
Wild Blueberry Extract Intervention in Healthy Older Adults: A Multi-Study, Randomised, Controlled Investigation of Acute Cognitive and Cardiovascular Effects

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. ROAB—Study 1
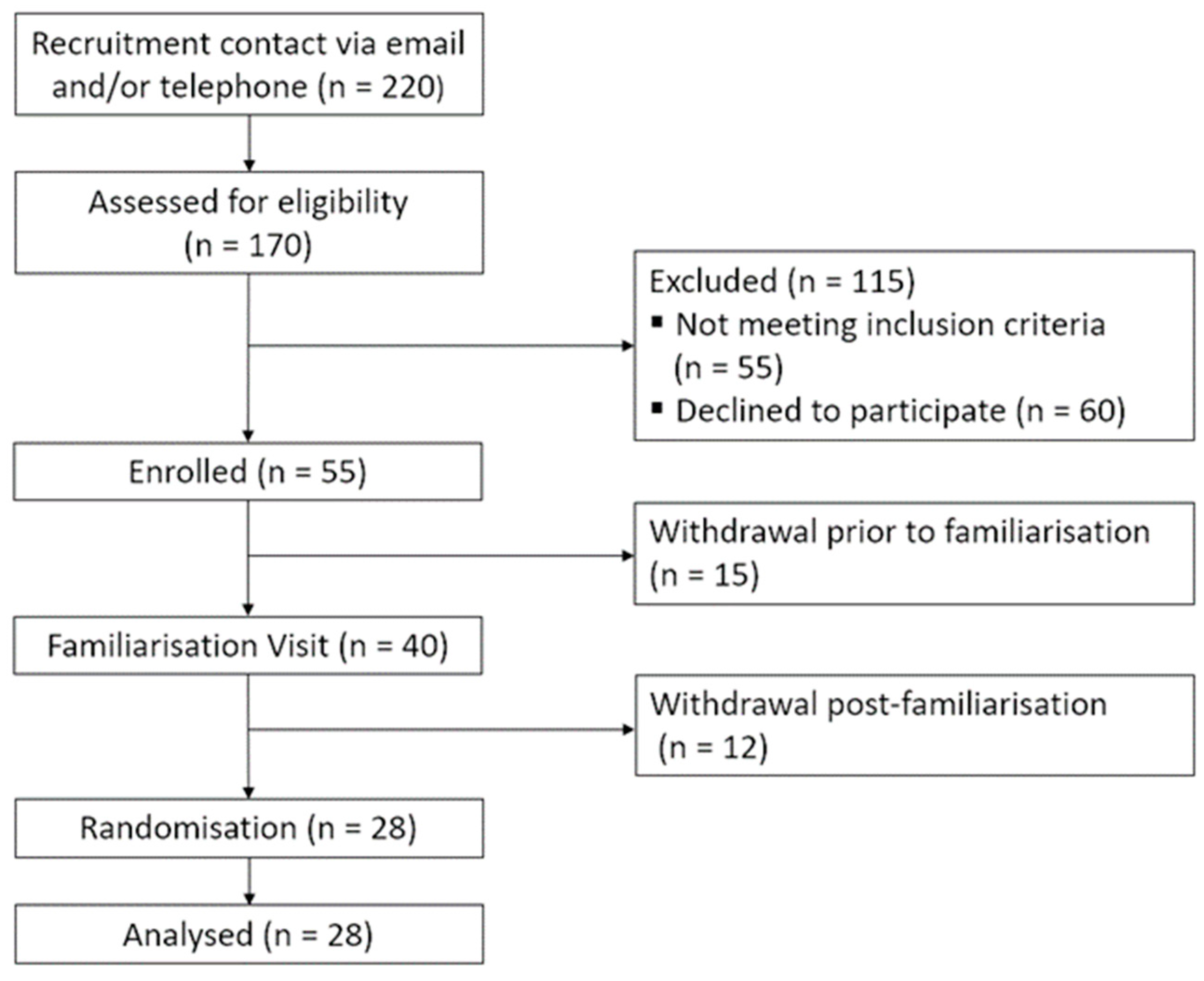
2.2.1. Participants
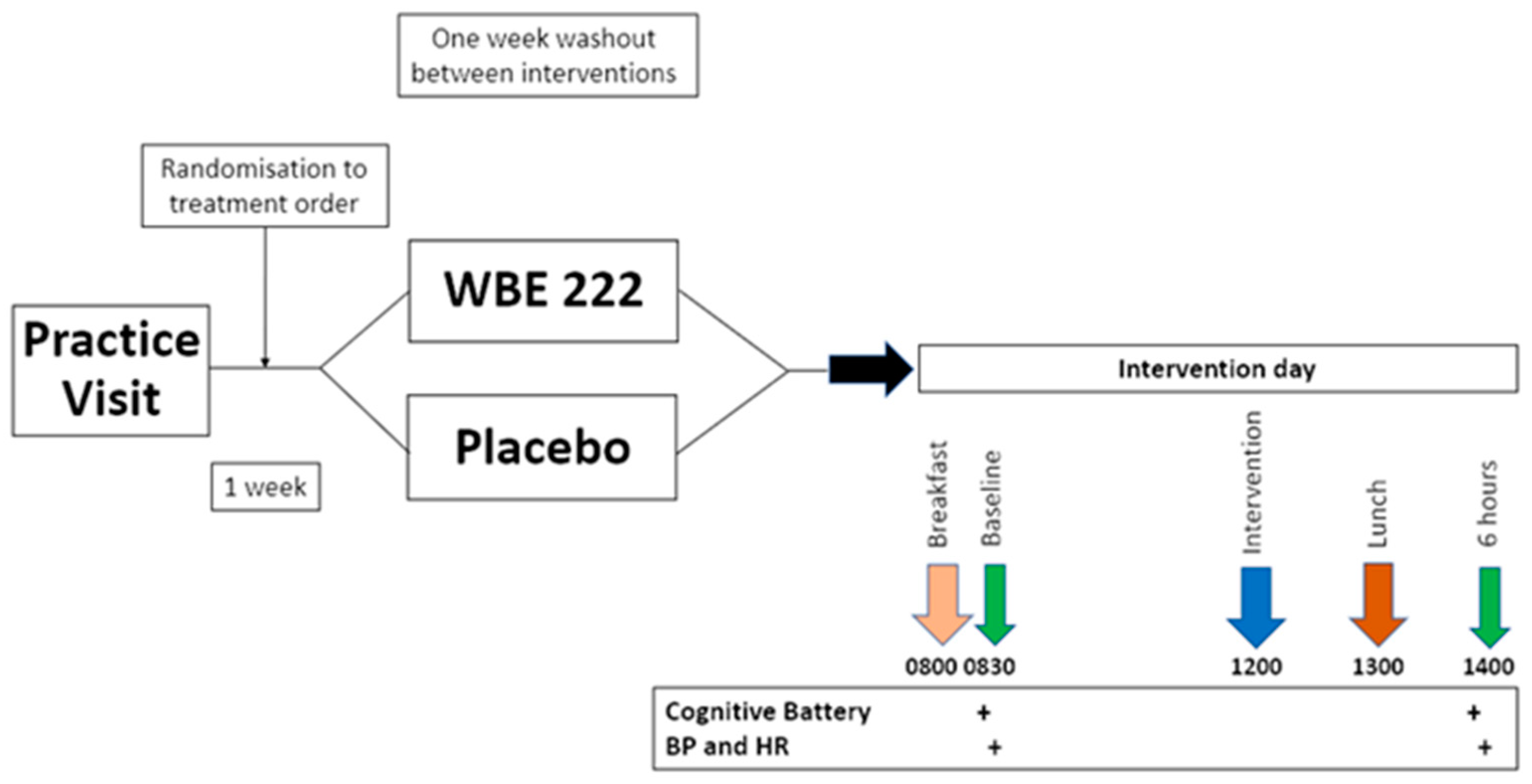
2.2.2. Design
2.2.3. Intervention
2.2.4. Screening Measures
2.2.5. Cognitive Tests
2.2.6. Mood
2.2.7. Cardiovascular Measures
2.2.8. Procedure
2.3. BEAT Study 2
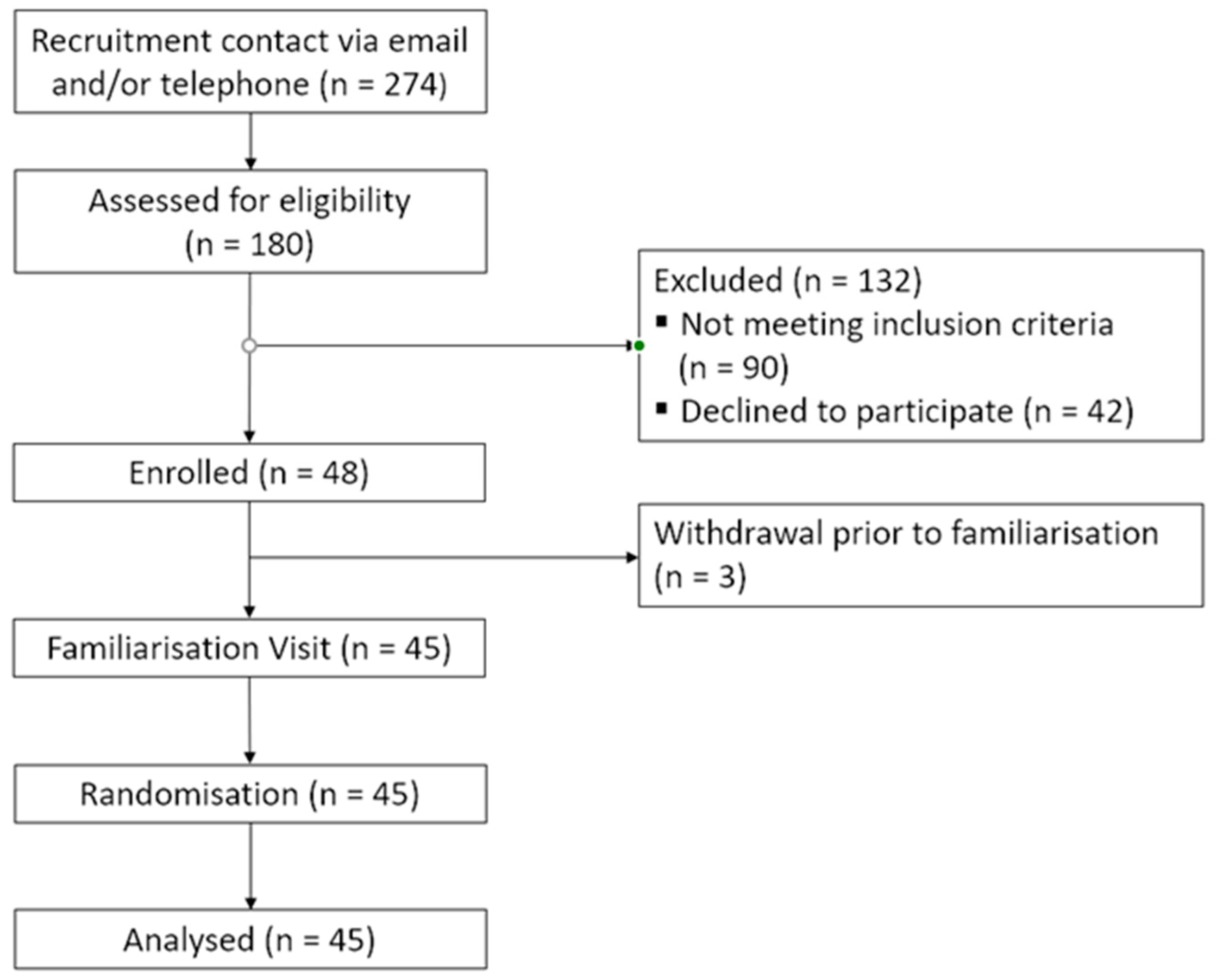
2.3.1. Participants
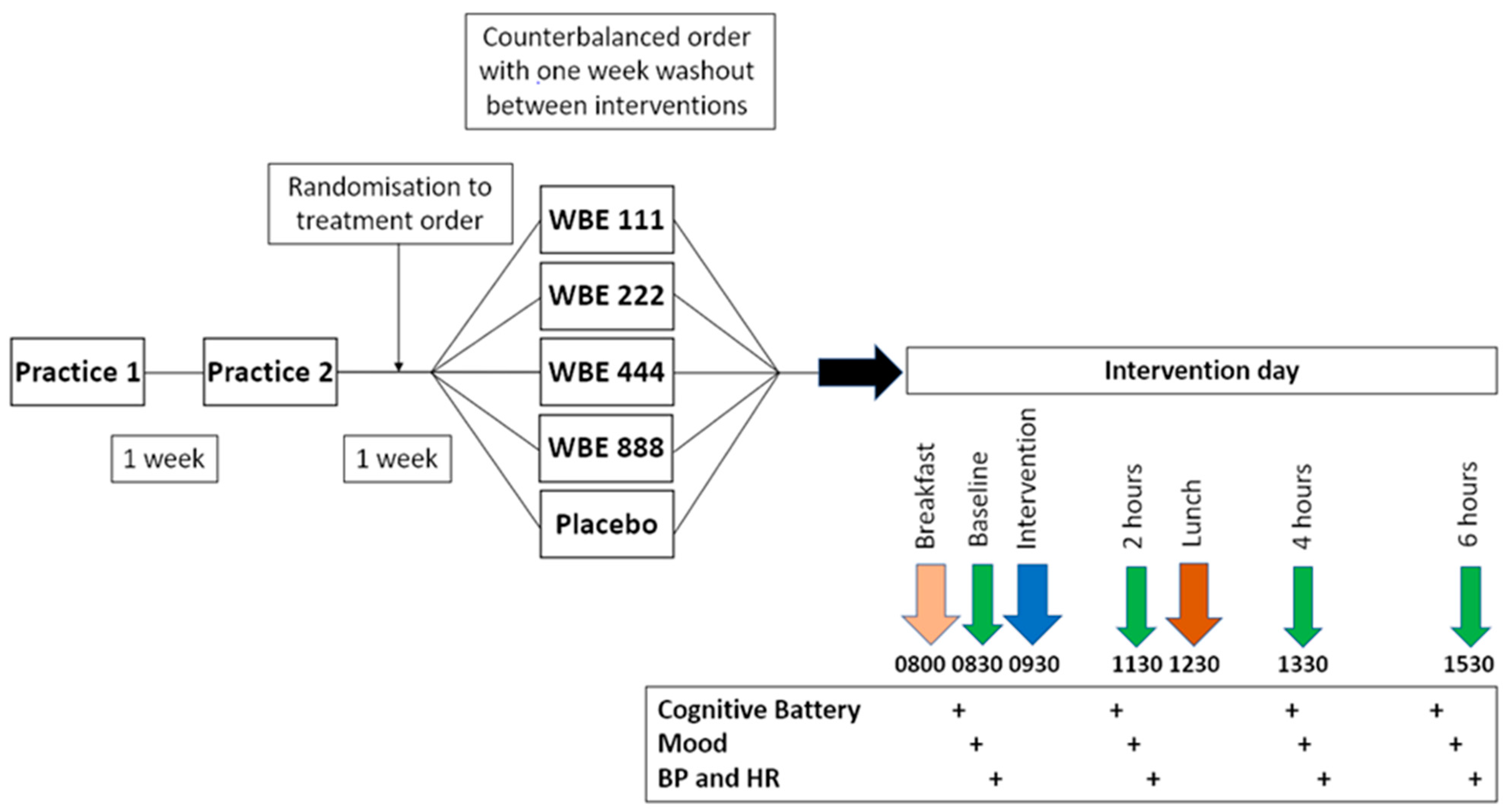
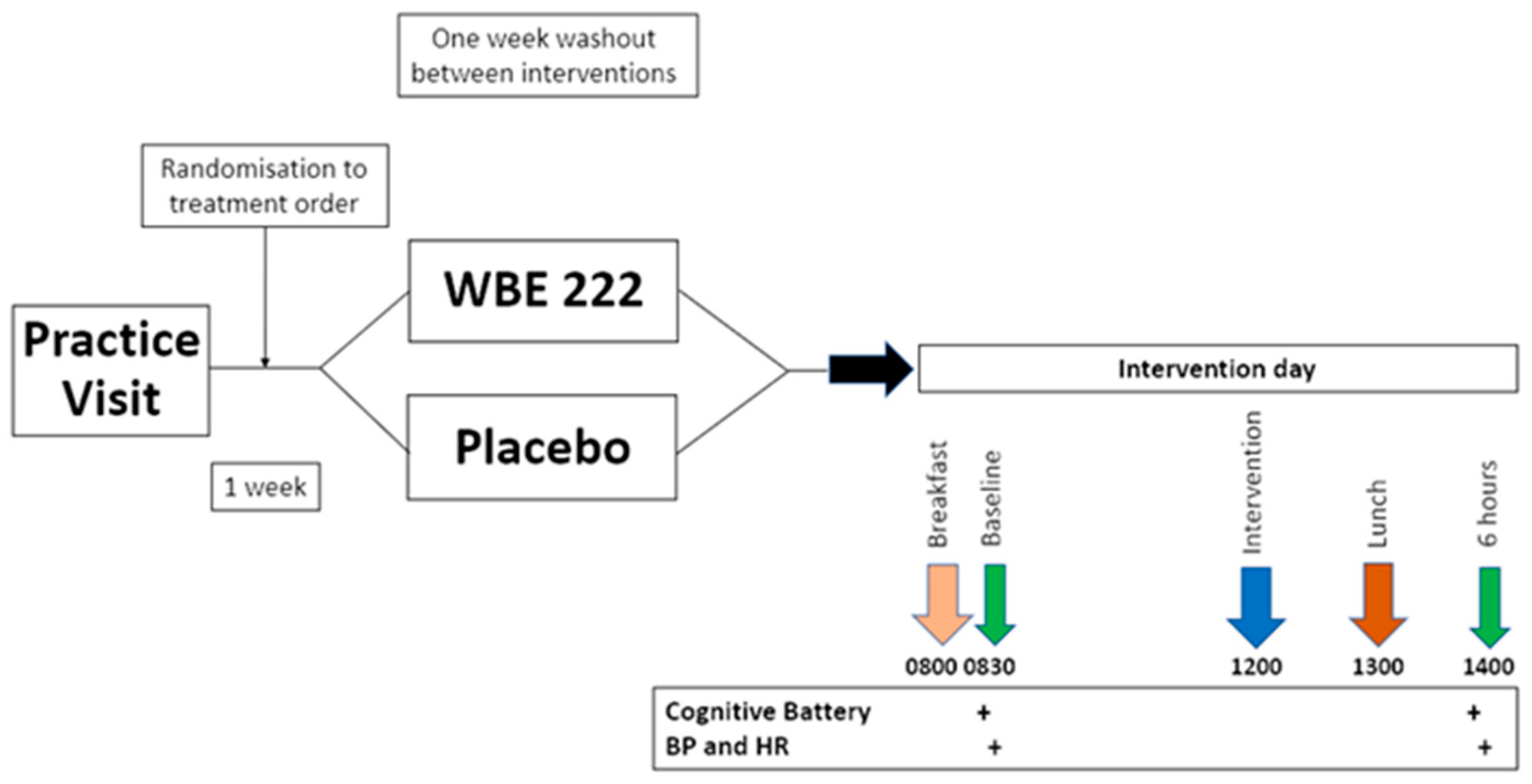
2.3.2. Design
2.3.3. Measures
2.3.4. Procedure
2.4. Analysis
3. Results
3.1. ROAB (Study 1) Results
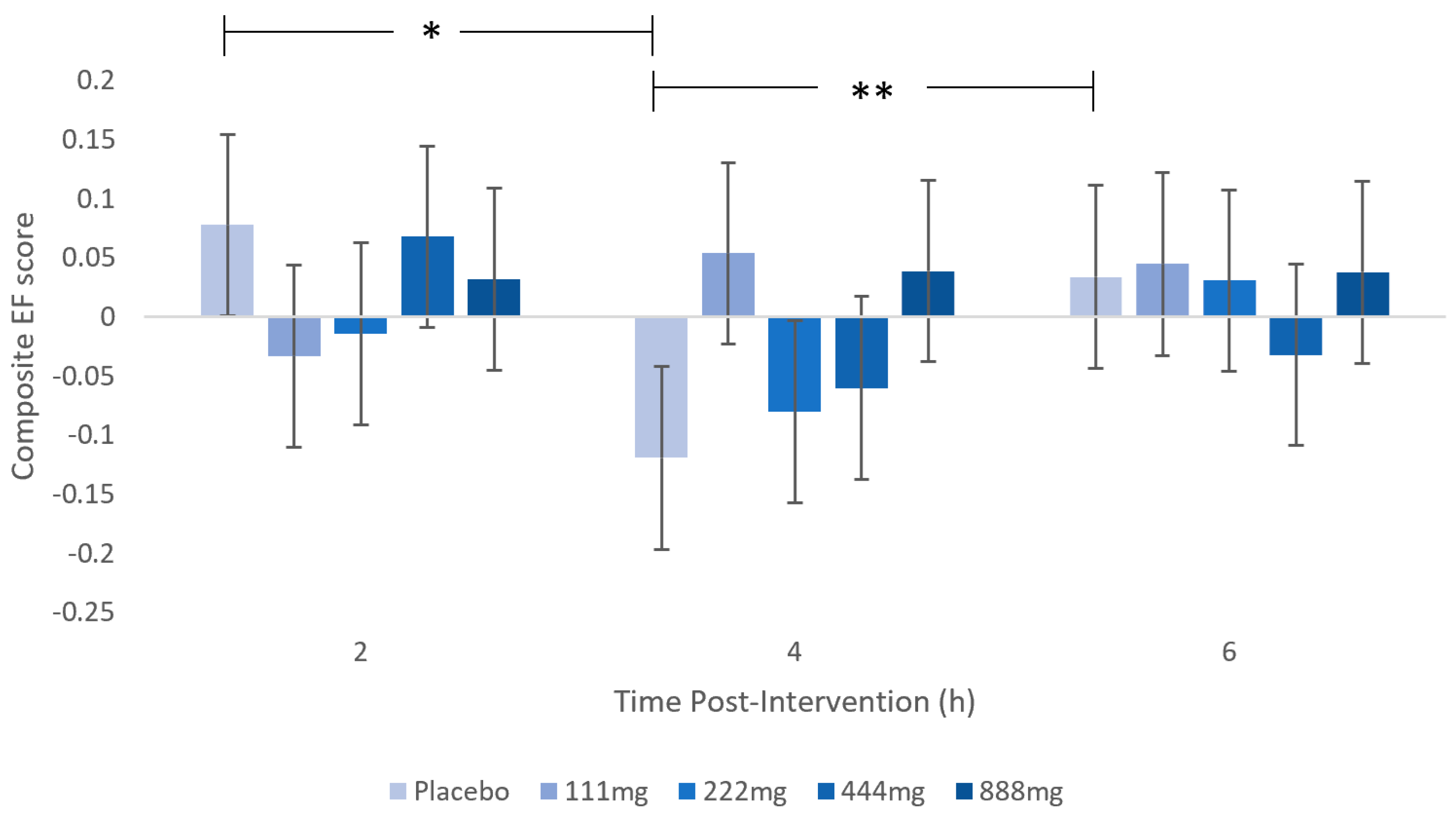
3.1.1. Executive Function Composite Measure
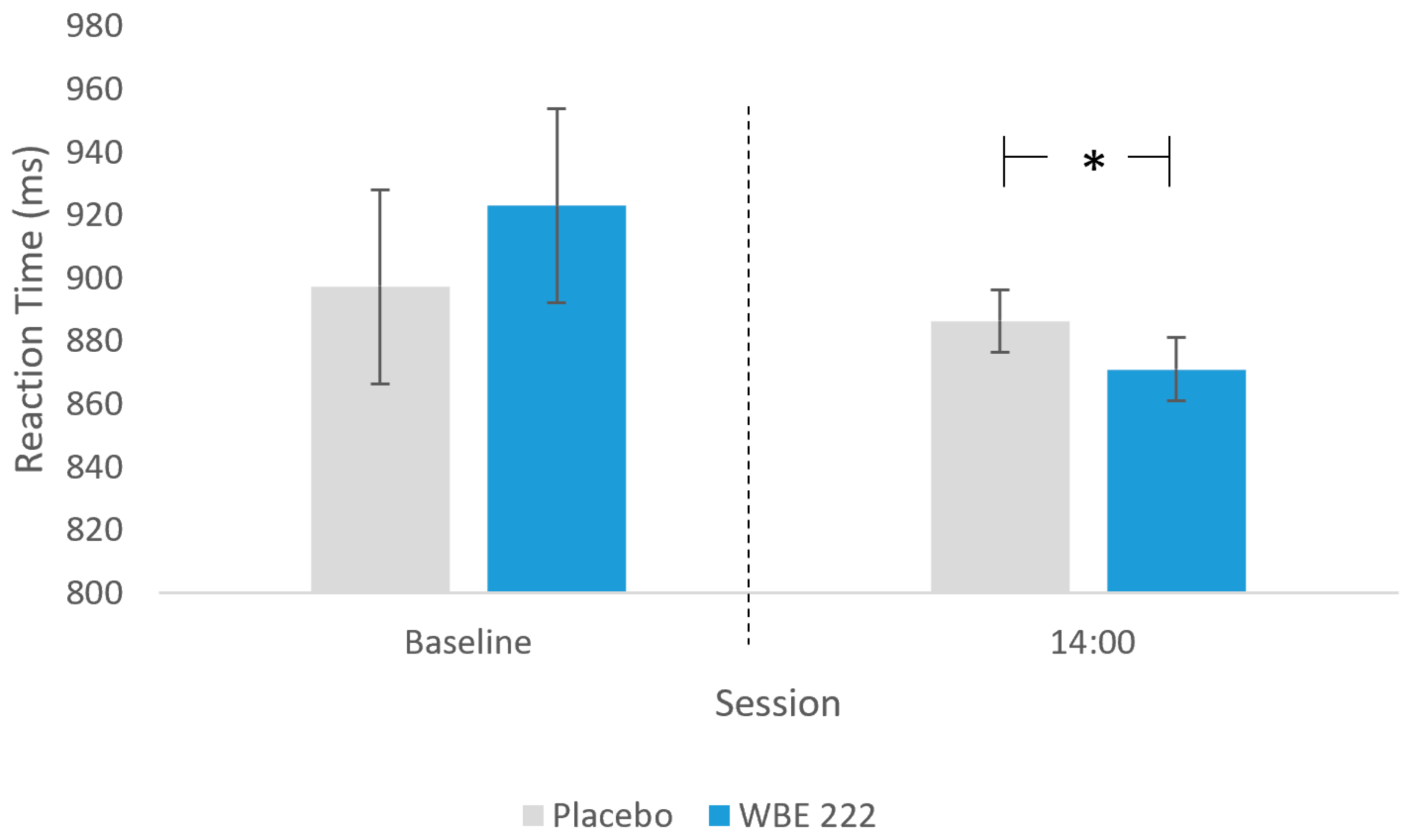
3.1.2. Task Switch Task (TST)
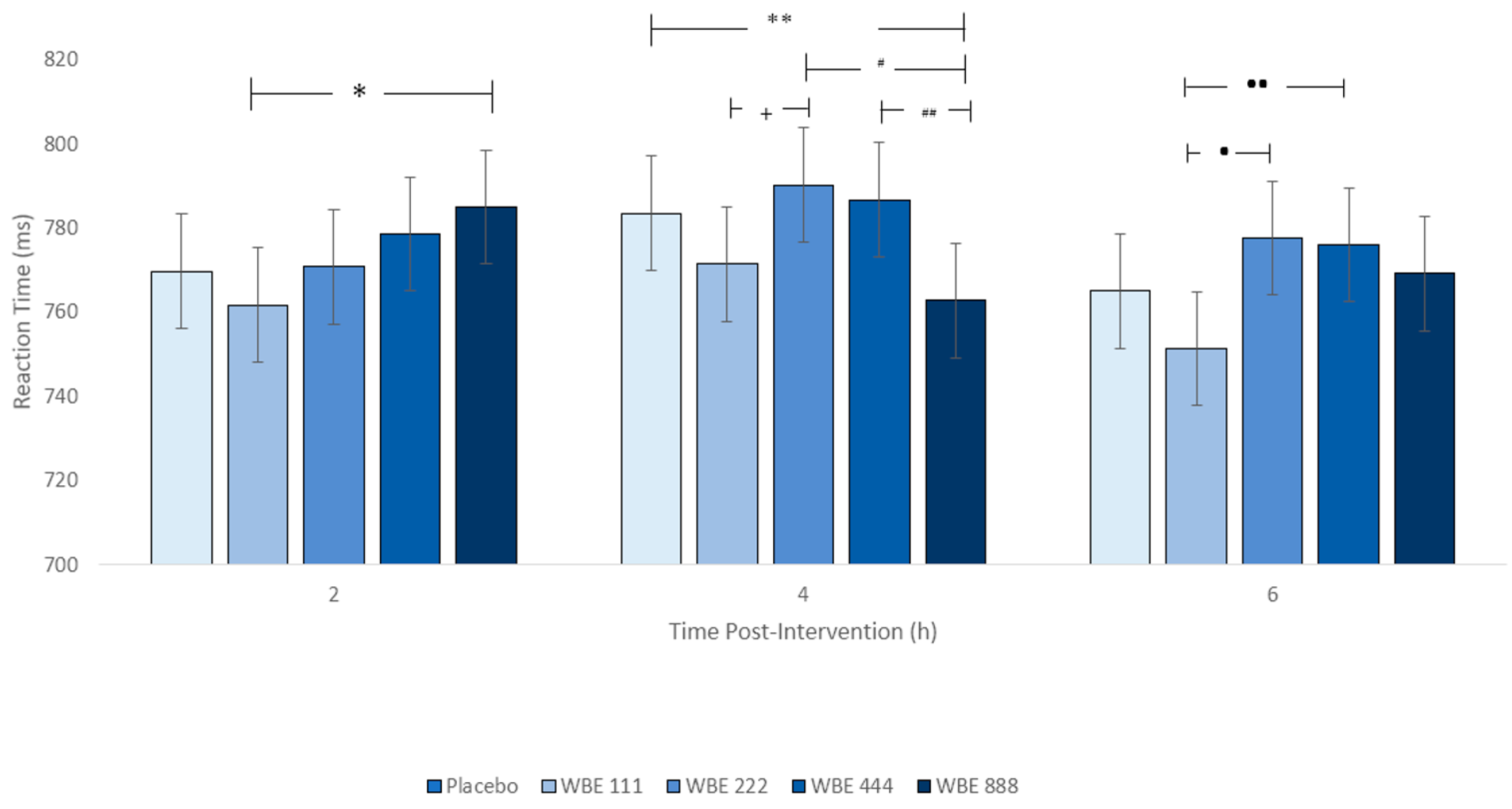
3.1.3. Choice Reaction Time (CRT)
3.1.4. RAVLT
3.1.5. TMT A and B, EM Composite, Corsi Blocks Task, and the Global Composite
3.1.6. Mood—Positive (PA) and Negative Affect (NA)
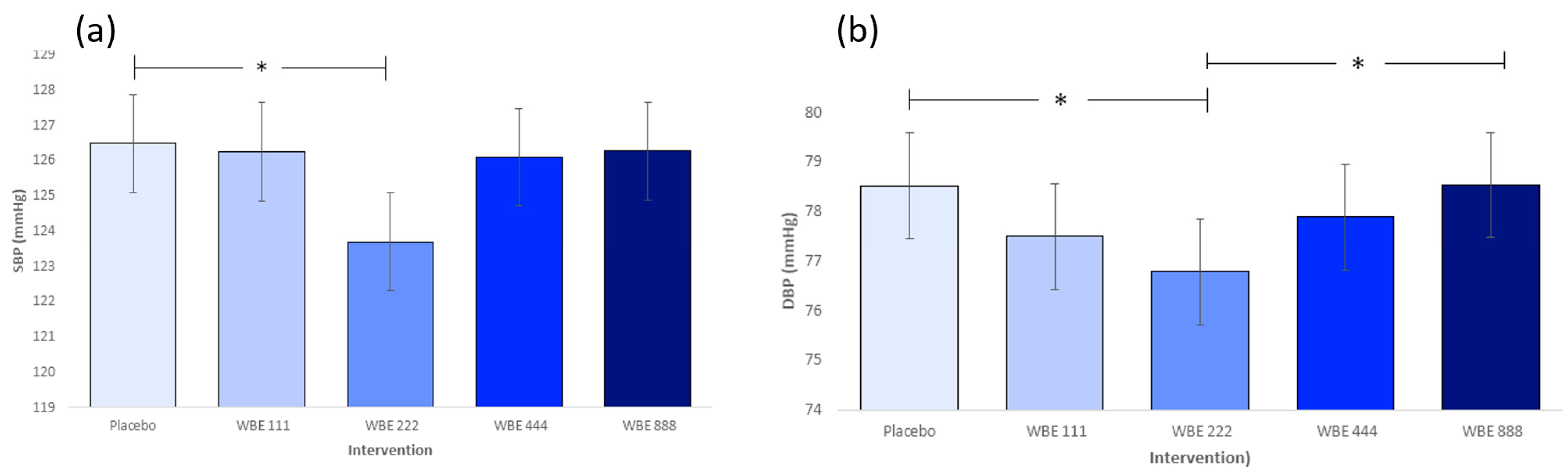
3.1.7. Blood Pressure and Heart Rate
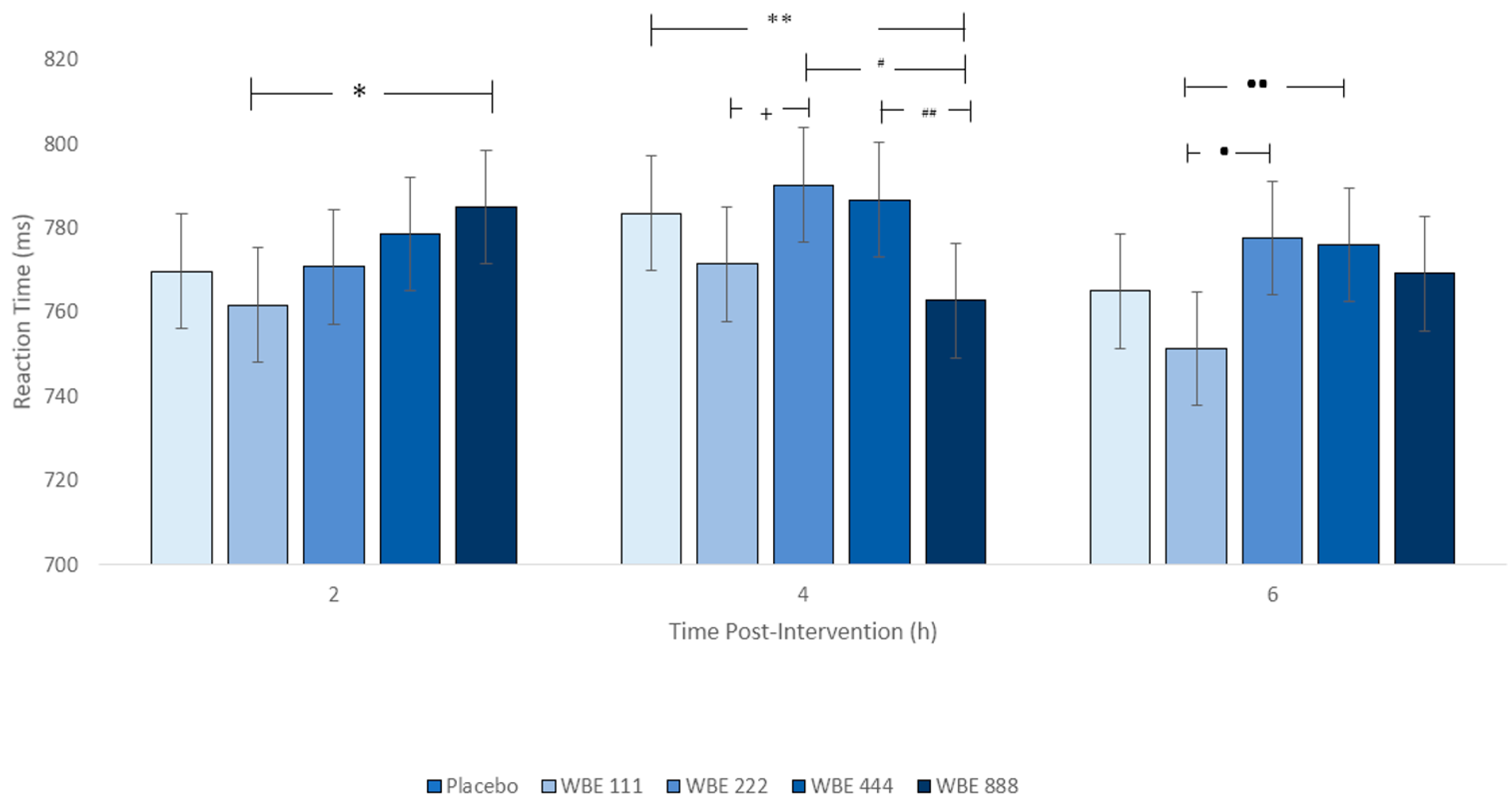
3.2. BEAT (Study 2) Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamport, D.J.; Pal, D.; Macready, A.L.; Barbosa-Boucas, S.; Fletcher, J.M.; Williams, C.M.; Spencer, J.P.; Butler, L.T. The effects of flavanone-rich citrus juice on cognitive function and cerebral blood flow: An acute, randomised, placebo-controlled cross-over trial in healthy, young adults. Br. J. Nutr. 2016, 116, 2160–2168. [Google Scholar] [CrossRef]
- Jackson, P.A.; Wightman, E.L.; Veasey, R.; Forster, J.; Khan, J.; Saunders, C.; Mitchell, S.; Haskell-Ramsay, C.F.; Kennedy, D.O. A Randomized, Crossover Study of the Acute Cognitive and Cerebral Blood Flow Effects of Phenolic, Nitrate and Botanical Beverages in Young, Healthy Humans. Nutrients 2020, 12, 2254. [Google Scholar] [CrossRef]
- Francis, S.T.; Head, K.; Morris, P.G.; Macdonald, I.A. The effect of flavanol-rich cocoa on the fMRI response to a cognitive task in healthy young people. J. Cardiovasc. Pharmacol. 2006, 47 (Suppl. 2), S215–S220. [Google Scholar] [CrossRef]
- Brickman, A.M.; Khan, U.A.; Provenzano, F.A.; Yeung, L.K.; Suzuki, W.; Schroeter, H.; Wall, M.; Sloan, R.P.; Small, S.A. Enhancing dentate gyrus function with dietary flavanols improves cognition in older adults. Nat. Neurosci. 2014, 17, 1798–1803. [Google Scholar] [CrossRef] [PubMed]
- Bell, L.; Williams, C.M. Blueberry benefits to cognitive function across the lifespan. Int. J. Food Sci. Nutr. 2021, 72, 650–652. [Google Scholar] [CrossRef]
- Lamport, D.J.; Williams, C.M. Polyphenols and cognition in humans: An overview of current evidence from recent systematic reviews and meta-analyses. Brain Plast. 2020, 6, 139–153. [Google Scholar] [CrossRef] [PubMed]
- Travica, N.; D’Cunha, N.M.; Naumovski, N.; Kent, K.; Mellor, D.D.; Firth, J.; Jacka, F. The effect of blueberry interventions on cognitive performance and mood: A systematic review of randomized controlled trials. Brain Behav. Immun. 2020, 85, 96–105. [Google Scholar] [CrossRef]
- Hein, S.; Whyte, A.R.; Wood, E.; Rodriguez-Mateos, A.; Williams, C.M. Systematic review of the effects of blueberry on cognitive performance as we age. J. Gerontol. Ser. A 2019, 74, 984–995. [Google Scholar] [CrossRef]
- Wang, Y.; Haskell-Ramsay, C.; Gallegos, J.L.; Lodge, J.K. Effects of chronic consumption of specific fruit (berries, cherries and citrus) on cognitive health: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Clin. Nutr. 2023, 77, 7–22. [Google Scholar] [CrossRef]
- Whyte, A.R.; Cheng, N.; Fromentin, E.; Williams, C.M. A Randomized, Double-Blinded, Placebo-Controlled Study to Compare the Safety and Efficacy of Low Dose Enhanced Wild Blueberry Powder and Wild Blueberry Extract (ThinkBlue™) in Maintenance of Episodic and Working Memory in Older Adults. Nutrients 2018, 10, 660. [Google Scholar] [CrossRef]
- Stebbins, N.B.; Howard, L.R.; Prior, R.L.; Brownmiller, C.; Mauromoustakos, A. Stabilization of anthocyanins in blackberry juice by glutathione fortification. Food Funct. 2017, 8, 3459–3468. [Google Scholar] [CrossRef]
- Cortez, R.; Luna-Vital, D.A.; Margulis, D.; Gonzalez de Mejia, E. Natural pigments: Stabilization methods of anthocyanins for food applications. Compr. Rev. Food Sci. Food Saf. 2017, 16, 180–198. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Mateos, A.; Rendeiro, C.; Bergillos-Meca, T.; Tabatabaee, S.; George, T.W.; Heiss, C.; Spencer, J.P. Intake and time dependence of blueberry flavonoid–induced improvements in vascular function: A randomized, controlled, double-blind, crossover intervention study with mechanistic insights into biological activity. Am. J. Clin. Nutr. 2013, 98, 1179–1191. [Google Scholar] [CrossRef]
- Dodd, G.F.; Williams, C.M.; Butler, L.T.; Spencer, J.P. Acute effects of flavonoid-rich blueberry on cognitive and vascular function in healthy older adults. Nutr. Healthy Aging 2019, 5, 119–132. [Google Scholar] [CrossRef]
- Whyte, A.R.; Williams, C.M. Effects of a single dose of a flavonoid-rich blueberry drink on memory in 8 to 10 y old children. Nutrition 2015, 31, 531–534. [Google Scholar] [CrossRef] [PubMed]
- Whyte, A.R.; Schafer, G.; Williams, C.M. Cognitive effects following acute wild blueberry supplementation in 7-to 10-year-old children. Eur. J. Nutr. 2016, 55, 2151–2162. [Google Scholar] [CrossRef] [PubMed]
- Whyte, A.R.; Schafer, G.; Williams, C.M. The effect of cognitive demand on performance of an executive function task following wild blueberry supplementation in 7 to 10 years old children. Food Funct. 2017, 8, 4129–4138. [Google Scholar] [CrossRef] [PubMed]
- Barfoot, K.L.; May, G.; Lamport, D.J.; Ricketts, J.; Riddell, P.M.; Williams, C.M. The effects of acute wild blueberry supplementation on the cognition of 7-10-year-old schoolchildren. Eur. J. Nutr. 2019, 58, 2911–2920. [Google Scholar] [CrossRef] [PubMed]
- Whyte, A.R.; Rahman, S.; Bell, L.; Edirisinghe, I.; Krikorian, R.; Williams, C.M.; Burton-Freeman, B. Improved metabolic function and cognitive performance in middle-aged adults following a single dose of wild blueberry. Eur. J. Nutr. 2021, 60, 1521–1536. [Google Scholar] [CrossRef]
- Valdez, P.; Ramírez, C.; García, A. Circadian rhythms in cognitive performance: Implications for neuropsychological assessment. Chronophysiol. Ther. 2012, 2, 81–92. [Google Scholar] [CrossRef]
- Ceglarek, A.; Hubalewska-Mazgaj, M.; Lewandowska, K.; Sikora-Wachowicz, B.; Marek, T.; Fafrowicz, M. Time-of-day effects on objective and subjective short-term memory task performance. Chronobiol. Int. 2021, 38, 1330–1343. [Google Scholar] [CrossRef] [PubMed]
- Monk, T.H. Aging human circadian rhythms: Conventional wisdom may not always be right. J. Biol. Rhythm. 2005, 20, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Valdez, P. Focus: Attention science: Circadian rhythms in attention. Yale J. Biol. Med. 2019, 92, 81. [Google Scholar]
- Müller, K.; Libuda, L.; Terschlüsen, A.M.; Kersting, M. A review of the effects of lunch: On adults’ short-term cognitive functioning. Can. J. Diet. Pract. Res. 2013, 74, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.P. Sleep deprivation. lunch and selective attention. Eur. J. Pharm. Med. Res. 2021, 8, 156–159. [Google Scholar]
- Smith, A.P.; Miles, C. The effects of lunch on cognitive vigilance tasks. Ergonomics 1986, 29, 1251–1261. [Google Scholar] [CrossRef] [PubMed]
- Blatter, K.; Opwis, K.; Münch, M.; Wirz-Justice, A.; Cajochen, C. Sleep loss-related decrements in planning performance in healthy elderly depend on task difficulty. J. Sleep Res. 2005, 14, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Whyte, A.R.; Cheng, N.; Butler, L.T.; Lamport, D.J.; Williams, C.M. Flavonoid-Rich Mixed Berries Maintain and Improve Cognitive Function Over a 6 h Period in Young Healthy Adults. Nutrients 2019, 11, 2685. [Google Scholar] [CrossRef] [PubMed]
- Barfoot, K.L.; Istas, G.; Feliciano, R.P.; Lamport, D.J.; Riddell, P.; Rodriguez-Mateos, A.; Williams, C.M. Effects of daily consumption of wild blueberry on cognition and urinary metabolites in school-aged children: A pilot study. Eur. J. Nutr. 2021, 60, 4263–4278. [Google Scholar] [CrossRef]
- Cheng, N.; Bell, L.; Lamport, D.J.; Williams, C.M. Dietary flavonoids and human cognition: A meta-analysis. Mol. Nutr. Food Res. 2022, 66, 2100976. [Google Scholar] [CrossRef]
- Miller, M.G.; Hamilton, D.A.; Joseph, J.A.; Shukitt-Hale, B. Dietary blueberry improves cognition among older adults in a randomized, double-blind, placebo-controlled trial. Eur. J. Nutr. 2018, 57, 1169–1180. [Google Scholar] [CrossRef] [PubMed]
- Haahr, M. RANDOM.ORG: True Random Number Service. Available online: https://www.random.org (accessed on 18 May 2023).
- Kupina, S.; Fields, C.; Roman, M.C.; Brunelle, S.L. Determination of Total Phenolic Content Using the Folin-C Assay: Single-Laboratory Validation, First Action 2017.13. J. AOAC Int. 2018, 101, 1466–1472. [Google Scholar] [CrossRef] [PubMed]
- Cassinese, C.; Combarieu, E.D.; Falzoni, M.; Fuzzati, N.; Pace, R.; Sardone, N. New liquid chromatography method with ultraviolet detection for analysis of anthocyanins and anthocyanidins in Vaccinium myrtillus fruit dry extracts and commercial preparations. J. AOAC Int. 2007, 90, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.E.; Willison, J. National Adult Reading Test (NART): Nfer-Nelson; NFER-NELSON Publishing Company Ltd.: Windsor, UK, 1991. [Google Scholar]
- Zelinski, E.M.; Gilewski, M.J. A 10-item Rasch modeled memory self-efficacy scale. Aging Ment. Health 2004, 8, 293–306. [Google Scholar] [CrossRef]
- Raven, J.; Raven, J.C.; Court, J.H. Raven Manual: Section 4, Advanced Progressive Matrices, 1998th ed.; Oxford Psychologists Press Ltd.: Oxford, UK, 1998. [Google Scholar]
- Dipietro, L.; Caspersen, C.J.; Ostfeld, A.M.; Nadel, E.R. A survey for assessing physical activity among older adults. Med. Sci. Sports Exerc. 1993, 25, 628–642. [Google Scholar] [CrossRef] [PubMed]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W.; Fischer, J.S. Neuropsychological Assessment; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Berch, D.B.; Krikorian, R.; Huha, E.M. The Corsi block-tapping task: Methodological and theoretical considerations. Brain Cogn. 1998, 38, 317–338. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063. [Google Scholar] [CrossRef]
- Bell, L.; Lamport, D.J.; Field, D.T.; Butler, L.T.; Williams, C.M. Practice effects in nutrition intervention studies with repeated cognitive testing. Nutr. Healthy Aging 2018, 4, 309–322. [Google Scholar] [CrossRef]
- Andrade, C. Z scores, standard scores, and composite test scores explained. Indian J. Psychol. Med. 2021, 43, 555–557. [Google Scholar] [CrossRef]
- Wang, J.; Logovinsky, V.; Hendrix, S.B.; Stanworth, S.H.; Perdomo, C.; Xu, L.; Dhadda, S.; Do, I.; Rabe, M.; Luthman, J.; et al. ADCOMS: A composite clinical outcome for prodromal Alzheimer’s disease trials. J. Neurol. Neurosurg. Psychiatry 2016, 87, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.Y.; Snyder, P.J.; Pietrzak, R.H.; Ukiqi, A.; Villemagne, V.L.; Ames, D.; Salvado, O.; Bourgeat, P.; Martins, R.N.; Masters, C.L.; et al. Sensitivity of composite scores to amyloid burden in preclinical Alzheimer’s disease: Introducing the Z-scores of Attention, Verbal fluency, and Episodic memory for Nondemented older adults composite score. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2016, 2, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Donohue, M.C.; Sperling, R.A.; Salmon, D.P.; Rentz, D.M.; Raman, R.; Thomas, R.G.; Weiner, M.; Aisen, P.S. The preclinical Alzheimer cognitive composite: Measuring amyloid-related decline. JAMA Neurol. 2014, 71, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2013; Volume 6, pp. 497–516. [Google Scholar]
- Senn, S. Change from baseline and analysis of covariance revisited. Statist. Med. 2006, 25, 4334–4344. [Google Scholar] [CrossRef]
- Kıskaç, M.; Soysal, P.; Smith, L.; Capar, E.; Zorlu, M. What is the Optimal Body Mass Index Range for Older Adults? Ann. Geriatr. Med. Res. 2022, 26, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Schuler, P.B.; Richardson, M.T.; Ochoa, P.; Wang, M.Q. Accuracy and repeatability of the Yale physical activity survey in assessing physical activity of older adults. Percept. Mot. Ski. 2001, 93, 163–177. [Google Scholar] [CrossRef] [PubMed]
- Steffen, Y.; Gruber, C.; Schewe, T.; Sies, H. Mono-O-methylated flavanols and other flavonoids as inhibitors of endothelial NADPH oxidase. Arch. Biochem. Biophys. 2008, 469, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Nehlig, A. The neuroprotective effects of cocoa flavanol and its influence on cognitive performance. Br. J. Clin. Pharmacol. 2013, 75, 716–727. [Google Scholar] [CrossRef] [PubMed]
- Monahan, K.D.; Feehan, R.P.; Kunselman, A.R.; Preston, A.G.; Miller, D.L.; Lott, M.E. Dose-dependent increases in flow-mediated dilation following acute cocoa ingestion in healthy older adults. J. Appl. Physiol. 2011, 111, 1568–1574. [Google Scholar] [CrossRef]
- Njike, V.Y.; Faridi, Z.; Shuval, K.; Dutta, S.; Kay, C.D.; West, S.G.; Katz, D.L. Effects of sugar-sweetened and sugar-free cocoa on endothelial function in overweight adults. Int. J. Cardiol. 2011, 149, 83–88. [Google Scholar] [CrossRef]
- Akazawa, N.; Kumagai, H.; Yoshikawa, T.; Myoenzono, K.; Tanahashi, K.; Maeda, S. Cerebral blood flow velocity is associated with endothelial function in men. J. Men’s Health 2021, 17, 41–46. [Google Scholar]
- Rees, A.; Dodd, G.F.; Spencer, J.P. The effects of flavonoids on cardiovascular health: A review of human intervention trials and implications for cerebrovascular function. Nutrients 2018, 10, 1852. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Intervention Formulation |
|---|---|
| Placebo | Inert artificially coloured maltodextrin (300 mg), once daily, 3-hard-capsule regimen |
| WBE 111 | 100 mg WBE + 11 mg L-cysteine + 1 mg L-glutathione, once daily, 3-hard-capsule regimen |
| WBE 222 | 200 mg WBE + 22 mg L-cysteine + 2 mg L-glutathione, once daily, 3-hard-capsule regimen |
| WBE 444 | 400 mg WBE + 44 mg L-cysteine + 4 mg L-glutathione, once daily, 3-hard-capsule regimen |
| WBE 888 | 800 mg WBE + 88 mg L-cysteine + 8 mg L-glutathione, once daily, 3-hard-capsule regimen |
| Composite Score | ROAB Cognitive Measures | BEAT Cognitive Measures |
|---|---|---|
| Global | All test measures | All test measures |
| Episodic memory | Corsi longest sequence remembered, Corsi total number of correct sequences remembered, Corsi latency, RAVLT word recognition accuracy, RAVLT delayed word recall accuracy, foil words rejected, RAVLT words learned, RAVLT total recall, and RAVLT PI, RAVLT RI, and RAVLT word recognition reaction time | Corsi longest sequence remembered, Corsi total number of correct sequences remembered, Corsi latency, RAVLT word recognition accuracy, RAVLT delayed word recall accuracy, RAVLT total recall, and RAVLT PI, RAVLT RI, and RAVLT word recognition reaction time |
| Executive function | CRT accuracy, Switching task accuracy, and TMT B-A, TMT A, TMT- B, CRT, and TST reaction time | Switching task accuracy and Switching task reaction time |
| Baseline Characteristics | ROAB (n = 28) | BEAT (n = 45) | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Age at enrolment (years) | 70.71 | 2.14 | 71.02 | 2.03 |
| Gender (M:F) | 11:17 | - | 18:27 | - |
| BMI (kg/m2) | 24.51 | 3.30 | 25.05 | 2.95 |
| MMSE (/30) | 27.9 | 1.58 | 28.53 | 1.38 |
| NART (number of errors/50) | 9 | 5.11 | 8.04 | 4.44 |
| Frequency of Forgetting 1 | 5.01 | 0.75 | 5.27 | 0.98 |
| Frequency of Forgetting 2 | 5.22 | 1.10 | 5.36 | 1.19 |
| Raven’s Progressive Matrices | 50.21 | 5.86 | 48.98 | 7.03 |
| Yale expenditure (kcal/week) | 5519 | 3798.36 | 6050 | 2384.61 |
| Energy consumption (kcal/day) | 1772 | 632.85 | 1904 | 778.82 |
| Fruit consumption (g/day) | 291 | 172.61 | 339 | 241.25 |
| Vegetable consumption (g/day) | 299 | 179.15 | 339 | 136.41 |
| Measure | Intervention | Timepoint | p-Value 2 h Comparison | |
|---|---|---|---|---|
| Baseline (Covariate) | 2 h | |||
| Executive Function Composite | Placebo | 0.30 (0.09) | −0.010 (0.04) | |
| WBB 222 | −0.46 (0.09) | 0.003 (0.04) | 0.52 | |
| Task Switch Task Accuracy | Placebo | 0.97 (0.006) | 0.97 (0.003) | |
| WBB 222 | 0.97 (0.006) | 0.97 (0.003) | 0.16 | |
| Task Switch Task RT (ms) | Placebo | 897 (31) | 886 (10) | |
| WBB 222 | 923 (31) | 871 (10) | 0.01 * | |
| Episodic Memory Composite | Placebo | −0.31 (0.08) | 0.011 (0.03) | |
| WBB 222 | 0.18 (0.08) | −0.01 (0.03) | 0.53 | |
| Word Recognition Accuracy | Placebo | 0.85 (0.02) | 0.80 (0.02) | |
| WBB 222 | 0.88 (0.02) | 0.80 (0.02) | 0.99 | |
| Word Recognition RT (ms) | Placebo | 1215 (51) | 1235 (39) | |
| WBB 222 | 1201 (51) | 1206 (39) | 0.52 | |
| Delayed Word Recall | Placebo | 8.79 (0.55) | 6.51 (0.40) | |
| WBB 222 | 9.22 (0.54) | 6.55 (0.40) | 0.94 | |
| Total Recall | Placebo | 49.82 (1.44) | 46.31 (0.99) | |
| WBB 222 | 50.63 (1.45) | 45.42 (0.99) | 0.53 | |
| Proactive Interference | Placebo | 0.94 (0.05) | 1.03 (0.05) | |
| WBB 222 | 0.95 (0.05) | 1.01 (0.05) | 0.74 | |
| Retroactive Interference | Placebo | 2.38 (0.30) | 3.02 (0.26) | |
| WBB 222 | 2.36 (0.32) | 2.91 (0.34) | 0.7 | |
| Immediate Recall | Placebo | 6.84 (0.25) | 5.80 (0.21) | |
| WBB 222 | 6.65 (0.25) | 5.96 (0.21) | 0.49 | |
| Corsi Longest Sequence | Placebo | 7.35 (0.22) | 7.39 (0.19) | |
| WBB 222 | 6.98 (0.22) | 7.35 (0.19) | 0.85 | |
| Corsi Total Correct Sequences | Placebo | 0.52 (0.02) | 0.54 (0.02) | |
| WBB 222 | 0.53 (0.02) | 0.51 (0.02) | 0.03 * | |
| Corsi Latency | Placebo | 1017 (30) | 1013 (21) | |
| WBB 222 | 1014 (30) | 1023 (21) | 0.72 | |
| Systolic BP (mm/Hg) | Placebo | 123.00 (2.40) | 124.54 (1.34) | |
| WBB 222 | 123.47 (2.40) | 124.18 (1.35) | 0.81 | |
| Diastolic BP (mm/Hg) | Placebo | 79.41 (4.43) | 75.49 (0.95) | |
| WBB 222 | 77.30 (4.42) | 75.47 (0.95) | 0.98 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, N.; Barfoot, K.L.; Le Cozannet, R.; Fança-Berthon, P.; Lamport, D.J.; Williams, C.M. Wild Blueberry Extract Intervention in Healthy Older Adults: A Multi-Study, Randomised, Controlled Investigation of Acute Cognitive and Cardiovascular Effects. Nutrients 2024, 16, 1180. https://doi.org/10.3390/nu16081180
Cheng N, Barfoot KL, Le Cozannet R, Fança-Berthon P, Lamport DJ, Williams CM. Wild Blueberry Extract Intervention in Healthy Older Adults: A Multi-Study, Randomised, Controlled Investigation of Acute Cognitive and Cardiovascular Effects. Nutrients. 2024; 16(8):1180. https://doi.org/10.3390/nu16081180
Chicago/Turabian StyleCheng, Nancy, Katie L. Barfoot, Romain Le Cozannet, Pascale Fança-Berthon, Daniel J. Lamport, and Claire M. Williams. 2024. "Wild Blueberry Extract Intervention in Healthy Older Adults: A Multi-Study, Randomised, Controlled Investigation of Acute Cognitive and Cardiovascular Effects" Nutrients 16, no. 8: 1180. https://doi.org/10.3390/nu16081180
APA StyleCheng, N., Barfoot, K. L., Le Cozannet, R., Fança-Berthon, P., Lamport, D. J., & Williams, C. M. (2024). Wild Blueberry Extract Intervention in Healthy Older Adults: A Multi-Study, Randomised, Controlled Investigation of Acute Cognitive and Cardiovascular Effects. Nutrients, 16(8), 1180. https://doi.org/10.3390/nu16081180