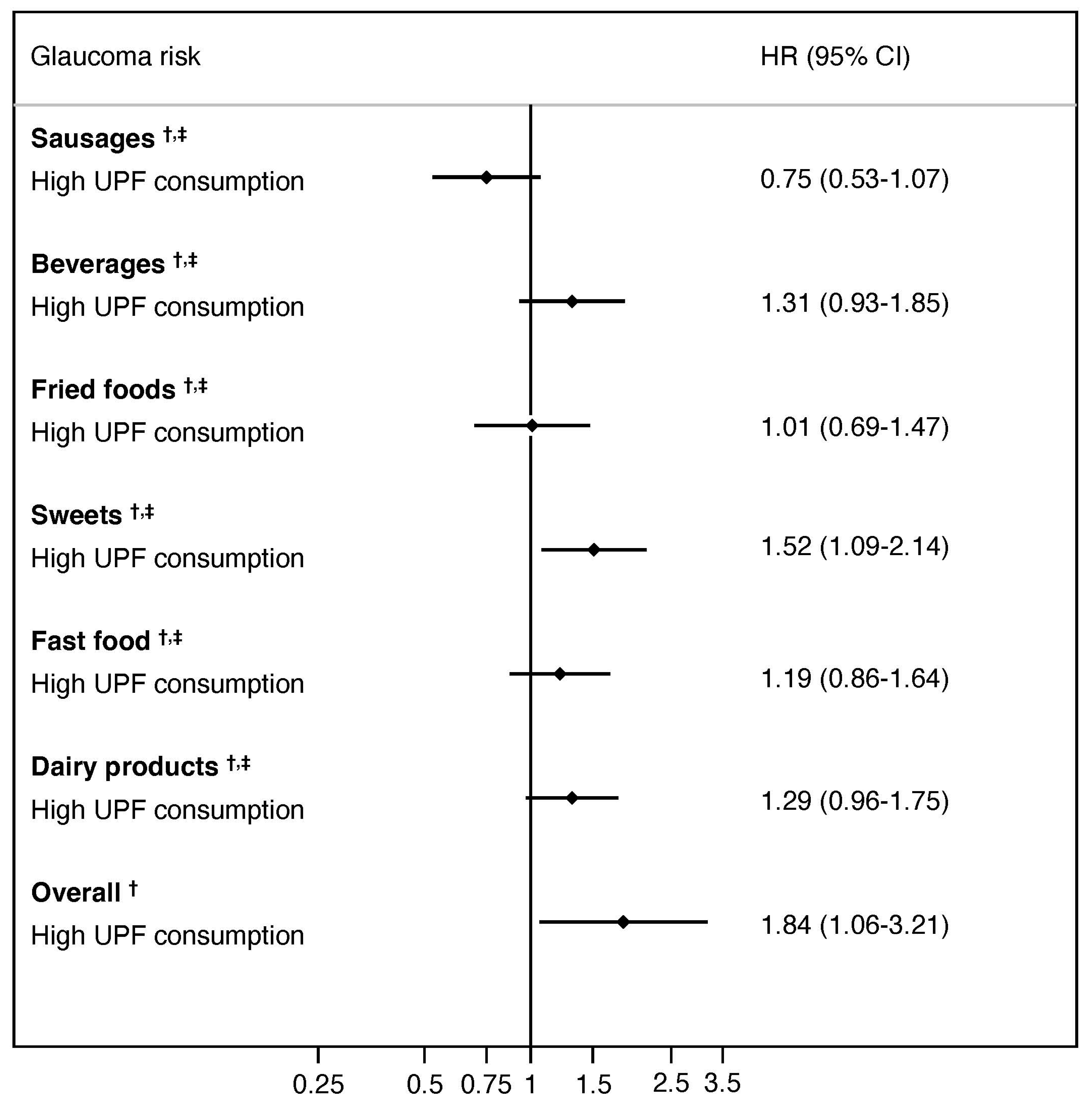
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stein, J.D.; Khawaja, A.P.; Weizer, J.S. Glaucoma in Adults—Screening, Diagnosis, and Management: A Review. JAMA 2021, 325, 164. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The Pathophysiology and Treatment of Glaucoma: A Review. JAMA 2014, 311, 1901. [Google Scholar] [CrossRef] [PubMed]
- Quigley, H.A. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Perez, C.I.; Singh, K.; Lin, S. Relationship of lifestyle, exercise, and nutrition with glaucoma. Curr. Opin. Ophthalmol. 2019, 30, 82–88. [Google Scholar] [CrossRef]
- Fahmideh, F.; Marchesi, N.; Barbieri, A.; Govoni, S.; Pascale, A. Non-drug interventions in glaucoma: Putative roles for lifestyle, diet and nutritional supplements. Surv. Ophthalmol. 2022, 67, 675–696. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, M.A.; Baker, P.I. Ultra-processed food and adverse health outcomes. BMJ 2019, 384, l2289. [Google Scholar] [CrossRef] [PubMed]
- Fardet, A.; Rock, E. Ultra-processed foods: A new holistic paradigm? Trends Food Sci. Technol. 2019, 93, 174–184. [Google Scholar] [CrossRef]
- Elizabeth, L.; Machado, P.; Zinöcker, M.; Baker, P.; Lawrence, M. Ultra-Processed Foods and Health Outcomes: A Narrative Review. Nutrients 2020, 12, 1955. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization. Ultra-Processed Food and Drink Products in Latin America: Sales, Sources, Nutrient Profiles, and Policy Implications; PAHO: Washington, DC, USA, 2019. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Levy, R.; Moubarac, J.-C.; Jaime, P.; Martins, A.P.; Canella, D.; Louzada, M.; Parra, D. The star shines bright. World Nutr. 2016, 7, 28–38. [Google Scholar]
- Monteiro, C.A. Nutrition and health. The issue is not food, nor nutrients, so much as processing. Public. Health Nutr. 2009, 12, 729–731. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.J. The role of the transnational ultra-processed food industry in the pandemic of obesity and its associated diseases: Problems and solutions. World Nutr. 2019, 10, 89–99. [Google Scholar] [CrossRef]
- Chang, K.; Gunter, M.J.; Rauber, F.; Levy, R.B.; Huybrechts, I.; Kliemann, N.; Millett, C.; Vamos, E.P. Ultra-processed food consumption, cancer risk and cancer mortality: A large-scale prospective analysis within the UK Biobank. eClinicalMedicine 2023, 56, 101840. [Google Scholar] [CrossRef]
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D.; Global Burden of Diseases Nutrition and Chronic Diseases Expert Group (NutriCoDE). Dietary quality among men and women in 187 countries in 1990 and 2010: A systematic assessment. Lancet Glob. Health 2015, 3, e132–e142. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Rojo, R.; Sandoval-Insausti, H.; López-Garcia, E.; Graciani, A.; Ordovás, J.M.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Consumption of Ultra-Processed Foods and Mortality: A National Prospective Cohort in Spain. Mayo Clin. Proc. 2019, 94, 2178–2188. [Google Scholar] [CrossRef] [PubMed]
- Latasa, P.; Louzada, M.L.D.C.; Martinez Steele, E.; Monteiro, C.A. Added sugars and ultra-processed foods in Spanish households (1990–2010). Eur. J. Clin. Nutr. 2018, 72, 1404–1412. [Google Scholar] [CrossRef]
- Moreno-Montañés, J.; Gutierrez-Ruiz, I.; Gándara, E.; Moreno-Galarraga, L.; Santiago, S.; Ruiz-Canela, M.; Martínez-González, J.; Martínez-González, M.Á.; Fernandez-Montero, A. Carbohydrate intake and risk of glaucoma in the sun cohort. Eur. J. Ophthalmol. 2022, 32, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Desmettre, T.; Rouland, J.F. Hypothèses sur le rôle des facteurs nutritionnels au cours des hypertonies oculaires et du glaucome. J. Français D’ophtalmologie 2005, 28, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Ramdas, W.D. The relation between dietary intake and glaucoma: A systematic review. Acta Ophthalmol. 2018, 96, 550–556. [Google Scholar] [CrossRef]
- Moreno-Montañés, J.; Gándara, E.; Moreno-Galarraga, L.; Hershey, M.S.; López-Gil, J.F.; Kales, S.; Bes-Rastrollo, M.; Martínez-González, M.Á.; Fernandez-Montero, A. ACE-Vitamin Index and Risk of Glaucoma: The SUN Project. Nutrients 2022, 14, 5129. [Google Scholar] [CrossRef]
- European Glaucoma Society. Terminology and Guidelines for Glaucoma, 5th ed.; Publicomm: Savona, Italy, 2020. [Google Scholar]
- de la Fuente-Arrillaga, C.; Vázquez Ruiz, Z.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ validated in Spain. Public. Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and Validation of a Food Frequency Questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- Llavero-Valero, M.; Escalada-San Martín, J.; Martínez-González, M.A.; Basterra-Gortari, F.J.; de la Fuente-Arrillaga, C.; Bes-Rastrollo, M. Ultra-processed foods and type-2 diabetes risk in the SUN project: A prospective cohort study. Clin. Nutr. 2021, 40, 2817–2824. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Donoso, C.; Sánchez-Villegas, A.; Martínez-González, M.A.; Gea, A.; Mendonça, R.D.; Lahortiga-Ramos, F.; Bes-Rastrollo, M. Ultra-processed food consumption and the incidence of depression in a Mediterranean cohort: The SUN Project. Eur. J. Nutr. 2020, 59, 1093–1103. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Fardet, A.; Méjean, C.; Labouré, H.; Andreeva, V.A.; Feron, G. The degree of processing of foods which are most widely consumed by the French elderly population is associated with satiety and glycemic potentials and nutrient profiles. Food Funct. 2017, 8, 651–658. [Google Scholar] [CrossRef]
- Machado, P.P.; Steele, E.M.; Louzada, M.L.D.C.; Levy, R.B.; Rangan, A.; Woods, J.; Gill, T.; Scrinis, G.; Monteiro, C.A. Ultra-processed food consumption drives excessive free sugar intake among all age groups in Australia. Eur. J. Nutr. 2020, 59, 2783–2792. [Google Scholar] [CrossRef] [PubMed]
- Bejarano, E.; Taylor, A. Too sweet: Problems of protein glycation in the eye. Exp. Eye Res. 2019, 178, 255–262. [Google Scholar] [CrossRef] [PubMed]
- D’Cunha, N.M.; Sergi, D.; Lane, M.M.; Naumovski, N.; Gamage, E.; Rajendran, A.; Kouvari, M.; Gauci, S.; Dissanayka, T.; Marx, W.; et al. The Effects of Dietary Advanced Glycation End-Products on Neurocognitive and Mental Disorders. Nutrients 2022, 14, 2421. [Google Scholar] [CrossRef] [PubMed]
- Nita, M.; Grzybowski, A. The Role of the Reactive Oxygen Species and Oxidative Stress in the Pathomechanism of the Age-Related Ocular Diseases and Other Pathologies of the Anterior and Posterior Eye Segments in Adults. Oxidative Med. Cell. Longev. 2016, 2016, 3164734. [Google Scholar] [CrossRef] [PubMed]
- Hussain, T.; Tan, B.; Yin, Y.; Blachier, F.; Tossou, M.C.B.; Rahu, N. Oxidative Stress and Inflammation: What Polyphenols Can Do for Us? Oxidative Med. Cell. Longev. 2016, 2016, 7432797. [Google Scholar] [CrossRef]
- Lamport, D.J.; Laville, M.; Lawton, C.L.; Meheust, A.; Nilson, A.; Normand, S.; Rivellese, A.A.; Theis, S.; Torekov, S.S.; Vinoy, S. Impact of postprandial glycaemia on health and prevention of disease. Obes. Rev. 2012, 13, 923–984. [Google Scholar] [CrossRef]
- Mignogna, C.; Costanzo, S.; Di Castelnuovo, A.; Ruggiero, E.; Shivappa, N.; Hebert, J.R.; Esposito, S.; De Curtis, A.; Persichillo, M.; Cerletti, C.; et al. The inflammatory potential of the diet as a link between food processing and low-grade inflammation: An analysis on 21,315 participants to the Moli-sani study. Clin. Nutr. 2022, 41, 2226–2234. [Google Scholar] [CrossRef] [PubMed]
- Bahrampour, N.; Shiraseb, F.; Noori, S.; Clark, C.C.T.; Mirzaei, K. Is there any putative mediatory role of inflammatory markers on the association between ultra-processed foods and resting metabolic rate? Front. Nutr. 2022, 9, 932225. [Google Scholar] [CrossRef]
- Silva Dos Santos, F.; Costa Mintem, G.; Oliveira de Oliveira, I.; Lessa Horta, B.; Ramos, E.; Lopes, C.; Petrucci Gigante, D. Consumption of ultra-processed foods and interleukin-6 in two cohorts from high- and middle-income countries. Br. J. Nutr. 2022, 21, 1–28. [Google Scholar] [CrossRef]
- Echevarria, F.D.; Formichella, C.R.; Sappington, R.M. Interleukin-6 Deficiency Attenuates Retinal Ganglion Cell Axonopathy and Glaucoma-Related Vision Loss. Front. Neurosci. 2017, 11, 318. [Google Scholar] [CrossRef] [PubMed]
- Poti, J.M.; Braga, B.; Qin, B. Ultra-processed Food Intake and Obesity: What Really Matters for Health—Processing or Nutrient Content? Curr. Obes. Rep. 2017, 6, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Paula Neto, H.A.; Ausina, P.; Gomez, L.S.; Leandro, J.G.B.; Zancan, P.; Sola-Penna, M. Effects of Food Additives on Immune Cells As Contributors to Body Weight Gain and Immune-Mediated Metabolic Dysregulation. Front. Immunol. 2017, 8, 1478. [Google Scholar] [CrossRef] [PubMed]
- Martini, D.; Godos, J.; Bonaccio, M.; Vitaglione, P.; Grosso, G. Ultra-Processed Foods and Nutritional Dietary Profile: A Meta-Analysis of Nationally Representative Samples. Nutrients 2021, 13, 3390. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Ray, R.M.; Tussing-Humphreys, L.M.; Pasquale, L.R.; Maki, P.; Haan, M.N.; Jackson, R.; Vajaranant, T.S. Effect of Low-Fat Dietary Modification on Incident Open-Angle Glaucoma. Ophthalmology 2022, 130, S0161642022009150. [Google Scholar] [CrossRef] [PubMed]
- Russo, R.; Nucci, C.; Adornetto, A. The promise of neuroprotection by dietary restriction in glaucoma. Neural. Regen. Res. 2022, 17, 45. [Google Scholar] [CrossRef]
- Lin, H.C.; Stein, J.D.; Nan, B.; Childers, D.; Newman-Casey, P.A.; Thompson, D.A.; Richards, J.E. Association of Geroprotective Effects of Metformin and Risk of Open-Angle Glaucoma in Persons with Diabetes Mellitus. JAMA Ophthalmol. 2015, 133, 915. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Giovannucci, E.L. Ultra-processed foods and health: A comprehensive review. Crit. Rev. Food Sci. Nutr. 2022, 63, 10836–10848. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Levy, R.B.; Claro, R.M.; de Castro, I.R.R.; Cannon, G. Increasing consumption of ultra-processed foods and likely impact on human health: Evidence from Brazil. Public. Health Nutr. 2010, 14, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Willett, W.C.; Rosner, B.A.; Buys, E.; Wiggs, J.L.; Pasquale, L.R. Association of Dietary Nitrate Intake with Primary Open-Angle Glaucoma: A Prospective Analysis From the Nurses’ Health Study and Health Professionals Follow-up Study. JAMA Ophthalmol. 2016, 134, 294. [Google Scholar] [CrossRef] [PubMed]
- Marhuenda-Muñoz, M.; Rinaldi de Alvarenga, J.F.; Hernáez, Á.; Tresserra-Rimbau, A.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Malcampo, M.; Martínez, J.A.; Alonso-Gómez, Á.M.; et al. High Fruit and Vegetable Consumption and Moderate Fat Intake Are Associated with Higher Carotenoid Concentration in Human Plasma. Antioxidants 2021, 10, 473. [Google Scholar] [CrossRef] [PubMed]
- Lawler, T.; Liu, Y.; Christensen, K.; Vajaranant, T.S.; Mares, J. Dietary Antioxidants, Macular Pigment, and Glaucomatous Neurodegeneration: A Review of the Evidence. Nutrients 2019, 11, 1002. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Group | Included Foods |
|---|---|
| Unprocessed or minimally processed foods | Vegetables, fruit, grains (including white rice and pasta), legumes, milk (whole, semi-skimmed, and nonfat), eggs, meats, poultry, fish and seafood, fermented milk like yogurt, water, natural juice, and coffee. |
| Processed culinary ingredients | Vegetable oils (olive, sunflower, corn), lard, sugar, chili, butter salt and honey. |
| Processed foods | Breads (both white and whole), cured traditional ham, bacon, condensed milk, cream, various cheeses, canned and bottled fruit, wine, and beer. |
| Ultra-processed foods | Potato chips, pizza, preprepared pies, breakfast cereals, margarine, cookies and chocolate cookies, doughnuts, muffins, croissants or other non-handmade pastries, cakes, churros, chocolates and candies, marzipan, nougat, carbonated drinks, artificially sugared beverages, fruit drinks, milkshakes, instant creams and soups, mayonnaise, and alcoholic drinks produced by fermentation followed by distillation such as whisky, gin, and rum. Whereas items such as ice cream, petit-suisse, flan, pudding, custard, processed meats (chorizo, salami, mortadella, sausage, hamburger, morcilla), ham, spicy sausage/meatballs, croquettes, pâté, and foie-gras. |
| Variable | UPF (up to 1 Serving/Day) | UPF (>1 to 3 Servings/Day) | UPF (>3 to 4 Servings/Day) | UPF (>4 Servings/Day) | p-Value |
|---|---|---|---|---|---|
| Participants, n (%) a | 1004 (5.2) | 8237 (42.8) | 4196 (21.8) | 5818 (30.2) | |
| UPF, servings/day | 0.7 (0.2) | 2.1 (0.5) | 3.5 (0.3) | 5.4 (1.5) | <0.001 |
| Age, years | 47.8 (12.6) | 40.7 (12.6) | 36.5 (11.6) | 34.3 (10.8) | <0.001 |
| Sex, women, n (%) | 643 (64.0) | 5163 (62.7) | 2587 (61.7) | 3176 (54.6) | <0.001 |
| University education, years | 5.1 (1.6) | 5.1 (1.5) | 5.0 (1.5) | 5.0 (1.5) | 0.380 |
| BMI, kg/m2 | 24.0 (3.5) | 23.7 (3.6) | 23.4 (3.5) | 23.4 (3.5) | <0.001 |
| Physical activity, METs-h/week | 22.8 (23.5) | 21.5 (22.6) | 21.3 (21.8) | 22.5 (24.2) | 0.012 |
| Total energy intake, kcal/day | 1687 (542) | 2074 (529) | 2404 (497) | 2777 (515) | <0.001 |
| Carbohydrates intake, % of energy | 32.8 (8.5) | 35.5 (6.8) | 36.7 (6.0) | 37.5 (6.0) | 0.003 |
| Protein intake, % of energy | 20.6 (4.9) | 19.0 (3.4) | 18.1 (2.8) | 17.0 (2.7) | <0.001 |
| Fat intake, % of energy | 44.1 (10.2) | 43.3 (7.8) | 43.3 (6.8) | 43.6 (7.0) | <0.001 |
| Adherence to the MedDiet, 0 to 9 score | 4.9 (1.7) | 4.4 (1.8) | 4.1 (1.8) | 3.8 (1.7) | <0.001 |
| Omega 3:6 intake ratio | 0.3 (0.3) | 0.2 (0.1) | 0.2 (0.1) | 0.1 (0.1) | <0.001 |
| Caffeine intake, mg/day | 34.1 (38.3) | 38.3 (36.5) | 42.1 (36.4) | 49.9 (45.0) | <0.001 |
| Ethanol intake, g/day | 6.0 (10.6) | 6.4 (9.9) | 6.5 (9.0) | 7.4 (11.2) | <0.001 |
| Smoking, packages-year b | 10.3 (13.5) | 7.2 (10.8) | 5.5 (9.1) | 4.8 (8.6) | <0.001 |
| Special diet, yes, n (%) | 190 (18.9) | 826 (10.0) | 293 (7.0) | 308 (5.3) | <0.001 |
| Cancer, n (%) | 45 (4.5) | 258 (3.1) | 104 (2.5) | 105 (1.8) | <0.001 |
| Hypertension, n (%) | 190 (18.9) | 1010 (12.3) | 376 (9.0) | 487 (8.4) | <0.001 |
| Type 2 diabetes, n (%) | 52 (5.2) | 181 (2.2) | 51 (1.2) | 76 (1.3) | <0.001 |
| CVD, n (%) | 37 (3.7) | 151 (1.8) | 52 (1.2) | 64 (1.1) | <0.001 |
| Variable | UPF (up to 1 Serving/Day) | UPF (>1 to 3 Servings/Day) | UPF (>3 to 4 Servings/Day) | UPF (>4 Servings/Day) | For Each Serving/Day Increment | p for Trend |
|---|---|---|---|---|---|---|
| Participants, n (%) a | 961 (5.0%) | 8585 (44.6%) | 4292 (22.3%) | 5417 (28.1%) | 19,255 | |
| Glaucoma cases, n (%) | 24 (2.5%) | 156 (1.8%) | 61 (1.4%) | 73 (1.3%) | 314 | |
| Persons/year | 12,540 | 107,286 | 54,899 | 73,563 | 24,828 | |
| Model 0, HR (95% CI) | 1 (Reference) | 1.16 (0.75–1.79) | 1.22 (0.76–1.97) | 1.36 (0.85–2.17) | 1.04 0.97–1.11) | 0.172 |
| Model 1, HR (95% CI) b | 1 (Reference) | 1.28 (0.83–1.97) | 1.41 (0.87–2.27) | 1.61 (1.00–2.50) | 1.07 (1.00–1.14) | 0.009 |
| Model 2, HR (95% CI) b | 1 (Reference) | 1.30 (0.84–2.01) | 1.44 (0.89–2.34) | 1.65 (1.02–2.67) | 1.07 (1.00–1.14) | 0.091 |
| Model 3, HR (95% CI) b | 1 (Reference) | 1.42 (0.90–2.23) | 1.62 (0.95–2.74) | 1.82 (1.04–3.16) | 1.07 (0.98–1.16) | 0.004 |
| Model 4, HR (95% CI) b | 1 (Reference) | 1.43 (0.91–2.26) | 1.66 (0.98–2.81) | 1.84 (1.06–3.21) | 1.07 (0.99–1.16) | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Gil, J.F.; Fernandez-Montero, A.; Bes-Rastrollo, M.; Moreno-Galarraga, L.; Kales, S.N.; Martínez-González, M.Á.; Moreno-Montañés, J. Is Ultra-Processed Food Intake Associated with a Higher Risk of Glaucoma? A Prospective Cohort Study including 19,255 Participants from the SUN Project. Nutrients 2024, 16, 1053. https://doi.org/10.3390/nu16071053
López-Gil JF, Fernandez-Montero A, Bes-Rastrollo M, Moreno-Galarraga L, Kales SN, Martínez-González MÁ, Moreno-Montañés J. Is Ultra-Processed Food Intake Associated with a Higher Risk of Glaucoma? A Prospective Cohort Study including 19,255 Participants from the SUN Project. Nutrients. 2024; 16(7):1053. https://doi.org/10.3390/nu16071053
Chicago/Turabian StyleLópez-Gil, José Francisco, Alejandro Fernandez-Montero, Maira Bes-Rastrollo, Laura Moreno-Galarraga, Stefanos N. Kales, Miguel Ángel Martínez-González, and Javier Moreno-Montañés. 2024. "Is Ultra-Processed Food Intake Associated with a Higher Risk of Glaucoma? A Prospective Cohort Study including 19,255 Participants from the SUN Project" Nutrients 16, no. 7: 1053. https://doi.org/10.3390/nu16071053
APA StyleLópez-Gil, J. F., Fernandez-Montero, A., Bes-Rastrollo, M., Moreno-Galarraga, L., Kales, S. N., Martínez-González, M. Á., & Moreno-Montañés, J. (2024). Is Ultra-Processed Food Intake Associated with a Higher Risk of Glaucoma? A Prospective Cohort Study including 19,255 Participants from the SUN Project. Nutrients, 16(7), 1053. https://doi.org/10.3390/nu16071053