Intake of Table Sugar and Their Corresponding Food Sources in Adults from the 2017–2018 Brazilian National Dietary Survey

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
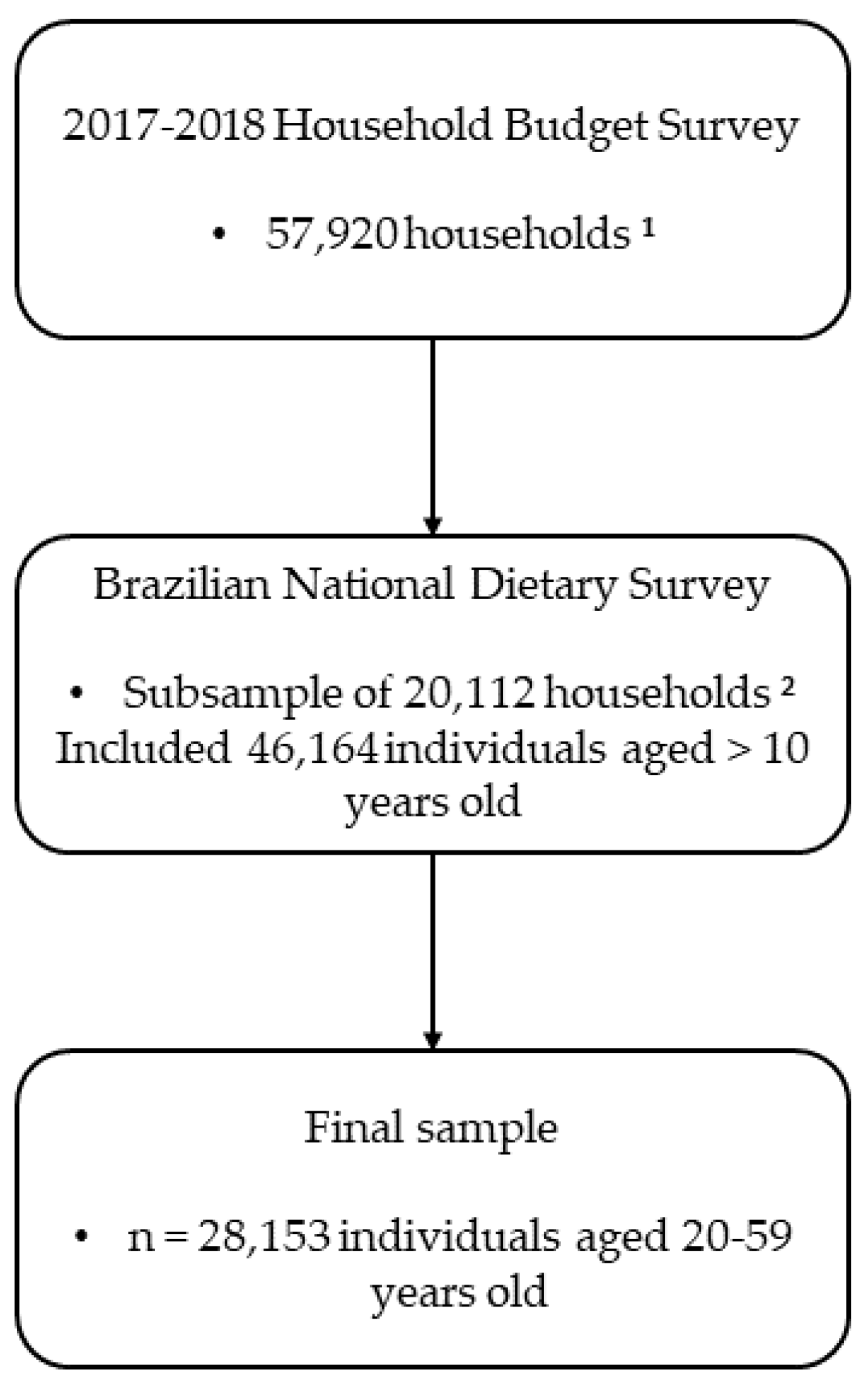
2.1. Study Design and Population
2.2. Sociodemographic and Anthropometric Information
2.3. Dietary Data
2.4. Food Grouping
2.5. Statistical Analyses
3. Results
3.1. Study Population Characteristics
3.2. Table Sugar Intake
3.3. Total Energy Intake (E%) Resulting from Daily Table Sugar Intake
3.4. Main Food Sources of Table Sugar
4. Discussion
5. Conclusions and Final Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moynihan, P.J.; Kelly, S.A.M. Effect on Caries of Restricting Sugars Intake: Systematic Review to Inform WHO Guidelines. J. Dent. Res. 2014, 93, 8. [Google Scholar] [CrossRef]
- Te Morenga, L.; Mallard, S.; Mann, J. Dietary Sugars and Body Weight: Systematic Review and Meta-Analyses of Randomised Controlled Trials and Cohort Studies. BMJ 2013, 346, e7492. [Google Scholar] [CrossRef]
- Huang, C.; Liang, Z.; Ma, J.; Hu, D.; Yao, F.; Qin, P. Total Sugar, Added Sugar, Fructose, and Sucrose Intake and All-Cause, Cardiovascular, and Cancer Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Nutrition 2023, 111, 112032. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Li, S.; Khan, J.; Dai, Z.; Li, C.; Hu, X.; Shen, Q.; Xue, Y. Sugar- and Artificially Sweetened Beverages Consumption Linked to Type 2 Diabetes, Cardiovascular Diseases, and All-Cause Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Nutrients 2021, 13, 2636. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 25 January 2024).
- Kazibwe, J.; Tran, P.B.; Annerstedt, K.S. The Household Financial Burden of Non-Communicable Diseases in Low- and Middle-Income Countries: A Systematic Review. Health Res. Policy Syst. 2021, 19, 96. [Google Scholar] [CrossRef] [PubMed]
- Budreviciute, A.; Damiati, S.; Sabir, D.K.; Onder, K.; Schuller-Goetzburg, P.; Plakys, G.; Katileviciute, A.; Khoja, S.; Kodzius, R. Management and Prevention Strategies for Non-Communicable Diseases (NCDs) and Their Risk Factors. Front. Public Health 2020, 8, 574111. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Erickson, J.; Slavin, J. Total, Added, and Free Sugars: Are Restrictive Guidelines Science-Based or Achievable? Nutrients 2015, 7, 2866–2878. [Google Scholar] [CrossRef]
- Hess, J.; Latulippe, M.E.; Ayoob, K.; Slavin, J. The Confusing World of Dietary Sugars: Definitions, Intakes, Food Sources and International Dietary Recommendations. Food Funct. 2012, 3, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Added Sugars on the Nutrition Facts Label|FDA. Available online: https://www.fda.gov/food/nutrition-facts-label/added-sugars-nutrition-facts-label (accessed on 25 January 2024).
- EFSA Panel on Dietetic Products Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Carbohydrates and Dietary Fibre. EFSA J. 2010, 8, 1462. [Google Scholar]
- Scientific Advisory Committee on Nutrition (SACN). Carbohydrates and Health; Public Health: London, UK, 2015.
- Amoutzopoulos, B.; Page, P.; Steer, T.; Roberts, C.; Collins, D. Free and Added Sugar Consumption and Adherence to Guidelines: The UK National Diet and Nutrition Survey (2014/15–2015/16). Nutrients 2020, 12, 393. [Google Scholar] [CrossRef]
- Brasil, Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Análise em Saúde e Vigilância de Doenças Não Transmissíveis. Plano de Ações Estratégicas Para o Enfrentamento Das Doenças Crônicas e Agravos Não Transmissíveis No Brasil 2021–2030; Ministério da Saúde: Brasília, Brazil, 2021.
- Levy, R.B.; Claro, R.M.; Bandoni, D.H.; Mondini, L.; Monteiro, C.A. Availability of Added Sugars in Brazil: Distribution, Food sources and Time Trends. Rev. Bras. Epidemiol. 2012, 15, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Marinho, A.R.; Severo, M.; Correia, D.; Lobato, L.; Vilela, S.; Oliveira, A.; Ramos, E.; Torres, D.; Lopes, C. Total, Added and Free Sugar Intakes, Dietary Sources and Determinants of Consumption in Portugal: The National Food, Nutrition and Physical Activity Survey (IAN-AF 2015-2016). Public Health Nutr. 2020, 23, 869–881. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares 2017–2018: Primeiros Resultados; IBGE: Rio de Janeiro, Brazil, 2019.
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares 2017–2018: Análise Do Consumo Alimentar Pessoal No Brasil; IBGE: Rio de Janeiro, Brazil, 2020.
- Félix, P.V.; De Castro, M.A.; Nogueira-de-Almeida, C.A.; Fisberg, M. Prevalence of Excess Sodium Intake and Their Corresponding Food Sources in Adults from the 2017-2018 Brazilian National Dietary Survey. Nutrients 2022, 14, 4018. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry: Report of a WHO Expert Committee; World Health Organization: Geneva, Switzerland, 1995. [Google Scholar]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares 2017–2018: Análise Da Segurança Alimentar No Brasil; IBGE: Rio de Janeiro, Brazil, 2020.
- Segall-Corrêa, A.M.; Marin-León, L.; Melgar-Quiñonez, H.; Pérez-Escamilla, R. Refinement of the Brazilian Household Food Insecurity Measurement Scale: Recommendation for a 14-Item EBIA. Rev. Nutr. 2014, 27, 241–251. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method Reduces Bias in the Collection of Energy Intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef]
- de Castro, M.A.; Baltar, V.T.; Selem, S.S.d.C.; Marchioni, D.M.L.; Fisberg, R.M. Empirically Derived Dietary Patterns: Interpretability and Construct Validity According to Different Factor Rotation Methods. Cad. Saude Publica 2015, 31, 298–310. [Google Scholar] [CrossRef] [PubMed]
- Harttig, U.; Haubrock, J.; Knüppel, S.; Boeing, H. The MSM Program: Web-Based Statistics Package for Estimating Usual Dietary Intake Using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65 (Suppl. S1), S87–S91. [Google Scholar] [CrossRef]
- Lachat, C.; Hawwash, D.; Ocké, M.C.; Berg, C.; Forsum, E.; Hörnell, A.; Larsson, C.; Sonestedt, E.; Wirfält, E.; Åkesson, A.; et al. Strengthening the Reporting of Observational Studies in Epidemiology-Nutritional Epidemiology (STROBE-Nut): An Extension of the STROBE Statement. PLoS Med. 2016, 13, e1002036. [Google Scholar] [CrossRef] [PubMed]
- Block, G.; Hartman, A.M.; Dresser, C.M.; Carroll, M.D.; Gannon, J.; Gardner, L. A Data-Based Approach to Diet Questionnaire Design and Testing. Am. J. Epidemiol. 1986, 124, 453–469. [Google Scholar] [CrossRef]
- Brasil, Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica. Guia Alimentar Para a População Brasileira; Ministério da Saúde: Brasília, Brazil, 2014.
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares 2008–2009: Análise Do Consumo Alimentar Pessoal No Brasil; IBGE: Rio de Janeiro, Brazil, 2011.
- Monteiro, L.S.; Hassan, B.K.; Rodrigues, P.R.M.; Yokoo, E.M.; Sichieri, R.; Pereira, R.A. Use of Table Sugar and Artificial Sweeteners in Brazil: National Dietary Survey 2008–2009. Nutrients 2018, 10, 295. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional de Saúde: 2013: Percepção Do Estado de Saúde, Estilos de Vida e Doenças Crônicas: Brasil, Grandes Regiões e Unidades Da Federação; IBGE: Rio de Janeiro, Brazil, 2014.
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional de Saúde: 2019: Percepção Do Estado de Saúde, Estilos de Vida, Doenças Crônicas e Saúde Bucal: Brasil e Grandes Regiões; IBGE: Rio de Janeiro, Brazil, 2020.
- Sociedade Brasileira de Diabetes. Diretrizes Da Sociedade Brasileira de Diabetes 2019–2020; Sociedade Brasileira de Diabetes: Brasília, Brazil, 2019. [Google Scholar]
- Stanhope, K. Sugar consumption, metabolic disease and obesity: The state of the controversy. Crit. Rev. Clin. Lab. Sci. 2016, 53, 52–67. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, K.M.; Kemps, E.; White, M.J.; Bartlett, S.E. The Impact of Free Sugar on Human Health—A Narrative Review. Nutrients 2023, 15, 889. [Google Scholar] [CrossRef] [PubMed]
- Souza, A.d.M.; Pereira, R.A.; Yokoo, E.M.; Levy, R.B.; Sichieri, R. Most Consumed Foods in Brazil: National Dietary Survey-2009. Rev. Saude Publica 2013, 47, 190s–199s. [Google Scholar] [CrossRef]
- Sichieri, R.; Bezerra, I.N.; Araújo, M.C.; De Moura Souza, A.; Yokoo, E.M.; Pereira, R.A. Major Food Sources Contributing to Energy Intake—A Nationwide Survey of Brazilians Aged 10 Years and Older. Br. J. Nutr. 2015, 113, 1638–1642. [Google Scholar] [CrossRef]
- Souza, R.A.G.; Yokoo, E.M.; Sichieri, R.; Pereira, R.A. Energy and Macronutrient Intakes in Brazil: Results of the First Nationwide Individual Dietary Survey. Public Health Nutr. 2015, 18, 3086–3095. [Google Scholar] [CrossRef]
- Palmeira, P.A.; Bem-Lignani, J.; Salles-Costa, R. Access to governmental programs/benefits and food insecurity in urban and rural areas of Northeast Brazil. Cien. Saude Colet. 2022, 27, 2583–2595. [Google Scholar] [CrossRef]
- de Castro, M.A.; Fontanelli, M.d.M.; Nogueira-de-Almeida, C.A.; Fisberg, M. Food Insecurity Reduces the Chance of Following a Nutrient-Dense Dietary Pattern by Brazilian Adults: Insights from a Nationwide Cross-Sectional Survey. Nutrients 2022, 14, 2126. [Google Scholar] [CrossRef]
- Trivellato, P.T.; Morais, D.C.; Lopes, S.O.; Miguel, E.S.; Franceschini, S.C.C.; Priore, S.E. Food and nutritional insecurity in families in the Brazilian rural environment: A systematic review. Cien. Saude Colet. 2019, 24, 865–874. [Google Scholar] [CrossRef]
- Costa, N.S.; Santos, M.O.; Carvalho, C.P.O.; Assunção, M.L.; Ferreira, H.S. Prevalence and Factors Associated with Food Insecurity in the Context of the Economic Crisis in Brazil. Curr. Dev. Nutr. 2017, 1, e000869. [Google Scholar] [CrossRef]
- Palmeira, P.A.; Bem-Lignani, J.; Maresi, V.A.; Mattos, R.A.; Interlenghi, G.S.; Salles-Costa, R. Temporal Changes in the Association between Food Insecurity and Socioeconomic Status in Two Population-Based Surveys in Rio de Janeiro, Brazil. Soc. Indic. Res. 2019, 144, 1349–1365. [Google Scholar] [CrossRef]
- dos Passos, K.E.; Bernardi, J.R.; Mendes, K.G. Analysis of the Nutritional Composition of the Brazilian Staple Foods Basket. Cien. Saude Colet. 2014, 19, 1623–1630. [Google Scholar] [PubMed]
- Antunes, A.B.S.; Cunha, D.B.; Baltar, V.T.; Steluti, J.; Pereira, R.A.; Yokoo, E.M.; Sichieri, R.; Marchioni, D.M. Dietary Patterns of Brazilian Adults in 2008–2009 and 2017–2018. Rev. Saude Publica 2021, 55, 8s. [Google Scholar] [CrossRef]
- Pereira, J.L.; de Castro, M.A.; Hopkins, S.; Gugger, C.; Fisberg, R.M.; Fisberg, M. Proposal for a Breakfast Quality Index for Brazilian Population: Rationale and Application in the Brazilian National Dietary Survey. Appetite 2017, 111, 12–22. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Population | Table Sugar Intake (g/Day) | |||||
|---|---|---|---|---|---|---|
| Characteristics | n | % (95% CI) 1 | Median | IQR | p-Value 2 | E% 3 |
| Overall population | 28,153 | 100 | 14.3 | (3.7, 31.8) | - | 3.2 |
| Geographic region | ||||||
| North | 4132 | 8.2 (7.7, 8.7) | 8.6 ab | (2.3, 23.7) | 1.9 | |
| Northeast | 9717 | 26.4 (25.6, 27.3) | 18.9 ab | (8.2, 36.4) | 4.2 | |
| Southeast | 7029 | 42.8 (41.7, 44.0) | 13.8 b | (2.7, 13.8) | 3.1 | |
| South | 3699 | 14.6 (13.9, 15.4) | 15.1 ab | (3.9, 32.5) | 3.4 | |
| Midwest | 3576 | 7.9 (7.5, 8.4) | 13.6 a | (2.9, 28.4) | <0.001 | 3.0 |
| Household area | ||||||
| Urban | 21,863 | 86.3 (85.7, 86.9) | 13.8 | (3.3, 31.7) | 3.1 | |
| Rural | 6290 | 13.7 (13.1, 14.3) | 16.5 | (4.1, 32.8) | <0.001 | 3.7 |
| Age group, years | ||||||
| 20–29 | 6665 | 25.1 (24.3, 26.0) | 14.2 c | (3.4, 32.0) | 3.2 | |
| 30–39 | 7598 | 26.9 (26.0, 27.9) | 16.1 abc | (4.0, 32.9) | 3.6 | |
| 40–49 | 7274 | 25.1 (24.2, 26.0) | 14.0 b | (3.9, 31.5) | 3.1 | |
| 50–59 | 6616 | 22.8 (22.0, 23.7) | 13.8 a | (2.9, 31.5) | <0.001 | 3.1 |
| Sex | ||||||
| Male | 13,338 | 49.8 (49.2, 50.4) | 16.1 | (3.9, 32.9) | 3.6 | |
| Female | 14,815 | 50.2 (49.6, 50.8) | 13.8 | (3.3, 30.6) | <0.001 | 3.1 |
| Self-reported ethnicity 4 | ||||||
| Mixed-race | 14,532 | 45.1 (44.0, 46.2) | 15.7 ab | (3.9, 32.0) | 3.5 | |
| White | 10,351 | 42.6 (41.4, 43.8) | 13.8 a | (3.3, 31.6) | 3.1 | |
| Black | 2963 | 11.2 (10.5, 11.9) | 14.3 | (3.6, 32.4) | 3.2 | |
| Asian | 145 | 0.6 (0.4, 0.9) | 10.7 b | (2.1, 23.7) | 2.4 | |
| Native | 141 | 0.4 (0.3, 0.1) | 13.7 | (2.9, 28.4) | 0.001 | 3.1 |
| Per capita family income 5 | ||||||
| ≤1 minimum wage | 13,218 | 40.4 (39.1, 41.7) | 15.9 | (4.1, 32.2) | 3.5 | |
| >1 minimum wage | 14,935 | 59.6 (58.3, 60.8) | 13.8 | (2.9, 31.6) | <0.001 | 3.1 |
| Education level | ||||||
| ≤9 years of schooling (below elementary school) | 12,702 | 39.8 (38.7, 40.9) | 15.9 | (4.1, 32.3) | 3.5 | |
| >9 years of schooling (above high school) | 15,451 | 60.2 (59.1, 61.3) | 13.8 | (2.9, 31.7) | <0.001 | 3.1 |
| Body Mass Index | ||||||
| Without excessive body weight | 12,676 | 44.4 (43.4, 45.4) | 15.4 | (3.9, 32.0) | 3.5 | |
| With excessive body weight | 15,477 | 55.6 (54.6, 56.5) | 13.9 | (3.5, 31.7) | 0.013 | 3.1 |
| Followed a specific diet | ||||||
| Yes | 3778 | 13.1 (12.4, 13.8) | 8.2 | (1.8, 23.7) | 1.8 | |
| No | 24,375 | 86.9 (86.2, 87.6) | 16.1 | (4.0, 32.8) | <0.001 | 3.6 |
| Frequent use of sugar/sweetener | ||||||
| Sugar | 23,257 | 79.7 (78.6, 80.7) | 18.8 a | (8.2, 34.2) | 4.2 | |
| Sweetener | 1899 | 7.8 (7.2, 8.5) | 2.0 a | (1.2, 3.9) | 0.5 | |
| Sugar and sweetener | 1362 | 5.6 (5.1, 6.2) | 11.5 a | (2.5, 27.3) | 2.6 | |
| No | 1635 | 6.9 (6.1, 7.8) | 2.2 a | (1.3, 5.0) | <0.001 | 0.5 |
| Food security status | ||||||
| Food security | 15,878 | 59.5 (58.1, 60.9) | 13.9 | (3.3, 32.0) | 3.1 | |
| Food insecurity | 12,275 | 40.5 (38.5, 42.5) | 15.4 | (3.9, 31.7) | 0.011 | 3.4 |
| Rank | Food Groups | % Total Table Sugar Intake | % of Consumers | Daily Food Group Intake (g/Day) | Food Group Table Sugar Density (g/100 g) |
|---|---|---|---|---|---|
| 1 | Coffee | 55.8 | 87.9 | 215.3 | 14.1 |
| 2 | Juice | 33.9 | 43.7 | 383.4 | 20.8 |
| 3 | Milk-based preparations and smoothies | 3.1 | 6.2 | 306.1 | 13.2 |
| 4 | Powdered and processed juice | 2.7 | 6.4 | 367.3 | 12.8 |
| 5 | Whole milk | 1.9 | 7.5 | 241.4 | 6.2 |
| 6 | Tea | 1.6 | 9.5 | 822.5 | 4.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ued, F.d.V.; Félix, P.V.; Nogueira-de-Almeida, C.A.; Fisberg, M. Intake of Table Sugar and Their Corresponding Food Sources in Adults from the 2017–2018 Brazilian National Dietary Survey. Nutrients 2024, 16, 1085. https://doi.org/10.3390/nu16071085
Ued FdV, Félix PV, Nogueira-de-Almeida CA, Fisberg M. Intake of Table Sugar and Their Corresponding Food Sources in Adults from the 2017–2018 Brazilian National Dietary Survey. Nutrients. 2024; 16(7):1085. https://doi.org/10.3390/nu16071085
Chicago/Turabian StyleUed, Fábio da Veiga, Paula Victória Félix, Carlos Alberto Nogueira-de-Almeida, and Mauro Fisberg. 2024. "Intake of Table Sugar and Their Corresponding Food Sources in Adults from the 2017–2018 Brazilian National Dietary Survey" Nutrients 16, no. 7: 1085. https://doi.org/10.3390/nu16071085
APA StyleUed, F. d. V., Félix, P. V., Nogueira-de-Almeida, C. A., & Fisberg, M. (2024). Intake of Table Sugar and Their Corresponding Food Sources in Adults from the 2017–2018 Brazilian National Dietary Survey. Nutrients, 16(7), 1085. https://doi.org/10.3390/nu16071085