Abstract
Resources are needed to aid healthcare providers and families in making end-of-life nutrition care decisions for residents living in long-term care settings. This scoping review aimed to explore what is reported in the literature about resources to support decision-making at the end of life in long-term care. Four databases were searched for research published from 2003 to June 2023. Articles included peer-reviewed human studies published in the English language that reported resources to support decision-making about end-of-life nutrition in long-term care settings. In total, 15 articles were included. Thematic analysis of the articles generated five themes: conversations about care, evidence-based decision-making, a need for multidisciplinary perspectives, honouring residents’ goals of care, and cultural considerations for adapting resources. Multidisciplinary care teams supporting residents and their families during the end of life can benefit from resources to support discussion and facilitate decision-making.
1. Introduction
End of life (EOL), defined as the terminal phase of life, often represents a stressful and challenging time for long-term care (LTC) residents and their families [1,2,3]. With an estimated 25–30% of LTC residents dying annually, quality EOL care is essential [4,5]. The goals of nutrition care in LTC are restoration/rehabilitation or maintenance and preservation of function, but at EOL, the focus is solely on quality of life and quality of care, emphasizing the symbolic and pleasurable qualities of eating and drinking [1,2]. This can be an abrupt shift in the goals of care that can be challenging for both families and healthcare providers (HCPs) to embrace [6].
The medical management of EOL is complex. In terms of nutrition care, there is no consensus diagnosis or prognostication that enables the confident assertion that it is the right time to change the goals of nutrition care to terminal care, focusing solely on comfort measures [1,7]. In fact, clinical scales often include eating and drinking as sentinel acts that signal EOL (e.g., the Palliative Performance Scale [8]), and disinterest in eating and drinking can be confounded as a sign of depression or apathy. Instead, HCPs monitor clinical signs and work with residents and families to make complex decisions about nutrition at EOL [9]. With a high prevalence of dementia in LTC and a high proportion of LTC residents rated as cognitively impaired [10], capacity can be limited, and decision-making about nutrition care falls to substitute decision-makers (often family members), which can be very stressful [3,6,7,11,12,13]. Both family members and HCPs experience moral strain about EOL nutrition, questioning whether to pursue aggressive nutrition care or discontinue it [14,15,16,17].
Within LTC, eating challenges are very common [18]. While much attention is focused on strategies to mitigate these challenges and increase intake, attention is needed on supporting declining intake as a function of EOL. Eating and drinking often progressively decrease as residents approach EOL, but the trajectory is varied and often difficult to anticipate; some may maintain pleasure from intake and others may experience discomfort, fatigue, or pain from intake [1,6]. Often, artificial nutrition and hydration (ANH) interventions are sought (e.g., medical enteral/parenteral feeding; clinical hydration via intravenous, nasogastric, hypodermoclysis, rectal) despite little evidence to support use [1,7,17,19,20,21]. Both mechanical and physiological harms are known to result from aggressive ANH at EOL (e.g., discomfort, restriction in mobility, pulmonary edema, nausea, and vomiting), yet HCPs and families often request such interventions [1,13,21,22,23]. Enteral tube feeding persists among residents with dementia at EOL despite strong evidence against its use [24,25,26]. Fear persists that withdrawing nutrition therapy is painful despite known physiological processes that support the amelioration of pain when nutrition is discontinued at EOL (e.g., azotemia, hyponatremia) [1,23,27]. Criteria to discontinue ANH are lacking; families find withdrawing ANH particularly difficult [16,28,29], and performance status scales (e.g., ECOG Performance Status Scale [30], Karnofsky Performance Status Scale [31]) are not helpful for determining when to shift nutrition goals of care. In terms of the clinical management of EOL, decisions about artificial nutrition create more ethical dilemmas than other treatments, including artificial hydration and antibiotic therapy [17]. Yet, discussion about nutrition and hydration decisions is often not germane to care, and evidence suggests that HCPs do not consistently involve residents and families in these important healthcare decisions [9].
Once strategies to address eating and drinking challenges have been exhausted, supports for transitioning into EOL care are needed [7]. Often, this is framed as compassionate terminal care or ‘comfort feeding only’. In this approach, quality of life is emphasized, and nutritional adequacy and functional properties of eating are discarded [32]. In this approach, there is flexibility to respond to the resident’s abilities and desires without repeated clinical assessments to determine physiological safety (e.g., dysphagia) and changes in their nutritional care plan. This can occur before active dying begins (i.e., days or hours to live) and can support HCPs and families in understanding that the EOL stage of care has begun [32].
Previous literature suggests that families lack information about how to incorporate nutrition and hydration into care plans to optimize quality of life at the EOL [33,34]. Conversely, research has shown that families who had a single, in-depth conversation with HCPs about EOL care options for LTC home residents living with advanced dementia had significantly higher satisfaction with care and documented significantly more decisions in their family resident’s advance care plan [35]. Because of the medical, emotional, and ethical complexity of EOL nutrition care, there is a need for resources to support HCPs and families in having discussions and making decisions about EOL nutrition care. Defined as evidence-based resources to support participation in healthcare choices [36,37], decision aids provide information about a health condition and the benefits and risks of treatment options to supplement patient/family-provider conversations about care and support values-based decision-making about care [38]. The purpose of this study was to conduct a scoping review of resources to support EOL decision-making for nutrition and hydration in the LTC context. The research question guiding the study was: What is reported in the literature about resources to support decision-making about EOL nutrition care in LTC settings?
2. Methods
We followed Levac et al.’s [39] adaptations of the Arksey and O’Malley [40] Click or tap here to enter text.six-stage framework for conducting a scoping study: identifying the research question, identifying relevant studies, study selection, charting the data, collating, summarizing, and reporting results, and consultation. With recommendations for enhancing each stage of the framework, Levac et al. [39] sought to better position researchers to achieve sufficient detail and description of analysis processes to facilitate greater consistency in scoping review processes and reporting. Recommended enhancements that were followed for this scoping review include linking the purpose and research question, balancing feasibility with the breadth of the scoping process, selecting studies and extracting data using an iterative team approach, incorporating qualitative thematic analysis, identifying implications for policy, practice, or research, and undergoing consultation as part of the scoping study methodology [39].
2.1. Search Strategy
Search terms were developed through consultation with a university librarian and the Saskatchewan Long-Term Care Network, a group of patient-family partners, clinicians, and academics working together on initiatives to improve LTC in Saskatchewan, Canada. Feedback was obtained to ensure search terms encompassed all concepts relevant to the research question. Search terms are listed in Table 1.

Table 1.
Search terms.
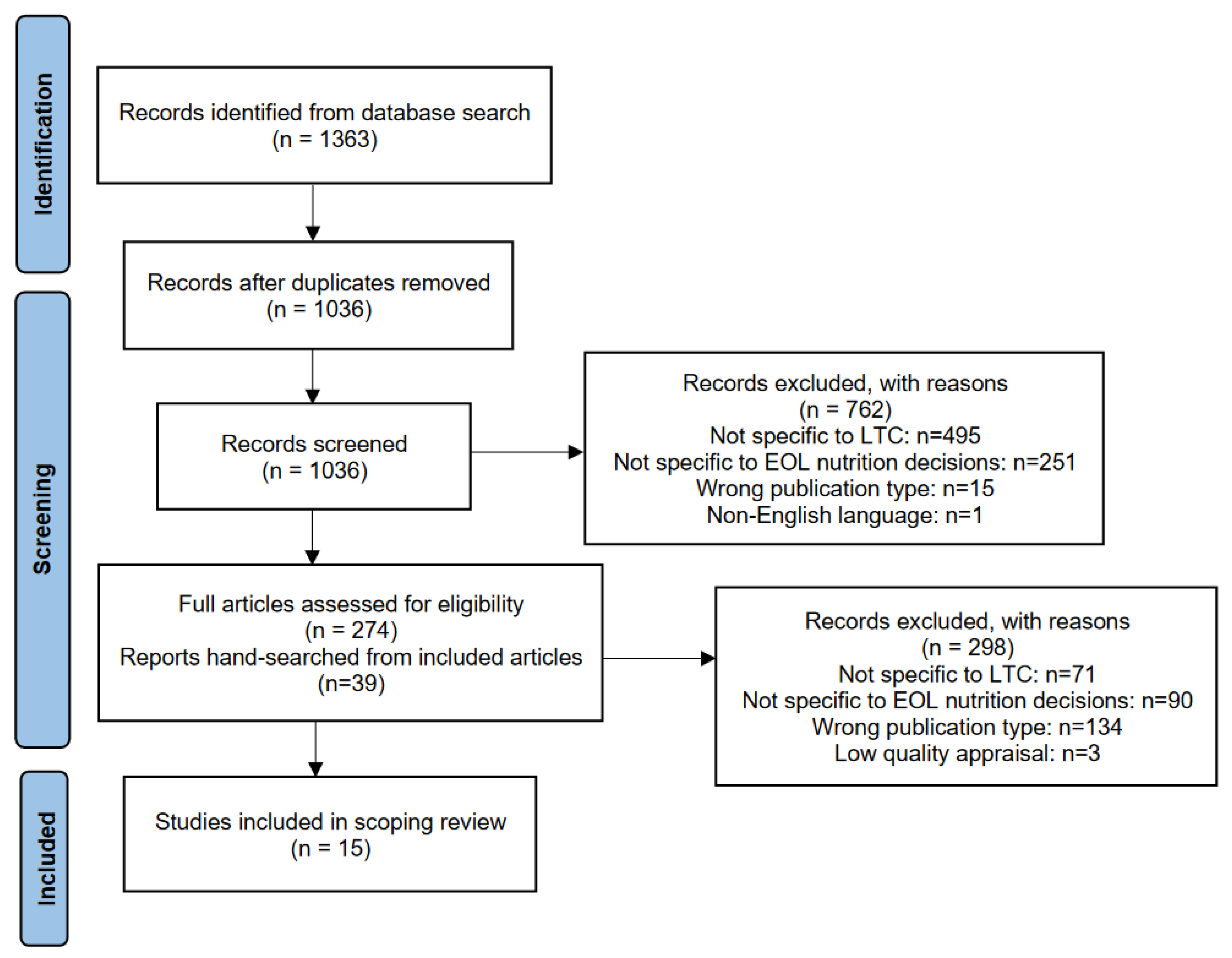
We searched MEDLINE, CINAHL, Web of Science, and Embase. Preliminary searches were conducted to evaluate the research question, search terms, and scope of results. A search was conducted on 13 June 2023. A total of 1363 papers were retrieved and uploaded to Rayyan software [41] for de-duplication, after which 1038 remained. The use of the “blind option” in the Rayyan software [41] allowed independent review and selection of all records by the researchers. Two researchers (HA and NA) independently screened titles and abstracts against inclusion and exclusion criteria. Conflicts were resolved by a third reviewer (AC). The research articles included were peer-reviewed human studies published in the English language from 2003 to June 2023 that reported tangible resources to support decision-making about EOL nutrition in LTC. Articles were excluded if they were non-human studies, published in a non-English language, a review article, or published prior to 2003. After initial screening, 274 papers remained. Of the 274 articles, 71 were excluded due to not being specific to the LTC setting, 90 did not have specific content pertaining to nutrition, and 134 were not research papers (e.g., editorial, narrative description). Under the supervision of AC, researchers HA and NA conducted independent full-text screenings of the articles against the inclusion and exclusion criteria. The citation lists of the remaining articles were then hand-searched by NA and cross checked by HA to identify potential references that met the inclusion criteria. An additional 39 papers were selected and screened by HA and NA, of which five were included. This rendered a total of 18 papers that advanced for quality appraisal.
2.2. Quality Appraisal
Using the Critical Appraisal Skills Programme (CASP) checklists [42], the quality of the included articles was appraised independently by reviewers HA and NA and confirmed by AC. The CASP checklists provided an opportunity for discussion among the researchers about the quality and content of the studies. Though CASP checklists do not provide a cut-off score for low quality, three articles were excluded based on consensus agreement that they were of low quality and misfit with the research question. The search and article screening are presented in a chart of search results (Figure 1).

Figure 1.
Chart of the search process.
A total of 15 papers were included for analysis in the scoping review.
2.3. Data Analysis
The following data were summarized from the included studies: publication year, study location, design, key findings, and implications. Further, the following data were extracted to characterize the decision aids related to each study: type of decision aid, target audience, goals of the study, and existing gaps. These findings are summarized in table form (Table 2).
Table 2.
Overview of Findings.
Following the extraction of the above data, thematic analysis was conducted by researchers HA and NA under the guidance of AC to identify key themes captured in the included studies.
3. Results
In total, 15 papers related to 12 different resources for supporting nutrition care decisions at EOL were included in this scoping review. All papers represented research undertaken in high-income countries. The resources span a variety of types and purposes, and the corresponding research approaches and findings vary accordingly. See Table 2 for an overview of included studies. Five key themes were identified from the studies: conversations about care, evidence-based decision-making, a need for multidisciplinary perspectives, honouring residents’ goals of care, and cultural considerations for adapting resources.
3.1. Conversations about Care
Each of the included studies emphasized the importance of conversations between residents, families, and HCPs for aligning goals of care, aiding in the shared decision-making process, and optimizing the quality of decisions made. Formal documents, such as advance directives or advance care plans, were recommended for promoting resident autonomy and involvement in treatment decisions [43,44,45,46,47,48,49,50,51,52,53,54,55,56,57]. Care conferences were identified as key opportunities for more formal conversations, and regular informal conversations were equally important opportunities for HCPs to communicate changes in a resident’s health and to clarify goals of care with residents and families [43]. For each resource/intervention, the authors identified the importance of early distribution and usage for promoting more frequent and in-depth conversations about care, particularly regarding the course of dementia and available treatment options to avoid unwanted, futile, or burdensome interventions [43,44,50]. Use of resources to support decision-making was consistently associated with more frequent discussions amongst families and HCPs [43,50], with greater impact in facilities with fewer nurse practitioners or physician assistants present [49], and greater family participation in decision-making [45,52]. Additionally, an international team of researchers found that such resources can be used to overcome staff-family communication barriers [57].
3.2. Evidence-Based Decision-Making
Some authors posited that because of a lack of information on the risks and marginal benefits of certain ANH interventions in EOL dementia care, such interventions may placate families or caregivers by providing the sense that efforts were exhausted to preserve nutritional intake [50,53]. In fact, tube feedings were perceived by staff and families alike as providing nourishment and care, despite the lack of evidence for a clear and consistent benefit to residents [50,53,55]. With the use of resources to support decision-making, carers had increased knowledge about treatments [46,50,51,53], significantly better decisional capacity [45], reduced decisional conflict [49,50,51,53] and ultimately were more likely to avoid unnecessary or burdensome interventions, including tube feeding [50,53]. Such resources prompted and provided frameworks for conversations and presented unequivocal information about treatments, which some equated to myth-busting, making it easier to arrive at a decision.
3.3. A Need for Multidisciplinary Perspectives
Care teams were best positioned to support residents and families when bolstered with multiple HCP perspectives. Specifically, nurse practitioners were named as a key human health resource whose proximity to the care team helped to inform and support both families and other HCPs, namely physicians [47,56]. Most authors reiterated that the importance of a cohesive and collaborative care team cannot be overemphasized. On the other hand, none of the studies mentioned the role of registered dietitians except for one that noted the lack of dietitian involvement as a limitation to the study [46]. Moreover, only two decision aids were developed in partnership with residents and families using a co-design approach [43,46]. These two resources focus on family satisfaction with EOL care. Many studies did, however, test the content, effectiveness, and acceptability of the respective resources among family [43,49,50,51,52,53,56] and resident populations, including residents living with dementia [45,50].
3.4. Honouring Residents’ Goals of Care
Of central importance within each resource was to respect and honour each resident’s goals of care. Most authors noted the importance of advance care plans for documenting residents’ preferences. In instances where residents’ wishes were not made clear (e.g., using an advance care plan) or a resident lacked capacity to share their preferences, authors advised that caregivers use their best judgment based on personal knowledge of the resident [44,52,55]. Resources to support decisions are typically presented and clarified for each aspect of care for families and HCPs to consider. Since enhancing a resident’s quality of life in accordance with their goals of care was of primary importance, many such resources provided synopses of treatment options, thus providing the information necessary to weigh the associated benefits, risks, and burdens of available options [45,46,50]. Specifically, providing families and HCPs with knowledge of the course of the illness trajectory towards EOL was important for understanding prognoses and minimizing further stress and anxiety related to observed changes in residents during EOL [55].
3.5. Cultural Considerations for Adapting Resources
One resource, a comfort care booklet [58], originally developed in Canada in English and French, was adapted for implementation in Italy, Japan, and the Netherlands [59]. Because of cultural differences in EOL care provision, an international team of researchers worked to adapt the booklet, revising the content to meet local legal and ethical frameworks. The translated versions of the booklet were evaluated for acceptability and usefulness among HCPs [44,48,57] and families [56]. While the need for and perceived usefulness of the booklet was nearly universal among HCPs and families [44,56], evaluations of its format varied for staff and families, denoting the importance of cultural context. One study found that resources to support EOL care were endorsed, particularly among nurses, regardless of format [59]. Families were more sensitive to the format of the booklet, with the authors suggesting greater adaptation to text and photos to better suit families’ preferences for obtaining information [56].
4. Discussion
Choices about eating and drinking are some of the most common yet challenging decisions that families and HCPs face in LTC [16,60]. This scoping review aimed to understand what resources exist to support decision-making about EOL nutrition care within the LTC setting. Decision aids provide structured, evidence-based information about the risks and benefits of available treatments, improving the quality and efficiency of decision-making for HCPs and families [46,50,52,61]. Other resources to support decision-making include descriptions of illness trajectories, information about treatment and care options, and advance care plans. Yet few tangible resources are available to aid decision-making about EOL nutrition in LTC. For those that have been reported in the literature, implementing such resources increased knowledge about EOL nutrition for HCPs and families [50,52,53], reduced decisional conflict [49,50,51,53], increased staff-family communication [43,49,50], and better positioned carers to consider available treatment options while prioritizing resident goals of care and quality of life.
There is a clear need for increased conversation and better support for families in EOL nutrition care decision-making [3,6,13,62]. Engaging families and HCPs in discussions about care facilitates shared and informed decision-making that leads to better health outcomes and quality of care [61]. While staff shortages and time constraints are commonly identified as barriers to staff-family discussions about care, clinical judgment does not supersede facilitating shared decision-making among care partners. For instance, Roach et al. [62] found that staff conflated caregiver guilt with desire for ANH, including tube feeding. The authors warned that in the absence of staff-family conversations, staff biases and assumptions may lead to more aggressive and burdensome treatments than are aligned with families’ actual goals or preferences. Similarly, other studies show that staff-family conflicts can arise when HCPs disregard patient/family wishes or pursue unwanted, invasive treatments, contributing to unease and distress or increasing caregiver burden for families [3,63]. Resources to support decision-making can be used to mitigate time constraints that limit opportunities for staff-family discussions by making the necessary information available to reach an informed consensus that optimizes the quality of decisions made and care provided.
Since the roles of most HCPs are not well defined in the EOL nutrition context, it remains unclear who provides support and assistance or where families can seek information about EOL nutrition care. Nurses are highlighted throughout the literature as a key human resource whose proximity to families and other HCPs leads to naturally occurring opportunities for conversations about care [64,65]. Since nursing care is fundamental for supporting vital nutritional needs when challenges arise with a patient’s natural oral intake of food, nurses hold the unique position of “skilled companion” for patients and families, which predisposes them to opportunities for building relationships and leading multidisciplinary conversations about a patient’s care [65]. Some of the studies indicated that physicians and physician assistants may assume responsibility for facilitating EOL care decisions. Without defined roles, there remains hesitation and challenges in supporting families with EOL decision-making, particularly when family conflicts arise [13,64,66]. Further complicating the situation is that HCPs hold differing perspectives as to the benefits of ANH or how to engage families in decision-making around EOL nutrition [16,59].
Among HCPs, registered dietitians possess the specialized training in nutrition care that should position them as a key member of the multidisciplinary care team who can facilitate EOL nutrition care discussions with families and substitute decision makers or support other members of the care team [67]. Baird-Schwartz [68] argues that dietitians have a strong role on health care teams, helping to facilitate decisions about eating, drinking, and ANH as a component of care. Surprisingly, the role of dietitians was not addressed in the studies included in this review. In fact, the only paper that mentioned dietitians noted that their absence in the study represented a limitation. Dietitians are poised to make a strong contribution to supportive multidisciplinary care teams for residents at EOL.
A key consideration for the implementation of resources to support decision-making is staff availability. For instance, texture-modified therapeutic diets can be beneficial for residents who experience dysphagia, which is common among residents with severe dementia; however, assistance with eating is often required (e.g., supportive hand feeding, prompting, cueing to swallow). On the other hand, resources to support decision-making can outline other potential treatment options, such as the use of special utensils and oral care. Urban-rural differences in staff availability in LTC have also been shown to impact the uptake of decision aids [49]. Findings showed that rural LTC homes with fewer available staff found greater benefit from resources to support decision-making compared to their more highly staffed urban counterparts [49]. This suggests that decision aids helped to alleviate some of the pressure faced by HCPs, or perhaps supported HCPs and families to use their time together more effectively [49].
Though much of the literature captured in this review focused on supporting families and HCPs in decision-making, the authors of the included papers reiterated that the goal is that decisions be made with a resident-focused approach. Some authors illustrated the components of a resident-focused approach to decision-making [68,69]. For instance, Arcand [70] showed that with appropriate information and communication, families and HCPs can reach a consensus (ideally informed by the resident’s values) even when a resident is unable to participate in the decision-making process, allowing for care provision that supports the resident’s goals. Advance care plans or directives are sometimes conceptualized as processes that help residents and families consider potential scenarios, clarify goals of care, and make decisions to support their personal choices. However, advance care plans vary widely, and their use is not consistent, with evidence suggesting that they lack detail specific to eating and drinking at EOL and can be perceived as not relevant to a specific decision because they are not regularly updated [6]. Resources to support decisions about EOL nutrition care could perhaps be useful to supplement or guide interpretation of the information expressed within an advance care plan.
Cultural differences impact the development and uptake of decision aids for EOL nutrition care in LTC [13,34,70,71]. A notable gap in the existing literature was the limited mention of the cultural relevancy of available decision aids. Given the wide variation in cultural beliefs and values about EOL generally and EOL nutrition care specifically [7], recognition of cultural safety within decision aids is imperative.
Similarly, most of the resources to support decision-making did not include residents or family members/substitute decision makers in the development stage. One study, however, engaged residents living with mild dementia in the co-production process [46]. Although the ratio of residents to HCPs included in the study was low, the authors noted that capturing resident perspectives was valuable for informing the overall design of the decision aid. Since a resident’s goals of care are of central importance to any decision aid, including those designed for use by HCPs [72], engaging residents in the coproduction process is necessary for developing decision aids that represent integrated perspectives and lived experiences [46]. Future studies should draw on diverse groups of residents, staff, and families to generate culturally safe decision aids [71]. Additionally, currently available resources focus primarily on residents living with dementia or those who lack decision-making capacity. More inclusive resources would account for resident and family participation in the decision-making process; engaging residents and families is an important step towards cultivating inclusive LTC homes.
Limitations
Some limitations of our study should be noted. First, our inclusion and exclusion criteria omitted reviews based on the assumption that all relevant studies would be captured in the search and therefore retrieve only duplicate studies. It is possible, however, that by omitting review articles, we may have missed other authors’ interpretations of the findings. Second, our search strategy focused on retrieving evidence-based resources to support decision-making about nutrition at EOL that could be dispersed and implemented in LTC settings. Thus, more resources could exist but not be reflected in this study.
5. Conclusions
Decisions about EOL nutrition and hydration can be complex and multifaceted. Multidisciplinary care teams supporting residents and their families during EOL can benefit from resources to support discussion and facilitate decision-making.
Author Contributions
Conceptualization, A.C., P.H., A.W.-G., E.Y., and C.L.; methodology, A.C.; software, H.A., N.A., and A.C.; formal analysis, H.A., N.A., and A.C.; resources, A.C. and P.H.; data curation, H.A., N.A., and A.C.; writing—original draft preparation, H.A., N.A., and A.C.; writing—review and editing, P.H., A.W.-G., E.Y., and C.L.; supervision, A.C.; project administration, A.C.; funding acquisition, A.C. and P.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Saskatchewan Health Research Foundation, Align grant number 6481 and a University of Saskatchewan Interdisciplinary Summer Student Research Award.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Preedy, V. Handbook of Nutrition and Diet in Palliative Care, 2nd ed.; CRC Press: London, UK, 2019. [Google Scholar]
- del Río, M.I.; Shand, B.; Bonati, P.; Palma, A.; Maldonado, A.; Taboada, P.; Nervi, F. Hydration and nutrition at the end of life: A systematic review of emotional impact, perceptions, and decision-making among patients, family, and health care staff. Psycho-Oncology 2011, 21, 913–921. [Google Scholar] [CrossRef] [PubMed]
- Waldrop, D.P.; McGinley, J.M. Beyond Advance Directives: Addressing Communication Gaps and Caregiving Challenges at Life’s End. J. Pain Symptom Manag. 2022, 63, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Vossius, C.; Selbæk, G.; Benth, J.; Bergh, S. Mortality in nursing home residents: A longitudinal study over three years. PLoS ONE 2018, 13, e0203480. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Residential Care Facilities. 2010. Available online: https://www150.statcan.gc.ca/n1/en/pub/83-237-x/83-237-x2012001-eng.pdf?st=jBKM2RVH (accessed on 10 April 2024).
- Barrado-Martín, Y.; Nair, P.; Anantapong, K.; Aker, N.; Moore, K.J.; Smith, C.H.; Rait, G.; Sampson, E.L.; Ma, J.M.; Davies, N. Family caregivers’ and professionals’ experiences of supporting people living with dementia’s nutrition and hydration needs towards the end of life. Health Soc. Care Community 2022, 30, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.N. To What Extent Does Clinically Assisted Nutrition and Hydration Have a Role in the Care of Dying People? J. Palliat. Care 2020, 35, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Ho, F.; Lau, F.; Downing, M.G.; Lesperance, M. A reliability and validity study of the Palliative Performance Scale. BMC Palliat. Care 2008, 7, 10. [Google Scholar] [CrossRef]
- Kingdon, A.; Spathis, A.; Antunes, B.; Barclay, S. Medical communication and decision-making about assisted hydration in the last days of life: A qualitative study of doctors experienced with end of life care. Palliat. Med. 2022, 36, 1080–1091. [Google Scholar] [CrossRef] [PubMed]
- Canadian Institute for Health Information. Dementia in Long-Term Care. 2023. Available online: https://www.cihi.ca/en/dementia-in-canada/dementia-care-across-the-health-system/dementia-in-long-term-care (accessed on 10 April 2024).
- Ribera-Casado, J.-M. Feeding and hydration in terminal stage patients. Eur. Geriatr. Med. 2015, 6, 87–90. [Google Scholar] [CrossRef]
- Hochwald, I.H.; Yakov, G.; Radomyslsky, Z.; Danon, Y.; Nissanholtz-Gannot, R. Ethical challenges in end-stage dementia: Perspectives of professionals and family care-givers. Nurs. Ethics 2021, 28, 1228–1243. [Google Scholar] [CrossRef]
- Roach, A.; Rogers, A.H.; Mitchell, S.L.; McCarthy, E.P.; Lopez, R.P. Staff and Proxy Views of Multiple Family Member Involvement in Decision Making for Nursing Home Residents with Advanced Dementia. J. Hosp. Palliat. Nurs. 2023, 25, 263–270. [Google Scholar] [CrossRef]
- Baillie, J.; Anagnostou, D.; Sivell, S.; Van Godwin, J.; Byrne, A.; Nelson, A. Symptom management, nutrition and hydration at end-of-life: A qualitative exploration of patients’, carers’ and health professionals’ experiences and further research questions. BMC Palliat. Care 2018, 17, 60. [Google Scholar] [CrossRef] [PubMed]
- Raijmakers, N.J.; Clark, J.B.; van Zuylen, L.; Allan, S.G.; van der Heide, A. Bereaved relatives’ perspectives of the patient’s oral intake towards the end of life: A qualitative study. Palliat. Med. 2013, 27, 665–672. [Google Scholar] [CrossRef]
- Dunn, H. Hard Choices for Loving People: CRP, Feeding Tubes, Palliative Care, Comfort Measures, and the Patient with a Serious Illness, 6th ed.; Quality of Life Publishing Co.: Naples, FL, USA, 2019. [Google Scholar]
- Pengo, V.; Zurlo, A.; Voci, A.; Valentini, E.; De Zaiacomo, F.; Catarini, M.; Iasevoli, M.; Maggi, S.; Pegoraro, R.; Manzato, E.; et al. Advanced dementia: Opinions of physicians and nurses about antibiotic therapy, artificial hydration and nutrition in patients with different life expectancies. Geriatr. Gerontol. Int. 2017, 17, 487–493. [Google Scholar] [CrossRef]
- Barrado-Martín, Y.; Hatter, L.; Moore, K.J.; Sampson, E.L.; Rait, G.; Manthorpe, J.; Smith, C.H.; Nair, P.; Davies, N. Nutrition and hydration for people living with dementia near the end of life: A qualitative systematic review. J. Adv. Nurs. 2021, 77, 664–680. [Google Scholar] [CrossRef] [PubMed]
- Henry, B. Evolving ethical and legal implications for feeding at the end of life. Ann. Palliat. Med. 2017, 6, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Ying, I. Artificial nutrition and hydration in advanced dementia. Can. Fam. Physician 2015, 61, 245–248. [Google Scholar] [PubMed]
- Nakanishi, M.; Hattori, K. Percutaneous endoscopic gastrostomy (PEG) tubes are placed in elderly adults in Japan with advanced dementia regardless of expectation of improvement in quality of life. J. Nutr. Health Aging 2014, 18, 503–509. [Google Scholar] [CrossRef]
- Lokker, M.E.; Van der Heide, A.; Oldenmenger, W.H.; Van der Rijt, C.C.; Van Zuylen, L. Hydration and symptoms in the last days of life. BMJ Support. Palliat. Care 2021, 11, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Dev, R.; Dalal, S.; Bruera, E. Is there a role for parenteral nutrition or hydration at the end of life? Curr. Opin. Support. Palliat. Care 2012, 6, 365–370. [Google Scholar] [CrossRef]
- Druml, C.; Ballmer, P.E.; Druml, W.; Oehmichen, F.; Shenkin, A.; Singer, P.; Soeters, P.; Weimann, A.; Bischoff, S.C. ESPEN guideline on ethical aspects of artificial nutrition and hydration. Clin. Nutr. 2016, 35, 545–556. [Google Scholar] [CrossRef]
- Lee, Y.-F.; Hsu, T.-W.; Liang, C.-S.; Yeh, T.-C.; Chen, T.-Y.; Chen, N.-C.; Chu, C.-S. The Efficacy and Safety of Tube Feeding in Advanced Dementia Patients: A Systemic Review and Meta-Analysis Study. J. Am. Med. Dir. Assoc. 2021, 22, 357–363. [Google Scholar] [CrossRef]
- Davies, N.; Barrado-Martín, Y.; Vickerstaff, V.; Rait, G.; Fukui, A.; Candy, B.; Smith, C.H.; Manthorpe, J.; Moore, K.J.; Sampson, E.L. Enteral tube feeding for people with severe dementia. Emergencias 2021, 2021, CD013503. [Google Scholar] [CrossRef]
- Hui, D.; Dev, R.; Bruera, E. The Last Days of Life: Symptom Burden and Impact on Nutrition and Hydration in Cancer Patients. Curr. Opin. Support. Palliat. Care 2015, 9, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Somers, E.; Grey, C.; Satkoske, V. Withholding versus withdrawing treatment: Artificial nutrition and hydration as a model. Curr. Opin. Support. Palliat. Care 2016, 10, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Harrop, E.; Morgan, F.; Byrne, A.; Nelson, A. “It still haunts me whether we did the right thing”: A qualitative analysis of free text survey data on the bereavement experiences and support needs of family caregivers. BMC Palliat. Care 2016, 15, 92. [Google Scholar] [CrossRef] [PubMed]
- Eastern Cooperative Oncology Group (ECOG) Performance Status Scale. Available online: https://ecog-acrin.org/resources/ecog-performance-status/ (accessed on 10 April 2024).
- Péus, D.; Newcomb, N.; Hofer, S. Appraisal of the Karnofsky Performance Status and proposal of a simple algorithmic system for its evaluation. BMC Med. Inform. Decis. Mak. 2013, 13, 72. [Google Scholar] [CrossRef] [PubMed]
- Palecek, E.J.; Teno, J.M.; Casarett, D.J.; Hanson, L.C.; Rhodes, R.L.; Mitchell, S.L. Comfort Feeding Only: A Proposal to Bring Clarity to Decision-Making Regarding Difficulty with Eating for Persons with Advanced Dementia. J. Am. Geriatr. Soc. 2010, 58, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Loofs, T.S.; Haubrick, K. End-of-Life Nutrition Considerations: Attitudes, Beliefs, and Outcomes. Am. J. Hosp. Palliat. Med. 2021, 38, 1028–1041. [Google Scholar] [CrossRef] [PubMed]
- Xie, B.; Berkley, A.S.; Kwak, J.; Fleischmann, K.R.; Champion, J.D.; Koltai, K.S. End-of-life decision making by family caregivers of persons with advanced dementia: A literature review of decision aids. SAGE Open Med. 2018, 6, 2050312118777517. [Google Scholar] [CrossRef]
- Reinhardt, J.P.; Chichin, E.; Posner, L.; Kassabian, S. Vital Conversations with Family in the Nursing Home: Preparation for End-Stage Dementia Care. J. Soc. Work End Life Palliat. Care 2014, 10, 112–126. [Google Scholar] [CrossRef]
- Volk, R.J.; Llewellyn-Thomas, H.; Stacey, D.; Elwyn, G. Ten years of the International Patient Decision Aid Standards Collaboration: Evolution of the core dimensions for assessing the quality of patient decision aids. BMC Med. Inform. Decis. Mak. 2012, 13, S1. [Google Scholar] [CrossRef]
- Stacey, D.; Légaré, F.; Lewis, K.; Barry, M.J.; Bennett, C.L.; Eden, K.B.; Holmes-Rovner, M.; Llewellyn-Thomas, H.; Lyddiatt, A.; Thomson, R.; et al. Decision Aids for People Facing Health Treatment or Screening Decisions (Review). 2017. Available online: www.cochranelibrary.com (accessed on 18 March 2024).
- Graham, I.D.; Logan, J.; Bennett, C.L.; Presseau, J.; O’Connor, A.M.; Mitchell, S.L.; Tetroe, J.M.; Cranney, A.; Hebert, P.; Aaron, S.D. Physicians’ intentions and use of three patient decision aids. BMC Med. Inform. Decis. Mak. 2007, 7, 20. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’brien, K.K. Scoping Studies: Advancing the Methodology. 2010. Available online: http://www.cihr-irsc.ca (accessed on 10 April 2024).
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. J. Soc. Res. Method. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Systematic Reviews. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- CASP Checklists. 2023. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 10 April 2024).
- Arcand, M.; Monette, J.; Monette, M.; Sourial, N.; Fournier, L.; Gore, B.; Bergman, H. Educating Nursing Home Staff About the Progression of Dementia and the Comfort Care Option: Impact on Family Satisfaction with End-of-Life Care. J. Am. Med. Dir. Assoc. 2009, 10, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Arcand, M.; Brazil, K.; Nakanishi, M.; Nakashima, T.; Alix, M.; Desson, J.-F.; Morello, R.; Belzile, L.; Beaulieu, M.; Hertogh, C.M.; et al. Educating families about end-of-life care in advanced dementia: Acceptability of a Canadian family booklet to nurses from Canada, France, and Japan. Int. J. Palliat. Nurs. 2013, 19, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.-Z.D.; Bourgeois, M.S. Effects of Visual Aids for End-of-Life Care on Decisional Capacity of People with Dementia. Am. J. Speech-Lang. Pathol. 2020, 29, 185–200. [Google Scholar] [CrossRef]
- Davies, N.; Sampson, E.L.; West, E.; DeSouza, T.; Manthorpe, J.; Moore, K.; Walters, K.; Dening, K.H.; Ward, J.; Rait, G. A decision aid to support family carers of people living with dementia towards the end-of-life: Coproduction process, outcome and reflections. Health Expect. 2021, 24, 1677–1691. [Google Scholar] [CrossRef] [PubMed]
- Eggenberger, S.K.; Nelms, T.P. Artificial hydration and nutrition in advanced Alzheimer’s disease: Facilitating family decision-making. J. Clin. Nurs. 2004, 13, 661–667. [Google Scholar] [CrossRef]
- van der Steen, J.T.; Hertogh, C.M.P.M.; de Graas, T.; Nakanishi, M.; Toscani, F.; Arcand, M. Translation and cross-cultural adaptation of a family booklet on comfort care in dementia: Sensitive topics revised before implementation. J. Med. Ethics 2013, 39, 104–109. [Google Scholar] [CrossRef]
- Ersek, M.; Sefcik, J.S.; Lin, F.C.; Lee, T.J.; Gilliam, R.; Hanson, L.C. Provider Staffing Effect on a Decision Aid Intervention. Clin. Nurs. Res. 2014, 23, 36–53. [Google Scholar] [CrossRef]
- Hanson, L.C.; Carey, T.S.; Caprio, A.J.; Joon Lee, T.; Ersek, M.; Garrett, J.; Jackman, A.; Gilliam, R.; Wessell, K.; Mitchell, S.L.; et al. Improving Decision Making for Feeding Options in Advanced Dementia: A Randomized, Controlled Trial. J. Am. Geriatr. Soc. 2011, 59, 2009–2016. [Google Scholar] [CrossRef]
- Loizeau, A.J.; Theill, N.; Cohen, S.M.; Eicher, S.; Mitchell, S.L.; Meier, S.; McDowell, M.; Martin, M.; Riese, F. Fact Box decision support tools reduce decisional conflict about antibiotics for pneumonia and artificial hydration in advanced dementia: A randomized controlled trail. J. Am. Geriatr. Soc. 2019, 48, 67–74. [Google Scholar] [CrossRef]
- Riedl, L.; Bertok, M.; Hartmann, J.; Fischer, J.; Rossmeier, C.; Dinkel, A.; Ortner, M.; Diehl-Schmid, J. Development and testing of an informative guide about palliative care for family caregivers of people with advanced dementia. BMC Palliat. Care 2020, 19, 30. [Google Scholar] [CrossRef] [PubMed]
- Snyder, E.A.; Caprio, A.J.; Wessell, K.; Lin, F.C.; Hanson, L.C. Impact of a Decision Aid on Surrogate Decision-Makers’ Perceptions of Feeding Options for Patients with Dementia. J. Am. Med. Dir. Assoc. 2013, 14, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Holmes, S. Withholding or withdrawing nutrition at the end of life. Nurs. Stand. 2010, 25, 43–46. [Google Scholar] [CrossRef]
- Suter, P.M.; Rogers, J.; Strack, C. Artificial Nutrition and Hydration for the Terminally Ill A Reasoned Approach. 2008. Available online: www.homehealthcarenurseonline.com (accessed on 10 April 2024).
- van der Steen, J.T.; Arcand, M.; Toscani, F.; de Graas, T.; Finetti, S.; Beaulieu, M.; Brazil, K.; Nakanishi, M.; Nakashima, T.; Knol, D.L.; et al. A Family Booklet About Comfort Care in Advanced Dementia: Three-Country Evaluation. J. Am. Med. Dir. Assoc. 2012, 13, 368–375. [Google Scholar] [CrossRef]
- van der Steen, J.T.; Heck, S.; Juffermans, C.C.; Garvelink, M.M.; Achterberg, W.P.; Clayton, J.; Thompson, G.; Koopmans, R.T.; van der Linden, Y.M. Practitioners’ perceptions of acceptability of a question prompt list about palliative care for advance care planning with people living with dementia and their family caregivers: A mixed-methods evaluation study. BMJ Open 2021, 11, e044591. [Google Scholar] [CrossRef] [PubMed]
- Arcand, M.; Caron, C. Comfort Care at the End of Life for Persons with Alzheimer’s Disease or Other Degenerative Diseases of the Brain—A Guide for Caregivers; Centre d’expertise en sante de Sherbrooke: Sherbrooke, QC, Canada, 2005. [Google Scholar]
- van der Steen, J.T.; Toscani, F.; de Graas, T.; Finetti, S.; Nakanishi, M.; Nakashima, T.; Brazil, K.; Hertogh, C.M.P.M.; Arcand, M. Physicians’ and Nurses’ Perceived Usefulness and Acceptability of a Family Information Booklet about Comfort Care in Advanced Dementia. J. Palliat. Med. 2011, 14, 614–622. [Google Scholar] [CrossRef]
- Givens, J.L.; Kiely, D.K.; Carey, K.; Mitchell, S.L. Healthcare proxies of nursing home residents with advanced dementia: Decisions they confront and their satisfaction with decision-making: Clinical investigations. J. Am. Geriatr. Soc. 2009, 57, 1149–1155. [Google Scholar] [CrossRef]
- Mitchell, S.L.; Tetroe, J.; O’Connor, A.M. A Decision Aid for Long-Term Tube Feeding in Cognitively Impaired Older Persons. J. Am. Geriatr. Soc. 2001, 49, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Roach, A.; Rogers, A.H.; Hendricksen, M.; McCarthy, E.P.; Mitchell, S.L.; Lopez, R.P. Guilt as an Influencer in End-of-Life Care Decisions for Nursing Home Residents with Advanced Dementia. J. Gerontol. Nurs. 2022, 48, 22–27. [Google Scholar] [CrossRef]
- Noh, H.; Kwak, J. End-of-life decision making for persons with dementia: Proxies’ perception of support. Dementia 2016, 17, 478–493. [Google Scholar] [CrossRef] [PubMed]
- Firnhaber, G.C.; Roberson, D.W.; Kolasa, K.M. Nursing staff participation in end-of-life nutrition and hydration decision-making in a nursing home: A qualitative study. J. Adv. Nurs. 2020, 76, 3059–3068. [Google Scholar] [CrossRef]
- Albanesi, B.; Marchetti, A.; D’Angelo, D.; Capuzzo, M.T.; Mastroianni, C.; Artico, M.; Lusignani, M.; Piredda, M.; De Marinis, M.G. Exploring Nurses’ Involvement in Artificial Nutrition and Hydration at the End of Life: A Scoping Review. J. Parenter. Enter. Nutr. 2020, 44, 1220–1233. [Google Scholar] [CrossRef]
- De, D.; Thomas, C. Enhancing the Decision Making Process when Considering Artificial Nutrition in Advanced Dementia Care. Int. J. Palliat. Nurs. 2019, 25, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Keller, H.; Slaughter, S.; Gramlich, L.; Namasivayam-MacDonald, A.; Bell, J.J. Multidisciplinary Nutrition Care: Benefitting Patients with Malnutrition Across Healthcare Sectors. In Interdisciplinary Nutritional Management and Care for Older Adults: An Evidence-Based Practical Guide for Nurses; Springer: Cham, Switzerland, 2021; pp. 177–188. [Google Scholar] [CrossRef]
- Schwartz, D.B.; Barrocas, A.; Wesley, J.R.; Kliger, G.; Pontes-Arruda, A.; Márquez, H.A.; James, R.L.; Monturo, C.; Lysen, L.K.; DiTucci, A. Gastrostomy Tube Placement in Patients with Advanced Dementia or Near End of Life. Nutr. Clin. Pract. 2014, 29, 829–840. [Google Scholar] [CrossRef]
- Mitchell, S.L. A 93-Year-Old Man with Advanced Dementia and Eating Problems. JAMA 2007, 298, 2527–2536. [Google Scholar] [CrossRef]
- Arcand, M. End-of-life issues in advanced dementia: Part 1: Goals of care, decision-making process, and family education. Can. Fam. Physician 2015, 61, 330–334. [Google Scholar] [PubMed]
- Mayers, T.; Kashiwagi, S.; Mathis, B.J.; Kawabe, M.; Gallagher, J.; Aliaga, M.L.M.; Kai, I.; Tamiya, N. International review of national-level guidelines on end-of-life care with focus on the withholding and withdrawing of artificial nutrition and hydration. Geriatr. Gerontol. Int. 2019, 19, 847–853. [Google Scholar] [CrossRef]
- Dobak, S. Navigating Conversations Surrounding Nutrition Support at the End of Life. Support Line. 2019, Volume 41, pp. 18–23. Available online: https://www.proquest.com/docview/2225773481/3214204D71854CCEPQ/1?sourcetype=Trade%20Journals (accessed on 10 April 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).