
Bile Acids and Risk of Adverse Cardiovascular Events and All-Cause Mortality in Patients with Acute Coronary Syndrome

 , , , ,
, , , ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Ascertainment of the Outcomes
2.3. Bile Acids Profiling
2.4. Covariate Assessment
2.5. Statistical Analyses
2.5.1. Univariate Analyses
2.5.2. Multivariate Analyses
3. Results
3.1. Baseline Characteristics of the Population
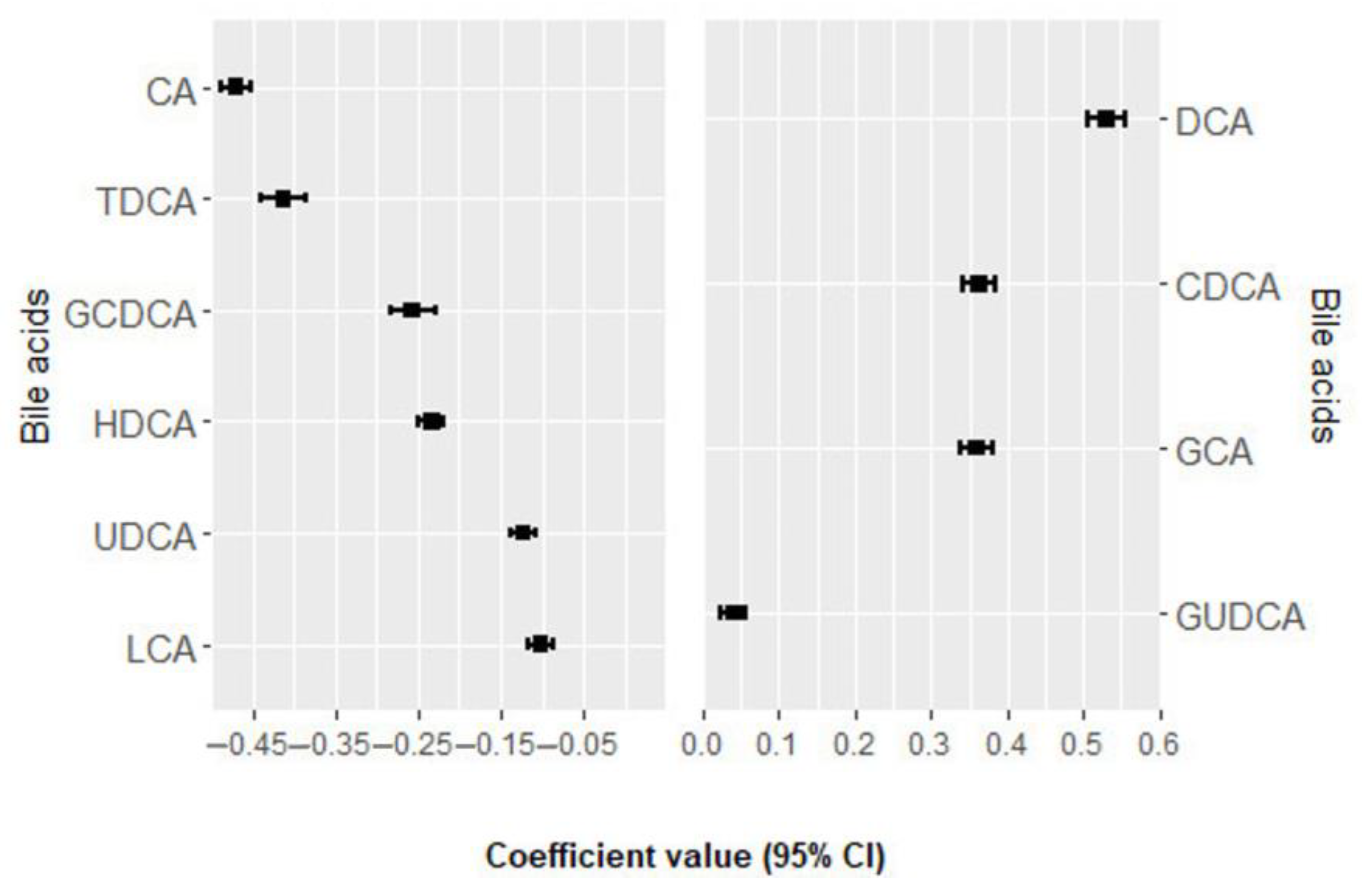
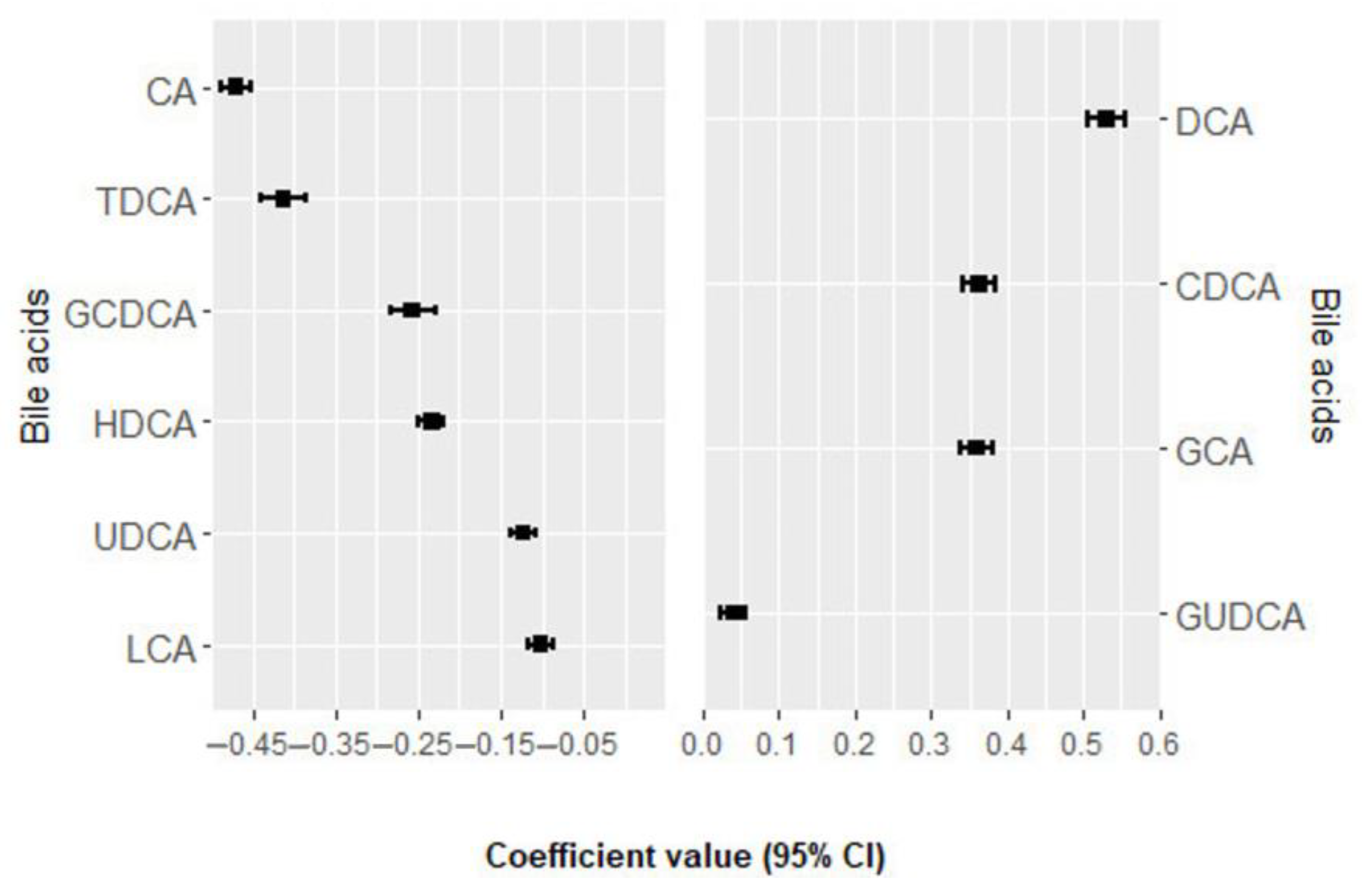
3.2. Association of Bile Acids with MACE
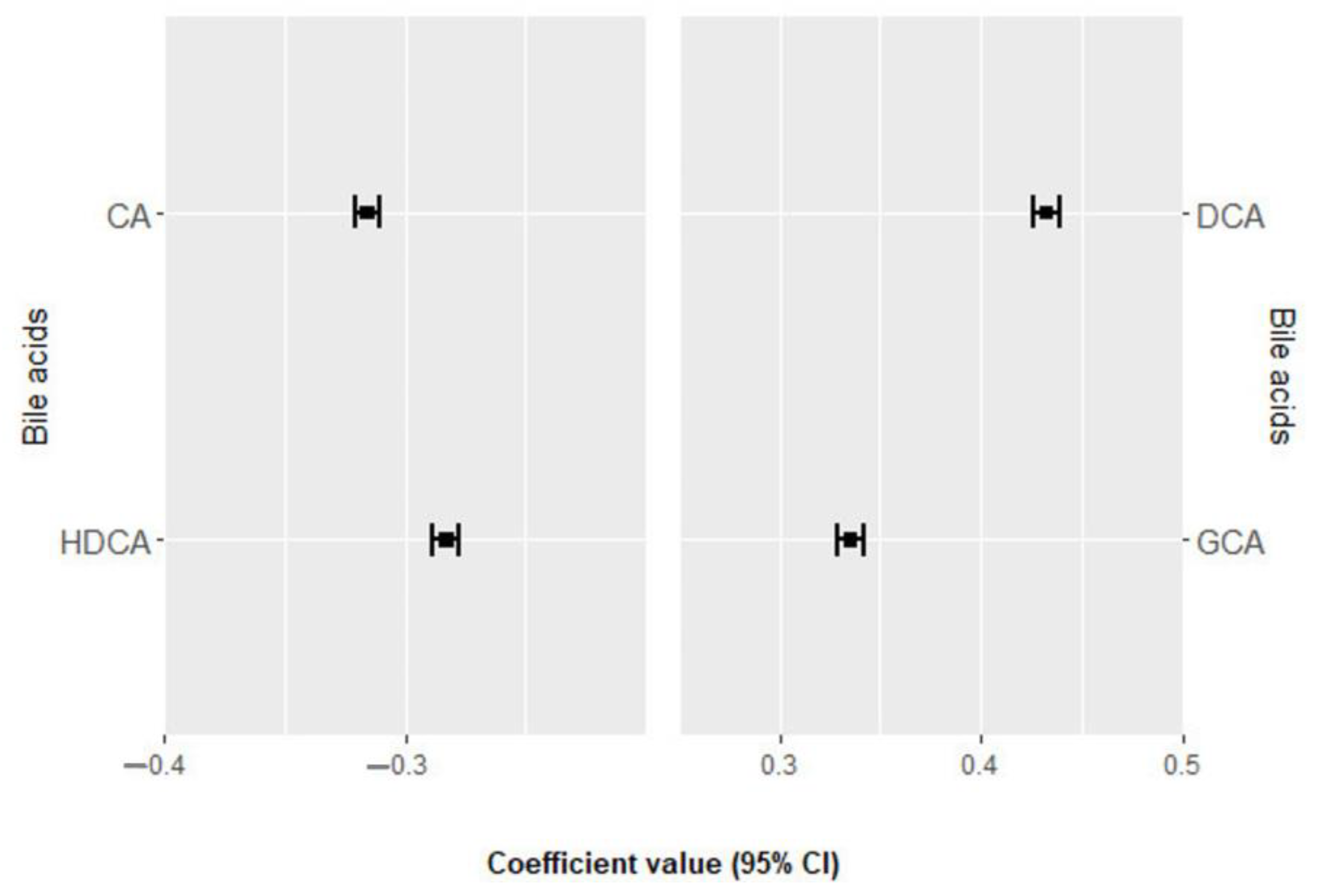
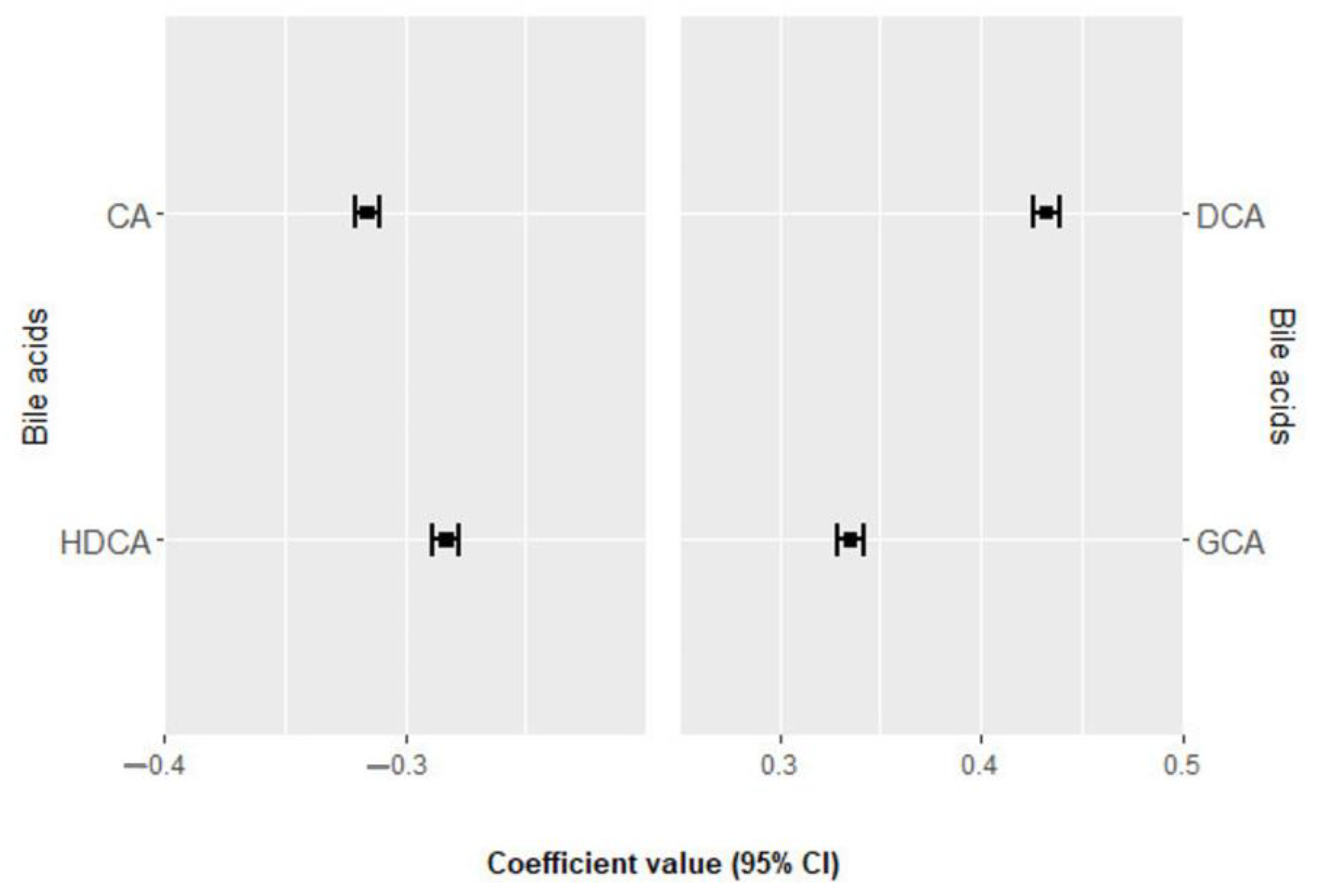
3.3. Association of Bile Acids with All-Cause Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, J.N.; Negrelli, J.M.; Manek, M.B.; Hawes, E.M.; Viera, A.J. Diagnosis and Management of Acute Coronary Syndrome: An Evidence-Based Update. J. Am. Board Fam. Med. 2015, 28, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-gimenez, R.; Peiró, Ó.M.; Bonet, G.; Bulló, M.; Papandreou, C. Plasma Trimethylamine-N-Oxide, Its Precursors and Risk of Cardiovascular Events in Patients with Acute Coronary Syndrome: Mediating Effects of Renal Function. Front. Cardiovasc. Med. 2023, 9, 1000815. [Google Scholar] [CrossRef] [PubMed]
- Surendran, A.; Atefi, N.; Zhang, H.; Aliani, M.; Ravandi, A. Defining Acute Coronary Syndrome through Metabolomics. Metabolites 2021, 11, 685. [Google Scholar] [CrossRef] [PubMed]
- Li, M.N.; Qian, S.H.; Yao, Z.Y.; Ming, S.P.; Shi, X.J.; Kang, P.F.; Zhang, N.R.; Wang, X.J.; Gao, D.S.; Gao, Q.; et al. Correlation of Serum N-Acetylneuraminic Acid with the Risk and Prognosis of Acute Coronary Syndrome: A Prospective Cohort Study. BMC Cardiovasc. Disord. 2020, 20, 404. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Gimenez, R.; Peiró, Ó.M.; Bonet, G.; Carrasquer, A.; Fragkiadakis, G.A.; Bulló, M.; Papandreou, C.; Bardaji, A. TCA Cycle Metabolites Associated with Adverse Outcomes after Acute Coronary Syndrome: Mediating Effect of Renal Function. Front. Cardiovasc. Med. 2023, 10, 1157325. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Gimenez, R.; Ahmed-Khodja, W.; Molina, Y.; Peiró, O.M.; Bonet, G.; Carrasquer, A.; Fragkiadakis, G.A.; Bulló, M.; Bardaji, A.; Papandreou, C. Gut Microbiota-Derived Metabolites and Cardiovascular Disease Risk: A Systematic Review of Prospective Cohort Studies. Nutrients 2022, 14, 2654. [Google Scholar] [CrossRef] [PubMed]
- Heianza, Y.; Ma, W.; Manson, J.A.E.; Rexrode, K.M.; Qi, L. Gut Microbiota Metabolites and Risk of Major Adverse Cardiovascular Disease Events and Death: A Systematic Review and Meta-Analysis of Prospective Studies. J. Am. Heart Assoc. 2017, 6, e004947. [Google Scholar] [CrossRef] [PubMed]
- Guzior, D.V.; Quinn, R.A. Review: Microbial Transformations of Human Bile Acids. Microbiome 2021, 9, 140. [Google Scholar] [CrossRef]
- Di Ciaula, A.; Garruti, G.; Baccetto, R.L.; Molina-Molina, E.; Bonfrate, L.; Wang, D.Q.H.; Portincasa, P. Bile Acid Physiology. Ann. Hepatol. 2017, 16, s4–s14. [Google Scholar] [CrossRef]
- Jin, M.; Qian, Z.; Yin, J.; Xu, W.; Zhou, X. The Role of Intestinal Microbiota in Cardiovascular Disease. J. Cell. Mol. Med. 2019, 23, 2343–2350. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.T.; Wang, J.; Liang, Y.; Wu, X.Y.; Li, W.Q.; Wang, Y.H.; Jing, A.R.; Liang, M.M.; Sun, L.; Dou, J.; et al. The Level of Serum Total Bile Acid Is Related to Atherosclerotic Lesions, Prognosis and Gut Lactobacillus in Acute Coronary Syndrome Patients. Ann. Med. 2023, 55, 2232369. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Alpert, J.S.; White, H.D.; Zealand, N.; Allan, S.; Germany, H.A.K.; Denmark, P.M.C.; et al. Third Universal Definition of Myocardial Infarction. Eur. Heart J. 2012, 33, 2551–2567. [Google Scholar] [CrossRef] [PubMed]
- Mateu-Fabregat, J.; Mostafa, H.; Sanchez-Gimenez, R.; Peiró, Ó.M.; Bonet, G.; Carrasquer, A.; Fragkiadakis, G.A.; Bardaji, A.; Bulló, M.; Papandreou, C. Bile Acids and Risk of Adverse Cardiovascular Events and All-Cause Mortality in Patients with Acute Coronary Syndrome; Mendeley Data: London, UK, 2023; Version 1. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate? Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, S.; Bohlin, J. Statistical Predictions with Glmnet. Clin. Epigenetics 2019, 11, 123. [Google Scholar] [CrossRef] [PubMed]
- Gromski, P.; Xu, Y.; Kotze, H.; Correa, E.; Ellis, D.; Armitage, E.; Turner, M.; Goodacre, R. Influence of Missing Values Substitutes on Multivariate Analysis of Metabolomics Data. Metabolites 2014, 4, 433–452. [Google Scholar] [CrossRef] [PubMed]
- Alhmoud, T.; Kumar, A.; Lo, C.C.; Al-Sadi, R.; Clegg, S.; Alomari, I.; Zmeili, T.; Gleasne, C.D.; Mcmurry, K.; Dichosa, A.E.K.; et al. Investigating Intestinal Permeability and Gut Microbiota Roles in Acute Coronary Syndrome Patients. Hum. Microbiome J. 2019, 13, 100059. [Google Scholar] [CrossRef] [PubMed]
- Shin, N.R.; Whon, T.W.; Bae, J.W. Proteobacteria: Microbial Signature of Dysbiosis in Gut Microbiota. Trends Biotechnol. 2015, 33, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Jie, Z.; Xia, H.; Zhong, S.L.; Feng, Q.; Li, S.; Liang, S.; Zhong, H.; Liu, Z.; Gao, Y.; Zhao, H.; et al. The Gut Microbiome in Atherosclerotic Cardiovascular Disease. Nat. Commun. 2017, 8, 845. [Google Scholar] [CrossRef] [PubMed]
- Emoto, T.; Yamashita, T.; Sasaki, N.; Hirota, Y.; Hayashi, T.; So, A.; Kasahara, K.; Yodoi, K.; Matsumoto, T.; Mizoguchi, T.; et al. Analysis of Gut Microbiota in Coronary Artery Disease Patients: A Possible Link between Gut Microbiota and Coronary Artery Disease. J. Atheroscler. Thromb. 2016, 23, 908–921. [Google Scholar] [CrossRef]
- Gurvich, C.; Thomas, N.; Hudaib, A.-R.; Van Rheenen, T.E.; X Thomas, E.H.; Tan, E.J.; Neill, E.; Carruthers, S.P.; Sumner, P.J.; Romano-Silva, M.; et al. The Relationship between Cognitive Clusters and Telomere Length in Bipolar-Schizophrenia Spectrum Disorders. Psychol. Medicne 2023, 53, 5119–5126. [Google Scholar] [CrossRef] [PubMed]
- Prete, R.; Long, S.L.; Gallardo, A.L.; Gahan, C.G.; Corsetti, A.; Joyce, S.A. Beneficial Bile Acid Metabolism from Lactobacillus Plantarum of Food Origin. Sci. Rep. 2020, 10, 1165. [Google Scholar] [CrossRef] [PubMed]
- Wise, J.L.; Cummings, B.P. The 7-α-Dehydroxylation Pathway: An Integral Component of Gut Bacterial Bile Acid Metabolism and Potential Therapeutic Target. Front. Microbiol. 2023, 13, 1093420. [Google Scholar] [CrossRef] [PubMed]
- Monma, T.; Iwamoto, J.; Ueda, H.; Tamamushi, M.; Kakizaki, F.; Konishi, N.; Yara, S.; Miyazaki, T.; Hirayama, T.; Ikegami, T.; et al. Evaluation of Gut Dysbiosis Using Serum and Fecal Bile Acid Profiles. World J. Clin. Cases 2022, 10, 12462–12803. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Iwamoto, J.; Honda, A.; Tsuji, T.; Tamamushi, M.; Ueda, H.; Monma, T.; Konishi, N.; Yara, S.; Hirayama, T.; et al. Detection of Gut Dysbiosis Due to Reduced Clostridium Subcluster XIVa Using the Fecal or Serum Bile Acid Profile. Inflamm. Bowel Dis. 2018, 24, 1035–1044. [Google Scholar] [CrossRef] [PubMed]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet Rapidly and Reproducibly Alters the Human Gut Microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Frazier, R.; Cai, X.; Lee, J.; Bundy, J.D.; Jovanovich, A.; Chen, J.; Deo, R.; Lash, J.P.; Anderson, A.H.; Go, A.S.; et al. Deoxycholic Acid and Risks of Cardiovascular Events, ESKD, and Mortality in CKD: The CRIC Study. Kidney Med. 2022, 4, 100387. [Google Scholar] [CrossRef] [PubMed]
- Proungvitaya, S.; Sombattheera, S.; Boonsiri, P.; Limpaiboon, T.; Wongkham, S.; Wongkham, C.; Titapun, A.; Proungvitaya, T. Diagnostic Value of Serum Bile Acid Composition Patterns and Serum Glycocholic Acid Levels in Cholangiocarcinoma. Oncol. Lett. 2017, 14, 4943–4948. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Ma, J.; Gu, L.; Chen, P.; Chen, L.; Zhang, X. Serum Glycocholic Acid-to-Total Bile Acid Ratio Is Independently Associated with Nonalcoholic Fatty Liver Disease: A Retrospective Cross-Sectional Study. Biomed Res. Int. 2021, 2021, 6698085. [Google Scholar] [CrossRef]
- Zhang, W.; Sun, Y.; Wei, S.; Wei, B.; Xu, X.; Tang, Y. Untargeted Metabolomics Reveals the Mechanism of Quercetin Enhancing the Bioavailability of Ticagrelor. Biomed. Chromatogr. 2021, 35, e5206. [Google Scholar] [CrossRef]
- Yu, X.H.; Sun, J.; Wang, Y.; Zhou, Y. Bin Biomarkers of Unstable Angina Pectoris and Yangxin Decoction Intervention. Medicine 2017, 96, e6998. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Ma, W.Q.; Fu, M.J.; Li, J.; Hu, C.H.; Chen, Y.; Zhou, M.M.; Gao, Z.J.; He, Y.L. Overview of Bile Acid Signaling in the Cardiovascular System. World J. Clin. Cases 2021, 9, 308–320. [Google Scholar] [CrossRef] [PubMed]
- Quante, M.; Iske, J.; Uehara, H.; Minami, K.; Nian, Y.; Maenosono, R.; Matsunaga, T.; Liu, Y.; Azuma, H.; Perkins, D.; et al. Taurodeoxycholic Acid and Valine Reverse Obesity-Associated Augmented Alloimmune Responses and Prolong Allograft Survival. Am. J. Transplant. 2022, 22, 402–413. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Patients (n = 309) |
|---|---|
| Age, years | 64.9 ± 12.3 |
| Men, % | 71.2 |
| Body mass index, kg/m2 | 28.1 ± 4.0 |
| eGFR, (mL/min/1.73 m2) | 81.3 (62.1–96.7) |
| Type 2 diabetes, n (%) | 115 (37.2) |
| Hypertension, n (%) | 209 (67.6) |
| Dyslipidemia, n (%) | 188 (60.8) |
| Smoking | |
| Never, n (%) | 110 (35.6) |
| Former, n (%) | 105 (33.9) |
| Current, n (%) | 94 (30.4) |
| Discharge diagnostic | |
| Unstable angina, n (%) | 49 (15.9) |
| STEMI, n (%) | 68 (22.0) |
| NSTEMI, n (%) | 191 (62.0) |
| Medications | |
| Statins, n (%) | 156 (50.5) |
| Beta-blockers, n (%) | 94 (30.4) |
| Aspirin, n (%) | 125 (40.5) |
| Diuretics, n (%) | 78 (25.2) |
| Oral antidiabetic agents, n (%) | 70 (22.7) |
| Insulin medication, n (%) | 27 (8.7) |
| Bile Acids Score | HR per 1 SD Increment (95% CI) | p Value |
|---|---|---|
| MACE | ||
| Crude model | 1.47 (1.24, 1.74) | <0.001 |
| MV | 1.35 (1.12, 1.63) | 0.0014 |
| All-cause mortality | ||
| Crude model | 1.31 (1.059, 1.613) | 0.012 |
| MV | 1.12 (0.87, 1.41) | 0.368 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mateu-Fabregat, J.; Mostafa, H.; Sanchez-Gimenez, R.; Peiró, Ó.M.; Bonet, G.; Carrasquer, A.; Fragkiadakis, G.A.; Bardaji, A.; Bulló, M.; Papandreou, C. Bile Acids and Risk of Adverse Cardiovascular Events and All-Cause Mortality in Patients with Acute Coronary Syndrome. Nutrients 2024, 16, 1062. https://doi.org/10.3390/nu16071062
Mateu-Fabregat J, Mostafa H, Sanchez-Gimenez R, Peiró ÓM, Bonet G, Carrasquer A, Fragkiadakis GA, Bardaji A, Bulló M, Papandreou C. Bile Acids and Risk of Adverse Cardiovascular Events and All-Cause Mortality in Patients with Acute Coronary Syndrome. Nutrients. 2024; 16(7):1062. https://doi.org/10.3390/nu16071062
Chicago/Turabian StyleMateu-Fabregat, Javier, Hamza Mostafa, Raul Sanchez-Gimenez, Óscar M. Peiró, Gil Bonet, Anna Carrasquer, Georgios A. Fragkiadakis, Alfredo Bardaji, Mònica Bulló, and Christopher Papandreou. 2024. "Bile Acids and Risk of Adverse Cardiovascular Events and All-Cause Mortality in Patients with Acute Coronary Syndrome" Nutrients 16, no. 7: 1062. https://doi.org/10.3390/nu16071062
APA StyleMateu-Fabregat, J., Mostafa, H., Sanchez-Gimenez, R., Peiró, Ó. M., Bonet, G., Carrasquer, A., Fragkiadakis, G. A., Bardaji, A., Bulló, M., & Papandreou, C. (2024). Bile Acids and Risk of Adverse Cardiovascular Events and All-Cause Mortality in Patients with Acute Coronary Syndrome. Nutrients, 16(7), 1062. https://doi.org/10.3390/nu16071062