Abstract
Introduction Emerging evidence suggests an association between obesity and Functional Gastrointestinal Disorders (FGIDs). Childhood obesity and FGIDs share many common features, such as high prevalence in the pediatric population, risk factors related to diet and lifestyle, gut microbiota impairments, and psychological distress. This narrative review aims to summarize the main evidence regarding FGIDs in childhood obesity, with a specific focus on the role of diet and its impact on the microbiota. Additionally, the review highlights potential common-ground solutions for preventing and managing both obesity and FGIDs. Methods A comprehensive PubMed search was conducted. Keywords used included terms related to children and adolescents, obesity, functional gastrointestinal disorders, and microbiota. Results The review emphasizes the importance of holistic, multidisciplinary approaches to managing symptoms. In addition to nutrition education, physical activity, and medical care, complementary strategies such as psychological interventions and personalized dietary modifications (e.g., low-FODMAP and fiber-enriched diets) are critical. Given the interplay between gut microbiota alterations, obesity, and FGIDs, microbiota modulation through probiotics, prebiotics, and integrative support shows significant promise. However, the variability in current evidence underlines the need for robust longitudinal studies to develop standardized protocols and maximize treatment efficacy. Conclusions Bridging gaps in knowledge and practice with an integrated, evidence-based framework could improve patient outcomes and deepen understanding of the complex relationship between metabolic and gastrointestinal health in children and adolescents.
1. Introduction
Functional Gastrointestinal Disorders (FGIDs) encompass a range of chronic gastrointestinal symptoms, often accompanied by pain, with no identifiable medical condition. Functional bowel disorders are a type of functional gastrointestinal disorders including conditions characterized by symptoms originating from the middle or lower gastrointestinal tract [1]. Main Functional Bowel Disorders (FBDs) in children and adolescents are Irritable Bowel Syndrome (IBS) and Functional Dyspepsia (FD), (included among Functional Abdominal Pain Disorders by Rome IV criteria) and Functional Constipation (FC) (included among Functional Defecation Disorders by Rome IV criteria) [2].
Nowadays, well-defined epidemiological data about the prevalence of FGIDs in pediatric patients is still lacking. According to a systematic review, prevalence rates of FGIDs in children and adolescents could range from 9% to 29% [3]. Notably, IBS is one of the most widespread conditions among FGIDs. A meta-analysis reported that the pooled global prevalence of IBS reached 8.8% in children and adolescent aged 4–18 years [4]. Rather, the estimated prevalence of IBS in the European Mediterranean region is 4% in the same population [5]. Regarding FC, a study reported a pooled global prevalence in children equal to 14.4%, specifically in Europe at 8.3% [6]. Instead, the prevalence of FD in children is estimated to range from 3% to 27%, and it poses a significant economic burden on healthcare systems. Children with FD who show partial or no response to treatment often incur higher medical costs, further contributing to healthcare expenditures [7]. FGIDs in children imply relevant healthcare costs and loss of economic productivity for parents or caregivers [8,9]. For example, globally, FC accounts for 25% of pediatric gastroenterologist consultations and 3% of all general pediatric visits [6].
IBS diagnosis is symptoms-based. The main symptom is abdominal pain, which can be related to defecation or/and diarrhea, constipation, or both conditions [2]. It has been hypothesized that IBS may arise from disruption of the brain-gut axis. There is an ongoing debate about whether the primary dysfunction onsets in the gut (e.g., accumulation of inflammatory cells in the intestinal mucosa) or in the central nervous system (e.g., increased release of corticotrophin releasing factor, CRF) [10]. The disruption of the brain-gut axis leads to different pathophysiological changes, such as visceral hypersensitivity, gastrointestinal dysmotility, increased gut permeability, and intestinal low-grade inflammation with the involvement of microbiota [10,11]. A child’s psychological distress can be associated with IBS [2,11]. Indeed, risk factors for IBS include excess worry, anxiety, and depression, but also gastrointestinal infections and diet (e.g., important assumption of spicy or fried food) [10].
Patients affected by FD complain one or more of the following bothersome symptoms, such as postprandial fullness, early satiation, and epigastric pain or burning not in concomitance with defecation, at least four days per month [2]. Different pathophysiological pathways are hypothesized as responsible for FD development such as motor abnormalities (e.g., delayed gastric emptying or antral hypomotility), visceral hypersensitivity to gastric distension, genetic predisposition, low-grade inflammation and psychosocial factors (e.g., anxiety) [2,12].
FC is a disorder characterized by infrequent defecations associated with painful and hard bowel movements, retentive behavior, presence of a large fecal mass in the rectum or large diameter stools able to clog the toilet, or episodes of overflow fecal incontinence [2]. Pathophysiological mechanisms are multifactorial and include stool withholding, dietary habits, physical activity, and anorectal dysfunctions [6]. A child’s avoiding defecation instinct because of pain or social reasons is the most important trigger of the disorder [2].
According to WHO, in 2022, 160 million children and adolescents aged 5–19 years were living with obesity worldwide [13]. Currently, childhood obesity is a global health issue, exhibiting characteristics of a pandemic. Furthermore, causes of childhood obesity can include individual determinants, as well as social and environmental factors. Indeed, the “obesogenic environment” plays an important role in the development and perpetuation of obesity among children and adolescents. Specifically, two of the main drivers of childhood obesity are a dietary pattern characterized by energy dense nutrient poor foods and a sedentary lifestyle [14]. Obesity in children and adolescents aged 4–18 years is a significant public health issue, as it increases the risk of cardiometabolic and psychosocial comorbidities during childhood and adolescence, and is associated with premature mortality in adulthood [14].
Moreover, emerging evidence suggests an association between obesity and FGIDs [15,16]. Childhood obesity and FGIDs share many similar features such as high incidence in the children population, risk factors related to diet and lifestyle, gut microbiota impairment, and psychological distress. Studies addressing this issue are heterogeneous, especially in terms of FGIDs diagnostic criteria considered and cohorts analyzed [17].
Our review aims to summarize the main evidence regarding FGIDs in childhood obesity, with a specific focus on the role of diet and its impact on microbiota. Additionally, this review could contribute to pointing out common-grounded solutions for preventing and treating both obesity and FGIDs.
2. Methods
This is a narrative review to explore the association between childhood obesity and FBDs. To accomplish this, a comprehensive search of the PubMed database was conducted, focusing on English-language articles published over the past 25 years.
The review included a variety of publication types, such as original research studies, systematic and narrative reviews, meta-analysesand longitudinal studies, while excluding case reports, case series, letters, and commentaries. Relevant studies exploring specific interventions, including probiotics, prebiotics, and dietary modifications, were included if they contributed to understanding pediatric FBDs and obesity.
The search strategy employed specific keywords, both individually and in combination, including: child OR children OR childhood OR adolescent AND obesity OR obese OR overweight AND functional gastrointestinal disorder* OR functional gastrointestinal disease* OR constipation OR functional constipation OR dyspepsia OR abdominal pain OR functional bowel disorder* OR functional bowel disease* AND biotic OR probiotic* OR prebiotic* OR synbiotic OR fiber AND microbiota OR gut microbiota.
Articles were initially screened based on titles (n = 3275) and abstracts (n = 2432), and those deemed relevant were subjected to a full-text review for further evaluation (n = 130). Selected studies (n = 120) were critically assessed to ensure a comprehensive understanding of the topic. The draft of this review was collaboratively prepared, thoroughly reviewed, and approved by all co-authors to ensure the accuracy and depth of the final analysis.
The process for manuscript selection is summarized in Figure 1.
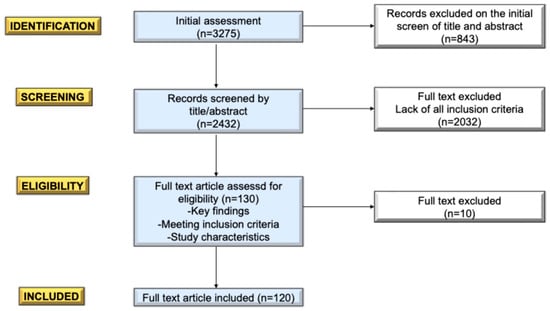
Figure 1.
Flowgram of the selection of the manuscripts.
3. Functional Bowel Disorders in Children with Obesity: State of the Problem
In the last twenty years, childhood obesity has reached epidemic proportions. In 2006, 16.6% of children and adolescents aged 2 to 19 had a weight at or above the 95th percentile for age. More than 7% of children and adolescents had obesity in 2016 compared with less than 1% in 1975 [18].
According to global health estimates provided by World Health Organization (WHO) 38.2 million of children under the age of 5 years present overweight or obesity in 2019 [13]. The rapidly increasing prevalence of obesity in children is the most important problem facing pediatricians today [19,20,21].
In addition to the well-known association with cardiovascular disease and diabetes, recent studies have reported an association between obesity and FGIDs [15,16]. Teitelbaum et al. [22] found a significantly higher prevalence of obesity in children with FGIDs compared to the control group; in a retrospective study evaluating the association with obesity in children and adolescents referred to a pediatric gastroenterologist, 23% of patients affected by FC were living with obesity, while 24.8% of patients with IBS were affected by obesity. The study also took into consideration recent evaluations regarding gastrointestinal motility disorders, delayed gastric emptying and alteration of the gastric antrum, or functional dyspepsia, were also found in children with Functional Abdominal Pain (FAP). The association between these disorders and overweight has been established through prior research [23]. Greater gastric distension in overweight children can lead to a reduction in the tone of the stomach muscle wall, altering the sensitivity of the mechanoreceptors and also causing an abnormal perception of satiety [24]. This retrospective study also highlighted a higher prevalence of overweight/obesity in females, who are more subdued to gastrointestinal motility disorders than males. It could be caused by the action of ovarian hormones or by gender differences in the microbiome, but it’s still being studied [25].
Galai et al. [26] in a retrospective study reported that adolescents with FAP had higher prevalence of overweight/obesity compared to controls (39.5% vs. 30%).
Tambucci et al. found a significantly higher prevalence of FGIDs in children and adolescents living with obesity or overweight rather than in normal-weight children [27]. The study enrolled 103 children and 115 controls, all patients were evaluated by an endocrinologist and a gastroenterologist and Rome III questionnaires were used for the diagnosis of functional gastric disorder. A statistically significant difference was noted between the two groups for functional constipation, functional dyspepsia, and irritable bowel syndrome, but no statistically significant difference was observed for FAP. Notably, the prevalence of FC and IBS was respectively 18.44% and 10.67% in children with overweight/obesity.
The study by Phatak et al. [28] found a higher prevalence of FBDs in children with obesity/overweight (16.1%) compared to normal weight subjects (6.9%). The study was performed on children between ages of 4 and 18 years from the Yale Pediatric Primary Care clinic, FBDs studied were FC, FAP and IBS. A total of 450 children were recruited and almost half of the children with obesity/overweight had at least one functional gastrointestinal disorder.
Regarding FC, an association between obesity and increased prevalence of constipation has been noted [29]. A retrospective study was performed in June 2004 on 719 children, between the ages of 4 and 18 years, with chronic functional constipation; the control group consisted of 930 children in a pediatric clinic. Prevalence of obesity was significantly higher in constipated children (22.4%) compared with control children (11.7%), especially in males. The higher prevalence of obesity may be a result of dietary factors, activity or hormonal influences and needs additional evaluation.
A review published in 2022 by Zia JK et al. [30] highlights how it is necessary to implement studies on the pediatric population to determine the risk factors of IBS and other functional disorders, however finding a statistically significant association between obesity and functional gastrointestinal disorders.
Therefore, there is certainly a link between overweight and functional gastrointestinal disorders, although the results on each of the individual disorders are still conflicting according to different studies. The heterogeneity in findings across FBD subtypes, such as the stronger association between obesity and constipation compared to IBS, may stem from differences in gut motility, dietary patterns, or hormonal influences. Future research should stratify pediatric populations by FBD subtype to clarify these dynamics [29,31].
As reported, not only can obesity increase the prevalence of FBDs, but it can also modify their outcome. In this regard we mention a prospective cohort study from 2011 [32], which included 188 children, of which 20% present obesity. The results of the study demonstrated a statistically significant difference between normal weight patients and patients with obesity regarding the frequency of abdominal pain, intensity and limitation to daily activities.
Although obesity is known to increase the risk of reflux esophagitis, pediatric data on the association between obesity and gastroesophageal reflux are less clear: Elitsur et al. [31] showed that, within a group of children with reflux, esophagitis was observed in 65% of normal weight cases, in 69% and 68% of children with overweight with obesity respectively, with no significant difference between these groups. Similarly, Patel et al. [33] did not find a significant difference in the prevalence of reflux esophagitis among normal weight patients (23.9%) and overweight (24.5%). On the contrary, in adults the difference between the normal weight and overweight groups was statistically significant.
The pathophysiology of FBDs remains uncertain, with multifactorial underlying mechanisms. Evidence suggests a relationship between the microbiome, obesity, and FBDs, which could be leveraged to improve these gastrointestinal disorders. Notably, improvements in eating habits appear to be closely linked with enhancements in the microbiome, leading to better BMI outcomes and relief from functional disorders [34,35]. Current research indicates that factors such as diet, exercise, stress, and medications significantly influence gut microbiota alterations. Exploring this relationship presents a promising therapeutic approach [36,37].
A diet high in fat is risky for many reasons, some studies have highlighted that it is even responsible for greater malignant tumor progression, through the destruction of the intestinal microbiota. Not only does overweight alter the intestinal microbiota, but at the same time the inflammatory alteration induced by a pathological microbiota alters hypothalamic gene expression, vagus nerve activity and angiogenesis, creating a vicious circle. Some recent studies have compared the intestinal microbiome of normal weight subjects with patients with obesity and have noted that biodiversity is greatly reduced in subjects, also reducing the ability to resist external infections and increasing inflammation and intestinal permeability [38,39,40].
The proper functioning of the intestinal barrier is essential to prevent bacterial infiltration. Many pathologies, including IBS and various functional intestinal disorders, are characterized by an altered, more permeable intestinal barrier, which increases bacterial translocation. Individuals with IBD have significantly higher intestinal permeability compared with healthy controls; that suggests that one of the mechanisms underlying disease pathogenesis in IBD is damage to the structural barrier of the GI tract. Individuals with IBD have elevated levels of circulating proinflammatory mediators and this systemic inflammation has been suggested to be due to MT because elevated serum levels of LPS, bacterial DNA and LBP can be detected [41,42,43,44,45,46,47,48].
As detailed in the following sections, in the pediatric field, combined strategies, such as diet, nutritional education, use of biotics and integrative support, serve as cornerstone approaches for achieving improved symptom management.
In Table 1 the main papers referred to state of the problem about FGIDs in children and adolescents with obesity are reported.

Table 1.
Summary of the papers referred to state of the problem about Functional Gastrointestinal Disorders (FGIDs) in children and adolescents with obesity.
4. Diet, Nutritional Education and Support
4.1. The Role of Diet in FBDs
Among pathogenic mechanisms involved in FBDs, aspects related to nutrition—such as diet type, eating behaviors, gastrointestinal tract function, motility, and intestinal inflammation—play a significant role [49,50]. Currently, the pathophysiology of FBDs remains uncertain, with underlying mechanisms that are multifactorial. Among these mechanisms, aspects related to nutrition—such as diet type, eating behaviors, gastrointestinal tract function, motility, and intestinal inflammation—play a significant role [49,50]. In addition to the conventional treatment options, specific dietary patterns have shown potential benefits. These include the low-FODMAP (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) diet, as well as diets that restrict fructose, lactose, or gluten [4,51,52,53,54]. A recent systematic review and meta-analysis by Hua et al. [55] aimed to compare the effectiveness of various dietary approaches in children and adolescents with functional abdominal pain disorders but found no significant differences between the dietary treatments. In the following paragraphs, we summarize the characteristics and supporting evidence for each dietary approach.
4.1.1. FODMAP Diet
Fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) are short-chain carbohydrates that are poorly absorbed in the small intestine, which can lead to bloating and gas. FODMAPs are found in various food groups, particularly in vegetables such as beetroot, broccoli, Brussels sprouts, cabbage, fennel, garlic, leek, onion, pumpkin, shallot, courgette, and squash, as well as in cereals like corn, rye, and wheat when consumed in large quantities [56].
Among legumes, those with the highest FODMAP content include beans, chickpeas, lentils, peas, red beans, and soybeans. FODMAPs are also present in certain fruits, such as apricots, bananas, blueberries, cranberries, currants, quinces, grapefruits, melons, persimmons, plums, pomegranates, and watermelons, as well as in dried fruits like almonds, cashews, hazelnuts, and pistachios [57].
A low-FODMAP diet is widely used to manage irritable bowel syndrome (IBS) in adults [58]. However, given the broad range of foods to limit, this diet may be challenging for pediatric patients. In 2022, the ESPGHAN (European Society for Pediatric Gastroenterology Hepatology and Nutrition) published a Position Paper on the use of a low-FODMAP diet in children [59], concluding that further evidence is needed to support its use in pediatrics, with some promising findings for IBS. Emerging evidence suggests that dietary interventions, such as low-FODMAP diets, modulate microbiota diversity and fermentation patterns, which can alleviate symptoms like bloating and abdominal pain. However, the long-term impact on microbiota composition and pediatric health remains underexplored [59].
A recent systematic review [60] examined the effects of a low-FODMAP diet on FBDs in children, but the results were insufficient to support specific therapeutic recommendations, except for irritation bowel syndrome, aligning with ESPGHAN’s guidelines [59].
This year, a trial evaluated the impact of a low-FODMAP diet on health-related quality of life in a sample of Egyptian children [61]. Researchers enrolled 84 children aged 5–15 years, randomly assigned to either a low-FODMAP or a standard diet group. Each participant received a list of foods to include and avoid (high-FODMAP foods) and followed dietary advice for six weeks [61]. Weekly assessments included a visual analogue scale (VAS) for pain severity, the Pediatric Quality of Life Inventory (PedsQL), and the GI Symptoms Module Scale.
Results indicated a significant reduction in abdominal pain severity, improved gastrointestinal symptoms, and an enhanced health-related quality of life in children who adhered to the low-FODMAP diet [61]. Interestingly, none of the studies analyzed in Katzagoni et al.’s systematic review reported high health-related quality of life scores [60].
Another recent study, conducted by Tenenbaum et al. [62] in 2024, explored whether quality of life could predict adherence to the low-FODMAP diet in children with FBDs. They found a positive association between quality of life and adherence to the diet. Given the complexity of this dietary strategy, close nutritional follow-up is essential not only to prevent nutrient deficiencies but also to reduce stress in the child by providing recipes or alternatives to maintain dietary variety, thereby improving adherence. However, further studies are needed to clarify the effectiveness of the low-FODMAP diet in children with FBDs.
4.1.2. Fructose or Lactose-Restricted Diet
Fructose and lactose malabsorption are also potential contributors to symptoms associated with FBDs, as both can lead to bacterial fermentation in the intestinal lumen, although through different mechanisms [63,64]. In clinical practice, lactose- and fructose-free diets have been proposed to help manage FBDs symptoms. The aforementioned systematic review [60] gathered evidence regarding this approach, but unfortunately, there is currently insufficient data to recommend lactose- or fructose-free diets universally. While some patients may experience symptom relief with dietary restrictions, further studies are needed to clarify factors such as individual tolerance levels and the threshold amounts that can be consumed without discomfort.
Regarding lactose, it is important to note that the ESPGHAN committee published a position paper on the use of infant formulas in treating functional gastrointestinal disorders [65]. They concluded that there is limited evidence supporting the use of specialized formulas and emphasized that breastfeeding should not be discontinued in favor of formula feeding.
Another noteworthy consideration is that lactose-free diets in children might lead to reduced protein and calcium intake, potentially resulting in shorter stature and lower bone mineral density [66]. However, this claim remains controversial [67,68,69], and further large-scale studies are needed to clarify the relationship between growth outcomes and a lactose-free diet.
In contrast, the link between excess fructose intake and childhood obesity, along with associated conditions such as Nonalcoholic Fatty Liver Disease (NAFLD), is well-established [70,71]. Fructose is present not only in fruits and certain vegetables (e.g., tomatoes) but also as a common sweetener in fruit juices, sodas, and processed sweets. Even though evidence does not currently support fructose restriction as a treatment for FBDs symptoms, it is advisable for children to significantly reduce their intake of these fructose-rich products [72].
Lastly, for managing chronic constipation, the use of certain sugars such as cane sugar, fig syrup, and blackstrap molasses has also been explored as alternative remedies [73,74,75]. Beleli et al. [73] showed that 4′-galactooligosaccharides derived from sugars can improve constipation symptoms in pediatric populations, highlighting their potential as a dietary intervention. Similarly, Dehghani et al. [74] conducted a randomized controlled trial comparing blackstrap molasses with polyethylene glycol, and despite no significant differences between groups, both treatments were shown to have beneficial effects and may represent well-tolerated options for pediatric functional constipation. Additionally, Tajik et al. (2018) explored the use of red sugar versus fig syrup, concluding that both showed promising results as natural treatments for children with functional constipation [75]. However, the heterogeneity of the available evidence, including differences in study design, population characteristics, dosages, and outcome measures, prevents us from making definitive recommendations. However, the heterogeneity of available evidence prevents us from making definitive recommendations.
4.1.3. Gluten-Free Diet
The final dietary approach for managing FBDs is a gluten-free diet. Gluten intake has often been linked to the development of FBDs and worsening of symptoms, although this connection remains unclear [76]. Currently, evidence on the effects of gluten exclusion for FBDs symptoms in children is limited. According to the recent systematic review mentioned earlier [60], only three trials have investigated this relationship [77,78,79], each with varying study designs, interventions, and outcomes. As a result, there is currently no support for the use of a gluten-free diet in managing FBDs in children.
A gluten-free diet requires the complete elimination of gluten-containing grains, such as wheat, barley, rye, and their derivatives. Additionally, gluten can be added as an ingredient in processed foods. Cross-contact during both industrial and home preparation can also lead to contamination, potentially introducing gluten traces in foods that would otherwise be gluten-free.
This potential for contamination might contribute to a finding from a study by Fioti et al. [80], where over 50% of adolescents surveyed expressed concern that a gluten-free diet restricts their food choices. Alongside psychosocial effects, economic implications are also noteworthy: gluten-free foods are often more expensive and less accessible than gluten-containing alternatives [81]. Further studies are necessary to clarify whether a gluten-free diet could be beneficial for children with FBDs.
4.2. Nutritional Education and Additional Strategies for Managing FBDs in Children with Obesity
The management of FBDs and obesity involves a unique approach because of the strong pathological correlations of these disorders. Nutritional education and lifestyle management are the primary therapeutic approaches to consider, alongside providing reassurance to the patient and their family. Patients should receive a clear understanding of the diagnosis, a full explanation of the link between overweight and FBDs and be told what organic diseases have been excluded. Exclusion of organic diseases, setting realistic therapeutic goals and sharing the therapeutic decision with the patients give them more satisfaction, better adherence to the outlined therapy and reduce the drop-out [60].
Nutritional education provides elementary rules that should be practiced daily in addition to any indication to specific dietary regimens [55]. The different dietary interventions are characterized by the absence of significant differences in terms of efficacy and safety [55]. The process of deciding which therapy to use for everyone should be guided by a thorough evaluation conducted by the dietitian, with patients actively participating in this process [82]. Moreover, food precautions should be applied in the management and prevention of FBDs [55]. Fiber supplementation in daily practice could be considered because of fibers leads to higher treatment success with minimal side effects [83]. Fiber improves regularity by stimulating bowel movements and can help regulate gastrointestinal symptoms. They also act as prebiotics, supporting gut health and digestion. Additionally, fiber retains water in the stool, promoting texture while promoting a feeling of fullness that can help with weight management [84]. Despite the positive effects, evidence does not indicate the use of fibers supplements and extra fluid intake in the treatment of specific FBDs such as functional constipation [85,86].
Dietary management is the crucial key in controlling functional gastrointestinal disorders symptoms. In several studies, dietary education was provided by a dietitian with verbal instructions or written material [87]. However, given the significant differences in nutrition education and the lack of specialized instructional materials, further efforts are needed to establish a consistent and effective method of educating patients about dietary interventions. Adherence to diet could allow resolution and control of FBDs [88]. Several aspects may represent barriers to adherence: the length of dietary intervention, individual preferences, attitudes towards certain food and diets, nutritional knowledge, physical and social factors [89,90]. Family dynamics and parenting style can influence health care (including approach to decision-making, communication with clinician, medication adherence) and adherence outcomes in pediatric functional constipation. To improve medical regimens and achieve better outcomes, it is essential to study, understand, and incorporate family dynamics into the treatment approach for pediatric constipation [91]. To maximize effectiveness of nutritional interventions and adherence, it is relevant to find ways to assess and address these burdens during clinical contests and nutritional education [89,90,92].
Patient education about physical activity is necessary for the prevention and treatment of FBDs. The role of physical activity in the management of functional constipation is varied. Few studies are conducted on pediatric patients [93,94,95,96], but many studies conducted in adulthood underline the importance of physical activity in the treatment of FBDs [97,98,99].
A negative correlation between physical activity and functional constipation has been demonstrated in several study on children [93,94]. However, insufficient physical activity and excessive sedentary behaviors are associated with functional constipation in Asian adolescent [95]. Physical activity could reduce symptoms of functional constipation in the longer time. A high level of physical activity, established with an actigraph accelerometer in children with an average age of 25 months, allows to reduce the incidence of functional constipation in the fourth year of life. This result was obtained in children who practiced physical activity for more than 60 min/day [96]. Adult patients with IBS are suggested to engage in slow, low-intensity activities (cycling, swimming, yoga and aerobics) for 20 to 60 min three to five times a week. These kinds of physical activities have beneficial effects on gastrointestinal symptoms, particularly in reducing the occurrence of constipation, and the well-being of individuals with IBS [97]. Additionally, active individuals tend to have better eating habits, such as drinking more water and maintaining regular mealtimes [98]. In conclusion, physical activity combined with an adequate diet are two important therapeutic aspects of the management of overweight and gastrointestinal functional disorders. In addition, physical activity allows additional benefits, reducing symptoms of anxiety and depression [98,99].
Functional abdominal pain disorders (FAPDs), known as disorders of gut–brain interaction, are also related to emotional difficulties. Children and adolescents with FAPDs have higher levels of anxiety and depression, as well as lower quality of life, than healthy children [100]. Home and school related stressors are associated with the development of functional constipation in children [101]. Children and adolescents could have severe limitations in their social life and daily activities resulting from FAPDs due to the symptoms, and this can harm functional gastrointestinal disorders. In the management of patients with FBS, clinicians should instruct the patient to intervene psychologically, with active family participation and ongoing medical management, when they do not respond to conventional treatment [102]. Family interactions can influence the development and maintenance of FGIDs through their effects on the physical and psychosocial functioning of an individual [103].
Several studies show that cognitive behavioral therapy could play a crucial role in reducing intensity for children with pain, especially in abdominal migraine and abdominal functional pain [104,105]. A randomized controlled trial reported that children who received a combination of standard medical care and CBT, along with their parents, experienced significantly less abdominal pain than those who received medical care alone [106]. Additionally, a recent meta-analysis indicated that CBT effectively ameliorates functional abdominal pain, reduces pain intensity, and enhances physical quality of life in affected children [107].
These findings underscore the importance of integrating family-focused CBT approaches in managing pediatric FGIDs to achieve optimal therapeutic outcomes.
Figure 2 summarizes the evidence regarding dietary strategies and represents the various intervention areas that should be considered in the management of children with FBDs (Figure 2).
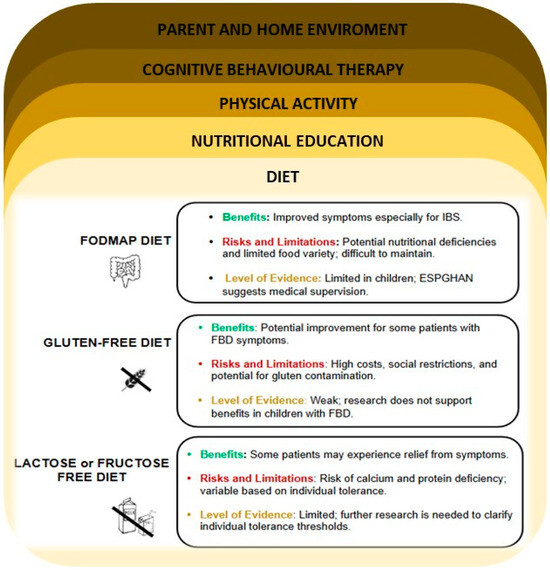
Figure 2.
Dietary strategies and intervention areas useful in the management of children with FBDs.
Given the established link between obesity and FGIDs [15,16,17], it is plausible that weight management, including weight loss, could alleviate FGID symptoms in affected children. Implementing healthy lifestyle changes, such as balanced nutrition and regular physical activity, may not only reduce BMI but also potentially improve gastrointestinal function.
5. Gut Implication
The human gut microbiota is a vast ecosystem of microorganisms that play a central role in various physiological functions, including metabolism, immune modulation, and gut health [108].
Increasing evidence points to a complex and bidirectional relationship between the gut microbiota, FBDs, and obesity, particularly in children. Indeed, changes in gut microbiota content are associated with the onset and persistence of FBDs as well as have been described as an important determinant in the pathophysiology of obesity [109]. When FBDs and obesity coexist, the altered microbiota tends to amplify dysfunctions present in each condition, worsening both gastrointestinal and metabolic symptoms [109,110]. Obesity-related systemic inflammation, coupled with gut dysbiosis, may exacerbate gut permeability (‘leaky gut’) and visceral hypersensitivity, both hallmarks of FBDs. These mechanisms underline the need for interventions targeting the microbiome to simultaneously address obesity and FBD symptoms.
5.1. The Impact of Gut Microbiota
5.1.1. Dysbiosis in Functional Bowel Disorders and Obesity
Gut microbiota composition in both FBDs and obesity is typically disrupted, showing reduced diversity and an overabundance of certain proinflammatory bacteria [111].
The balance between bacterial populations, rather than their absolute quantities, often plays a more critical role in shaping the functional impact of the gut microbiota. For instance, shifts in the Firmicutes-to-Bacteroidetes ratio have been highlighted as key determinants in obesity and related conditions [112,113]. Although the composition of dysbiotic microbiota is still controversial, some studies reported that children with obesity have higher levels of Firmicutes and lower levels of beneficial bacteria such as Bacteroidetes and Bifidobacteria, resulting in an enhanced capacity to derive energy from food due to a more active breakdown of carbohydrate complexes [112,113,114]. The composition of gut microbiota in FBDs is controversial, but patients seem to have a similar dysbiosis status [115]. As the gut microbiota is responsible for several mechanisms (e.g., the fermentation of undigested proteins and carbohydrates, the utilization of hydrogen, the transformation of bile acids and gas), dysbiosis can lead to disturbances of the intestine’s immune function, altered motility and gut permeability, commonly referred to as “leaky gut,” allowing bacterial components to enter the bloodstream [116]. The immune system activation associated with this process further exacerbates gut-related symptoms and can contribute to a chronic inflammatory state, often observed in individuals with FBDs [116]. These changes lead to worsened gastrointestinal symptoms, such as bloating, abdominal pain, and constipation [27].
5.1.2. Microbiota-Mediated Mechanisms and Therapeutic Implications
A study by Saulnier et al. [117] showed that the content of microbiota correlated with the severity and rate of abdominal pain in children with IBS. These symptoms may be intensified due to changes in microbiota-mediated production of short-chain fatty acids (SCFAs) and gasses like methane, which have been shown to affect gut motility and sensitivity [118]. Even the relationship between gut microbiota and FC is frequently explored through its impact on gut transit time. This could be due to microbial influence on gene expression that affects the gut’s motor responses, pH-dependent motility stimulation by fermentation, osmotic effects caused by microbial metabolites, and intestinal stretching due to increased intraluminal gas production, which triggers reflexive contractions of the smooth muscle [119,120]. The differences in the gut microbiota between children with FC and the control group were shown in different studies [119,120]. One study evidenced how children with obesity and FC had significantly lower levels of Bacteroidetes, in particular Prevotella, and higher levels of some groups of Firmicutes, such as Lactobacillus, compared with healthy children [120]. Other studies also highlighted increased levels of Bifidobacteria [119,121].
The coexistence of altered gut microbiota, obesity, and FBDs may have an impact on the efficacy of dietary and pharmacological interventions. For example, dietary modifications commonly recommended for FBDs, such as the low-FODMAP diet, may affect the microbiota composition by temporarily reducing bacterial fermentation [122]. The efficacy of specific probiotics, such as Lactobacillus reuteri and Bifidobacterium species, varies due to strain-specific mechanisms affecting motility and gut barrier integrity. For instance, while Lactobacillus reuteri DSM 17,938 showed benefits in some studies, others found limited effects on stool frequency, suggesting that patient-specific factors like baseline microbiota composition may influence outcomes [123]. Personalized interventions related to gut microbiota composition may be essential for improving clinical outcomes in children affected by both conditions.
5.2. The Role of Biotics and Integrative Support
5.2.1. Biotics
Given the role of diet in modulating gut microbiota and influencing symptoms of FBDs, additional strategies like probiotics and prebiotics hold promise in optimizing gut health and symptom management. The WHO defines probiotics as “live microorganisms which when administered in adequate amounts confer a health benefit on the host” [124]. Noteworthy, to be defined as probiotics, microorganisms must demonstrate evidence-based health benefits [125]. Probiotics have demonstrated effectiveness in preventing and/or treating many gastrointestinal disorders, such as infectious and antibiotic-associated diarrhea, ulcerative colitis, infantile colic, IBS, and FAP [126]. They interact with the host through mechanisms such as enhancing gut barrier function, modulating immune responses, and influencing microbial composition. The activity of probiotics is strain and species-specific and changes according to the physiology and eating habits of different subjects [127]. Specific probiotics can directly act on gut motility and barrier functions, host digestion, immune responses, nociception, metabolism, behavior, and microbiota composition [126]. Concerning functional constipation, a randomized control trial (RCT) involving 45 children over a 4-week protocol, evaluated the effects of Lactobacillus casei rhamnosus (Lcr35) on abdominal pain and intestinal transit. The authors compared the efficacy of Lcr35 with magnesium oxide (MgO) and placebo [128]. While improvements in abdominal pain and intestinal transit were observed, the results were not statistically significant. Furthermore, the efficacy of Lactobacillus reuteri DSM 17,938 has been assessed in several studies [128,129,130]. Kubota and colleagues also found a reduction in the abundance of the genus Dialister in the group of children administrated with the MgO, an osmotic laxative frequently used in constipation treatment, suggesting that further studies are needed to explore better the interplay between the treatment and the gut microbiota [129]. Besides, the results have been inconsistent so far.
Prebiotics are substrates selectively used by the host microbiota. These molecules exert a positive impact on intestinal barrier function by modulating tight junctions (TJs) through their interaction with the gut microbiota, providing health benefits [131]. Molecules that have been tested for treating FBDs include inulin, galacto-oligosaccharides (GOS), fructo-oligosaccharides (FOS), glucomannan, psyllium, and different fiber mixtures [131].
Lately, interest in the use of inulin in the treatment of FC has been rising. Closa-Monasterolo et al. showed that administering 2g/day of inulin for six weeks significantly improved stool consistency [132]. Lohner et al., in a cohort of children aged 3 to 7 years receiving 6 g/day of inulin for 24 weeks, demonstrated that the relative abundance of Bifidobacterium and Lactobacillus in stool samples of children receiving fructans, was respectively 19.9% and 7.8% higher compared to the control group at week 24 (p = 0.014 for Lactobacillus and p < 0.001 for Bifidobacterium). Also, children in the treated group experienced significantly softer stools, starting from week 12 [133].
Recent studies indicate that certain prebiotics may have a role in regulating mucus production, composition, and degradation. FOS has been studied as prebiotics in both animals and humans. These molecules may improve glucose, lipid, and energy metabolism in the host, by modifying the composition of the gut microbiota [134,135]. For instance, the administration of FOS has been shown to ameliorate metabolic disorders resulting from a high-fat diet by promoting the secretion of glucagon-like peptides 1 and 2 (GLP-1 and GLP-2) [136,137].
Research explored the effect of fiber mixtures at different dosages in pediatric populations. In particular, Kokke et al. studied the impact of a fiber blend (including soy fiber, inulin, GOS, and resistant starch) compared to lactulose in 97 children with FC [138]. However, no significant differences were observed in defecation frequency or abdominal pain. When compared to polyethylene glycol (PEG), a fiber mixture comprising acacia fiber, psyllium fiber, and fructose, yielded comparable results after 8 weeks in terms of bowel movement frequency, stool consistency, and fecal incontinence [138]. One systematic review and meta-analysis of three RCTs investigated the efficacy of glucomannan in the improvement of the symptoms in children with FC [139]. Staiano and colleagues reported a statistically significant improvement in stool consistency after a treatment of 12 weeks with 100 mg/kg of glucomannan in a cohort of 20 children (p < 0.01) [140].
Dietary fiber supplementation is a common approach for managing IBS, but its effectiveness can vary based on the type of fiber. Soluble fibers, found in some fruits and legumes, absorb water, slow down intestinal transit, and reduce cholesterol absorption [85]. In contrast, insoluble fibers, found in fruit peels and bran, increase fecal volume and accelerate intestinal transit, making them more suitable for IBS patients who experience constipation [141]. Baştürk et al. conducted an investigation using a synbiotic formulation that included the probiotic strains Lactobacillus casei, Lactobacillus rhamnosus, Lactobacillus plantarum, and Bifidobacterium lactis, with diverse prebiotics, including fiber, polydextrose, FOS, and GOS. After 4 weeks of treatment, the overall benefits observed from the synbiotic intervention were significantly greater than those in the placebo group [142]. Although especially probiotic supplements have shown significant improvements in abdominal symptoms compared to placebo in patients with IBS, there is still a lack of long-term evidence for their use, particularly in children [141].
5.2.2. Curcumin and Other Phytochemicals
Polyphenols, such as catechins, anthocyanins, curcumin, have shown promising effects on lipid metabolism, energy regulation, and weight management [143]. Animal and cell studies propose several mechanisms behind these benefits, including the inhibition of adipocyte differentiation, enhanced fatty acid oxidation, reduced fatty acid synthesis, stimulation of thermogenesis, facilitation of energy metabolism, and inhibition of digestive enzymes [144]. Anthocyanins also exhibit antibacterial properties, inhibiting the growth of pathogens like Bacillus cereus and Helicobacter pylori, suggesting their role in modulating gut microbiota that may contribute to obesity and inflammatory disease management [145].
Curcumin, recognized for its antioxidant properties, is one of the most studied polyphenol [144]. In a meta-analysis of RCTs, has been shown that curcumin reduce oxidative stress in a dose- and duration-dependent manner by scavenging free radicals and inhibiting the production of malondialdehyde [146]. Specifically, curcumin significantly reduced malondialdehyde [SMD −0.46 (CI 95%: −0.68 to −0.25)] and increased superoxide dismutase [0.82 (0.27 to 1.38)], glutathione peroxidase [8.90 (6.62 to 11.19)], and catalase [10.26 (0.92 to 19.61)], comparing with control group. Also, the co-administration of piperine and curcumin may have a potential to enhance curcumin’s effectiveness in supporting the antioxidant molecules role [146]. Once curcumin reaches the intestines, it is metabolized by the host’s microbiota. This process produces secondary metabolites that may promote the growth of beneficial bacterial strains in the host gut [147]. Additionally, curcumin has been studied as potential support in alleviating IBS symptoms other than metabolic disease and obesity [148], enhancing pain relief and quality of life, although the results are not consistent, particularly in children [149,150].
However, despite its therapeutic potential across several diseases, curcumin’s clinical utility is limited by its poor gastrointestinal absorption and low bioavailability [151]. These limitations are mainly due to its insolubility in water, rapid metabolism, and excretion [152]. However, recent evidence suggest a need to redefine bioavailability because of the gut microbiota’s role as a dynamic organ that interacts with and processes curcumin and other molecules [153,154]. Hassaninasab et al. demonstrated that Escherichia coli is the microorganism with the highest ability to metabolize native curcumin, leading to obtain tetrahydrocurcumin, the reduced analog of curcumin predominantly present in the gastrointestinal tract [147]. Furthermore, Bifidobacterium longum, Lactobacillus acidophilus, Bifidobacterium pseudocatenulatum, and Lactobacillus casei, have been shown to metabolize curcumin, reducing over 50% of the original compound, emphasizing their role in converting curcumin into bioactive metabolites that could enhance its physiological effects [155,156].
Despite curcumin’s good tolerability and its antioxidant and anti-inflammatory properties [157], evidence supporting its efficacy is still limited and its effect mainly comes from studies conducted on adult populations [158].
In Table 2, the summary of the papers referred to dietary interventions and integrative support in children with FBDs are resumed.
Table 2.
Summary of the papers referred to dietary interventions and integrative support in children with FBDs.
6. Limitations
We recognize several limitations in this review. First, this is a narrative review, which offers a non-systematic overview and analysis of the existing literature on the topic [15,27]. The absence of standardized guidelines for narrative reviews can lead to selection biases and often results in qualitative rather than quantitative analyses. For example, our review focused solely on articles available on PubMed, which may have excluded relevant studies indexed in other databases or published in non-English languages. This may have limited the diversity and comprehensiveness of the included studies.
Another limitation is the scarcity of long-term follow-up data in the available studies. Most of the reviewed evidence lacks robust longitudinal assessments leaving significant gaps in understanding how therapeutic approaches influence the progression and management of FGIDs over time. This limitation highlights the need for future studies with standardized follow-up protocols to evaluate the sustainability of interventions and their long-term impacts on pediatric populations.
Additionally, data on integrative support in pediatrics remain heterogeneous, with considerable variability in study designs, populations, and intervention protocols. The inconsistency of findings regarding the efficacy of probiotics, prebiotics, and other dietary interventions underscores the need for large-scale randomized controlled trials to establish evidence-based recommendations.
Furthermore, the complex interplay between gut microbiota, dietary factors, and psychosocial elements presents another challenge. Many studies do not adequately account for potential confounders, such as genetic predispositions, which may influence the outcomes and limit the generalizability of findings. Socioeconomic status, physical activity levels, and dietary patterns can act as confounders in studies linking obesity and FBDs. For example, sedentary behavior not only contributes to obesity but also influences gastrointestinal motility, underscoring the importance of multifaceted approaches in both research and clinical management.
To deepen our understanding of the relationship between of obesity and FGIDs, it will be crucial to integrate prevention and treatment strategies into broader frameworks that account for these multifactorial influences. Future research should prioritize interdisciplinary collaboration and aim to address these limitations by utilizing more comprehensive study designs, expanding inclusion criteria, and embracing innovative methodologies, such as microbiome analyses and machine learning models for data integration.
7. Conclusions
A potential association between obesity and FGIDs has been identified with both conditions sharing common characteristics, including high prevalence in children, diet- and lifestyle-related risk factors, gut microbiota imbalances, and psychological challenges. Managing this dual condition in pediatric patients presents unique challenges, particularly due to poor adherence to conventional treatments. This narrative review emphasizes the need for holistic and multidisciplinary approaches to symptom management. Nutrition education, physical activity, and medical care must be complemented by additional strategies such as psychological interventions and personalized dietary modifications, including low-FODMAP and fiber-enriched regimens. These strategies not only address immediate symptoms but also provide a foundation for long-term health benefits. Considering the interplay between gut microbiota alterations, obesity, and FGIDs, the modulation of gut microbiota through probiotics, prebiotics, and integrative support shows significant promise. Although current evidence highlights their potential in prevention and treatment, the variability in findings calls for robust, well-designed longitudinal studies to establish standardized protocols and maximize their efficacy. Addressing this issue holistically and combining these approaches will not only enhance the scientific understanding of the connection between obesity, gut microbiota, and FBDs but also improve the quality of clinical and preventive care for pediatric patients. Future research should aim to elucidate the bidirectional mechanisms linking these conditions, focusing on personalized interventions tailored to individual gut microbiota profiles. Standardization of diagnostic criteria and measures of intervention efficacy is crucial to facilitate the reproducibility and applicability of findings.
Ultimately, bridging the gaps in knowledge and practice through an integrated, evidence-based framework has the potential to improve patient outcomes and deepen our understanding of the intricate relationship between metabolic and gastrointestinal health in children.
Author Contributions
Conceptualization, V.C., H.C., M.G.W. and G.Z.; methodology, V.C., H.C., F.L., D.P., S.B., C.G., C.R.R., M.V.C., G.L., M.G.W. and G.Z.; writing—original draft preparation, F.L., D.P., S.B., C.G., C.R.R. and M.V.C.; writing—review and editing, V.C., H.C., F.L., D.P., S.B., C.G., C.R.R., M.V.C., G.L., M.G.W. and G.Z.; supervision, V.C., H.C., M.G.W. and G.Z. All authors have read and agreed to the published version of the manuscript.
Funding
Project performed in the context of (1) National Recovery and resilience Plan (NRRP), Mission 4 Component 2 Investment 1.3-Call for proposal No. 341 of 15 March 2022 of Italian Ministry of University and Research funded by the European Union-NextGenerationEU. Project code PE00000003, Concession Decree No. 1550 of 11 October 2022 adopted by the Italian Ministry of University and Research, CUP F13C22001210007, Project title “ON Foods-Research and innovation network on food and nutrition Sustainability, Safety and Security-Working ON Foods”; (2) PODiaCar Project 101128946—PODiaCar—EU4H-2022-PJ-3 co-funded by European Union; (3) The authors would like to acknowledge the Obelisk consortium for its valuable contributions to this field of research. The content of this publication reflects the views of the authors only. OBELISK Project (FIGHTING CHILDHOOD OBESITY TO STAY HEALTHY ALL OVER THE LIFE) has received funding from the European Union’s Horizon Europe Research and Innovation programme under grant agreement No 101080465.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Correction Statement
This article has been republished with a minor correction to the Funding statement. This change does not affect the scientific content of the article.
References
- Longstreth, G.F.; Thompson, W.G.; Chey, W.D.; Houghton, L.A.; Mearin, F.; Spiller, R.C. Functional Bowel Disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef]
- Hyams, J.S.; Di Lorenzo, C.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Childhood functional gastrointestinal disorders: Child/adolescent. Gastroenterology 2016, 150, 1456–1468.e2. [Google Scholar] [CrossRef]
- Boronat, A.C.; Ferreira-Maia, A.P.; Matijasevich, A.; Wang, Y.-P. Epidemiology of Functional Gastrointestinal Disorders in Children and Adolescents: A Systematic Review. World J. Gastroenterol. 2017, 23, 3915–3927. [Google Scholar] [CrossRef]
- Korterink, J.J.; Diederen, K.; Benninga, M.A.; Tabbers, M.M. Epidemiology of Pediatric Functional Abdominal Pain Disorders: A Meta-Analysis. PLoS ONE 2015, 10, e0126982. [Google Scholar] [CrossRef] [PubMed]
- Scarpato, E.; Kolacek, S.; Jojkic-Pavkov, D.; Konjik, V.; Živković, N.; Roman, E.; Kostovski, A.; Zdraveska, N.; Altamimi, E.; Papadopoulou, A.; et al. Prevalence of Functional Gastrointestinal Disorders in Children and Adolescents in the Mediterranean Region of Europe. Clin. Gastroenterol. Hepatol. 2018, 16, 870–876. [Google Scholar] [CrossRef]
- Tran, D.L.; Sintusek, P. Functional Constipation in Children: What Physicians Should Know. World J. Gastroenterol. 2023, 29, 1261–1288. [Google Scholar] [CrossRef]
- Mani, J.; Madani, S.; Thomas, R. Economic Impact and Prognostic Factors of Functional Dyspepsia in Children. J. Pediatr. Gastroenterol. Nutr. 2020, 70, E65–E70. [Google Scholar] [CrossRef] [PubMed]
- Hoekman, D.R.; Rutten, J.M.T.M.; Vlieger, A.M.; Benninga, M.A.; Dijkgraaf, M.G.W. Annual Costs of Care for Pediatric Irritable Bowel Syndrome, Functional Abdominal Pain, and Functional Abdominal Pain Syndrome. J. Pediatr. 2015, 167, 1103–1108.e2. [Google Scholar] [CrossRef]
- Nurko, S.; Di Lorenzo, C. Functional Abdominal Pain: Time to Get Together and Move Forward. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 679–680. [Google Scholar] [CrossRef] [PubMed]
- Devanarayana, N.M.; Rajindrajith, S. Irritable Bowel Syndrome in Children: Current Knowledge, Challenges and Opportunities. World J. Gastroenterol. 2018, 24, 2211–2235. [Google Scholar] [CrossRef]
- Nightingale, S.; Sharma, A. Functional Gastrointestinal Disorders in Children: What Is New? J. Paediatr. Child. Health 2020, 56, 1724–1730. [Google Scholar] [CrossRef]
- Ganesh, M.; Nurko, S. Functional Dyspepsia in Children. Pediatr. Ann. 2014, 43, e101–e105. [Google Scholar] [CrossRef] [PubMed]
- Obesity and Overweight—World Health Organization (WHO). Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 10 October 2024).
- Jebeile, H.; Kelly, A.S.; O’Malley, G.; Baur, L.A. Obesity in Children and Adolescents: Epidemiology, Causes, Assessment, and Management. Lancet Diabetes Endocrinol. 2022, 10, 351–365. [Google Scholar] [CrossRef]
- Phatak, U.P.; Pashankar, D.S. Obesity and Gastrointestinal Disorders in Children. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Rajindrajith, S.; Devanarayana, N.M.; Benninga, M.A. Obesity and Functional Gastrointestinal Diseases in Children. J. Neurogastroenterol. Motil. 2014, 20, 414–416. [Google Scholar] [CrossRef]
- Pogodina, A.; Romanitsa, A.; Rychkova, L. Functional Bowel Disorders and Obesity in Children: State of the Problem. IJBM 2020, 10, 316–323. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128·9 Million Children, Adolescents, and Adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Wong, A.H.C.; Hon, K.L. Childhood Obesity: An Updated Review. Curr. Pediatr. Rev. 2024, 20, 2–26. [Google Scholar] [CrossRef]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef]
- Teitelbaum, J.E.; Sinha, P.; Micale, M.; Yeung, S.; Jaeger, J. Obesity Is Related to Multiple Functional Abdominal Diseases. J. Pediatr. 2009, 154, 444–446. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.J.; Leahy, F.E.; McGowan, A.A.; Bluck, L.J.C.; Coward, W.A.; Jebb, S.A. Delayed Gastric Emptying in the Obese: An Assessment Using the Non-Invasive (13)C-Octanoic Acid Breath Test. Diabetes Obes. Metab. 2004, 6, 264–270. [Google Scholar] [CrossRef]
- Di Ciaula, A.; Wang, D.Q.-H.; Portincasa, P. Gallbladder and Gastric Motility in Obese Newborns, Pre-Adolescents and Adults. J. Gastroenterol. Hepatol. 2012, 27, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- Yoon, K.; Kim, N. Roles of Sex Hormones and Gender in the Gut Microbiota. J. Neurogastroenterol. Motil. 2021, 27, 314–325. [Google Scholar] [CrossRef] [PubMed]
- Galai, T.; Moran-Lev, H.; Cohen, S.; Ben-Tov, A.; Levy, D.; Weintraub, Y.; Amir, A.; Segev, O.; Yerushalmy-Feler, A. Higher Prevalence of Obesity among Children with Functional Abdominal Pain Disorders. BMC Pediatr. 2020, 20, 193. [Google Scholar] [CrossRef] [PubMed]
- Tambucci, R.; Quitadamo, P.; Ambrosi, M.; De Angelis, P.; Angelino, G.; Stagi, S.; Verrotti, A.; Staiano, A.; Farello, G. Association Between Obesity/Overweight and Functional Gastrointestinal Disorders in Children. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 517–520. [Google Scholar] [CrossRef]
- Phatak, U.P.; Pashankar, D.S. Prevalence of Functional Gastrointestinal Disorders in Obese and Overweight Children. Int. J. Obes. 2014, 38, 1324–1327. [Google Scholar] [CrossRef] [PubMed]
- Pashankar, D.S.; Loening-Baucke, V. Increased Prevalence of Obesity in Children with Functional Constipation Evaluated in an Academic Medical Center. Pediatrics 2005, 116, e377–e380. [Google Scholar] [CrossRef] [PubMed]
- Zia, J.K.; Lenhart, A.; Yang, P.-L.; Heitkemper, M.M.; Baker, J.; Keefer, L.; Saps, M.; Cuff, C.; Hungria, G.; Videlock, E.J.; et al. Risk Factors for Abdominal Pain-Related Disorders of Gut-Brain Interaction in Adults and Children: A Systematic Review. Gastroenterology 2022, 163, 995–1023.e3. [Google Scholar] [CrossRef] [PubMed]
- Elitsur, Y.; Dementieva, Y.; Elitsur, R.; Rewalt, M. Obesity Is Not a Risk Factor in Children with Reflux Esophagitis: A Retrospective Analysis of 738 Children. Metab. Syndr. Relat. Disord. 2009, 7, 211–214. [Google Scholar] [CrossRef]
- Bonilla, S.; Wang, D.; Saps, M. Obesity Predicts Persistence of Pain in Children with Functional Gastrointestinal Disorders. Int. J. Obes. 2011, 35, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.R.; Ward, M.J.; Beneck, D.; Cunningham-Rundles, S.; Moon, A. The Association between Childhood Overweight and Reflux Esophagitis. J. Obes. 2010, 2010, 136909. [Google Scholar] [CrossRef][Green Version]
- Meng, D.; Ai, S.; Spanos, M.; Shi, X.; Li, G.; Cretoiu, D.; Zhou, Q.; Xiao, J. Exercise and Microbiome: From Big Data to Therapy. Comput. Struct. Biotechnol. J. 2023, 21, 5434–5445. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Santolaya, J.L.; Wright, T.F.; Liu, Q.; Fujikawa, T.; Chi, S.; Bergstrom, C.P.; Lopez, A.; Chen, Q.; Vale, G.; et al. Interaction between the Gut Microbiota and Colonic Enteroendocrine Cells Regulates Host Metabolism. Nat. Metab. 2024, 6, 1076–1091. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Yi, D.Y.; Lee, Y.M.; Choi, Y.J.; Kim, J.Y.; Hong, Y.H.; Park, J.Y.; Kim, S.Y.; Lee, N.M.; Yun, S.W.; et al. Association between Body Mass Index and Fecal Calprotectin Levels in Children and Adolescents with Irritable Bowel Syndrome. Medicine 2022, 101, e29968. [Google Scholar] [CrossRef] [PubMed]
- Rainone, V.; Schneider, L.; Saulle, I.; Ricci, C.; Biasin, M.; Al-Daghri, N.M.; Giani, E.; Zuccotti, G.V.; Clerici, M.; Trabattoni, D. Upregulation of Inflammasome Activity and Increased Gut Permeability Are Associated with Obesity in Children and Adolescents. Int. J. Obes. 2016, 40, 1026–1033. [Google Scholar] [CrossRef]
- Nemchenko, U.M.; Grigorova, E.V.; Pogodina, A.V.; Belkova, N.L.; Voropaeva, N.M.; Romanitsa, A.I.; Grigoryeva, E.A.; Savelkaeva, M.V.; Rychkova, L.V. The Relationship between the Composition of the Microbiota and Functional Intestinal Disorders in Obese Adolescents. Klin. Lab. Diagn. 2022, 67, 106–109. [Google Scholar] [CrossRef]
- Chen, J.; Liu, X.; Zou, Y.; Gong, J.; Ge, Z.; Lin, X.; Zhang, W.; Huang, H.; Zhao, J.; Saw, P.E.; et al. A High-Fat Diet Promotes Cancer Progression by Inducing Gut Microbiota-Mediated Leucine Production and PMN-MDSC Differentiation. Proc. Natl. Acad. Sci. USA 2024, 121, e2306776121. [Google Scholar] [CrossRef]
- DiBaise, J.K.; Zhang, H.; Crowell, M.D.; Krajmalnik-Brown, R.; Decker, G.A.; Rittmann, B.E. Gut Microbiota and Its Possible Relationship with Obesity. Mayo Clin. Proc. 2008, 83, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Brenchley, J.M.; Douek, D.C. Microbial Translocation across the GI Tract. Annu. Rev. Immunol. 2012, 30, 149–173. [Google Scholar] [CrossRef]
- Vermeire, S.; Van Assche, G.; Rutgeerts, P. C-Reactive Protein as a Marker for Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2004, 10, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Hollander, D.; Vadheim, C.M.; Brettholz, E.; Petersen, G.M.; Delahunty, T.; Rotter, J.I. Increased Intestinal Permeability in Patients with Crohn’s Disease and Their Relatives. A Possible Etiologic Factor. Ann. Intern. Med. 1986, 105, 883–885. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, K.R.; Halliday, M.I.; Barclay, G.R.; Milne, L.; Brown, D.; Stephens, S.; Maxwell, R.J.; Rowlands, B.J. Significance of Systemic Endotoxaemia in Inflammatory Bowel Disease. Gut 1995, 36, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Mulders, R.J.; de Git, K.C.G.; Schéle, E.; Dickson, S.L.; Sanz, Y.; Adan, R.A.H. Microbiota in Obesity: Interactions with Enteroendocrine, Immune and Central Nervous Systems. Obes. Rev. 2018, 19, 435–451. [Google Scholar] [CrossRef] [PubMed]
- Duan, M.; Wang, Y.; Zhang, Q.; Zou, R.; Guo, M.; Zheng, H. Characteristics of Gut Microbiota in People with Obesity. PLoS ONE 2021, 16, e0255446. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Jiang, W.; Huang, W.; Lin, Y.; Chan, F.K.L.; Ng, S.C. Gut Microbiota in Patients with Obesity and Metabolic Disorders—A Systematic Review. Genes. Nutr. 2022, 17, 2. [Google Scholar] [CrossRef]
- Scheithauer, T.P.M.; Rampanelli, E.; Nieuwdorp, M.; Vallance, B.A.; Verchere, C.B.; van Raalte, D.H.; Herrema, H. Gut Microbiota as a Trigger for Metabolic Inflammation in Obesity and Type 2 Diabetes. Front. Immunol. 2020, 11, 571731. [Google Scholar] [CrossRef]
- Zeevenhooven, J.; Browne, P.D.; L’Hoir, M.P.; De Weerth, C.; Benninga, M.A. Infant Colic: Mechanisms and Management. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 479–496. [Google Scholar] [CrossRef]
- Corsello, A.; Pugliese, D.; Gasbarrini, A.; Armuzzi, A. Diet and Nutrients in Gastrointestinal Chronic Diseases. Nutrients 2020, 12, 2693. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Zogg, H.; Ghoshal, U.C.; Ro, S. Current Treatment Options and Therapeutic Insights for Gastrointestinal Dysmotility and Functional Gastrointestinal Disorders. Front. Pharmacol. 2022, 13, 808195. [Google Scholar] [CrossRef] [PubMed]
- Tuck, C.J.; Reed, D.E.; Muir, J.G.; Vanner, S.J. Implementation of the Low FODMAP Diet in Functional Gastrointestinal Symptoms: A Real-world Experience. Neurogastroenterol. Motil. 2020, 32, e13730. [Google Scholar] [CrossRef] [PubMed]
- Wirth, S.; Klodt, C.; Wintermeyer, P.; Berrang, J.; Hensel, K.; Langer, T.; Heusch, A. Positive or Negative Fructose Breath Test Results do not Predict Response to Fructose Restricted Diet in Children with Recurrent Abdominal Pain: Results from a Prospective Randomized Trial. Klin. Padiatr. 2014, 226, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Rej, A.; Avery, A.; Aziz, I.; Black, C.J.; Bowyer, R.K.; Buckle, R.L.; Seamark, L.; Shaw, C.C.; Thompson, J.; Trott, N.; et al. Diet and Irritable Bowel Syndrome: An Update from a UK Consensus Meeting. BMC Med. 2022, 20, 287. [Google Scholar] [CrossRef]
- Hua, C.; Chen, Y.-L.; Tao, Q.-F.; Shi, Y.-Z.; Li, L.-W.; Xie, C.-R.; Chen, M.; Zhou, Z.-L.; Zheng, H. Dietary Interventions for Pediatric Patients with Functional Abdominal Pain Disorders: A Systematic Review and Network Meta-Analysis. Eur. J. Pediatr. 2023, 182, 2943–2956. [Google Scholar] [CrossRef]
- Usai Satta, P.; Mocci, G.; Lai, M. FODMAP Diet in Celiac Disease and Gluten-Related Disorders. Nutrients 2024, 16, 4190. [Google Scholar] [CrossRef]
- Roncoroni, L.; Elli, L.; Doneda, L.; Bascuñán, K.A.; Vecchi, M.; Morreale, F.; Scricciolo, A.; Lombardo, V.; Pellegrini, N. A Retrospective Study on Dietary FODMAP Intake in Celiac Patients Following a Gluten-Free Diet. Nutrients 2018, 10, 1769. [Google Scholar] [CrossRef] [PubMed]
- Lucas Zapata, P.; García Navarro, E.; Ribes Koninckx, C. The Low-FODMAP Diet. An. Pediatría (Engl. Ed.) 2024, 101, 36–45. [Google Scholar] [CrossRef]
- Thomassen, R.A.; Luque, V.; Assa, A.; Borrelli, O.; Broekaert, I.; Dolinsek, J.; Martin-de-Carpi, J.; Mas, E.; Miele, E.; Norsa, L.; et al. An ESPGHAN Position Paper on the Use of Low-FODMAP Diet in Pediatric Gastroenterology. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Katsagoni, C.N.; Karagianni, V.-M.; Papadopoulou, A. Efficacy of Different Dietary Patterns in the Treatment of Functional Gastrointestinal Disorders in Children and Adolescents: A Systematic Review of Intervention Studies. Nutrients 2023, 15, 2708. [Google Scholar] [CrossRef] [PubMed]
- El Ezaby, S.A.; Manzour, A.F.; Eldeeb, M.; El Gendy, Y.G.; Abdel Hamid, D.M. Effect of the Low Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAP) Diet on Control of Pediatric Irritable Bowel Syndrome and Quality of Life Among a Sample of Egyptian Children: A Randomized Controlled Clinical Trial. Cureus 2024, 16, e61017. [Google Scholar] [CrossRef]
- Tenenbaum, R.B.; Czyzewski, D.; McMeans, A.; Narayana, V.; Chumpitazi, B.P.; Levy, R.L.; Shulman, R.J.; Musaad, S.; Mirabile, Y.Z.; Self, M. Factors Associated with Adherence to a Low Fermentable Carbohydrate Diet in Children with Functional Gastrointestinal Disorders. J. Acad. Nutr. Diet. 2024, 124, 757–762. [Google Scholar] [CrossRef]
- Posovszky, C.; Roesler, V.; Becker, S.; Iven, E.; Hudert, C.; Ebinger, F.; Calvano, C.; Warschburger, P. Roles of Lactose and Fructose Malabsorption and Dietary Outcomes in Children Presenting with Chronic Abdominal Pain. Nutrients 2019, 11, 3063. [Google Scholar] [CrossRef] [PubMed]
- Kwiecień, J.; Hajzler, W.; Kosek, K.; Balcerowicz, S.; Grzanka, D.; Gościniak, W.; Górowska-Kowolik, K. No Correlation between Positive Fructose Hydrogen Breath Test and Clinical Symptoms in Children with Functional Gastrointestinal Disorders: A Retrospective Single-Centre Study. Nutrients 2021, 13, 2891. [Google Scholar] [CrossRef] [PubMed]
- Haiden, N.; Savino, F.; Hill, S.; Kivelä, L.; De Koning, B.; Köglmeier, J.; Luque, V.; Moltu, S.J.; Norsa, L.; De Pipaon, M.S.; et al. Infant Formulas for the Treatment of Functional Gastrointestinal Disorders: A Position Paper of the ESPGHAN Nutrition Committee. J. Pediatr. Gastroenterol. Nutr. 2024, 79, 168–180. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Williams, S.M.; Jones, I.E.; Goulding, A. Children Who Avoid Drinking Cow Milk Have Low Dietary Calcium Intakes and Poor Bone Health. Am. J. Clin. Nutr. 2002, 76, 675–680. [Google Scholar] [CrossRef]
- Lizzi, M.; Sgrazzutti, L.; Porreca, A.; Di Filippo, P.; Cauzzo, C.; Di Pillo, S.; Chiarelli, F.; Attanasi, M. Longitudinal Prospective Anthropometric Evaluation in Caucasian Prepubertal Children with Lactose Intolerance. Front. Pediatr. 2023, 11, 1219195. [Google Scholar] [CrossRef] [PubMed]
- Pienar, C.; Pop, L.; Lăzărescu, M.; Costăchescu, R.; Șeclăman, E. Anthropometric and Metabolic Profile of Children with Gene Polymorphisms for Primary Lactose Intolerance. Exp. Ther. Med. 2021, 22, 1333. [Google Scholar] [CrossRef]
- Lehtimäki, T.; Hemminki, J.; Rontu, R.; Mikkilä, V.; Räsänen, L.; Laaksonen, M.; Hutri-Kähönen, N.; Kähönen, M.; Viikari, J.; Raitakari, O. The Effects of Adult-Type Hypolactasia on Body Height Growth and Dietary Calcium Intake from Childhood into Young Adulthood: A 21-Year Follow-up Study--the Cardiovascular Risk in Young Finns Study. Pediatrics 2006, 118, 1553–1559. [Google Scholar] [CrossRef]
- Jin, R.; Welsh, J.A.; Le, N.-A.; Holzberg, J.; Sharma, P.; Martin, D.R.; Vos, M.B. Dietary Fructose Reduction Improves Markers of Cardiovascular Disease Risk in Hispanic-American Adolescents with NAFLD. Nutrients 2014, 6, 3187–3201. [Google Scholar] [CrossRef] [PubMed]
- Farías, C.; Cisternas, C.; Gana, J.C.; Alberti, G.; Echeverría, F.; Videla, L.A.; Mercado, L.; Muñoz, Y.; Valenzuela, R. Dietary and Nutritional Interventions in Nonalcoholic Fatty Liver Disease in Pediatrics. Nutrients 2023, 15, 4829. [Google Scholar] [CrossRef] [PubMed]
- Staltner, R.; Burger, K.; Baumann, A.; Bergheim, I. Fructose: A Modulator of Intestinal Barrier Function and Hepatic Health? Eur. J. Nutr. 2023, 62, 3113–3124. [Google Scholar] [CrossRef] [PubMed]
- Beleli, C.A.V.; Antonio, M.A.R.G.M.; Dos Santos, R.; Pastore, G.M.; Lomazi, E.A. Effect of 4′galactooligosaccharide on Constipation Symptoms. J. Pediatr. 2015, 91, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Dehghani, S.M.; Bahroloolomifard, M.S.; Yousefi, G.; Pasdaran, A.; Hamedi, A. A Randomized Controlled Double Blinded Trial to Evaluate Efficacy of Oral Administration of Black Strap Molasses (Sugarcane Extract) in Comparison with Polyethylene Glycol on Pediatric Functional Constipation. J. Ethnopharmacol. 2019, 238, 111845. [Google Scholar] [CrossRef]
- Tajik, P.; Goudarzian, A.H.; Shadnoush, M.; Bagheri, B. Effect of Red Sugar on Functional Constipation in Children Compared to Figs Syrup; a Randomized Controlled Trial Study. Gastroenterol. Hepatol. Bed Bench 2018, 11, 313–318. [Google Scholar]
- Llanos-Chea, A.; Fasano, A. Gluten and Functional Abdominal Pain Disorders in Children. Nutrients 2018, 10, 1491. [Google Scholar] [CrossRef] [PubMed]
- Francavilla, R.; Cristofori, F.; Verzillo, L.; Gentile, A.; Castellaneta, S.; Polloni, C.; Giorgio, V.; Verduci, E.; D’Angelo, E.; Dellatte, S.; et al. Randomized Double-Blind Placebo-Controlled Crossover Trial for the Diagnosis of Non-Celiac Gluten Sensitivity in Children. Am. J. Gastroenterol. 2018, 113, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Piwowarczyk, A.; Horvath, A.; Pisula, E.; Kawa, R.; Szajewska, H. Gluten-Free Diet in Children with Autism Spectrum Disorders: A Randomized, Controlled, Single-Blinded Trial. J. Autism Dev. Disord. 2020, 50, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Ghalichi, F.; Ghaemmaghami, J.; Malek, A.; Ostadrahimi, A. Effect of Gluten Free Diet on Gastrointestinal and Behavioral Indices for Children with Autism Spectrum Disorders: A Randomized Clinical Trial. World J. Pediatr. 2016, 12, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Fiori, F.; Bravo, G.; Neuhold, S.; Bartolone, G.; Pilo, C.; Parpinel, M.; Pellegrini, N. Compliance and Attitudes towards the Gluten-Free Diet in Celiac Patients in Italy: What Has Changed after a Decade? Nutrients 2024, 16, 2493. [Google Scholar] [CrossRef]
- Wang, X.; Anders, S.; Jiang, Z.; Bruce, M.; Gidrewicz, D.; Marcon, M.; Turner, J.M.; Mager, D.R. Food Insecurity Impacts Diet Quality and Adherence to the Gluten-free Diet in Youth with Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2024, 79, 1180–1191. [Google Scholar] [CrossRef] [PubMed]
- Rej, A.; Avery, A.; Ford, A.C.; Holdoway, A.; Kurien, M.; McKenzie, Y.; Thompson, J.; Trott, N.; Whelan, K.; Williams, M.; et al. Clinical Application of Dietary Therapies in Irritable Bowel Syndrome. J. Gastrointest. Liver Dis. 2018, 27, 307–316. [Google Scholar] [CrossRef] [PubMed]
- de Bruijn, C.M.; Rexwinkel, R.; Gordon, M.; Sinopoulou, V.; Benninga, M.A.; Tabbers, M.M. Dietary Interventions for Functional Abdominal Pain Disorders in Children: A Systematic Review and Meta-Analysis. Expert Rev. Gastroenterol. Hepatol. 2022, 16, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.K.; Rossi, M.; Bajka, B.; Whelan, K. Dietary Fibre in Gastrointestinal Health and Disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Axelrod, C.H.; Saps, M. The Role of Fiber in the Treatment of Functional Gastrointestinal Disorders in Children. Nutrients 2018, 10, 1650. [Google Scholar] [CrossRef]
- Tabbers, M.M.; DiLorenzo, C.; Berger, M.Y.; Faure, C.; Langendam, M.W.; Nurko, S.; Staiano, A.; Vandenplas, Y.; Benninga, M.A.; European Society for Pediatric Gastroenterology, Hepatology, and Nutrition; et al. Evaluation and Treatment of Functional Constipation in Infants and Children: Evidence-Based Recommendations from ESPGHAN and NASPGHAN. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 258–274. [Google Scholar] [CrossRef] [PubMed]
- Alfaro-Cruz, L.; Heitkemper, M.; Chumpitazi, B.P.; Shulman, R.J. Literature Review: Dietary Intervention Adherence and Adherence Barriers in Functional Gastrointestinal Disorder Studies. J. Clin. Gastroenterol. 2020, 54, 203–211. [Google Scholar] [CrossRef]
- Story, M.; Neumark-Sztainer, D.; French, S. Individual and Environmental Influences on Adolescent Eating Behaviors. J. Am. Diet. Assoc. 2002, 102, S40–S51. [Google Scholar] [CrossRef] [PubMed]
- Patrick, H.; Nicklas, T.A. A Review of Family and Social Determinants of Children’s Eating Patterns and Diet Quality. J. Am. Coll. Nutr. 2005, 24, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Arcila-Agudelo, A.M.; Ferrer-Svoboda, C.; Torres-Fernàndez, T.; Farran-Codina, A. Determinants of Adherence to Healthy Eating Patterns in a Population of Children and Adolescents: Evidence on the Mediterranean Diet in the City of Mataró (Catalonia, Spain). Nutrients 2019, 11, 854. [Google Scholar] [CrossRef]
- Burton, C.; Allan, E.; Eckhardt, S.; Grange, D.L.; Ehrenreich-May, J.; Singh, M.; Dimitropoulos, G. Case Presentations Combining Family-Based Treatment with the Unified Protocols for Transdiagnostic Treatment of Emotional Disorders in Children and Adolescents for Comorbid Avoidant Restrictive Food Intake Disorder and Autism Spectrum Disorder. J. Can. Acad. Child. Adolesc. Psychiatry 2021, 30, 280–291. [Google Scholar] [PubMed]
- Radziszewska, M.; Smarkusz-Zarzecka, J.; Ostrowska, L. Nutrition, Physical Activity and Supplementation in Irritable Bowel Syndrome. Nutrients 2023, 15, 3662. [Google Scholar] [CrossRef] [PubMed]
- Inan, M.; Aydiner, C.Y.; Tokuc, B.; Aksu, B.; Ayvaz, S.; Ayhan, S.; Ceylan, T.; Basaran, U.N. Factors Associated with Childhood Constipation. J. Paediatr. Child. Health 2007, 43, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Chien, L.-Y.; Liou, Y.M.; Chang, P. Low Defaecation Frequency in Taiwanese Adolescents: Association with Dietary Intake, Physical Activity and Sedentary Behaviour. J. Paediatr. Child. Health 2011, 47, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Ho, S.-Y.; Lo, W.-S.; Lam, T.-H. Physical Activity and Constipation in Hong Kong Adolescents. PLoS ONE 2014, 9, e90193. [Google Scholar] [CrossRef] [PubMed]
- Driessen, L.M.; Kiefte-de Jong, J.C.; Wijtzes, A.; de Vries, S.I.; Jaddoe, V.W.V.; Hofman, A.; Raat, H.; Moll, H.A. Preschool Physical Activity and Functional Constipation: The Generation R Study. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 768–774. [Google Scholar] [CrossRef]
- Johannesson, E.; Ringström, G.; Abrahamsson, H.; Sadik, R. Intervention to Increase Physical Activity in Irritable Bowel Syndrome Shows Long-Term Positive Effects. World J. Gastroenterol. 2015, 21, 600–608. [Google Scholar] [CrossRef]
- Sadeghian, M.; Sadeghi, O.; Hassanzadeh Keshteli, A.; Daghaghzadeh, H.; Esmaillzadeh, A.; Adibi, P. Physical Activity in Relation to Irritable Bowel Syndrome among Iranian Adults. PLoS ONE 2018, 13, e0205806. [Google Scholar] [CrossRef] [PubMed]
- Shahabi, L.; Naliboff, B.D.; Shapiro, D. Self-Regulation Evaluation of Therapeutic Yoga and Walking for Patients with Irritable Bowel Syndrome: A Pilot Study. Psychol. Health Med. 2016, 21, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, N.R.; Moorman, E.; Brown, C.M.; Mallon, D.; Chundi, P.K.; Mara, C.A.; Pentiuk, S.; Lynch-Jordan, A.M.; Dykes, D.M.H.; Elfers, J.; et al. Integrating Psychological Screening Into Medical Care for Youth with Abdominal Pain. Pediatrics 2018, 142, e20172876. [Google Scholar] [CrossRef]
- Liyanarachchi, H.; Rajindrajith, S.; Kuruppu, C.; Chathurangana, P.; Ranawaka, R.; Devanarayana, N.M.; Benninga, M.A. Association between Childhood Constipation and Exposure to Stressful Life Events: A Systematic Review. Neurogastroenterol. Motil. 2022, 34, e14231. [Google Scholar] [CrossRef]
- Bonnert, M.; Olén, O.; Lalouni, M.; Benninga, M.A.; Bottai, M.; Engelbrektsson, J.; Hedman, E.; Lenhard, F.; Melin, B.; Simrén, M.; et al. Internet-Delivered Cognitive Behavior Therapy for Adolescents with Irritable Bowel Syndrome: A Randomized Controlled Trial. Am. J. Gastroenterol. 2017, 112, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Van Oudenhove, L.; Crowell, M.D.; Drossman, D.A.; Halpert, A.D.; Keefer, L.; Lackner, J.M.; Murphy, T.B.; Naliboff, B.D.; Levy, R.L. Biopsychosocial Aspects of Functional Gastrointestinal Disorders. Gastroenterology 2016, 150, 1355–1367.e2. [Google Scholar] [CrossRef] [PubMed]
- Person, H.; Keefer, L. Psychological Comorbidity in Gastrointestinal Diseases: Update on the Brain-Gut-Microbiome Axis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 107, 110209. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-Y.; Chen, S.-N.; Lee, C.-H.; Huang, Y.-J. A Systematic Review and Meta-Analysis of Randomized Control Trials: Efficacy of Cognitive Behavioral Therapies for the Management of Functional and Recurrent Abdominal Pain Disorders in Children and Adolescents. Cogn. Behav. Ther. 2023, 52, 438–459. [Google Scholar] [CrossRef] [PubMed]
- Robins, P.M.; Smith, S.M.; Glutting, J.J.; Bishop, C.T. A Randomized Controlled Trial of a Cognitive-Behavioral Family Intervention for Pediatric Recurrent Abdominal Pain. J. Pediatr. Psychol. 2005, 30, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Jia, N.; Zhang, Y.; Hao, Y.; Xiao, F.; Sun, C.; Cui, X.; Wang, F. Effect of Cognitive-Behavior Therapy for Children with Functional Abdominal Pain: A Meta-Analysis. BMC Gastroenterol. 2024, 24, 62. [Google Scholar] [CrossRef]
- Hou, K.; Wu, Z.-X.; Chen, X.-Y.; Wang, J.-Q.; Zhang, D.; Xiao, C.; Zhu, D.; Koya, J.B.; Wei, L.; Li, J.; et al. Microbiota in Health and Diseases. Signal Transduct. Target. Ther. 2022, 7, 135. [Google Scholar] [CrossRef]
- Cho, K.Y. Association of Gut Microbiota with Obesity in Children and Adolescents. Clin. Exp. Pediatr. 2023, 66, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Geng, J.; Ni, Q.; Sun, W.; Li, L.; Feng, X. The Links between Gut Microbiota and Obesity and Obesity Related Diseases. Biomed. Pharmacother. 2022, 147, 112678. [Google Scholar] [CrossRef] [PubMed]
- Shin, A.; Preidis, G.A.; Shulman, R.; Kashyap, P.C. The Gut Microbiome in Adult and Pediatric Functional Gastrointestinal Disorders. Clin. Gastroenterol. Hepatol. 2019, 17, 256–274. [Google Scholar] [CrossRef]
- Chen, X.; Sun, H.; Jiang, F.; Shen, Y.; Li, X.; Hu, X.; Shen, X.; Wei, P. Alteration of the Gut Microbiota Associated with Childhood Obesity by 16S rRNA Gene Sequencing. PeerJ 2020, 8, e8317. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, C.C.; Monteil, M.A.; Davis, E.M. Overweight and Obesity in Children Are Associated with an Abundance of Firmicutes and Reduction of Bifidobacterium in Their Gastrointestinal Microbiota. Child. Obes. 2020, 16, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-M.; Lv, Q.; Chen, Y.-J.; Yan, L.-B.; Xiong, X. Association between Childhood Obesity and Gut Microbiota: 16S rRNA Gene Sequencing-Based Cohort Study. World J. Gastroenterol. 2024, 30, 2249–2257. [Google Scholar] [CrossRef] [PubMed]
- Rajilić–Stojanović, M.; Biagi, E.; Heilig, H.G.H.J.; Kajander, K.; Kekkonen, R.A.; Tims, S.; De Vos, W.M. Global and Deep Molecular Analysis of Microbiota Signatures in Fecal Samples from Patients with Irritable Bowel Syndrome. Gastroenterology 2011, 141, 1792–1801. [Google Scholar] [CrossRef]
- Chumpitazi, B.P.; Shulman, R.J. Underlying Molecular and Cellular Mechanisms in Childhood Irritable Bowel Syndrome. Mol. Cell Pediatr. 2016, 3, 11. [Google Scholar] [CrossRef] [PubMed]
- Saulnier, D.M.; Ringel, Y.; Heyman, M.B.; Foster, J.A.; Bercik, P.; Shulman, R.J.; Versalovic, J.; Verdu, E.; Dinan, T.G.; Hecht, G.; et al. The Intestinal Microbiome, Probiotics and Prebiotics in Neurogastroenterology. Gut Microbes 2013, 4, 17–27. [Google Scholar] [CrossRef]
- Bin Waqar, S.H.; Rehan, A. Methane and Constipation-Predominant Irritable Bowel Syndrome: Entwining Pillars of Emerging Neurogastroenterology. Cureus 2019, 11, e4764. [Google Scholar] [CrossRef]
- De Meij, T.G.J.; De Groot, E.F.J.; Eck, A.; Budding, A.E.; Kneepkens, C.M.F.; Benninga, M.A.; Van Bodegraven, A.A.; Savelkoul, P.H.M. Characterization of Microbiota in Children with Chronic Functional Constipation. PLoS ONE 2016, 11, e0164731. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Liu, W.; Alkhouri, R.; Baker, R.D.; Bard, J.E.; Quigley, E.M.; Baker, S.S. Structural Changes in the Gut Microbiome of Constipated Patients. Physiol. Genom. 2014, 46, 679–686. [Google Scholar] [CrossRef]
- Zoppi, G.; Cinquetti, M.; Luciano, A.; Benini, A.; Muner, A.; Minelli, E.B. The Intestinal Ecosystem in Chronic Functional Constipation. Acta Paediatr. 1998, 87, 836–841. [Google Scholar] [CrossRef]
- Brown, S.C.; Whelan, K.; Gearry, R.B.; Day, A.S. Low FODMAP Diet in Children and Adolescents with Functional Bowel Disorder: A Clinical Case Note Review. JGH Open 2020, 4, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Horvath, A.; Dziechciarz, P.; Szajewska, H. Meta-Analysis: Lactobacillus Rhamnosus GG for Abdominal Pain-Related Functional Gastrointestinal Disorders in Childhood. Aliment. Pharmacol. Ther. 2011, 33, 1302–1310. [Google Scholar] [CrossRef] [PubMed]
- FAO. Joint FAO/WHO Expert Consultation on Evaluation of Health and Nutritional Properties of Probiotics in Food Including Powder Milk with Live Lactic Acid Bacteria; FAO: Rome, Italy, 2002; p. 34. [Google Scholar]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. The International Scientific Association for Probiotics and Prebiotics Consensus Statement on the Scope and Appropriate Use of the Term Probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef]
- Sánchez, B.; Delgado, S.; Blanco-Míguez, A.; Lourenço, A.; Gueimonde, M.; Margolles, A. Probiotics, Gut Microbiota, and Their Influence on Host Health and Disease. Mol. Nutr. Food Res. 2017, 61, 1600240. [Google Scholar] [CrossRef] [PubMed]
- Derrien, M.; van Hylckama Vlieg, J.E.T. Fate, Activity, and Impact of Ingested Bacteria within the Human Gut Microbiota. Trends Microbiol. 2015, 23, 354–366. [Google Scholar] [CrossRef] [PubMed]
- Bu, L.-N.; Chang, M.-H.; Ni, Y.-H.; Chen, H.-L.; Cheng, C.-C. Lactobacillus casei rhamnosus Lcr35 in Children with Chronic Constipation. Pediatr. Int. 2007, 49, 485–490. [Google Scholar] [CrossRef]
- Kubota, M.; Ito, K.; Tomimoto, K.; Kanazaki, M.; Tsukiyama, K.; Kubota, A.; Kuroki, H.; Fujita, M.; Vandenplas, Y. Lactobacillus reuteri DSM 17938 and Magnesium Oxide in Children with Functional Chronic Constipation: A Double-Blind and Randomized Clinical Trial. Nutrients 2020, 12, 225. [Google Scholar] [CrossRef] [PubMed]
- García Contreras, A.A.; Vásquez Garibay, E.M.; Sánchez Ramírez, C.A.; Fafutis Morris, M.; Delgado Rizo, V. Lactobacillus reuteri DSM 17938 and Agave Inulin in Children with Cerebral Palsy and Chronic Constipation: A Double-Blind Randomized Placebo Controlled Clinical Trial. Nutrients 2020, 12, 2971. [Google Scholar] [CrossRef] [PubMed]
- Putignani, L.; Del Chierico, F.; Vernocchi, P.; Cicala, M.; Cucchiara, S.; Dallapiccola, B.; Dysbiotrack Study Group. Gut Microbiota Dysbiosis as Risk and Premorbid Factors of IBD and IBS Along the Childhood-Adulthood Transition. Inflamm. Bowel Dis. 2016, 22, 487–504. [Google Scholar] [CrossRef]
- Closa-Monasterolo, R.; Ferré, N.; Castillejo-DeVillasante, G.; Luque, V.; Gispert-Llaurado, M.; Zaragoza-Jordana, M.; Theis, S.; Escribano, J. The Use of Inulin-Type Fructans Improves Stool Consistency in Constipated Children. A Randomised Clinical Trial: Pilot Study. Int. J. Food Sci. Nutr. 2017, 68, 587–594. [Google Scholar] [CrossRef]
- Lohner, S.; Jakobik, V.; Mihályi, K.; Soldi, S.; Vasileiadis, S.; Theis, S.; Sailer, M.; Sieland, C.; Berényi, K.; Boehm, G.; et al. Inulin-Type Fructan Supplementation of 3- to 6-Year-Old Children Is Associated with Higher Fecal Bifidobacterium Concentrations and Fewer Febrile Episodes Requiring Medical Attention. J. Nutr. 2018, 148, 1300–1308. [Google Scholar] [CrossRef] [PubMed]
- Abot, A.; Wemelle, E.; Laurens, C.; Paquot, A.; Pomie, N.; Carper, D.; Bessac, A.; Mas Orea, X.; Fremez, C.; Fontanie, M.; et al. Identification of New Enterosynes Using Prebiotics: Roles of Bioactive Lipids and Mu-Opioid Receptor Signalling in Humans and Mice. Gut 2021, 70, 1078–1087. [Google Scholar] [CrossRef]
- Everard, A.; Lazarevic, V.; Derrien, M.; Girard, M.; Muccioli, G.G.; Neyrinck, A.M.; Possemiers, S.; Van Holle, A.; François, P.; De Vos, W.M.; et al. Responses of Gut Microbiota and Glucose and Lipid Metabolism to Prebiotics in Genetic Obese and Diet-Induced Leptin-Resistant Mice. Diabetes 2011, 60, 2775–2786. [Google Scholar] [CrossRef]
- Cani, P.D.; Possemiers, S.; Van de Wiele, T.; Guiot, Y.; Everard, A.; Rottier, O.; Geurts, L.; Naslain, D.; Neyrinck, A.; Lambert, D.M.; et al. Changes in Gut Microbiota Control Inflammation in Obese Mice through a Mechanism Involving GLP-2-Driven Improvement of Gut Permeability. Gut 2009, 58, 1091–1103. [Google Scholar] [CrossRef]
- Cani, P.D.; Knauf, C.; Iglesias, M.A.; Drucker, D.J.; Delzenne, N.M.; Burcelin, R. Improvement of Glucose Tolerance and Hepatic Insulin Sensitivity by Oligofructose Requires a Functional Glucagon-like Peptide 1 Receptor. Diabetes 2006, 55, 1484–1490. [Google Scholar] [CrossRef]
- Kokke, F.T.M.; Scholtens, P.A.M.J.; Alles, M.S.; Decates, T.S.; Fiselier, T.J.W.; Tolboom, J.J.M.; Kimpen, J.L.L.; Benninga, M.A. A Dietary Fiber Mixture versus Lactulose in the Treatment of Childhood Constipation: A Double-Blind Randomized Controlled Trial. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 592–597. [Google Scholar] [CrossRef]
- Han, Y.; Zhang, L.; Liu, X.-Q.; Zhao, Z.-J.; Lv, L.-X. Effect of Glucomannan on Functional Constipation in Children: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Asia Pac. J. Clin. Nutr. 2017, 26, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.; Simeone, D.; Del Giudice, E.; Miele, E.; Tozzi, A.; Toraldo, C. Effect of the Dietary Fiber Glucomannan on Chronic Constipation in Neurologically Impaired Children. J. Pediatr. 2000, 136, 41–45. [Google Scholar] [CrossRef]
- Barbara, G.; Cremon, C.; Bellini, M.; Corsetti, M.; Di Nardo, G.; Falangone, F.; Fuccio, L.; Galeazzi, F.; Iovino, P.; Sarnelli, G.; et al. Italian Guidelines for the Management of Irritable Bowel Syndrome: Joint Consensus from the Italian Societies of: Gastroenterology and Endoscopy (SIGE), Neurogastroenterology and Motility (SINGEM), Hospital Gastroenterologists and Endoscopists (AIGO), Digestive Endoscopy (SIED), General Medicine (SIMG), Gastroenterology, Hepatology and Pediatric Nutrition (SIGENP) and Pediatrics (SIP). Dig. Liver Dis. 2023, 55, 187–207. [Google Scholar] [CrossRef] [PubMed]
- Baştürk, A.; Artan, R.; Atalay, A.; Yılmaz, A. Investigation of the Efficacy of Synbiotics in the Treatment of Functional Constipation in Children: A Randomized Double-Blind Placebo-Controlled Study. Turk. J. Gastroenterol. 2017, 28, 388–393. [Google Scholar] [CrossRef]
- Vieira, A.T.; Fukumori, C.; Ferreira, C.M. New Insights into Therapeutic Strategies for Gut Microbiota Modulation in Inflammatory Diseases. Clin. Transl. Immunol. 2016, 5, e87. [Google Scholar] [CrossRef] [PubMed]
- Dehzad, M.J.; Ghalandari, H.; Nouri, M.; Askarpour, M. Antioxidant and Anti-Inflammatory Effects of Curcumin/Turmeric Supplementation in Adults: A GRADE-Assessed Systematic Review and Dose-Response Meta-Analysis of Randomized Controlled Trials. Cytokine 2023, 164, 156144. [Google Scholar] [CrossRef]
- Nohynek, L.J.; Alakomi, H.-L.; Kähkönen, M.P.; Heinonen, M.; Helander, I.M.; Oksman-Caldentey, K.-M.; Puupponen-Pimiä, R.H. Berry Phenolics: Antimicrobial Properties and Mechanisms of Action Against Severe Human Pathogens. Nutr. Cancer 2006, 54, 18–32. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, M.; Kheirouri, S. Curcumin Reduces Malondialdehyde and Improves Antioxidants in Humans with Diseased Conditions: A Comprehensive Meta-Analysis of Randomized Controlled Trials. BioMedicine 2019, 9, 23. [Google Scholar] [CrossRef] [PubMed]
- Scazzocchio, B.; Minghetti, L.; D’Archivio, M. Interaction between Gut Microbiota and Curcumin: A New Key of Understanding for the Health Effects of Curcumin. Nutrients 2020, 12, 2499. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Nishikawa, S.; Ikehata, A.; Dochi, K.; Tani, T.; Takahashi, T.; Imaizumi, A.; Tsuda, T. Curcumin Improves Glucose Tolerance via Stimulation of Glucagon-like Peptide-1 Secretion. Mol. Nutr. Food Res. 2017, 61, 1600471. [Google Scholar] [CrossRef] [PubMed]
- Suskind, D.L.; Wahbeh, G.; Burpee, T.; Cohen, M.; Christie, D.; Weber, W. Tolerability of Curcumin in Pediatric Inflammatory Bowel Disease: A Forced-Dose Titration Study. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 277–279. [Google Scholar] [CrossRef]
- Jafarzadeh, E.; Shoeibi, S.; Bahramvand, Y.; Nasrollahi, E.; Maghsoudi, A.S.; Yazdi, F.; KarkonShayan, S.; Hassani, S. Turmeric for Treatment of Irritable Bowel Syndrome: A Systematic Review of Population-Based Evidence. Iran. J. Public Health 2022, 51, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, B.B.; Sung, B. Pharmacological Basis for the Role of Curcumin in Chronic Diseases: An Age-Old Spice with Modern Targets. Trends Pharmacol. Sci. 2009, 30, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Stohs, S.J.; Chen, O.; Ray, S.D.; Ji, J.; Bucci, L.R.; Preuss, H.G. Highly Bioavailable Forms of Curcumin and Promising Avenues for Curcumin-Based Research and Application: A Review. Molecules 2020, 25, 1397. [Google Scholar] [CrossRef] [PubMed]
- Altveş, S.; Yildiz, H.K.; Vural, H.C. Interaction of the Microbiota with the Human Body in Health and Diseases. Biosci. Microbiota Food Health 2020, 39, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Jabczyk, M.; Nowak, J.; Hudzik, B.; Zubelewicz-Szkodzińska, B. Curcumin and Its Potential Impact on Microbiota. Nutrients 2021, 13, 2004. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Chaturvedi, M.; Mishra, S.; Kumar, P.; Somvanshi, P.; Chaturvedi, R. Reductive Metabolites of Curcumin and Their Therapeutic Effects. Heliyon 2020, 6, e05469. [Google Scholar] [CrossRef] [PubMed]
- Jazayeri, S.D.; Shuhaimi, M.; Abd Manap, Y.; Ali, A. Survival of Bifidobacteria and Other Selected Intestinal Bacteria in TPY Medium Supplemented with Curcumin as Assessed in Vitro. Int. J. Probiotics Prebiotics 2009, 4, 15–22. [Google Scholar]
- Servida, S.; Piontini, A.; Gori, F.; Tomaino, L.; Moroncini, G.; De Gennaro Colonna, V.; La Vecchia, C.; Vigna, L. Curcumin and Gut Microbiota: A Narrative Overview with Focus on Glycemic Control. Int. J. Mol. Sci. 2024, 25, 7710. [Google Scholar] [CrossRef]
- Ng, Q.X.; Soh, A.Y.S.; Loke, W.; Venkatanarayanan, N.; Lim, D.Y.; Yeo, W.-S. A Meta-Analysis of the Clinical Use of Curcumin for Irritable Bowel Syndrome (IBS). J. Clin. Med. 2018, 7, 298. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).