
Evaluation of Arsenic and Cobalt Levels in Pediatric Patients Receiving Long-Term Parenteral Nutrition
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials
Study Participants
3. Methods
3.1. Test Tubes
3.2. Determination of As and Co
3.3. Quality Control
3.4. Statistical Analysis
4. Results
4.1. Serum and Urine As and Co Levels in the Study and Control Groups
4.2. Sex-Dependent Differences in Serum and Urine As and Co
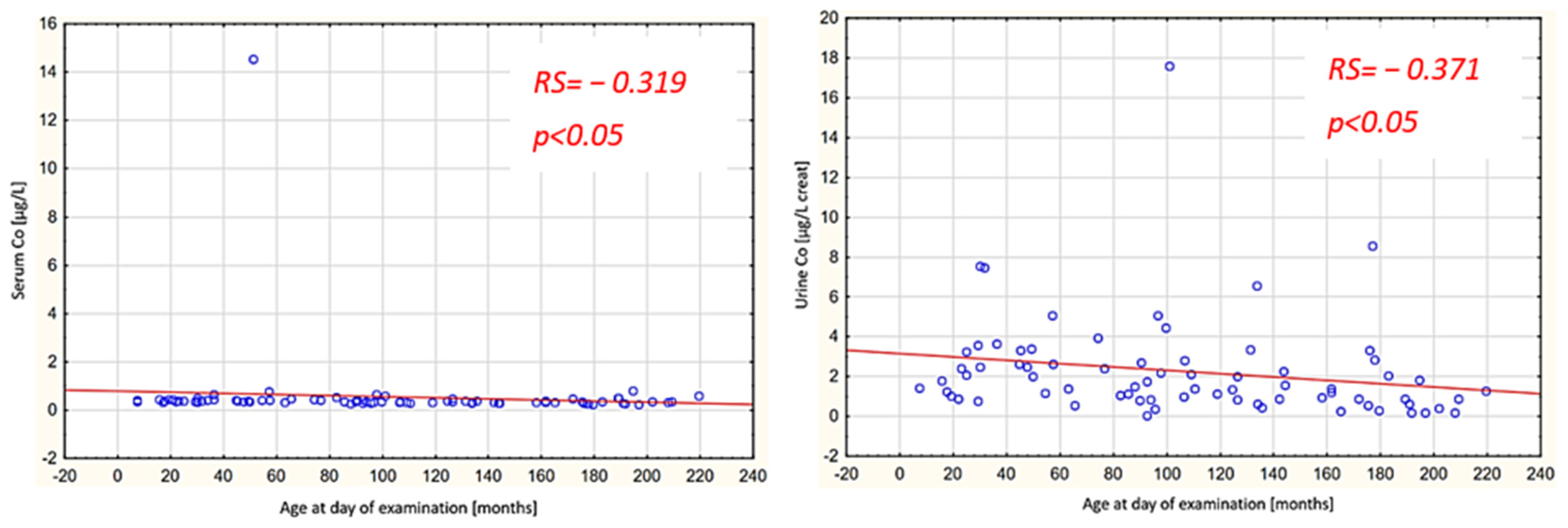
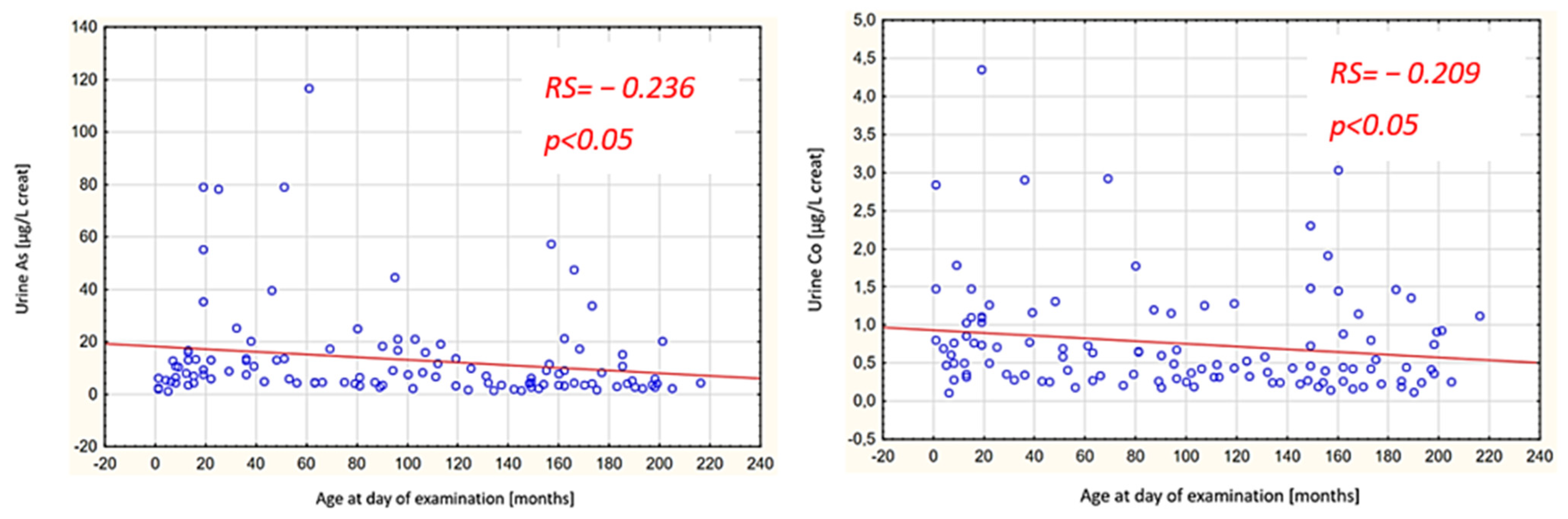
4.3. Age-Dependent Differences in Serum and Urine As and Co
5. Discussion
5.1. Arsenic
5.2. Cobalt
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bering, J.; DiBaise, J.K. Short bowel syndrome: Complications and management. Nutr. Clin. Pract. 2023, 38 (Suppl. S1), S46–S58. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.-K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.-L.; et al. ESPEN micronutrient guideline. Clin. Nutr. 2022, 41, 1357–1424. [Google Scholar] [CrossRef] [PubMed]
- Hardy, G.; Wong, T.; Morrissey, H.; Anderson, C.; Moltu, S.J.; Poindexter, B.; Lapillonne, A.; Ball, P.A. Parenteral Provision of Micronutrients to Pediatric Patients: An International Expert Consensus Paper. J. Parenter. Enter. Nutrition 2020, 44 (Suppl. S2), S5–S23. [Google Scholar] [CrossRef]
- Domellöf, M.; Szitanyi, P.; Simchowitz, V.; Franz, A.; Mimouni, F.; ESPGHAN/ESPEN/ESPR/CSPEN working group on pediatric parenteral nutrition. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Iron and trace minerals. Clin. Nutr. 2018, 37, 2354–2359. [Google Scholar] [CrossRef]
- Vanek, V.W.; Borum, P.; Buchman, A.; Fessler, T.A.; Howard, L.; Jeejeebhoy, K.; Kochevar, M.; Shenkin, A.; Valentine, C.J.; Novel Nutrient Task Force, Parenteral Multi-Vitamin and Multi–Trace Element Working Group; et al. A.S.P.E.N. position paper: Recommendations for changes in commercially available parenteral multivitamin and multi-trace element products. Nutr. Clin. Pract. 2012, 27, 440–491. [Google Scholar] [CrossRef]
- Romanowska, H.; Bartoszewicz, K.; Danko, M.; Wielopolska, J.; Popińska, K.; Żydak, J.; Sibilska, M.; Borkowska, A.; Szlagatys-Sidorkiewicz, A.; Książyk, J. Unexpected Serum and Urine Aluminum Concentrations in Pediatric Patients on Home Parenteral Nutrition. Nutrients 2023, 15, 3597. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.C., Jr.; Ruella Oliveira, S.; Barbosa, F., Jr.; Tinkov, A.A.; VSkalny, A.; Santamaría, A.; Lee, E.; Bowman, A.B.; Aschner, M. Evaluating the risk of manganese-induced neurotoxicity of parenteral nutrition: Review of the current literature. Expert Opin. Drug Metab. Toxicol. 2021, 17, 581–593. [Google Scholar] [CrossRef]
- Hardy, G.; Reilly, C. Technical aspects of trace element supplementation. Curr. Opin. Clin. Nutr. Metab. Care 1999, 2, 277–285. [Google Scholar] [CrossRef]
- Jomova, K.; Jenisova, Z.; Feszterova, M.; Baros, S.; Liska, J.; Hudecova, D.; Rhodes, C.J.; Valko, M. Arsenic: Toxicity, oxidative stress and human disease. J. Appl. Toxicol. 2011, 31, 95–107. [Google Scholar] [CrossRef]
- Alao, M.E.; Perin, J.; Brooks, W.A.; Hossain, L.; Goswami, D.; Zaman, K.; Yunus, M.; Khan, M.A.; Jahan, Y.; Ahmed, D.; et al. Urinary arsenic is associated with wasting and underweight status in young children in rural Bangladesh. Environ. Res. 2021, 195, 110025. [Google Scholar] [CrossRef]
- Rahman, M.M.; Naidu, R.; Bhattacharya, P. Arsenic contamination in groundwater in the Southeast Asia region. Environ. Geochem. Health 2009, 31 (Suppl. S1), 9–21. [Google Scholar] [CrossRef]
- Baeyens, W.; Vrijens, J.; Gao, Y.; Croes, K.; Schoeters, G.; Den Hond, E.; Sioen, I.; Bruckers, L.; Nawrot, T.; Nelen, V.; et al. Trace metals in blood and urine of newborn/mother pairs, adolescents and adults of the Flemish population (2007–2011). Int. J. Hyg. Environ. Health 2014, 217, 878–890. [Google Scholar] [CrossRef] [PubMed]
- Gundert-Remy, U.; Damm, G.; Foth, H.; Freyberger, A.; Gebel, T.; Golka, K.; Röhl, C.; Schupp, T.; Wollin, K.-M.; Hengstler, J.G. High exposure to inorganic arsenic by food: The need for risk reduction. Arch. Toxicol. 2015, 89, 2219–2227. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press (US): Washington, DC, USA, 2001; ISBN 978-0-309-07279-3. Available online: http://www.ncbi.nlm.nih.gov/books/NBK222310/ (accessed on 2 February 2024).
- Sawada, N. Association between Arsenic Intake and Cancer-From the Viewpoint of Epidemiological Study. Nihon Eiseigaku Zasshi 2018, 73, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Wilk, A.; Wiszniewska, B. Arsenic and Selenium Profile in Erythrocytes of Renal Transplant Recipients. Biol. Trace Elem. Res. 2020, 197, 421–430. [Google Scholar] [CrossRef]
- Bohrer, D.; do Nascimento, P.C.; Becker, E.; de Carvalho, L.M.; Dessuy, M. Arsenic species in solutions for parenteral nutrition. JPEN J. Parenter. Enteral Nutr. 2005, 29, 1–7. [Google Scholar] [CrossRef]
- Al-Saleh, I.; Al-Rouqi, R.; Alnuwaysir, H.; Aldhalaan, H.; Alismail, E.; Binmanee, A.; Hawari, A.; Alhazzani, F.; Bin Jabr, M. Exposure of preterm neonates to toxic metals during their stay in the Neonatal Intensive Care Unit and its impact on neurodevelopment at 2 months of age. J. Trace Elem. Med. Biol. 2023, 78, 127173. [Google Scholar] [CrossRef]
- Munteanu, C.R.; Suntharalingam, K. Advances in cobalt complexes as anticancer agents. Dalton Trans. 2015, 44, 13796–13808. [Google Scholar] [CrossRef]
- Scarselli, A.; Di Marzio, D.; Iavicoli, S. Assessment of exposure to cobalt and its compounds in Italian industrial settings. Med. Lav. 2020, 111, 22–31. [Google Scholar] [CrossRef]
- Moulin, J.J.; Wild, P.; Romazini, S.; Lasfargues, G.; Peltier, A.; Bozec, C.; Deguerry, P.; Pellet, F.; Perdrix, A. Lung cancer risk in hard-metal workers. Am. J. Epidemiol. 1998, 148, 241–248. [Google Scholar] [CrossRef]
- Pluhator-Murton, M.M.; Fedorak, R.N.; Audette, R.J.; Marriage, B.J.; Yatscoff, R.W.; Gramlich, L.M. Trace element contamination of total parenteral nutrition. 1. Contribution of component solutions. JPEN J. Parenter. Enteral Nutr. 1999, 23, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Nañagas, K.A.; Tormoehlen, L.M. Extremely high urine arsenic level after remote seafood ingestion. Am. J. Ther. 2014, 21, e75–e77. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, J.S.; Garry, M.R.; Perez, V.; Chang, E.T. Low-level arsenic exposure and developmental neurotoxicity in children: A systematic review and risk assessment. Toxicology 2015, 337, 91–107. [Google Scholar] [CrossRef]
- Gardner, R.M.; Kippler, M.; Tofail, F.; Bottai, M.; Hamadani, J.; Grandér, M.; Nermell, B.; Palm, B.; Rasmussen, K.M.; Vahter, M. Environmental exposure to metals and children’s growth to age 5 years: A prospective cohort study. Am. J. Epidemiol. 2013, 177, 1356–1367. [Google Scholar] [CrossRef]
- Rychert-Stos, M.; Walczak, M.; Horodnicka-Jozwa, A.; Romanowska, H.; Katuszonek, D.; Wyka, K.; Chojnacka, H.; Marciniak, W.; Lubiński, J.; Petriczko, E. Do trace elements influence the course of newly diagnosed type 1 diabetes mellitus? Neuro Endocrinol. Lett. 2022, 43, 247–256. [Google Scholar]
- Rocha, G.H.O.; Steinbach, C.; Munhoz, J.R.; Madia, M.a.O.; Faria, J.K.; Hoeltgebaum, D.; Barbosa, F.; Batista, B.L.; Souza, V.C.O.; Nerilo, S.B.; et al. Trace metal levels in serum and urine of a population in southern Brazil. J. Trace Elem. Med. Biol. 2016, 35, 61–65. [Google Scholar] [CrossRef]
- Jacobson, S.; Wester, P.-O. Balance study of twenty trace elements during total parenteral nutrition in man. Br. J. Nutr. 1977, 37, 107–126. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Schulz, C.; Kaus, S.; Seiwert, M.; Seifert, B. German Environmental Survey 1998 (GerES III): Environmental pollutants in the urine of the German population. Int. J. Hyg. Environ. Health 2003, 206, 15–24. [Google Scholar] [CrossRef]
- NHANES. Fourth National Report on Human Exposure to Environmental Chemicals. 2009. Available online: http://www.cdc.gov/exposurereport/ (accessed on 10 March 2024).
- Angelova, M.G.; Petkova-Marinova, T.V.; Pogorielov, M.V.; Loboda, A.N.; Nedkova-Kolarova, V.N.; Bozhinova, A.N. Trace Element Status (Iron, Zinc, Copper, Chromium, Cobalt, and Nickel) in Iron-Deficiency Anaemia of Children under 3 Years. Anemia 2014, 2014, 718089. [Google Scholar] [CrossRef]
- Kamath, L.; Ratageri, V.H.; Kanthi, A.S.; Fattepur, S.R.; Desai, R.H. Status of Vitamin B12, Zinc, Copper, Selenium, Manganese, Molybdenum and Cobalt in Severe Acute Malnutrition. Indian. J. Pediatr. 2023, 90, 988–993. [Google Scholar] [CrossRef]
- Nicoloff, G.; Angelova, M.; Christova, I.; Nikolov, A.; Alexiev, A. Serum cobalt in children with essential hypertension. Am. J. Hum. Biol. 2006, 18, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wang, C.; Wang, Y.; Zhao, X.; Li, N. Determination of 11 minerals in children using inductively coupled plasma mass spectrometry. BMC Pediatr. 2021, 21, 483. [Google Scholar] [CrossRef] [PubMed]
- Junqué, E.; Grimalt, J.O.; Fernández-Somoano, A.; Tardón, A. Urinary cobalt and ferritin in four-years-old children. Environ. Res. 2020, 183, 109147. [Google Scholar] [CrossRef] [PubMed]
- Roca, M.; Sánchez, A.; Pérez, R.; Pardo, O.; Yusà, V. Biomonitoring of 20 elements in urine of children. Levels and predictors of exposure. Chemosphere 2016, 144, 1698–1705. [Google Scholar] [CrossRef]
- Chang, L.; Shen, S.; Zhang, Z.; Song, X.; Jiang, Q. Study on the relationship between age and the concentrations of heavy metal elements in human bone. Ann. Transl. Med. 2018, 6, 320. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Trace Element | Group Size | Median | Range [Min–Max] | Lower Q | Upper Q | p-Value | |
|---|---|---|---|---|---|---|---|
| As in serum [µg/L] | Study group | 83 | 0.63 | 0.51–3.04 | 0.59 | 0.77 | NS |
| Control group | 121 | 0.65 | 0.37–8.91 | 0.58 | 0.78 | ||
| Co in serum [µg/L] | Study group | 83 | 0.37 | 0.24–14.54 | 0.33 | 0.42 | p < 0.001 |
| Control group | 121 | 0.29 | 0.16–0.79 | 0.24 | 0.34 | ||
| As in urine [µg/g creatinine] | Study group | 74 | 4.59 | 0.1–124.56 | 2.84 | 11.03 | p < 0.01 |
| Control group | 114 | 6.97 | 1.14–116.7 | 4.04 | 13.67 | ||
| Co in urine [µg/g creatinine] | Study group | 74 | 1.46 | 0.03–17.6 | 0.88 | 2.72 | p < 0.001 |
| Control group | 114 | 0.5 | 0.11–4.35 | 0.3 | 1.03 |
| Trace Element | Gender | Group Size | Median | Range [Min–Max] | Lower Q | Upper Q | p-Value |
|---|---|---|---|---|---|---|---|
| Study group | |||||||
| As in serum [µg/L] | Female | 31 | 0.61 | 0.51–2.32 | 0.57 | 0.72 | p < 0.05 |
| Male | 52 | 0.63 | 0.55–3.04 | 0.6 | 0.8 | ||
| As in urine [µg/g creatinine] | Female | 28 | 3.5 | 0.87–21.85 | 2.16 | 6.28 | p < 0.05 |
| Male | 46 | 5.73 | 0.1–124.55 | 3.15 | 14.24 | ||
| Co in serum [µg/L] | Female | 31 | 0.37 | 0.27–0.77 | 0.34 | 0.42 | NS |
| Male | 52 | 0.36 | 0.24–14.54 | 0.32 | 0.43 | ||
| Co in urine [µg/g creatinine] | Female | 28 | 1.37 | 0.2–7.53 | 0.94 | 2.44 | NS |
| Male | 46 | 1.81 | 0.03–17.6 | 0.87 | 3.31 | ||
| Control group | |||||||
| As in serum [µg/L] | Female | 54 | 0.66 | 0.51–1.9 | 0.6 | 0.77 | NS |
| Male | 67 | 0.61 | 0.37–8.9 | 0.57 | 0.85 | ||
| As in urine [µg/g creatinine] | Female | 51 | 6.89 | 1.36–79.23 | 4.28 | 16.07 | NS |
| Male | 63 | 7.05 | 1.15–116.71 | 3.68 | 13.10 | ||
| Co in serum [µg/L] | Female | 54 | 0.28 | 0.16–0.79 | 0.25 | 0.38 | NS |
| Male | 67 | 0.3 | 0.16–0.54 | 0.24 | 0.33 | ||
| Co in urine [µg/g creatinine] | Female | 51 | 0.58 | 0.18–4.35 | 0.32 | 1.16 | NS |
| Male | 63 | 0.48 | 0.11–3.03 | 0.27 | 0.89 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romanowska, H.; Wilk, A.; Danko, M.; Borkowska, A.; Popińska, K.; Sibilska, M.; Żydak, J.; Marciniak, W.; Szlagatys-Sidorkiewicz, A.; Książyk, J. Evaluation of Arsenic and Cobalt Levels in Pediatric Patients Receiving Long-Term Parenteral Nutrition. Nutrients 2024, 16, 1179. https://doi.org/10.3390/nu16081179
Romanowska H, Wilk A, Danko M, Borkowska A, Popińska K, Sibilska M, Żydak J, Marciniak W, Szlagatys-Sidorkiewicz A, Książyk J. Evaluation of Arsenic and Cobalt Levels in Pediatric Patients Receiving Long-Term Parenteral Nutrition. Nutrients. 2024; 16(8):1179. https://doi.org/10.3390/nu16081179
Chicago/Turabian StyleRomanowska, Hanna, Aleksandra Wilk, Mikołaj Danko, Anna Borkowska, Katarzyna Popińska, Marta Sibilska, Joanna Żydak, Wojciech Marciniak, Agnieszka Szlagatys-Sidorkiewicz, and Janusz Książyk. 2024. "Evaluation of Arsenic and Cobalt Levels in Pediatric Patients Receiving Long-Term Parenteral Nutrition" Nutrients 16, no. 8: 1179. https://doi.org/10.3390/nu16081179