
Beyond BMI: Exploring Adolescent Lifestyle and Health Behaviours in Transylvania, Romania

 ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection and Questionnaire Measurements
2.3. Ethical Considerations
2.4. Statistical Analyses
3. Results
3.1. Demographic Characteristics of the Study Group
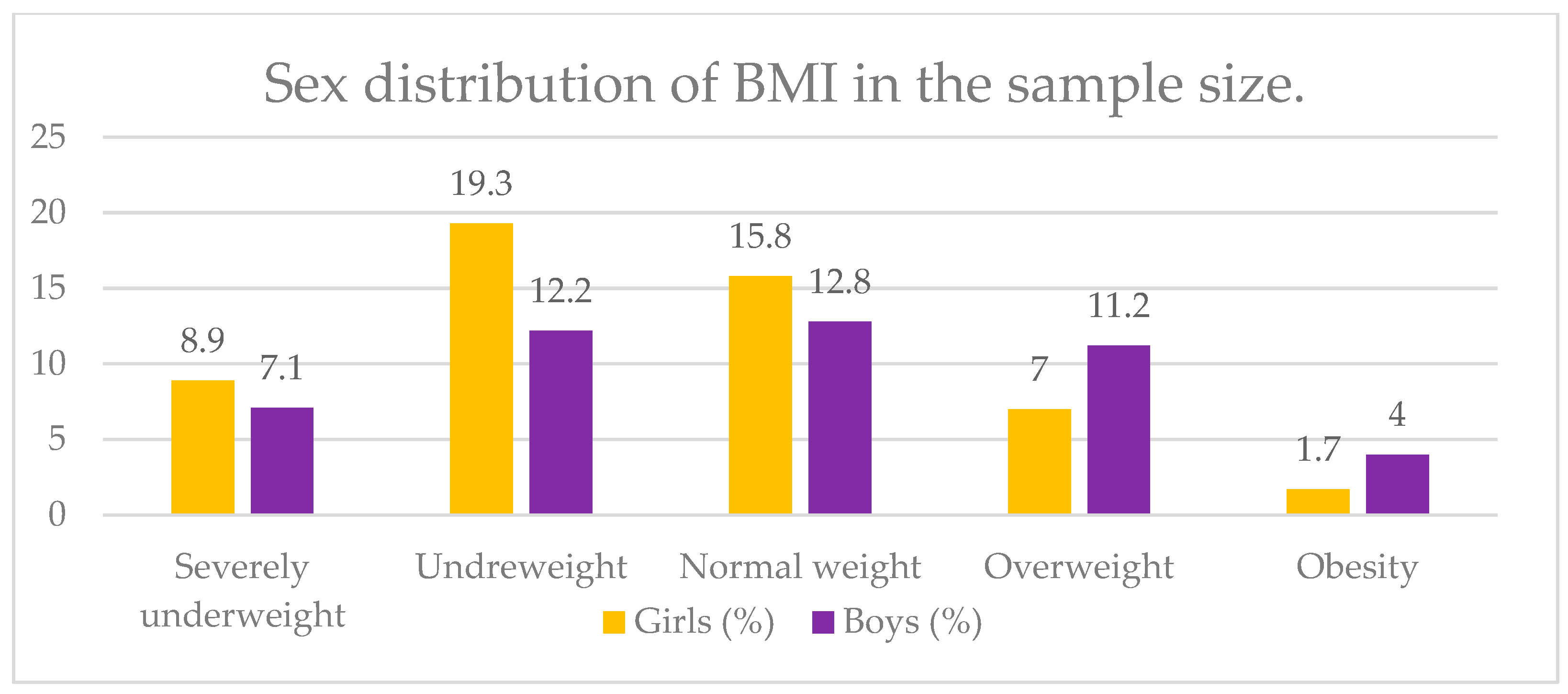
3.2. Assessment of Nutritional Status and Health Status
3.3. Dietary Behaviors
3.4. Addictive Behaviors—Alcohol, Cigarette and Drug Consumption
3.5. Physical Activity and Sedentary Behaviors
3.6. Hours Spent in Front of the Computer (Screen Time) and Social Networks
3.7. Hygiene—Oral Health and Washing Hands
3.8. Factors Associated with Nutritional Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Coming of Age: Adolescent Health. 2021. Available online: https://www.who.int/news-room/spotlight/coming-of-age-adolescent-health (accessed on 26 October 2024).
- Achak, D.; Azizi, A.; El-Ammari, A.; Marfak, I.Y.; Saad, E.; Nejjari, C.; Hilali, A.; Peltzer, K.; Marfak, A. The health behaviors differences among male and female school-age adolescents in the Middle East and North Africa region countries: A meta-analysis of the Global School-based Student Health Survey data. Front. Public Health 2024, 12, 1448386. [Google Scholar] [CrossRef] [PubMed]
- Abdalmaleki, E.; Abdi, Z.; Isfahani, S.R.; Safarpoor, S.; Haghdoost, B.; Sazgarnejad, S.; Ahmadnezhad, E. Global school-based student health survey: Country profiles and survey results in the eastern Mediterranean region countries. BMC Public Health 2022, 22, 130. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Status Report on Noncommunicable Diseases 2014. World Health Organization. Available online: https://www.who.int/publications/i/item/9789241564854 (accessed on 26 October 2024).
- United Nations International Children’s Emergency Fund (UNICEF). Non-Communicable Diseases Are Critically Important for Adolescents Now and in the Future. 2021. Available online: https://data.unicef.org/topic/child-health/noncommunicable-diseases/ (accessed on 26 October 2024).
- United Nations International Children’s Emergency Fund (UNICEF). Non-Communicable Diseases. Behaviours That Lead to Disease Often Emerge During Childhood and Adolescence. Available online: https://www.unicef.org/health/non-communicable-diseases (accessed on 26 October 2024).
- Çam, H.H.; Top, F.U. Prevalence and determinants of behavioral risk factors for noncommunicable diseases among students aged 13–19 years in Turkey. Arch. Pediatr. 2024, 31, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Maheshwari, A.; Sharma, N.; Anand, K. Lifestyle associated risk factors in adolescents. Indian J. Pediatr. 2006, 73, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Yogesh, M.; Kagathara, N.; Ram, R.; Misra, S.; Kagathara, J. Exploring Behavioral Risk Factors for Non-communicable Diseases Among Undergraduate Medical Students in Western Gujarat: A Cross-Sectional Study. Cureus 2023, 15, e49188. [Google Scholar]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Noncommunicable Disease Surveillance, Monitoring and Reporting. Available online: https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/global-school-based-student-health-survey (accessed on 26 October 2024).
- Baker, R.; Taylor, E.; Essafi, S.; Jarvis, J.D.; Odok, C. Engaging young people in the prevention of noncommunicable diseases. Bull. World Health Organ. 2016, 94, 484. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, G.; Petrou, I.; Manou, M.; Tragomalou, A.; Ramouzi, E.; Vourdoumpa, A.; Genitsaridi, S.-M.; Kyrkili, A.; Diou, C.; Papadopoulou, M.; et al. Dietary and Physical Activity Habits of Children and Adolescents before and after the Implementation of a Personalized, Intervention Program for the Management of Obesity. Nutrients 2024, 16, 3477. [Google Scholar] [CrossRef] [PubMed]
- Roșioară, A.-I.; Năsui, B.A.; Ciuciuc, N.; Sîrbu, D.M.; Curșeu, D.; Pop, A.L.; Popescu, C.A.; Popa, M. Status of Healthy Choices, Attitudes and Health Education of Children and Young People in Romania—A Literature Review. Medicina 2024, 60, 725. [Google Scholar] [CrossRef] [PubMed]
- Pop, T.L.; Burlea, M.; Falup-Pecurariu, O.; Borzan, C.; Gabor-Harosa, F.; Herdea, V.; Pop, C.F.; Rajka, D.; Ognean, M.L.; Căinap, S.S. Overview of the pediatric healthcare system in Romania. Turk. Pediatr. Ars. 2020, 55, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Song, J.; MacGregor, G.A.; He, F.J. Consumption of Soft Drinks and Overweight and Obesity Among Adolescents in 107 Countries and Regions. JAMA Netw. Open 2023, 6, e2325158. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Lopez Sanchez, G.F.; Tully, M.A.; Rahmati, M.; Oh, H.; Kostev, K.; Butler, L.T.; Barnett, Y.; Keyes, H.; Shin, J.I.; et al. Temporal trends of carbonated soft-drink consumption among adolescents aged 12–15 years from eighteen countries in Africa, Asia and the Americas. Br. J. Nutr. 2024, 131, 1633–1640. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, G.J.; Mendes, A.E.P.; Costa, E.A.; Carvalho, D.V. Trends in food consumption by adults in a Brazilian northeastern state. J. Taibah Univ. Med. Sci. 2023, 18, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Bere, E.; Sørli Glomnes, E.; te Velde, S.J.; Klepp, K.-I. Determinants of adolescents’ soft drink consumption. Public Health Nutr. 2008, 11, 49–56. [Google Scholar] [CrossRef] [PubMed]
- da Silva, A.G.; Souza, J.B.; Gomes, C.S.; da Silva, T.P.R.; de Sá, A.C.M.G.N.; Malta, D.C. Multiple behavioral risk factors for non-communicable diseases among the adolescent population in Brazil: The analysis derived from the Brazilian national survey of school health 2019. BMC Pediatr. 2024, 24, 122. [Google Scholar] [CrossRef] [PubMed]
- Nasui, B.A.; Ungur, R.A.; Nasui, G.A.; Popescu, C.A.; Hofer, A.M.; Dersidan, S.; Popa, M.; Silaghi, H.; Silaghi, C.A. Adolescents’ Lifestyle Determinants in Relation to Their Nutritional Status during COVID-19 Pandemic Distance Learning in the North-Western Part of Romania—A Cross-Sectional Study. Children 2023, 10, 922. [Google Scholar] [CrossRef] [PubMed]
- Mititelu, M.; Stanciu, G.; Licu, M.; Neacșu, S.M.; Călin, M.F.; Roșca, A.C.; Stanciu, T.I.; Busnatu, Ș.S.; Olteanu, G.; Boroghină, S.C.; et al. Evaluation of the Consumption of Junk Food Products and Lifestyle among Teenagers and Young Population from Romania. Nutrients 2024, 16, 1769. [Google Scholar] [CrossRef] [PubMed]
- Beal, T.; Morris, S.S.; Tumilowicz, A. Global Patterns of Adolescent Fruit, Vegetable, Carbonated Soft Drink, and Fast-Food Consumption: A Meta-Analysis of Global School-Based Student Health Surveys. Food Nutr. Bull. 2019, 40, 444–459. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation 2020. Healthy Diet. Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet#:~:text=A%20healthy%20diet%20includes%20the,cassava%20and%20other%20starchy%20roots (accessed on 5 January 2025).
- Mielgo-Ayuso, J.; Valtueña, J.; Huybrechts, I.; Breidenassel, C.; Cuenca-García, M.; De Henauw, S.; Stehle, P.; Kafatos, A.; Kersting, M.; Widhalm, K.; et al. Fruit and vegetables consumption is associated with higher vitamin intake and blood vitamin status among European adolescents. Eur. J. Clin. Nutr. 2017, 71, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Pem, D.; Jeewon, R. Fruit and Vegetable Intake: Benefits and Progress of Nutrition Education Interventions- Narrative Review Article. Iran J. Public Health. 2015, 44, 1309–1321. [Google Scholar] [PubMed] [PubMed Central]
- Win, T.Z.; Kamiya, Y.; Sheng Ng, C.F.; Smith, C.; Han, S.M. Lifestyle Risk Behaviours and Nutritional Status Associated with Mental Health Problems among Myanmar Adolescents: Secondary Analysis of a Nationwide 2016 School Survey. Int. J. Environ. Res. Public Health 2023, 20, 6660. [Google Scholar] [CrossRef] [PubMed]
- Rosi, A.; Scazzina, F.; Giampieri, F.; Abdelkarim, O.; Aly, M.; Pons, J.; Vázquez-Araújo, L.; Frias-Toral, E.; Cano, S.S.; Elío, I.; et al. Adherence to the Mediterranean diet in 5 Mediterranean countries: A descriptive analysis of the DELICIOUS project. Mediterr. J. Nutr. Metab. 2024, 17. [Google Scholar] [CrossRef]
- Barbu, C.G.; Teleman, M.D.; Albu, A.I.; Sirbu, A.E.; Martin, S.C.; Bancescu, A.; Fica, S.V. Obesity and eating behaviors in school children and adolescents –data from a cross-sectional study from Bucharest, Romania. BMC Public Health 2015, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; López Sánchez, G.F.; Tully, M.A.; Jacob, L.; Kostev, K.; Oh, H.; Butler, L.; Barnett, Y.; Shin, J.I.; Koyanagi, A. Temporal Trends in Food Insecurity (Hunger) among School-Going Adolescents from 31 Countries from Africa, Asia, and the Americas. Nutrients 2023, 15, 3226. [Google Scholar] [CrossRef] [PubMed]
- Prevalence of Moderate or Severe Food Insecurity in the Population (%)—Romania. World Bank Group. Available online: https://data.worldbank.org/indicator/SN.ITK.MSFI.ZS?locations=RO (accessed on 1 December 2024).
- Global Hunger Index. 2024. Available online: https://www.globalhungerindex.org/romania.html (accessed on 5 January 2025).
- World Health Organization (WHO). WHO Guidelines on Physical Activity and Sedentary Behaviour. 2020. Available online: https://iris.who.int/bitstream/handle/10665/337001/9789240014886-eng.pdf (accessed on 26 October 2024).
- Tremblay, M.S.; Carson, V.; Chaput, J.-P.; Gorber, S.C.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-h Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41 (Suppl. 3), S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Abonie, U.S.; Ackah, M. Prevalence and disparities in adolescents’ sedentary behavior from twenty-three African countries: Evidence from World Health Organization Global School-based Student Health Survey. Public Health 2024, 231, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Matheson, A.; Lambrick, D.; Faulkner, J.; Lounsbury, D.W.; Vaidya, A.; Page, R. Dietary practices, physical activity and social determinants of non-communicable diseases in Nepal: A systemic analysis. PLoS ONE 2023, 18, e0281355. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Saunders, D.H.; Shenkin, S.D.; Sproule, J. Lifestyle intervention for improving school achievement in overweight or obese children and adolescents. Cochrane Database Syst. Rev. 2014, CD009728. [Google Scholar] [CrossRef] [PubMed]
- Romanian Parliament. Law on Health Reform. No 65 of 22 March 2022 on the Completion of Law No 95/2006 Published in Official Journal of Romania (Monitorul Oficial) No. 281/23 March 2022. Available online: https://legislatie.just.ro/Public/DetaliiDocumentAfis/253114 (accessed on 5 January 2025). (In Romanian)
- National Anti-Drog Agency. Romania, Below the European Average in Drug Consumption Among Adolescents. Available online: https://ana.gov.ro/wp-content/uploads/2025/01/ESPAD-2019_3.pdf (accessed on 5 January 2025).
- Albert-Lőrincz, E.; Paulik, E.; Szabo, B.; Foley, K.; Gasparik, A.I. Adolescent smoking and the social capital of local communities in three counties in Romania. Gac. Sanit. 2019, 33, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Sârbu, E.A.; Marici, M.; Bostan, S.; Gavrila-Ardelean, L. Physical and Recreational Activities, Sedentary Screen Time, Time Spent with Parents and Drug Use in Adolescents. Int. J. Environ. Res. Public Health 2023, 20, 1434. [Google Scholar] [CrossRef] [PubMed]
- UNICEF Romania. Country Program for UNICEF in Romania 2023–2027. Available online: https://www.unicef.org/romania/media/13026/file/Programul%20de%20%C8%9Bar%C4%83%20pentru%20UNICEF%20%C3%AEn%20Rom%C3%A2nia%202023-2027.pdf (accessed on 26 October 2024). (In Romanian).
- The School Population in the National Education System was 3.47 Million Pupils and Students in the Year 2022/2023. Available online: https://www.agerpres.ro/economic/2023/06/20/populatia-scolara-din-sistemul-national-de-educatie-a-fost-de-3-47-milioane-de-elevi-si-studenti-in-anul-2022-2023--1126750#:~:text=Popula%C5%A3ia%20%C5%9Fcolar%C4%83%20din%20sistemul%20na%C5%A3ional,INTERNE (accessed on 26 October 2024). (In Romanian).
- Ministry of Education. Report Regarding the Condition of the Preuniversity Education from Romania 2022–2023. Available online: https://www.edu.ro/sites/default/files/_fi%C8%99iere/Minister/2023/Transparenta/Rapoarte_sistem/Raport-Starea-invatamantului-preuniversitar-2022-2023.pdf (accessed on 26 October 2024). (In Romanian)
- World Health Organization (WHO). Tools and Toolkits/Growth Reference Data for 5–19 Years/Indicators/BMI-for-Age (5–19 Years). Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age (accessed on 26 October 2024).
- Eurostat. Statistics Explained. Self-Perceived Health Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Self-perceived_health_statistics (accessed on 1 December 2024).
- Lange, S.J.; Moore, L.V.; Harris, D.M.; Merlo, C.L.; Lee, S.H.; Demissie, Z.; Galuska, D.A. Percentage of Adolescents Meeting Federal Fruit and Vegetable Intake Recommendations—Youth Risk Behavior Surveillance System, United States, 2017. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Zakrzewski-Fruer, J.K.; Seall, C.; Tolfrey, K. Breakfast Consumption Suppresses Appetite but Does Not Increase Daily Energy Intake or Physical Activity Energy Expenditure When Compared with Breakfast Omission in Adolescent Girls Who Habitually Skip Breakfast: A 7-Day Randomised Crossover Trial. Nutrients 2021, 13, 4261. [Google Scholar] [CrossRef] [PubMed]
- Pop, T.L.; Maniu, D.; Rajka, D.; Lazea, C.; Cismaru, G.; Ştef, A.; Căinap, S.S. Prevalence of Underweight, Overweight and Obesity in School-Aged Children in the Urban Area of the Northwestern Part of Romania. Int. J. Environ. Res. Public Health 2021, 18, 5176. [Google Scholar] [CrossRef] [PubMed]
- Rădulescu, C.; Ghiorghiu, I.A.; Plesca, D.A. Prevalence and possible complications of pediatric obesity in Romania: A review of recent literature. Rom. J. Pediatr. 2020, 69, 5–12. [Google Scholar] [CrossRef]
- Luca, A.-C.; Curpan, A.-S.; Braha, E.E.; Ţarcă, E.; Iordache, A.-C.; Luca, F.-A.; Adumitrachioaiei, H. Increasing Trends in Obesity-Related Cardiovascular Risk Factors in Romanian Children and Adolescents—Retrospective Study. Healthcare 2022, 10, 2452. [Google Scholar] [CrossRef] [PubMed]
- Miron, V.D.; Bar, G.; Filimon, C.; Gaidamut, V.A.; Craiu, M. Monitoring of Excess Body Weight in Children in the Emergency Department of a Tertiary Pediatric Hospital in Bucharest, Romania. Maedica 2021, 16, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Paştiu, C.A.; Maican, S.Ş.; Dobra, I.B.; Muntean, A.C.; Haţegan, C. Food insecurity among consumers from rural areas in Romania. Front. Nutr. 2024, 10, 1345729. [Google Scholar] [CrossRef] [PubMed]
- Heinen, M.M.; Bel-Serrat, S.; Kelleher, C.C.; Buoncristiano, M.; Spinelli, A.; Nardone, P.; Milanović, S.M.; Rito, A.I.; Bosi, A.T.B.; Gutiérrrez-González, E.; et al. Urban and rural differences in frequency of fruit, vegetable, and soft drink consumption among 6–9-year-old children from 19 countries from the WHO European region. Obes Rev. 2021, 22 (Suppl. 6), e13207. [Google Scholar] [CrossRef] [PubMed]
- Wijnhoven, T.M.; van Raaij, J.M.; Yngve, A.; Sjöberg, A.; Kunešová, M.; Duleva, V.; Petrauskiene, A.; Rito, A.I.; Breda, J. WHO European Childhood Obesity Surveillance Initiative: Health-risk behaviours on nutrition and physical activity in 6–9-year-old schoolchildren. Public Health Nutr. 2015, 18, 3108–3124. [Google Scholar] [CrossRef] [PubMed]
- Anton-Păduraru, D.-T.; Gotcă, I.; Mocanu, V.; Popescu, V.; Iliescu, M.-L.; Miftode, E.-G.; Boiculese, V.-L. Assessment of Eating Habits and Perceived Benefits of Physical Activity and Body Attractiveness among Adolescents from Northeastern Romania. Appl. Sci. 2021, 11, 11042. [Google Scholar] [CrossRef]
- Stoica, R.A.; Diaconu, C.C.; Rizzo, M.; Toth, P.P.; Stefan, S.D.; Serafinceanu, C.; Nikolic, D.; Poiana, C.; Ionescu-Tirgoviste, C.; Pantea-Stoian, A. Weight loss programmes using low carbohydrate diets to control the cardiovascular risk in adolescents (Review). Exp. Ther. Med. 2021, 21, 90. [Google Scholar] [CrossRef] [PubMed]
- Antonogeorgos, G.; Kogias, C.; Douros, K.; Panagiotakos, D. Greater fruit and vegetables consumption, and adherence to a Mediterranean type of diet reduces the risk for asthma in children; a systematic review and meta-analysis. Int. J. Food Sci. Nutr. 2024, 75, 4–30. [Google Scholar] [CrossRef]
- Nguyen, M.; Jarvis, S.E.; Chiavaroli, L.; Mejia, S.B.; Zurbau, A.; Khan, T.A.; Tobias, D.K.; Willett, W.C.; Hu, F.B.; Hanley, A.J.; et al. Consumption of 100% Fruit Juice and Body Weight in Children and Adults: A Systematic Review and Meta-Analysis. JAMA Pediatr. 2024, 178, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Mensink, G.B.M.; Schienkiewitz, A.; Rabenberg, M.; Borrmann, A.; Richter, A.; Haftenberger, M. Consumption of sugary soft drinks among children and adolescents in Germany. Results of the cross-sectional KiGGS Wave 2 study and trends. J. Health Monit. 2018, 3, 31–37. [Google Scholar]
- Schneider, S.; Schilling, L.; Osenbrügge, N. Determinants of soft drink consumption among children and adolescents in developed countries—A systematic review. Cent. Eur. J. Public Health 2021, 29, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Marinoni, M.; Parpinel, M.; Gasparini, A.; Ferraroni, M.; Edefonti, V. Risky behaviors, substance use, and other lifestyle correlates of energy drink consumption in children and adolescents: A systematic review. Eur. J. Pediatr. 2022, 181, 1307–1319. [Google Scholar] [CrossRef]
- Gračner, T.; Marquez-Padilla, F.; Hernandez-Cortes, D. Changes in Weight-Related Outcomes Among Adolescents Following Consumer Price Increases of Taxed Sugar-Sweetened Beverages. JAMA Pediatr. 2022, 176, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.M.; Frisvold, D.E.; Tefft, N. The effects of soft drink taxes on child and adolescent consumption and weight outcomes. J. Public Econ. 2010, 94, 967–974. [Google Scholar] [CrossRef]
- Marica, I. Study: Per Capita Purchasing Power is EUR 9092 in Romania, Half the European Average. Available online: https://www.romania-insider.com/purchasing-power-romania-europe-2024 (accessed on 1 December 2024).
- The Economic Problem of Romania in Europe. World Bank Group Romania. 2024. Available online: https://www.worldbank.org/en/country/romania/overview (accessed on 1 December 2024).
- Kjeld, S.G.; Lund, L.; Madsen, K.R.; Damsgaard, M.T.; Bast, L.S. Trends in Use of Alcohol and Cigarettes among Danish Adolescents, 2002–2018: Exclusive and Dual Use. Int. J. Environ. Res. Public Health 2022, 19, 3490. [Google Scholar] [CrossRef] [PubMed]
- Charrier, L.; van Dorsselaer, S.; Canale, N.; Baska, T.; Kilibarda, B. A Focus on Adolescent Substance Use in Europe, Central Asia and Canada. Health Behaviour in School-Aged Children International Report from the 2021/2022 Survey. Volume 3. World Health Organization. Regional Office for Europe. Available online: https://iris.who.int/handle/10665/376573 (accessed on 5 January 2025).
- Vaičiūnas, T.; Žemaitaitytė, M.; Lange, S.; Štelemėkas, M.; Oja, L.; Petkevičienė, J.; Kowalewska, A.; Pudule, I.; Piksööt, J.; Šmigelskas, K. Trends in Adolescent Substance Use: Analysis of HBSC Data for Four Eastern European Countries, 1994–2018. Int. J. Environ. Res. Public Health 2022, 19, 15457. [Google Scholar] [CrossRef] [PubMed]
- Motoc, G.V.; Juncar, R.I.; Moca, A.E.; Motoc, O.; Vaida, L.L.; Juncar, M. The Relationship between Age, Gender, BMI, Diet, Salivary pH and Periodontal Pathogenic Bacteria in Children and Adolescents: A Cross-Sectional Study. Biomedicines 2023, 11, 2374. [Google Scholar] [CrossRef] [PubMed]
- Funieru, C.; Nicolescu, M.I.; Băicuş, C.; Slușanschi, O.; Bica, C.I.; Moldoveanu, A.; Perpelea, A.C.; Țandără, A.T. Oral Hygiene Profile of Schoolchildren from Bucharest, Romania—How It Can Be Used and Improved for Better Prevention of Oral Diseases. Healthcare 2024, 12, 1293. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, R.; Sava-Rosianu, R.; Jumanca, D.; Balean, O.; Damian, L.-R.; Campus, G.G.; Maricutoiu, L.; Alexa, V.T.; Sfeatcu, R.; Daguci, C.; et al. Dental Caries, Oral Health Behavior, and Living Conditions in 6–8-Year-Old Romanian School Children. Children 2022, 9, 903. [Google Scholar] [CrossRef] [PubMed]
- Tudoroniu, C.; Popa, M.; Iacob, S.M.; Pop, A.L.; Năsui, B.A. Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits among 10 to 19-Year-Old Cluj-Napoca Romanian Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 6923. [Google Scholar] [CrossRef] [PubMed]
- Saveanu, C.I.; Cretu, C.C.; Bamboi, I.; Săveanu, A.E.; Anistoroaei, D. Title Cross-Sectional Study to Evaluate Knowledge and Attitudes on Oral Hygiene of Romanian Students. Medicina 2022, 58, 406. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, R.; Sava-Rosianu, R.; Jumanca, D.; Balean, O.; Damian, L.-R.; Fratila, A.D.; Maricutoiu, L.; Hajdu, A.I.; Focht, R.; Dumitrache, M.A.; et al. The Impact of Parental Education on Schoolchildren’s Oral Health—A Multicenter Cross-Sectional Study in Romania. Int. J. Environ. Res. Public Health 2022, 19, 11102. [Google Scholar] [CrossRef] [PubMed]
- Sfeatcu, R.; Cărămidă, M.; Sava-Rosianu, R.; Matichescu, M.L.; Galuscan, A.; Dumitrache, M.A. Carious status and socio-behavioral risk factors among 12-year-old children in South-Central region in Romania. BMC Oral Health 2023, 23, 644. [Google Scholar] [CrossRef] [PubMed]
- Trandafir, A.-V.; Lotrean, L.M. Education for Improving Awareness and Practices Regarding Hand Hygiene Among Romanian School Children. Sustainability 2025, 17, 304. [Google Scholar] [CrossRef]
- Štefan, L.; Sorić, M.; Devrnja, A.; Petrić, V.; Mišigoj-Duraković, M. One-year changes in physical activity and sedentary behavior among adolescents: The Croatian Physical Activity in Adolescence Longitudinal Study (CRO-PALS). Int. J. Adolesc. Med. Health 2018, 8, 32. [Google Scholar] [CrossRef] [PubMed]
- Tanveer, M.; Asghar, E.; Badicu, G.; Tanveer, U.; Roy, N.; Zeba, A.; Badri Al-Mhanna, S.; Batrakoulis, A. Associations of School-Level Factors and School Sport Facility Parameters with Overweight and Obesity among Children and Adolescents in Pakistan: An Empirical Cross-Sectional Study. Sports 2024, 12, 235. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Liang, X.; Sit, C.H.P. Physical Activity and Mental Health in Children and Adolescents With Neurodevelopmental Disorders: A Systematic Review and Meta-Analysis. JAMA Pediatr. 2024, 178, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Ludwig-Walz, H.; Siemens, W.; Heinisch, S.; Dannheim, I.; Loss, J.; Bujard, M. How the COVID-19 pandemic and related school closures reduce physical activity among children and adolescents in the WHO European Region: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 149. [Google Scholar] [CrossRef] [PubMed]
- Zurita-Ortega, F.; Badicu, G.; Chacón-Cuberos, R.; Castro-Sánchez, M. Motivational Climate and Physical Activity: A Multigroup Analysis in Romanian and Spanish University Students. Int. J. Environ. Res. Public Health 2019, 16, 2013. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, B.B.; Hergenroeder, A.L.; Katzmarzyk, P.T.; Lee, I.M.; Jakicic, J.M. Definition, measurement, and health risks associated with sedentary behavior. Med. Sci. Sports Exerc. 2015, 47, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, V.A.; Starc, G.; Brandes, M.; Kaj, M.; Blagus, R.; Leskošek, B.; Suesse, T.; Dinya, E.; Guinhouya, B.C.; Zito, V.; et al. Physical activity, screen time and the COVID-19 school closures in Europe—An observational study in 10 countries. Eur. J. Sport Sci. 2022, 22, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Popescu, A.M.; Balica, R.Ș.; Lazăr, E.; Bușu, V.O.; Vașcu, J.E. Smartphone addiction risk, technology-related behaviors and attitudes, and psychological well-being during the COVID-19 pandemic. Front. Psychol. 2022, 13, 997253. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | Questions | Coding |
|---|---|---|
| Sociodemographic | ||
| Age | How old are you? | 11 or younger, 12–14 “≤14” 15–18 or older “≥15” |
| Sex | What is your sex? | Female “Girls”, Male “Boys” |
| Background | What residential area do you live in? | “Rural”, “Urban” |
| Well-being and Health | ||
| Food insecurity | During the past 30 days, how often did you go hungry because there was not enough food in your home? | Most of the time/Always Rarely/Sometimes “Yes” Never/ “No” |
| Self-perceived health status | How would you describe your health in general? | Excellent/Very good/Good “Positive Perception About Health” Acceptable/Poor “Negative Perception About Health” |
| Nutritional status (Calculated by BMI—WHO Z scores cut-off) | How tall are you without shoes? What is your weight? | <−2SD from median for BMI by age and sex “Underweight” >+1SD from median for BMI by age and sex “Overweight” >+2SD from median for BMI by age and sex “Obese” |
| Nutritional Behaviors | ||
| Fruit daily intake | In the past 7 days, how many times did you eat fruits such as apples, pears, plums, bananas, melons, etc.? | Less than 2 portion/day (1/day/4 to 6 times in the last 7 days/1 to 3 times in the last 7 days/I haven’t eaten fruit in the last 7 days) “Yes—risk factor” 2 or more portion/ day “No—risk factor” |
| Vegetable daily intake | In the past 7 days, how many times did you eat vegetables such as tomatoes, cucumbers, carrots, lettuce, broccoli, etc. (excluding potatoes)? | Less than 3 portions/day (1/day/4 to 6 times in the last 7 days/ 1 to 3 times in the last 7 days/I haven’t eaten vegetables in the last 7 days) ”Yes—risk factor” 3 or more portions/day “No—risk factor” |
| Carbonated soft drinks | In the past 7 days, how many times did you drink a can, bottle or glass of a carbonated soft drink like Coca-Cola or Sprite? | More than 1/day “Yes—risk factor” Less than 1/day (4 to 6 times in the last 7 days/1 to 3 times in the last 7 days/I have not had any carbonated drinks in the last 7 days) “No—risk factor” |
| Sugary drinks | In the past 7 days, how many times did you drink a can, bottle or glass of a sugar-sweetened beverage (like sports drinks, energy drinks, sugar-sweetened teas, coffees, or flavoured waters)? | More than 1/day “Yes—risk factor” Less than 1/day (4 to 6 times in the last 7 days/1 to 3 times in the last 7 days/I have not had any sugary drinks in the last 7 days) ”No—risk factor” |
| Physical Activity and Sedentary Behaviors | ||
| Physical activity | During the past 7 days, on how many days were you physically active for a total of at least 60 min per day? Add up all the time you spent doing any kind of physical activity each day. | 0–4 days “Yes” “Insufficient Active” ≥5 days “No”—“Active enough” |
| Physical exercise—stretching | In the past 7 days, how many days did you do exercises to strengthen or tone your muscles, such as push-ups, squats, or weight lifting? | Less than 5 days/week (0, 1, 2, 3, 4)—“Insufficient Active” More than 5 days/week—“Active Enough” |
| Walking/cycling to school | In the past 7 days, how many days did you walk or bicycle to or from school? | 0–2 days “Yes” “Insufficient Active” ≥3 days “No”—“Active enough” |
| Physical education class | In this school year, how many days did you attend the physical education class each week? | 0–2 days “Yes” “Insufficient Active” ≥3 days “No”—“Active enough” |
| Sitting time hours/ day | On a typical day, how much time do you spend sitting and watching TV, playing computer games, chatting with friends, using your mobile phone? | ≥3 h per day “Yes—risk factor” ≤2 h per day “No—risk factor” |
| Sleep hours per night | During school time, how many hours do you sleep each night? | <8 h per night “Not Enough Sleep” ≥8 h per night “Enough Sleep” |
| Addictive behaviors influencing health. | ||
| Ever smoking | Have you ever tried smoking cigarettes, even a puff or two? | “Yes” “No” |
| Age beginning smoking | How old were you when you first tried smoking a cigarette? | I have never tried smoking a cigarette “Never” 7 years old or younger/8–14 years “≤14” 15–18 years “≥14” |
| Active smoking—normal cigarettes | In the past 30 days, how many days did you smoke cigarettes? | ≥1 days “Yes” 0 day “No” |
| Active smoking—electronic cigarettes | In the past 30 days, how many days did you use electronic cigarettes? | ≥1 days “Yes” 0 day “No” |
| Alcohol consumption | Have you ever consumed alcohol? (a serving is a glass of wine/beer/strength, etc.) | “Yes” “No” |
| Age of first alcohol consumption | How old were you when you first drank more than a few sips of alcohol? | I have never had a drink of alcohol other than a few sips “Never” 7 years old or younger/8–14 years “≤14” 15–18 years “≥14” |
| Active alcohol consumption | In the past 30 days, how many days did you drink at least one drink that contained alcohol? | ≥1 days “Yes” 0 day “No” |
| How did they obtain the alcohol | In the past 30 days, how did you get the alcohol you drank? | I did not drink alcohol in the past 30 days “Never had alcohol” I got it from my family “Family” I gave someone else money to buy it for me/I got it from my friends “Friends” I bought it in a shop/I stole it or got it without permission/I got it in another way “Other sources” |
| Drug consumption | Have you ever used drugs? (e.g., cannabis, marijuana, amphetamines, cocaine, heroin) | “Yes” “No” |
| Age of first drug consumption (years) | How old were you when you first used drugs? | I have never used drugs “Never” 7 years old or younger/8–14 years “≤14” 15–18 years “≥14” |
| Cannabis consumption | In your lifetime, how many times have you used cannabis (also called marijuana or weed)? | ≥1 days “Yes” 0 day “No” |
| Amphetamine and methamphetamine | During your lifetime, how many times have you used amphetamines or methamphetamines for non-medical purposes? | ≥1 days “Yes” 0 day “No” |
| Social behaviors—use of social networks | ||
| Screen time—hours/day | On a typical school day, how many hours of screen time do you spend? | Less than 2 h/day—“No risk factor” More than 2 h/day—“ Risk factor” |
| Use of social network | In the past 7 days, how many hours a day did you use your mobile phone for social networks, for online communication or to surf the Internet? | Less than 2 h/day—“No risk factor” More than 2 h/day—“ Risk factor” |
| Parental rules for screen time and social network | Do your parents or guardians have rules about how you can use social media, online communication or the Internet? | “Yes” “No” |
| Having a personal mobile phone | Do you have your own mobile phone to use? | “Yes” “No” |
| Hand Hygiene and Oral Hygiene | ||
| Washing teeth 2/day | In the past 30 days, how many times a day did you usually brush your teeth? | I have not cleaned or brushed my teeth in the past 30 days/Less than once a day/Once a day “Not Properly” Twice a day/3 or more times a day “Properly” |
| Fluoride toothpaste | In the past 30 days, did you use a toothpaste that contains fluoride when you brushed your teeth? | I have not cleaned or brushed my teeth in the past 30 days/ No, I did not usually use a toothpaste that contains fluoride/I do not know if the toothpaste I usually used contains fluoride “No” Yes, I usually used a toothpaste that contains fluoride “Yes” |
| Gum problem → missing school | In the past 30 days, did you have any problems with your teeth or gums that caused you to miss school? | “Yes” “No” |
| Hand hygiene before eating | In the past 30 days, how often did you wash your hands before eating? | Most of the time/Always “Yes” Never/Rarely/Sometimes “No” |
| Hand hygiene after toilet | In the past 30 days, how often did you wash your hands after using the toilet or latrine? | Most of the time/Always “Yes” Never/Rarely/Sometimes “No” |
| Using soap while washing hands | In the past 30 days, how often did you use soap when washing your hands? | Most of the time/Always “Yes” Never/Rarely/Sometimes “No” |
| Variable | Item | Total—n (%) | Girls—n (%) | Boys—n (%) | p-Value |
|---|---|---|---|---|---|
| Well-being and health | |||||
| Food/nutrition vulnerability | No | 762 (84.7) | 397 (83.8) | 365 (85.7) | 0.459 |
| Yes | 138 (15.3) | 77 (16.2) | 61 (14.3) | ||
| Perceived health status | Negative perception | 122 (13.6) | 89 (18.8) | 33 (7.7) | <0.001 |
| Positive perception | 778 (86.4) | 385 (81.2) | 393 (92.3) | ||
| Nutritional status | Underweight, normal weight | 685 (76.1) | 396 (57.8) | 289 (42.2) | <0.001 |
| Overweight, obese | 215 (23.9) | 78 (36.3) | 137 (63.7) | ||
| Variable | Item | Total—n (%) | Girls—n (%) | Boys—n (%) | p-Value |
|---|---|---|---|---|---|
| Nutritional Behaviors | |||||
| Fruits daily intake | Less than 2 portion/day | 725 (80.6) | 384 (81) | 341 (80) | 0.736 |
| 2 or more portion/day | 175 (19.4) | 90 (19) | 85 (20) | ||
| Vegetable daily intake | Less than 3 portion/day | 794 (88.2) | 426 (89.9) | 368 (86.4) | 0.12 |
| 3 or more portion/day | 106 (11.8) | 48 (10.1) | 58 (13.6) | ||
| Carbonated soft drinks | more than 1/day | 280 (31.1) | 135 (28.5) | 145 (34) | 0.083 |
| less than 1/day | 620 (68.9) | 339 (71.5) | 281 (66) | ||
| Sugary drinks | more than 1/day | 261 (29) | 141 (29.7) | 120 (28.2) | 0.607 |
| less than 1/day | 639 (71) | 333 (70.3) | 306 (71.8) | ||
| Variable | Item | Total—n (%) | Girls—n (%) | Boys—n (%) | p-Value |
|---|---|---|---|---|---|
| Addictive behaviors | |||||
| Ever smoking | Yes | 351 (39) | 191 (40.3) | 160 (37.6) | 0.412 |
| No | 549 (61) | 283 (59.7) | 266 (62.4) | ||
| Age beginning smoking | Never | 554 (61.6) | 287 (60.5) | 267 (62.7) | 0.226 |
| ≤14 | 147 (16.3) | 72 (15.2) | 75 (17.6) | ||
| ≥14 | 199 (22.1) | 115 (24.3) | 84 (19.7) | ||
| Active smoking (last 30 days)—normal cigarettes | Yes | 166 (18.4) | 91 (19.2) | 75 (17.6) | 0.548 |
| No | 734 (81.6) | 383 (80.9) | 351 (82.4) | ||
| Active smoking (last 30 days)—electronic cigarettes | Yes | 131 (14.6) | 79 (16.7) | 52 (12.2) | 0.059 |
| No | 769 (85.4) | 395 (83.3) | 374 (87.8) | ||
| Alcohol consumption | Yes | 554 (61.6) | 277 (58.4) | 277 (65) | 0.047 |
| No | 346 (38.4) | 197 (41.6) | 149 (35) | ||
| Age of first alcohol consumption | Never | 392 (43.6) | 226 (47.7) | 166 (39) | <0.001 |
| ≤14 | 200 (22.2) | 78 (16.5) | 122 (28.6) | ||
| ≥14 | 308 (34.2) | 170 (35.9) | 138 (32.4) | ||
| Active alcohol consumption (last 30 days) | Yes | 298 (33.1) | 137 (28.9) | 161 (37.8) | 0.005 |
| No | 602 (66.9) | 337 (71.1) | 265 (62.2) | ||
| How did they obtain the alcohol | Never had alcohol | 589 (65.4) | 331 (69.8) | 258 (60.6) | <0.001 |
| Family | 74 (8.2) | 34 (7.2) | 40 (9.4) | ||
| Friends | 110 (12.2) | 70 (14.8) | 40 (9.4) | ||
| Other sources | 127 (14.1) | 39 (8.2) | 88 (20.6) | ||
| Drug consumption | Yes | 21 (2.3) | 5 (1.1) | 16 (3.8) | 0.008 |
| No | 879 (97.7) | 469 (98.9) | 410 (96.2) | ||
| Age of first drug consumption (years) | Never | 882 (98) | 470 (99.2) | 412 (96.7) | 0.023 |
| ≤14 | 3 (0.3) | 0 (0) | 3 (0.7) | ||
| ≥14 | 15 (1.7) | 4 (0.8) | 11 (2.6) | ||
| Cannabis consumption | Yes | 15 (1.7) | 2 (0.4) | 13 (3.1) | 0.003 |
| No | 885 (98.3) | 472 (99.6) | 413 (96.9) | ||
| Amphetamine and methamphetamine | Yes | 6 (0.7) | 470 (99.2) | 424 (99.5) | 0.689 |
| No | 894 (99.3) | 4 (0.8) | 2 (0.5) | ||
| Variable | Item | Total—n (%) | Girls—n (%) | Boys—n (%) | p-Value |
|---|---|---|---|---|---|
| Physical activity—Sedentary behaviors | |||||
| Active 60 min/day | No | 493 (54.8) | 303 (63.9) | 190 (44.6) | <0.001 |
| Yes | 407 (45.2) | 171 (36.1) | 236 (55.4) | ||
| Physical exercise—stretching | Less than 5 days/week | 502 (55.8) | 330 (69.6) | 172 (40.4) | <0.001 |
| More than 5 days/week | 398 (44.2) | 144 (30.4) | 254 (59.6) | ||
| Walking/cycling to school | No | 295 (32.8) | 150 (31.6) | 145 (34) | 0.477 |
| Yes | 605 (67.2) | 324 (68.4) | 281 (66) | ||
| Physical education class | No | 516 (57.3) | 294 (62) | 222 (52.1) | 0.003 |
| Yes | 384 (42.7) | 180 (38) | 204 (47.9) | ||
| Sitting time hours/day | More than 2 h/day | 675 (75) | 368 (77.6) | 307 (72.1) | 0.064 |
| Less than 2 h/day | 225 (25) | 106 (22.4) | 119 (27.9) | ||
| Sleep hours per night | <8 | 532 (59.1) | 292 (61.6) | 240 (56.3) | 0.118 |
| ≥8 | 368 (40.9) | 182 (38.4) | 186 (43.7) | ||
| Variable | Item | Total—n (%) | Girls—n (%) | Boys—n (%) | p-Value |
|---|---|---|---|---|---|
| Social behaviors—Blue screens | |||||
| Screen time hours/day | Less than 2 h/day | 308 (34.2) | 147 (31) | 161 (37.8) | 0.035 |
| More than 2 h/day | 592 (65.8) | 327 (69) | 265 (62.2) | ||
| Use of social networks | Less than 2 h/day | 288 (32) | 127 (26.8) | 161 (37.8) | <0.001 |
| More than 2 h/day | 612 (68) | 347 (73.2) | 265 (62.2) | ||
| Parental rules for screen time and social networks | Yes | 274 (30.4) | 140 (29.5) | 134 (31.5) | 0.562 |
| No | 626 (69.6) | 334 (70.5) | 292 (68.5) | ||
| Having personal mobile phone | Yes | 888 (98.7) | 470 (99.2) | 418 (98.1) | 0.246 |
| No | 12 (1.3) | 4 (0.8) | 8 (1.9) | ||
| Variable | Item | Total—n (%) | Girls—n (%) | Boys—n (%) | p-Value |
|---|---|---|---|---|---|
| Hygiene Behaviors | |||||
| Cleaning teeth twice/day | No | 198 (22) | 62 (13.1) | 136 (31.9) | <0.001 |
| Yes | 702 (78) | 412 (86.9) | 290 (68.1) | ||
| Fluoride toothpaste | No | 592 (65.8) | 314 (66.2) | 278 (65.3) | 0.779 |
| Yes | 308 (34.2) | 160 (33.8) | 148 (34.7) | ||
| Gum problem → missing school | No | 865 (96.1) | 450 (94.9) | 451 (97.4) | 0.05 |
| Yes | 35 (3.9) | 24 (5.1) | 11 (2.6) | ||
| Hand hygiene before eating | No | 24 (2.7) | 9 (1.9) | 15 (3.5) | 0.15 |
| Yes | 876 (97.3) | 465 (98.1) | 411 (96.5) | ||
| Hand hygiene after toilet | No | 8 (0.9) | 4 (0.8) | 4 (0.9) | 1 |
| Yes | 892 (99.1) | 470 (99.2) | 422 (99.1) | ||
| Using soap while washing hands | No | 10 (1.1) | 2 (0.4) | 8 (1.9) | 0.037 |
| Yes | 890 (98.9) | 472 (99.6) | 418 (98.1) | ||
| Model | B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for EXP(B) | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Sex | 0.409 | 0.151 | 7.337 | 1 | 0.007 | 1.506 | 1.12 | 2.024 |
| Physical exercise | 1.526 | 0.152 | 101.235 | 1 | <0.001 | 4.598 | 3.416 | 6.19 |
| Walking/cycling to school | 0.307 | 0.158 | 3.784 | 1 | 0.052 | 1.359 | 0.998 | 1.85 |
| Sitting time hours/ day | 0.23 | 0.179 | 1.647 | 1 | 0.199 | 1.258 | 0.886 | 1.787 |
| Sleep hours per night | 0.087 | 0.156 | 0.315 | 1 | 0.574 | 1.091 | 0.804 | 1.481 |
| Parental rules for screen time | 0.18 | 0.167 | 1.159 | 1 | 0.282 | 1.197 | 0.863 | 1.66 |
| Constant | −0.072 | 0.092 | 0.623 | 1 | 0.43 | 0.93 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roșioară, A.-I.; Năsui, B.A.; Ciuciuc, N.; Sîrbu, D.M.; Curșeu, D.; Vesa, Ș.C.; Popescu, C.A.; Bleza, A.; Popa, M. Beyond BMI: Exploring Adolescent Lifestyle and Health Behaviours in Transylvania, Romania. Nutrients 2025, 17, 268. https://doi.org/10.3390/nu17020268
Roșioară A-I, Năsui BA, Ciuciuc N, Sîrbu DM, Curșeu D, Vesa ȘC, Popescu CA, Bleza A, Popa M. Beyond BMI: Exploring Adolescent Lifestyle and Health Behaviours in Transylvania, Romania. Nutrients. 2025; 17(2):268. https://doi.org/10.3390/nu17020268
Chicago/Turabian StyleRoșioară, Alexandra-Ioana, Bogdana Adriana Năsui, Nina Ciuciuc, Dana Manuela Sîrbu, Daniela Curșeu, Ștefan Cristian Vesa, Codruța Alina Popescu, Andreea Bleza, and Monica Popa. 2025. "Beyond BMI: Exploring Adolescent Lifestyle and Health Behaviours in Transylvania, Romania" Nutrients 17, no. 2: 268. https://doi.org/10.3390/nu17020268
APA StyleRoșioară, A.-I., Năsui, B. A., Ciuciuc, N., Sîrbu, D. M., Curșeu, D., Vesa, Ș. C., Popescu, C. A., Bleza, A., & Popa, M. (2025). Beyond BMI: Exploring Adolescent Lifestyle and Health Behaviours in Transylvania, Romania. Nutrients, 17(2), 268. https://doi.org/10.3390/nu17020268