

Online Questionnaire with Fibromyalgia Patients Shows Negative Correlations between Disease Severity and Adherence to Mediterranean Diet
 , ,
, ,  , , ,
, , ,  and
and
Abstract
:1. Introduction
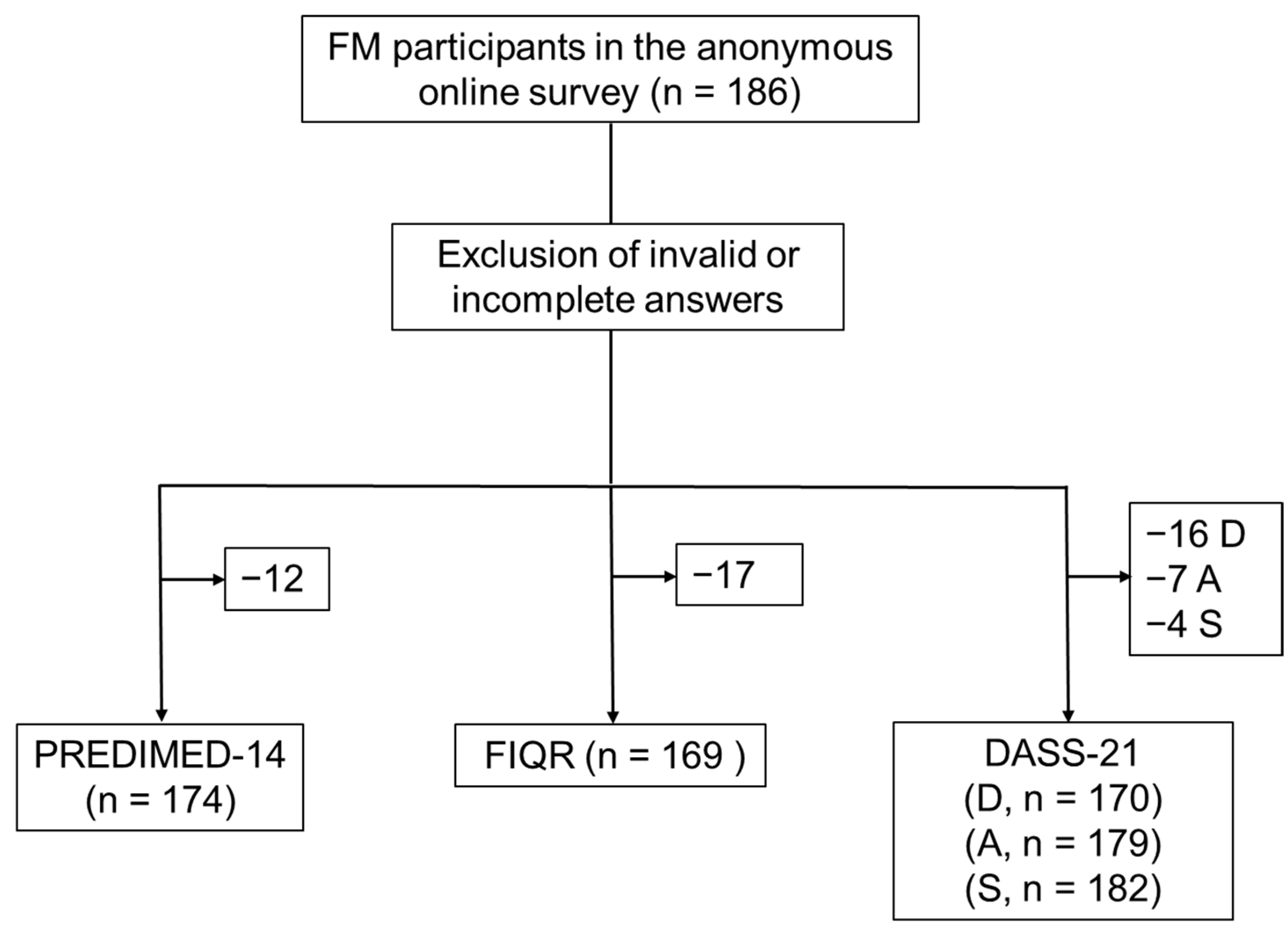
2. Materials and Methods
2.1. Ethical Approval and Patient Recruitment
2.2. Questionnaires
2.3. Statistical Analyses
3. Results
3.1. Demographics and Clinical Characteristics
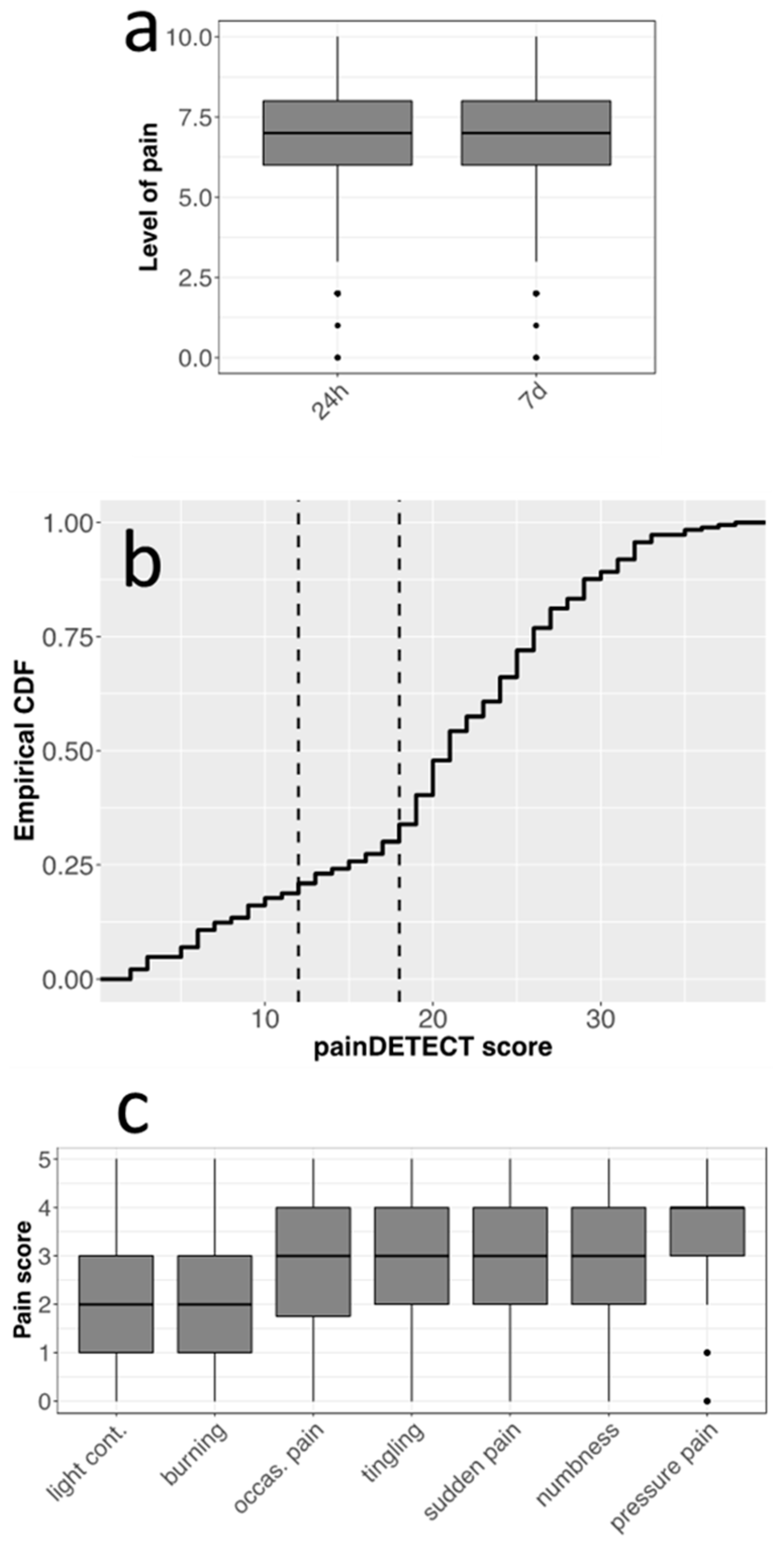
3.2. FM Severity and Symptoms
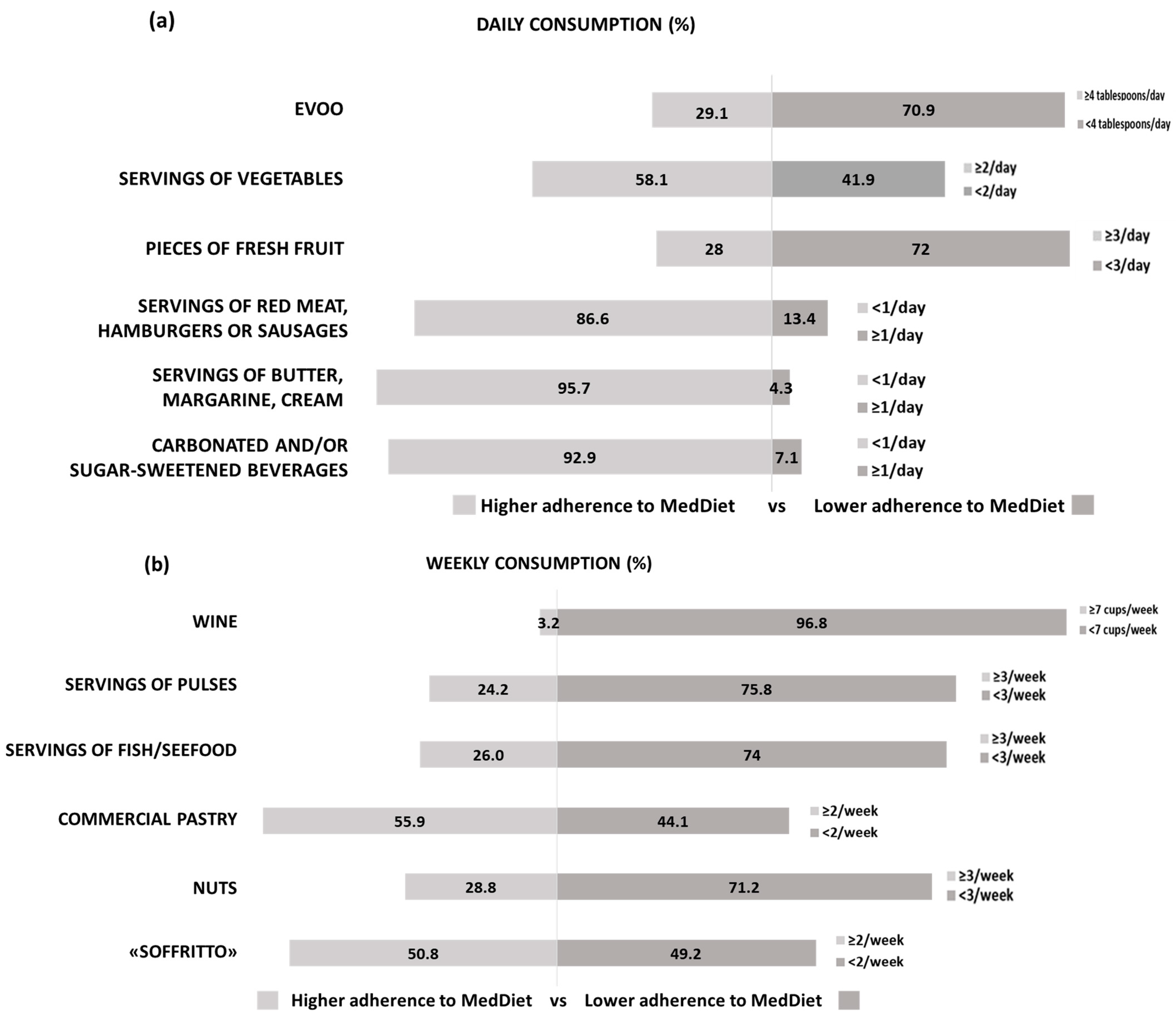
3.3. Eating Habits and MedDiet
3.4. Regression between PREDIMED-14 and FIQR or Pain Metrics
4. Discussion
4.1. Survey Participants Suffered from High-Severity FM
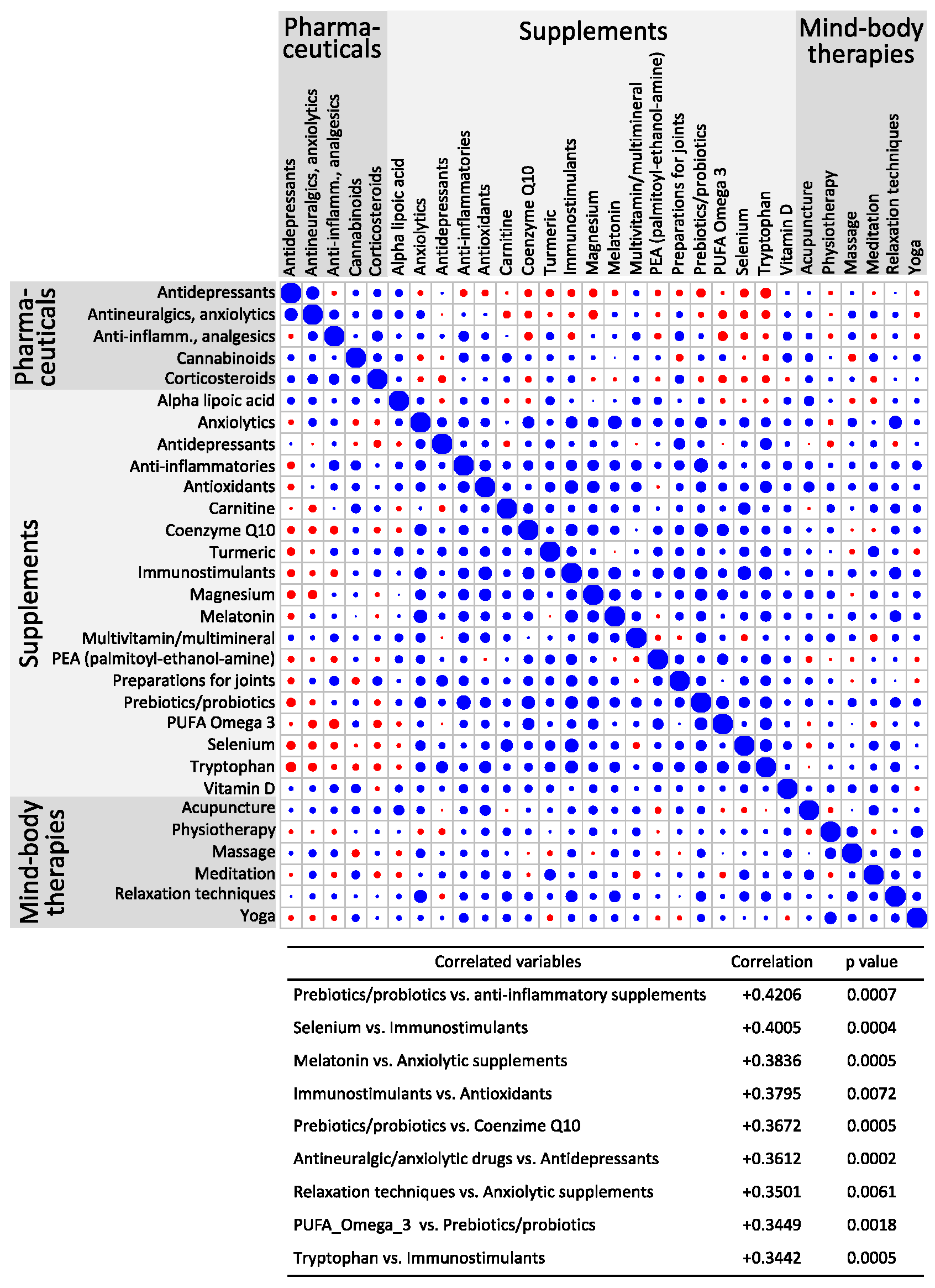
4.2. Survey Participants Extensively Used Pharmaceuticals and Supplements
4.3. FM Patients Should Improve Lifestyle and Eating Habits to Improve Wellbeing
4.4. FM Patients Should Increase the Adherence to the MedDiet
4.5. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clauw, D.J. Fibromyalgia: An overview. Am. J. Med. 2009, 122, S3–S13. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.T.; Atzeni, F.; Beasley, M.; Fluss, E.; Sarzi-Puttini, P.; Macfarlane, G.J. The prevalence of fibromyalgia in the general population: A comparison of the American College of Rheumatology 1990, 2010, and modified 2010 classification criteria. Arthritis Rheumatol. 2015, 67, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Chinn, S.; Caldwell, W.; Gritsenko, K. Fibromyalgia Pathogenesis and Treatment Options Update. Curr. Pain. Headache Rep. 2016, 20, 25. [Google Scholar] [CrossRef] [PubMed]
- Devigili, G.; Di Stefano, G.; Donadio, V.; Frattale, I.; Mantovani, E.; Nolano, M.; Occhipinti, G.; Provitera, V.; Quitadamo, S.; Tamburin, S.; et al. Clinical criteria and diagnostic assessment of fibromyalgia: Position statement of the Italian Society of Neurology-Neuropathic Pain Study Group. Neurol. Sci. 2023, 44, 2561–2574. [Google Scholar] [CrossRef] [PubMed]
- Demori, I.; Molinari, E.; Rapallo, F.; Mucci, V.; Marinelli, L.; Losacco, S.; Burlando, B. Online Questionnaire with Fibromyalgia Patients Reveals Correlations among Type of Pain, Psychological Alterations, and Effectiveness of Non-Pharmacological Therapies. Healthcare 2022, 10, 1975. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Hauser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Maffei, M.E. Fibromyalgia: Recent Advances in Diagnosis, Classification, Pharmacotherapy and Alternative Remedies. Int. J. Mol. Sci. 2020, 21, 7877. [Google Scholar] [CrossRef] [PubMed]
- Siracusa, R.; Paola, R.D.; Cuzzocrea, S.; Impellizzeri, D. Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update. Int. J. Mol. Sci. 2021, 22, 3891. [Google Scholar] [CrossRef] [PubMed]
- Boomershine, C.S. Fibromyalgia: The prototypical central sensitivity syndrome. Curr. Rheumatol. Rev. 2015, 11, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, D.L. Pharmacological treatment of fibromyalgia and other chronic musculoskeletal pain. Best. Pract. Res. Clin. Rheumatol. 2007, 21, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Araujo, F.M.; DeSantana, J.M. Physical therapy modalities for treating fibromyalgia. F1000 Res. 2019, 8, F1000. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Hauser, W.; Fluss, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Ustianowska, K.; Ustianowski, Ł.; Machaj, F.; Gorący, A.; Rosik, J.; Szostak, B.; Szostak, J.; Pawlik, A. The Role of the Human Microbiome in the Pathogenesis of Pain. Int. J. Mol. Sci. 2022, 23, 13267. [Google Scholar] [CrossRef] [PubMed]
- Bjorklund, G.; Dadar, M.; Chirumbolo, S.; Aaseth, J. Fibromyalgia and nutrition: Therapeutic possibilities? Biomed. Pharmacother. 2018, 103, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Holton, K. The role of diet in the treatment of fibromyalgia. Pain Manag. 2016, 6, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Lattanzio, S.M. Fibromyalgia Syndrome: A Metabolic Approach Grounded in Biochemistry for the Remission of Symptoms. Front. Med. 2017, 4, 198. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.R.; Bernardo, A.; Costa, J.; Cardoso, A.; Santos, P.; de Mesquita, M.F.; Vaz Patto, J.; Moreira, P.; Leonor Silva, M.; Padrao, P. Dietary interventions in fibromyalgia: A systematic review. Ann. Med. 2019, 51, 2–14. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Giangrandi, I.; Dinu, M.; Sofi, F.; Colombini, B. Nutritional Interventions in the Management of Fibromyalgia Syndrome. Nutrients 2020, 12, 2525. [Google Scholar] [CrossRef] [PubMed]
- Zelber-Sagi, S.; Salomone, F.; Mlynarsky, L. The Mediterranean dietary pattern as the diet of choice for non-alcoholic fatty liver disease: Evidence and plausible mechanisms. Liver Int. 2017, 37, 936–949. [Google Scholar] [CrossRef] [PubMed]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, A.; Nolen-Doerr, E.; Mantzoros, C.S. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients 2020, 12, 3342. [Google Scholar] [CrossRef] [PubMed]
- Grimes, D.A.; Schulz, K.F. An overview of clinical research: The lay of the land. Lancet 2002, 359, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tolle, T.R. painDETECT: A new screening questionnaire to identify neuropathic components in patients with back pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Salaffi, F.; Franchignoni, F.; Giordano, A.; Ciapetti, A.; Sarzi-Puttini, P.; Ottonello, M. Psychometric characteristics of the Italian version of the revised Fibromyalgia Impact Questionnaire using classical test theory and Rasch analysis. Clin. Exp. Rheumatol. 2013, 31, S41–S49. [Google Scholar] [PubMed]
- Salaffi, F.; Di Carlo, M.; Arca, S.; Galeazzi, M. Categorisation of disease severity states in fibromyalgia: A first step to support decision-making in health care policy. Clin. Exp. Rheumatol. 2018, 36, 1074–1081. [Google Scholar] [PubMed]
- Martinez-Gonzalez, M.A.; Garcia-Arellano, A.; Toledo, E.; Salas-Salvado, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- Masocco, M.; Minardi, V.; Contoli, B.; Minelli, G.; Manno, V.; Cobellis, L.; Greco, D. Sovrappeso e obesità nella popolazione adulta in Italia: Trend temporali, differenze socio-anagrafiche e regionali con focus sulla Regione Campania. Boll. Epidemiol. Naz. 2023, 4, 1–8. [Google Scholar]
- Bailly, F.; Cantagrel, A.; Bertin, P.; Perrot, S.; Thomas, T.; Lansaman, T.; Grange, L.; Wendling, D.; Dovico, C.; Trouvin, A.-P. Part of pain labelled neuropathic in rheumatic disease might be rather nociplastic. RMD Open. 2020, 6, e001326. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Veronese, N.; Di Bella, G.; Cusumano, C.; Parisi, A.; Tagliaferri, F.; Ciriminna, S.; Barbagallo, M. Mediterranean diet in the management and prevention of obesity. Exp. Gerontol. 2023, 174, 112121. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Jauand, M.; Sitges, C.; Femenia, J.; Cifre, I.; Gonzalez, S.; Chialvo, D.; Montoya, P. Age-of-onset of menopause is associated with enhanced painful and non-painful sensitivity in fibromyalgia. Clin. Rheumatol. 2013, 32, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.A.; Clauw, D.J. Understanding fibromyalgia: Lessons from the broader pain research community. J. Pain. 2009, 10, 777–791. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.M.; Bushmakin, A.G.; Cappelleri, J.C.; Zlateva, G.; Sadosky, A.B. Minimal clinically important difference in the fibromyalgia impact questionnaire. J. Rheumatol. 2009, 36, 1304–1311. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.A.; Arnold, L.M. Measures of fibromyalgia: Fibromyalgia Impact Questionnaire (FIQ), Brief Pain Inventory (BPI), Multidimensional Fatigue Inventory (MFI-20), Medical Outcomes Study (MOS) Sleep Scale, and Multiple Ability Self-Report Questionnaire (MASQ). Arthritis Care Res. 2011, 63, S86–S97. [Google Scholar] [CrossRef] [PubMed]
- Lederman, S.; Arnold, L.M.; Vaughn, B.; Kelley, M.; Sullivan, G.M. Efficacy and Safety of Sublingual Cyclobenzaprine for the Treatment of Fibromyalgia: Results from a Randomized, Double-Blind, Placebo-Controlled Trial. Arthritis Care Res. 2023, 75, 2359–2368. [Google Scholar] [CrossRef] [PubMed]
- Tofferi, J.K.; Jackson, J.L.; O’Malley, P.G. Treatment of fibromyalgia with cyclobenzaprine: A meta-analysis. Arthritis Rheum. 2004, 51, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, J.; Shum, B.; Moore, R.A.; Wiffen, P.J.; Gilron, I. Combination pharmacotherapy for the treatment of fibromyalgia in adults. Cochrane Database Syst. Rev. 2018, 2, CD010585. [Google Scholar] [CrossRef] [PubMed]
- Rautiainen, S.; Manson, J.E.; Lichtenstein, A.H.; Sesso, H.D. Dietary supplements and disease prevention—A global overview. Nat. Rev. Endocrinol. 2016, 12, 407–420. [Google Scholar] [CrossRef] [PubMed]
- Makrani, A.H.; Afshari, M.; Ghajar, M.; Forooghi, Z.; Moosazadeh, M. Vitamin D and fibromyalgia: A meta-analysis. Korean J. Pain. 2017, 30, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Haddad, H.W.; Mallepalli, N.R.; Scheinuk, J.E.; Bhargava, P.; Cornett, E.M.; Urits, I.; Kaye, A.D. The Role of Nutrient Supplementation in the Management of Chronic Pain in Fibromyalgia: A Narrative Review. Pain. Ther. 2021, 10, 827–848. [Google Scholar] [CrossRef] [PubMed]
- Yong, W.C.; Sanguankeo, A.; Upala, S. Effect of vitamin D supplementation in chronic widespread pain: A systematic review and meta-analysis. Clin. Rheumatol. 2017, 36, 2825–2833. [Google Scholar] [CrossRef] [PubMed]
- Tague, S.E.; Clarke, G.L.; Winter, M.K.; McCarson, K.E.; Wright, D.E.; Smith, P.G. Vitamin D deficiency promotes skeletal muscle hypersensitivity and sensory hyperinnervation. J. Neurosci. 2011, 31, 13728–13738. [Google Scholar] [CrossRef] [PubMed]
- Lamberg-Allardt, C. Vitamin D in foods and as supplements. Prog. Biophys. Mol. Biol. 2006, 92, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Mohabbat, A.B.; Mahapatra, S.; Jenkins, S.M.; Bauer, B.A.; Vincent, A.; Wahner-Roedler, D.L. Use of Complementary and Integrative Therapies by Fibromyalgia Patients: A 14-Year Follow-up Study. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Engen, D.J.; McAllister, S.J.; Whipple, M.O.; Cha, S.S.; Dion, L.J.; Vincent, A.; Bauer, B.A.; Wahner-Roedler, D.L. Effects of transdermal magnesium chloride on quality of life for patients with fibromyalgia: A feasibility study. J. Integr. Med. 2015, 13, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Rodriguez, A.; Rubio-Arias, J.A.; Ramos-Campo, D.J.; Reche-Garcia, C.; Leyva-Vela, B.; Nadal-Nicolas, Y. Psychological and Sleep Effects of Tryptophan and Magnesium-Enriched Mediterranean Diet in Women with Fibromyalgia. Int. J. Environ. Res. Public Health 2020, 17, 2227. [Google Scholar] [CrossRef] [PubMed]
- Andretta, A.; Dias Batista, E.; Madalozzo Schieferdecker, M.E.; Rasmussen Petterle, R.; Boguszewski, C.L.; Dos Santos Paiva, E. Relation between magnesium and calcium and parameters of pain, quality of life and depression in women with fibromyalgia. Adv. Rheumatol. 2019, 59, 55. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Schweinhardt, P. Dysfunctional neurotransmitter systems in fibromyalgia, their role in central stress circuitry and pharmacological actions on these systems. Pain Res. Treat. 2012, 2012, 741746. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, C.; Cristiani, C.M.; Ilari, S.; Passacatini, L.C.; Malafoglia, V.; Viglietto, G.; Maiuolo, J.; Oppedisano, F.; Palma, E.; Tomino, C.; et al. Fibromyalgia and Irritable Bowel Syndrome Interaction: A Possible Role for Gut Microbiota and Gut-Brain Axis. Biomedicines 2023, 11, 1701. [Google Scholar] [CrossRef] [PubMed]
- Minerbi, A.; Gonzalez, E.; Brereton, N.J.B.; Anjarkouchian, A.; Dewar, K.; Fitzcharles, M.A.; Chevalier, S.; Shir, Y. Altered microbiome composition in individuals with fibromyalgia. Pain 2019, 160, 2589–25602. [Google Scholar] [CrossRef] [PubMed]
- Malatji, B.G.; Mason, S.; Mienie, L.J.; Wevers, R.A.; Meyer, H.; van Reenen, M.; Reinecke, C.J. The GC-MS metabolomics signature in patients with fibromyalgia syndrome directs to dysbiosis as an aspect contributing factor of FMS pathophysiology. Metabolomics 2019, 15, 54. [Google Scholar] [CrossRef] [PubMed]
- Floch, M.H.; Walker, W.A.; Sanders, M.E.; Nieuwdorp, M.; Kim, A.S.; Brenner, D.A.; Qamar, A.A.; Miloh, T.A.; Guarino, A.; Guslandi, M.; et al. Recommendations for Probiotic Use—2015 Update: Proceedings and Consensus Opinion. J. Clin. Gastroenterol. 2015, 49, S69–S73. [Google Scholar] [CrossRef] [PubMed]
- Dinan, T.G.; Cryan, J.F. The Microbiome-Gut-Brain Axis in Health and Disease. Gastroenterol. Clin. N. Am. 2017, 46, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Weiss, G.A.; Hennet, T. Mechanisms and consequences of intestinal dysbiosis. Cell Mol. Life Sci. 2017, 74, 2959–2977. [Google Scholar] [CrossRef] [PubMed]
- Mayer, E.A.; Tillisch, K.; Gupta, A. Gut/brain axis and the microbiota. J. Clin. Investig. 2015, 125, 926–938. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Tomaino, L.; Dernini, S.; Berry, E.M.; Lairon, D.; Ngo de la Cruz, J.; Bach-Faig, A.; Donini, L.M.; Medina, F.-X.; Belahsen, R.; et al. Updating the Mediterranean Diet Pyramid towards Sustainability: Focus on Environmental Concerns. Int. J. Environ. Res. Public Health 2020, 17, 8758. [Google Scholar] [CrossRef] [PubMed]
- D’Onghia, M.; Ciaffi, J.; Lisi, L.; Mancarella, L.; Ricci, S.; Stefanelli, N.; Meliconi, F.; Ursini, F. Fibromyalgia and obesity: A comprehensive systematic review and meta-analysis. Semin. Arthritis Rheum. 2021, 51, 409–424. [Google Scholar] [CrossRef]
- Ceron Lorente, L.; Garcia Rios, M.C.; Navarro Ledesma, S.; Tapia Haro, R.M.; Casas Barragan, A.; Correa-Rodriguez, M.; Aguilar Ferrandiz, M.E. Functional Status and Body Mass Index in Postmenopausal Women with Fibromyalgia: A Case-control Study. Int. J. Environ. Res. Public Health 2019, 16, 4540. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo-Alventosa, R.; Ingles, M.; Cortes-Amador, S.; Gimeno-Mallench, L.; Chirivella-Garrido, J.; Kropotov, J.; Serra-Ano, P. Low-Intensity Physical Exercise Improves Pain Catastrophizing and Other Psychological and Physical Aspects in Women with Fibromyalgia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 3634. [Google Scholar] [CrossRef] [PubMed]
- Mathkhor, A.J.; Ibraheem, N.M. Prevalence and Impact of obesity on fibromyalgia syndrome and its allied symptoms. J. Family Med. Prim. Care 2023, 12, 123–127. [Google Scholar] [CrossRef]
- Markkula, R.A.; Kalso, E.A.; Kaprio, J.A. Predictors of fibromyalgia: A population-based twin cohort study. BMC Musculoskelet. Disord. 2016, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Kadayifci, F.Z.; Bradley, M.J.; Onat, A.M.; Shi, H.N.; Zheng, S. Review of nutritional approaches to fibromyalgia. Nutr. Rev. 2022, 80, 2260–2274. [Google Scholar] [CrossRef] [PubMed]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Neumann, L.; Lerner, E.; Glazer, Y.; Bolotin, A.; Shefer, A.; Buskila, D. A cross-sectional study of the relationship between body mass index and clinical characteristics, tenderness measures, quality of life, and physical functioning in fibromyalgia patients. Clin. Rheumatol. 2008, 27, 1543–1547. [Google Scholar] [CrossRef] [PubMed]
- Senna, M.K.; Ahmad, H.S.; Fathi, W. Depression in obese patients with primary fibromyalgia: The mediating role of poor sleep and eating disorder features. Clin. Rheumatol. 2013, 32, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.E.; Kasper, J.M.; Ara, 13; Anastasio, N.C.; Hommel, J.D. Binge-Type Eating in Rats is Facilitated by Neuromedin U Receptor 2 in the Nucleus Accumbens and Ventral Tegmental Area. Nutrients 2019, 11, 327. [Google Scholar] [CrossRef] [PubMed]
- Metyas, C.; Aung, T.T.; Cheung, J.; Joseph, M.; Ballester, A.M.; Metyas, S. Diet and Lifestyle Modifications for Fibromyalgia. Curr. Rheumatol. Rev. 2024. [Google Scholar] [CrossRef] [PubMed]
- Arranz, L.I.; Canela, M.A.; Rafecas, M. Dietary aspects in fibromyalgia patients: Results of a survey on food awareness, allergies, and nutritional supplementation. Rheumatol. Int. 2012, 32, 2615–2621. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.M.; Jones, J.; Turk, D.C.; Russell, I.J.; Matallana, L. An internet survey of 2,596 people with fibromyalgia. BMC Musculoskelet. Disord. 2007, 8, 27. [Google Scholar] [CrossRef]
- Maddox, E.K.; Massoni, S.C.; Hoffart, C.M.; Takata, Y. Dietary Effects on Pain Symptoms in Patients with Fibromyalgia Syndrome: Systematic Review and Future Directions. Nutrients 2023, 15, 716. [Google Scholar] [CrossRef] [PubMed]
- Lowry, E.; Marley, J.; McVeigh, J.G.; McSorley, E.; Allsopp, P.; Kerr, D. Dietary Interventions in the Management of Fibromyalgia: A Systematic Review and Best-Evidence Synthesis. Nutrients 2020, 12, 2664. [Google Scholar] [CrossRef] [PubMed]
- Kocyigit, B.F.; Okyay, R.A. The relationship between body mass index and pain, disease activity, depression and anxiety in women with fibromyalgia. PeerJ 2018, 6, e4917. [Google Scholar] [CrossRef] [PubMed]
- Senna, M.K.; Sallam, R.A.; Ashour, H.S.; Elarman, M. Effect of weight reduction on the quality of life in obese patients with fibromyalgia syndrome: A randomized controlled trial. Clin. Rheumatol. 2012, 31, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Scoditti, E.; Tumolo, M.R.; Garbarino, S. Mediterranean Diet on Sleep: A Health Alliance. Nutrients 2022, 14, 2998. [Google Scholar] [CrossRef] [PubMed]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public. Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, J.; Fialho, M.; Santos, R.; Peixoto-Placido, C.; Madeira, T.; Sousa-Santos, N.; Virgolino, A.; Santos, O.; Vaz Carneiro, A. Is olive oil good for you? A systematic review and meta-analysis on anti-inflammatory benefits from regular dietary intake. Nutrition 2020, 69, 110559. [Google Scholar] [CrossRef] [PubMed]
- Cardamone, E.; Iacoponi, F.; Di Benedetto, R.; Lorenzoni, G.; Di Nucci, A.; Zobec, F.; Gregori, D.; Silano, M. Adherence to Mediterranean Diet and its main determinants in a sample of Italian adults: Results from the ARIANNA cross-sectional survey. Front. Nutr. 2024, 11, 1346455. [Google Scholar] [CrossRef]
- O’Mahony, L.F.; Srivastava, A.; Mehta, P.; Ciurtin, C. Is fibromyalgia associated with a unique cytokine profile? A systematic review and meta-analysis. Rheumatology 2021, 60, 2602–2614. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Lotti, S.; Napoletano, A.; Corrao, A.; Pagliai, G.; Tristan Asensi, M.; Gianfredi, V.; Nucci, D.; Colombini, B.; Sofi, F. Association between Psychological Disorders, Mediterranean Diet, and Chronotype in a Group of Italian Adults. Int. J. Environ. Res. Public Health 2022, 20, 335. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Cabello, P.; Soriano-Maldonado, A.; Delgado-Fernandez, M.; Alvarez-Gallardo, I.C.; Segura-Jimenez, V.; Estevez-Lopez, F.; Camiletti-Moirón, D.; Aparicio, V.A. Association of Dietary Habits with Psychosocial Outcomes in Women with Fibromyalgia: The al-Andalus Project. J. Acad. Nutr. Diet. 2017, 117, 422–432.e1. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Female | Male | No Answer | |||
|---|---|---|---|---|---|---|
| FM | 96.7 | 2.7 | 0.5 | |||
| Education | Primary | Lower secondary | Upper secondary | Academic degree | PhD or equivalent | |
| 0.5 | 25.4 | 51.9 | 12.9 | 9.2 | ||
| Marital status | Single | Married/cohabitant | Separated/divorced | Widowed | ||
| 15.0 | 61.3 | 20.9 | 2.7 | |||
| Employment | Grey-collar | White-collar | Blue- collar | Freelance | Unemployed/retired | No answer |
| 40.3 | 1.6 | 6.0 | 8.0 | 41.4 | 2.7 |
| Q1 a | Median | Mean ± SD | Q3 b | |
|---|---|---|---|---|
| Patient age (years) | 48.5 | 56 | 54 ± 10 | 60.5 |
| Height (cm) | 158 | 160 | 162 ± 6.8 | 166 |
| Weight (Kg) | 58 | 67 | 69.4 ± 16.2 | 79 |
| BMI | 21.8 | 25.6 | 26.5 ± 6.2 | 30.1 |
| Disease duration (years) | 5 | 9 | 10.7 ± 7.7 | 13 |
| (a) | Pharmaceuticals | Frequency (%) | (b) | Supplements | Frequency (%) |
|---|---|---|---|---|---|
| Anti-inflammatories/ analgesics | 60.8 | Vitamin D | 65 | ||
| Antidepressants | 40.3 | Magnesium | 49.5 | ||
| Antineuralgics/anxiolytics | 33.9 | Prebiotics/probiotics | 25.8 | ||
| Cannabinoids | 20.4 | Melatonin | 21 | ||
| Corticosteroids | 14 | Anti-inflammatories | 21 | ||
| None | 13.4 | Anxiolytics | 21 | ||
| Anti-oxidants | 19.9 | ||||
| Preparations for joints | 18.3 | ||||
| Immunostimulants | 17.2 | ||||
| Multivitamin/Multimineral | 17.2 | ||||
| Turmeric | 13 | ||||
| None | 14 |
| Therapy | Frequency (%) |
|---|---|
| Physiotherapy | 20 |
| Meditation | 20 |
| Relaxation techniques | 14.5 |
| Yoga | 14 |
| Massage | 12.4 |
| Acupuncture | 8.6 |
| None | 42.5 |
| Symptom | Frequency (%) |
|---|---|
| Fatigue | 84.4 |
| Brain fog | 80.1 |
| Sleep disturbance | 78.5 |
| Dizziness | 66.7 |
| Anxiety | 59.1 |
| Photophobia | 51.1 |
| Migraine | 49.5 |
| Constipation | 48.4 |
| Colitis/diarrhea | 45.2 |
| Depression | 37.1 |
| Diplopia | 34.4 |
| Nausea | 27.4 |
| Severity | Depression | Anxiety | Stress |
|---|---|---|---|
| Normal | 24.4 | 14 | 35.9 |
| Mild | 14.3 | 10.1 | 14.4 |
| Moderate | 28.6 | 29.8 | 25.4 |
| Severe | 9.5 | 12.4 | 17.7 |
| Extremely severe | 23.2 | 33.7 | 6.6 |
| FM Severity State | Frequency (%) |
|---|---|
| Remission | 3 |
| Mild | 8.3 |
| Moderate | 24.9 |
| High | 63.9 |
| FIQR Scores | Min | Q1 a | Median | Mean ± SD | Q3 b | Max |
|---|---|---|---|---|---|---|
| Total | 14.7 | 59.3 | 69.3 | 68.0 ± 17.1 | 81.3 | 100 |
| FIQR1 (Physical function) | 3.0 | 49.0 | 64.5 | 59.3 ± 19.2 | 74.0 | 90 |
| FIQR2 (Overall impact) | 0 | 10.0 | 14.0 | 13.1 ± 5.1 | 17.0 | 20 |
| FIQR3 (Symptoms) | 19.0 | 62.0 | 71.0 | 70.4 ± 14.8 | 82.0 | 100 |
| Type of Diet | Frequency (%) |
|---|---|
| Lactose-free | 64.8 |
| Gluten-free | 58.2 |
| Low-calorie Mediterranean | 31.9 |
| Vegetarian | 14.3 |
| Low FODMAP | 11 |
| Ketogenic/ VLCKD (800 kcal) | 9.9 |
| Vegan | 5.5 |
| Other/personalized | 36.3 |
| FIQR/ PREDIMED-14 | Pain Intensity/ PREDIMED-14 | PD-Q/ PREDIMED-14 | |
|---|---|---|---|
| R a | 0.238 | 0.20 | 0.055 |
| Slope b | –2.12 | –0.21 | –0.24 |
| p | 0.003 | 0.008 | 0.475 |
| FIQR/ PREDIMED-14 | Pain intensity/ PREDIMED-14 | ||
|---|---|---|---|
| R a | 0.222 | 0.202 | |
| Without propensity score | Delta b | –10.54 | –1.17 |
| p | 0.0005 | 0.0084 | |
| R a | 0.183 | 0.235 | |
| With propensity score | Delta b | –6.929 | –1.09 |
| p | 0.0216 | 0.0018 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Proietti, E.; Rapallo, F.; Molinari, E.; Mucci, V.; Marinelli, L.; Borgarelli, C.; Burlando, B.; Pisciotta, L.; Demori, I. Online Questionnaire with Fibromyalgia Patients Shows Negative Correlations between Disease Severity and Adherence to Mediterranean Diet. Nutrients 2024, 16, 1078. https://doi.org/10.3390/nu16071078
Proietti E, Rapallo F, Molinari E, Mucci V, Marinelli L, Borgarelli C, Burlando B, Pisciotta L, Demori I. Online Questionnaire with Fibromyalgia Patients Shows Negative Correlations between Disease Severity and Adherence to Mediterranean Diet. Nutrients. 2024; 16(7):1078. https://doi.org/10.3390/nu16071078
Chicago/Turabian StyleProietti, Elisa, Fabio Rapallo, Elena Molinari, Viviana Mucci, Lucio Marinelli, Consuelo Borgarelli, Bruno Burlando, Livia Pisciotta, and Ilaria Demori. 2024. "Online Questionnaire with Fibromyalgia Patients Shows Negative Correlations between Disease Severity and Adherence to Mediterranean Diet" Nutrients 16, no. 7: 1078. https://doi.org/10.3390/nu16071078
APA StyleProietti, E., Rapallo, F., Molinari, E., Mucci, V., Marinelli, L., Borgarelli, C., Burlando, B., Pisciotta, L., & Demori, I. (2024). Online Questionnaire with Fibromyalgia Patients Shows Negative Correlations between Disease Severity and Adherence to Mediterranean Diet. Nutrients, 16(7), 1078. https://doi.org/10.3390/nu16071078