Highlights
- Registered dietitian expert panelists reached a consensus on 9 evidence-based examination domains and 46 of 48 examination components for the development of a trauma-informed, culturally sensitive eating-disorder-specific nutrition-focused physical examination (ED-NFPE) tool.
- Panelists provided qualitative feedback on domain and component additions, exclusions, modifications, and trauma-informed culturally sensitive examination practice techniques suitable for all individuals, especially marginalized individuals, those with a history of trauma, and those with larger bodies.
- In addition to food and nutrition history, client history, and biochemical, medical, and diagnostic tests, a thorough trauma-informed, culturally sensitive ED-NFPE tool will close the gap in eating disorder patient care by enabling registered dietitians to identify signs and symptoms of malnutrition and other nutrition-related complications specific to individuals in this population.
Abstract
Objective: This study aimed to identify components of a trauma-informed, culturally sensitive eating-disorder-specific nutrition-focused physical examination (ED-NFPE) tool. Method: The modified Delphi methodology was used to develop a consensus on the clinical relevance of nine evidence-informed ED-specific nutrition examination domains and 46 components within those domains. Purposive sampling was used to recruit a panel of registered dietitian nutritionist (RDN) experts in the ED field. The panelists responded to survey statements on a five-point Likert scale. The panelists also provided qualitative feedback on domain and component additions, exclusions, modifications, and trauma-informed culturally sensitive examination practice techniques. Results: Twenty-two RDN expert panelists completed Round One of the study, and eighteen panelists completed Round Two (82% retention). Twenty-one were female. Fifteen panelists had ten or more years of experience in ED dietetics. Fifty percent held an advanced practice credential from the International Association of Eating Disorders Professionals (IAEDP). After the two survey rounds, the nine ED-NFPE domains and 46 of the 48 components achieved a consensus for clinical relevance. The panelists proposed two new examination components and provided qualitative feedback for trauma-informed culturally sensitive practice techniques in all nine domains. Conclusions: This modified Delphi study design was chosen to reach a consensus on developing an ED-NFPE tool, as there are few current evidence-based guidelines for nutrition examinations in ED care. An NFPE tool specifically designed to detect the nutrition-related findings of individuals with EDs would strengthen the overall nutrition assessment. RDNs at every level of care and with all degrees of experience could use an ED-NFPE to inform patient treatment goals.
1. Introduction
Eating disorders (EDs) are complex biopsychosocial illnesses [1]. Individuals of every age, weight, shape, and size can develop an ED [2]. They often affect marginalized and vulnerable populations such as people of color, certain religious groups, people that are lesbian, gay, bisexual, transgender, queer, and others (LGBTQ+), and those with neurodivergence and physical disabilities [3,4,5,6,7]. Individuals with EDs may have co-occurring mental or medical illnesses and a history of trauma [8,9,10,11,12,13]. Nine percent, or 28.8 million Americans, will experience an ED in their lifetime [14]. The global lifetime ED prevalence is nearly eight percent [15].
All ED subtypes are associated with nutrition-related medical complications, and al-though each individual with an ED may have a unique presentation, complications occur primarily due to ED behaviors such as restrictive eating, bingeing, purging, enema use, laxative, diuretic, and other substance abuse, overhydration, dehydration, excessive exercise, and others [2,16,17,18,19,20,21,22,23,24,25,26,27,28]. Complications of ED behaviors can be physical, psychological, and nutritional and include cardiorespiratory complications, bone, muscle, and fat changes, hydration and electrolyte imbalances, impaired cognition and psychosocial functioning, intraoral and extraoral issues, dermatologic abnormalities, parotid gland enlargement, gastrointestinal symptoms, and other complications affecting one or more organ systems (Figure 1) [13,16,17,18,19,20,21,22,23,24,25,26,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53]. Awareness of unique ED-related complications, timely ED-specific nutritional, psychiatric, psychological, and medical assessments, and treatment are critical factors in ED recovery [54,55,56]. Most complications associated with EDs can be reversed through effective treatment, including the cessation of ED behaviors, proper nutrition rehabilitation, and weight restoration (if needed) [18,37,57].
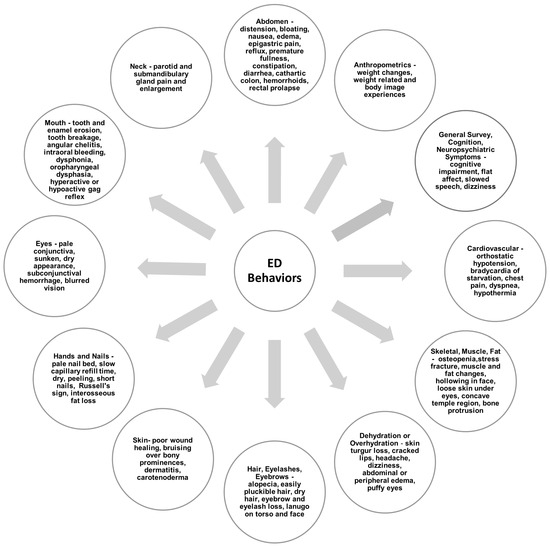
Figure 1.
Nutrition-related signs and symptoms of eating disorder behaviors [13,16,17,18,19,20,21,22,23,24,25,26,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53].
In addition to a comprehensive assessment of an individual’s eating and exercise patterns, height and weight history, and family history of EDs or other psychiatric illnesses, the American Psychiatric Association (APA) recommends that multidisciplinary initial physical assessments of individuals with EDs be performed [58]. These include the evaluation of body temperature, heart rate, resting and orthostatic blood pressure, pulse, height, weight, body mass index (BMI), and physical signs of malnutrition and purging behaviors [58]. The APA also recommends a wide-ranging biochemical assessment, an electrocardiogram, and a complete review of body systems [58]. Lastly, the APA emphasizes that individuals with EDs should receive a culturally appropriate, person-centered treatment plan that includes psychological, psychiatric, nutritional, and medical experts [58].
Although national and international organizations recommend comprehensive assessments, there are few current ED-specific nutrition assessment tools, clinical guidelines, or standards for examining or assessing this population for nutrition-related complications [3,27,58,59,60,61,62,63,64,65,66,67,68,69,70]. Table 1 outlines the primary ED diagnoses, several ED behavior types, and co-occurring considerations for an ED nutrition assessment.

Table 1.
Eating disorder diagnoses, behavior types, and co-occurring considerations.
Registered dietitian nutritionists (RDNs) play a central role in ED care, as nutritional rehabilitation is one of the cornerstones of short- and long-term ED treatment [3,27]. The Academy of Nutrition and Dietetics (AND) standards of practice for RDNs include performing a comprehensive nutrition assessment, establishing a nutrition diagnosis(es), developing a nutrition intervention plan, monitoring and evaluating this plan, and conducting patient discharge or modifying the level of care provided [3,59,90,91].
The nutrition assessment domains of the nutrition care process include (1) client history, (2) anthropometric measurements, (3) biochemical, medical, and diagnostic tests, (4) food and nutrition history, (5) nutrition-focused physical examination (NFPE), and (6) ongoing reassessment(s), monitoring, and evaluation [3,42,59,63,64,70,90,92,93,94,95].
According to the APA, in individuals with EDs, guilt, embarrassment, and shame about ED behaviors and symptoms may prevent them from providing a complete and accurate food- and nutrition-related history [28]. Additionally, weight and body mass index (BMI) are not always diagnostic features of individuals with diagnoses other than anorexia nervosa, such as bulimia nervosa, binge eating disorder, “unspecified feeding or eating disorder”, and “other specified feeding or eating disorder”. These individuals may present in a “larger” body or with a BMI in a “healthy” range [28,63,66,96,97,98]. Lastly, individuals with EDs often present with normal biochemical and medical diagnostic test findings despite illness severity [3,27].
Because food and nutrition history, weight and BMI, and biochemical and medical diagnostic tests may not capture the physical signs and symptoms of malnutrition or the degree or severity of an ED, a systematic head-to-toe assessment tool (NFPE) is a crucial component of the nutrition assessment process [23,27,54,66,74,90,99].
The NFPE assessment tool evolved from the Subjective Global Assessment (SGA) tool and the American Society of Parenteral and Enteral Nutrition (ASPEN)/AND criteria for malnutrition [69,100]. The SGA is a validated nutrition assessment tool developed in the 1980s [100]. Based on patient history and physical examination findings, the SGA has been used by RDNs and other medical professionals globally to help determine the presence and severity of malnutrition [100].
In 2009, etiology-based diagnostic criteria for malnutrition were defined by the European Society for Clinical Nutrition and Metabolism (ESPEN) and, similarly, by a working group of the American Society of Parenteral and Enteral Nutrition (ASPEN) and the Academy of Nutrition and Dietetics (AND) [69,101]. The AND/ASPEN criteria were developed from the SGA and then expanded to include a minimum of two among the following items: insufficient energy intake, weight loss, loss of muscle mass and subcutaneous fat stores, fluid retention, and reduction in functional status [69,100]. Malnutrition was also defined in the context of acute illness or injury, chronic illness, or social or environmental circumstances [69].
The NFPE is utilized by RDNs in various clinical settings worldwide to assess micronutrient and macronutrient deficiencies, excesses, and imbalances and support a malnutrition diagnosis [28,64,92,93,102,103,104,105]. Muscle and fat stores, fluid retention (hydration status), functional status (grip strength), and other signs and symptoms of nutrition-related complications can be assessed through the NFPE [42,92,93,102,103,104]. The AND consistently updates the standards of practice and professional performance for RDNs (novice through to expert) and includes an NFPE to assess for malnutrition and overall nutrition status [3,59,70,92,102,103,104,106].
The examination techniques of inspection, palpation, percussion, and auscultation are used in the traditional NFPE to identify nutrition-related signs and symptoms arising from disease pathology [42,70,102,103,104,106]. The traditional NFPE domains include (1) general appearance, (2) vital signs, (3) skin, (4) nails, (5) head and hair, (6) eyes and nose, (7) mouth (intra and extraoral), (8) neck and chest, (9) abdomen, and (10) musculoskeletal system [92,93,102,104].
There are no evidence-based guidelines or standards for the NFPE of individuals with EDs [3,27,59,99]. The traditional NFPE lacks the specificity to thoroughly capture the unique nutritional complications commonly seen in individuals with EDs [93,99]. The conventional NFPE does not incorporate the principles of trauma-informed care, patient-centeredness, or culturally sensitive guidelines for its use in clinical practice, which are key considerations for providing the highest-quality healthcare (Table 2) [3,27,90,93,99,107,108,109,110].
Table 2.
Principles of trauma-informed care, patient-centeredness, cultural sensitivity.
According to the Substance Abuse and Mental Health Services Administration (SAMHSA), a trauma-informed approach in healthcare contributes to a positive treatment outcome. Trauma-informed care prioritizes the physical and emotional safety of survivors [109,110].
Although not all individuals with EDs have a trauma history, trauma safeguards must be instituted in ED assessments and treatment [115]. Individuals with a trauma history may have a heightened fear of threat, high emotional reactivity, and sensitivity to criticism [9]. A trauma history may also predict ED treatment withdrawal and poor recovery outcomes [9,115]. Alternatively, a patient’s perception of a safe and supportive treatment environment can help to remove obstacles to effective treatment [115].
Person-centered, culturally sensitive guidelines ensure that the treatment provider treats the patient as a unique person, not a diagnosis [107,108]. The treatment provider should exhibit awareness of their personal and professional biases, bear knowledge of various cultures, races, ethnicities, and religions, and understand the health disparities of marginalized groups [74,107].
A trauma-informed ED-specific nutrition-focused physical examination (ED-NFPE) tool, conducted with cultural sensitivity, could more thoroughly and adeptly identify nutrition-related complications in individuals with EDs and improve patients’ experiences and clinical outcomes [3,27,74,93,107,108,109,110]. The results of this ED-NFPE, in combination with other nutrition assessment findings from food and nutrition history, medical and psychosocial history, biochemical data, and medical and diagnostic tests and procedures, could help to inform goals for nutrition rehabilitation [3,27,74,90,99].
This study aimed to identify the domains and components of an ED-NFPE tool for RDNs to utilize at various levels of ED care to assess nutrition-related complications in individuals with EDs. The study also aimed to identify trauma-informed, culturally sensitive practice tools and techniques based on the principles of trauma-informed care in behavioral health science [110,116]. To meet these objectives, the study’s first aim was to conduct a literature review to identify evidence to inform the development of the ED-NFPE tool. The second aim was to develop a web-based survey and recruit ED RDN expert panelists [117,118,119,120]. The second aim used the modified Delphi methodology to establish a consensus among the expert panelists on the clinical relevance of the proposed ED-NFPE domains and components and to obtain feedback on a trauma-informed, culturally sensitive examination approach for inclusion in the ED-NFPE tool [121]. The research team employed the grounded theory research strategy to analyze the qualitative data and support the study objectives [122].
2. Materials and Methods
2.1. Study Design
2.1.1. Delphi Approach Introduction
The Delphi and modified Delphi methods are widely used in mental health and ED research to develop clinical guidelines and improve mental health training, treatment, and cultural competence [60,65,123,124,125]. The modified Delphi method was chosen due to the complexities in the ED population and the need for expert opinions on ED care [121]. A modified Delphi approach, with iterative survey rounds and anonymous in-depth “discussion” and “communication” among expert panelists, will likely generate a strong consensus among the expert panel and reduce the impact of potential groupthink [121]. A literature review of the most commonly seen nutrition-related complications in EDs was conducted, and an analysis of the traditional NFPE domains and common nutrition-related complications in other clinical patient populations was performed. From the literature review, a pre-selected set of survey statements was developed. The modified method permitted a more focused study that could be conducted in six months with two to three rounds [121]. This type of study would also potentially maximize panelist participation and retention, as the time commitment was limited [121]. The researchers used the post-positivism research paradigm framework to obtain values-based, holistic, qualitative panelist feedback for trauma-informed, culturally sensitive examination techniques [126]. Three feedback rounds were determined a priori; however, only two were conducted to develop sufficient feedback and “communication” among panelists to achieve a consensus [121].
2.1.2. Literature Review
An electronic literature review was conducted using the PubMed, CINAHL, and Scopus databases to identify primary research articles, review articles, and case studies on medical, dental, and nutrition assessment techniques and the current assessment methods used in ED care and to identify the common nutrition-related signs and symptoms resulting from the ED behaviors of all ED subtypes in children, adolescents, and adults.
The keywords and MeSH terms used in numerous groupings included “feeding and eating disorders” (MeSH), “eating disorders”, “anorexia nervosa”, “bulimia or bulimic or bulimia nervosa”, “avoidant restrictive food intake disorder or ARFID”, “atypical anorexia nervosa”, “pica”, “eating disorders not otherwise specified”, “physical assessment”, “nutrition assessment”, “nutrition-focused physical examination”, “skin conditions”, “skin signs”, “dermatologic signs”, “Russell’s sign”, “micronutrient deficiencies”, “macronutrient deficiencies”, “malnutrition”, “dehydration”, “overhydration”, “hydration”, “mouth symptoms”, “oral symptoms”, “vital signs”, “cognition”, “fat loss”, “muscle loss”, “hair”, “nails”, “eyes”, “neurological consequences”, “abdominal issues”, “parotid gland”, “cardiovascular”, “eating disorder treatment guidelines”, “gaps in eating disorders treatment”, and “eating disorder nutrition treatment guidelines”.
Several articles were hand-selected from the reference lists of primary research, review articles, and PubMed-suggested articles. Duplicate articles were eliminated. Published guidelines from international organizations such as the Academy of Nutrition and Dietetics, Academy for Eating Disorders, Australian and New Zealand Academy for Eating Disorders, American Psychological Association, American Psychiatric Association, and National Institute for Health and Care Excellence were retrieved from searches on Google Scholar, UpToDate, and reference lists from the chosen articles. Articles were also reviewed to clarify potential circumstances common in patients with eating disorders that should be addressed before and during the examination. These include patients in larger bodies, patients with a trauma history, racial, ethnic, and religious diversity, neurodiverse patients, LGBTQ+ patients, and patients with gastrointestinal diseases or other medical or mental health comorbidities.
The search was limited to articles written in English. The other inclusion criteria were years of publication from 1987 to 2025, adults, adolescents, and children, inpatient and outpatient settings, all genders, and all subtypes of eating disorders. Articles written before 2000 were included for historical value as relevant to the development of the NFPE.
The ED-specific nutrition-related complications identified through the literature search were cross-referenced with the traditional NFPE domains and common clinical findings in other clinical patient populations and organized into examination domains that were more ED-specific and could be conducted with the primary techniques of discussion and observation. The literature search identified nine ED-specific examination domains, including (1) anthropometrics, (2) general survey, cognition, and neuropsychiatric symptoms, (3) vital signs, (4) bone loss and injury, fat and muscle stores, (5) hydration status, (6) skin, hands, and nails, (7) hair, eyelashes, eyebrows, and eyes, (8) orofacial (intra and extraoral) and neck, and (9) abdomen (gastrointestinal) [92,93,102,104].
As an alternative to the traditional NFPE examination techniques of inspection, palpation, percussion, and auscultation, the examination techniques for the ED-NFPE tool included (1) discussion and (2) observation, (3) and measuring blood pressure, temperature, radial pulse, capillary refill rate, and grip strength (with explicit patient permission) [93,102]. Discussion and observation examination techniques (with explicit patient permission) were selected by the authors to accurately assess individuals for nutrition-related complications in most domains while adhering to the principles of trauma-informed care, patient-centered care, and cultural sensitivity (i.e., ensuring patient safety and maintaining appropriate boundaries) [3,27,74]. Measuring blood pressure, temperature, radial pulse, capillary refill rate, and grip strength requires physical contact to be performed and was, therefore, excluded from the observation and discussion technique categories and organized into a separate technique. The identified examination domains and common ED findings that informed all survey statements for an ED-NFPE tool are outlined in Table 3: Eating-Disorder-Specific Nutrition-Focused Physical Examination Tool.
Table 3.
Eating-Disorder-Specific Nutrition-Focused Physical Examination Tool.
The search also identified the six principles of trauma-informed care and culturally sensitive guidelines [58,74,107,108,109,110,116]. These principles and guidelines provided background to evaluate the panelists’ qualitative open-ended feedback. After validation through evidentiary support, the panelists’ responses will also inform the future development of trauma-informed, culturally sensitive instructional guidelines for ED-NFPE tools [3,4,5,6,8,12,13,23,50,63,72,74,75,76,77,78,79,80].
2.2. Survey Development
The literature search results informed the construction of the Qualtrics survey (Qualtrics, Provo, Utah), the “Eating Disorders Nutrition Assessment Tool” Survey (survey is available in Supplementary Information) [150]. The survey consisted of panelist consent, instructions, demographic and professional information, and a series of closed- and open-ended statements organized by examination domain. An introduction and description of each domain preceded the closed-ended statements. Each statement was designed so the panelists could rate their agreement with the clinical relevance of the domains and components on a 5-point Likert scale (strongly disagree, disagree, neither agree nor disagree, agree, or strongly agree) [123,151].
An open-ended statement requesting panelist feedback for domain and component addition, omission, or modification followed the set of closed-ended statements. Lastly, the survey included an open-ended statement for each domain, stating, “If you feel the (anthropometrics) domain is clinically relevant, please provide feedback on any particular practice tools or techniques you may currently employ or would recommend promoting a trauma-informed, culturally specific assessment. Leave blank if you prefer not to answer or have no additional feedback”.
2.3. Survey Distribution and Panelist Recruitment
The study was conducted from May through to August 2024. Purposive sampling was used to recruit a panel of RDN experts in ED practice. Several ED organizations were contacted to request their members’ email addresses for study participation or to post the study invitation on their professional discussion boards or professional interest group online forums. The organizations included in recruitment were the Academy for Eating Disorders (AED), the Academy of Nutrition and Dietetics (AND) Behavioral Health Nutrition Practice Group, Eating Disorder Registered Dietitians and Professionals (EDRD Pro), and the International Federation of Eating Disorder Dietitians (IFEDD) [117,118,119,120,152].
Organization leaders posted an invitation to participate in an initial screening survey on professional online forums or an invitation was directly emailed to nutrition professionals from these professional interest groups and ED organizations. The invitation included a brief introduction to the research study, research team, Delphi methodology, and study purpose. The screening survey included a brief set of questions to assess panelist eligibility.
If potential expert panelists met the criteria from the screening survey and chose to participate, they were sent a second personalized email including a link to the survey. Participants were informed of the time commitment of their participation. To maintain interest and reduce the risk of attrition, participants were offered the opportunity to participate in a raffle for a USD 50.00 Amazon e-gift card for their participation [153].
The inclusion criteria required that the expert panelists were RDNs with five or more years of experience in ED treatment or held an advanced practice credential through the International Association of Eating Disorders Professionals (IAEDP), with a minimum of 2500 supervised hours of work in the ED field [152]. Experts were not required to have advanced training in trauma-informed care. Although panelist group size can vary in Delphi studies, the study sought to recruit 20 or more panelists [123].
2.4. Ethics
The Rutgers University Institutional Review Board approved the study protocol and consent for panelists’ screening and participation (Pro2023002454). The authors followed the recommended Conducting and Reporting of Delphi Studies (CREDES) guidelines outlined by Jünger and colleagues and the Reporting guidelines for Delphi techniques in health sciences: A methodological review by Spranger et al. [154,155]. The panelists were informed that their demographic information and survey responses would be de-identified. Their anonymous responses would be included in future rounds for other panelists to review [156].
2.5. Survey Process
Round One included study background information, panelist consent, instructions, and demographic and professional information. The panelists were instructed to respond to statements about the clinical relevance of the nine ED-NFPE domains and 46 components within these domains by rating their agreement with the statements on a 5-point Likert scale [123,151]. The panelists were also given the option to provide feedback for domain and component addition, omission, modification, and practice tools or techniques they may currently employ or recommend to promote a trauma-informed, culturally specific ED-NFPE.
The panelists were required to complete and return their Round One survey via email within three weeks. After Round One data collection and analysis, the panelists were provided with a summary of their responses, mean group responses, and all other panelists’ de-identified responses to open-ended statements to permit the panelists to compare their responses to other panelists’ responses and revise them if desired. The panelists were given another week to review and revise their responses if desired. The round then closed, and a final data analysis was conducted to determine if consensus was achieved on any domains and components. Open-ended qualitative responses were reviewed for potential additions, omissions, modifications, and approaches. Survey items from Round One that the panelists added were verified through an additional literature review and added based on the results of a review of evidence. Feedback on a trauma-informed, culturally sensitive approach was analyzed for shared content. These comments will be evaluated for evidentiary support in future studies.
Round Two followed the same sequence as Round One. Items from Round One that achieved consensus were visible to the panelists in Round Two but were closed for further comments. Round Two contained statements that did not reach consensus in Round One and statements for the two additional components recommended by the panelists. As in Round One, the panelists were provided with a results summary and the opportunity to review and revise their responses if desired. Of the 48 final components, 46 reached a consensus after Round Two. There was no upward scoring trend for the additional two components in Round Two. It was, therefore, determined by the research team that a third round was not indicated. The results of Round Two determined a final consensus on domains, components, and approaches.
2.6. Data Analysis
IBM SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY, USA: IBM Corp.) was used for data analysis [157]. Descriptive statistics (frequency and percentage) were used for panelist demographic information. The results for the clinical relevance of the ED-NFPE domains and components are reported as means and standard deviations (SDs). All research team members systematically read, hand-coded, and performed content analysis on the data from the qualitative responses to identify patterns in certain concepts or themes [122]. Based on previous Delphi studies on NFPE development, mental health, and ED practice, consensus was defined a priori as ≥75% of panelists answering “neither agree nor disagree”, “agree”, or “strongly agree” using the 5-point Likert scale, or as a rank of 4 ± 1 SD for each domain or component [65,151,158,159,160].
3. Results
3.1. Panelists
In total, 22 of the 44 panelists who participated in the eligibility screening survey met the eligibility criteria, consented to participate, and completed Round One (Table 4). Ninety-five percent identified as female. All panelists were 30 years old or older. Two-thirds had ten or more years of experience in ED dietetics. Fourteen worked thirty or more hours per week. Most panelists worked in an outpatient clinic or private practice. Three panelists were employed in a partial hospitalization program (PHP), intensive outpatient program (IOP), or “other” setting. All panelists were RDNs, with 50% holding an advanced practice credential from IAEDP. In the demographics portion of the survey, the panelists were not asked which country they lived in. They were, however, recruited from several international professional organizations, including IAEDP and IFEDD. Eighteen panelists completed Round Two (82% retention).
Table 4.
Demographics and professional characteristics of eating disorder dietitian expert panelists.
3.2. Round One
All nine domains (100%) and 44 of 46 components (95.6%) achieved consensus in Round One (Table 5). Two components, “BMI” and “measuring weight when weight restoration is not a treatment goal”, did not reach consensus.
Table 5.
Round One domains’ and components’ clinical relevance, consensus determination.
Several panelists recommended two new components. These components, “capillary refill time” and “grip strength”, were reviewed for evidentiary support through a literature search and added to the Round Two survey in the “vital signs” and “bone, body fat, and muscle” domains, respectively.
From the open-ended statements, the panelists provided feedback for revisions, stating that the discussion and observation of components should be case-dependent and carefully considered and timed because of the topic sensitivity and to prevent the reinforcement of eating disorder cognitions. Additionally, the panelists suggested that other treatment providers should perform some measurements, observations, and discussions, especially if the RDN performs telehealth treatment. Several panelists felt that they needed additional training to assess and interpret some component findings.
The panelists were also asked to provide feedback, based on their extensive experience, on practice tools to promote a trauma-informed, culturally specific approach to examination components. Through hand-coding, frequently mentioned responses emerged (Table 6).
Table 6.
Rounds One and Two feedback for trauma-informed, culturally sensitive techniques.
Each panelist was emailed a feedback form and could revise their ratings and responses by requesting a new survey link. Two panelists (9%) requested a new survey link and revised their responses.
3.3. Round Two
The statements that did not achieve a consensus on clinical relevance in Round One, body mass index (BMI) and “measuring weight when weight restoration is not a treatment goal” did not achieve consensus in Round Two (Table 7). The responses (N = 18) for these components remained low, with a frequency rating of ≤55.6%. The two newly recommended components, “assessing capillary refill rate” and “measuring grip strength”, achieved consensus, with frequency ratings of 88.9% and 100.0%, respectively. No additional additions, omissions, or revisions were suggested. Several new comments for a trauma-informed, culturally sensitive approach were offered, while various comments from Round One were re-stated in Round Two (Table 6).
Table 7.
Round Two domains’ and components’ clinical relevance, consensus determination.
As in Round One, the panelists were emailed personalized feedback forms and offered the opportunity to revise their responses. No panelists requested a new survey link for response revision.
At the end of Round Two, all nine assessment domains (100.0%) and 46 of the 48 (95.8%) final components achieved clinical relevance consensus with no ascendant response change in Round Two for the two remaining components, indicating no need for a third survey round. The research team evaluated the results and closed the study.
3.4. Domain 1—Anthropometrics
All panelists determined that Domain 1 was clinically relevant in an ED-NFPE (100%, n = 22). The panelists endorsed measuring height and growth trajectory using growth charts in children and adolescents and using BMI when plotting it against their growth curve, considering pubertal stage, family heritage, family eating patterns, and other medical and psychological considerations. Clarification was provided in Round Two that measurements in this domain and others could either be performed by the RDN or obtained by another clinician, shared with the RDN, and discussed with the patient in the nutrition assessment. The panelists proposed assessing medical conditions or medications that could affect weight and nutrient needs for all patients.
Panelist Feedback
In the open-ended statement where panelists could provide practice techniques promoting a trauma-informed, culturally specific assessment, multiple panelists recommended asking the patient for permission before weighing them, assessing their fears about being weighed, and discussing with the patient whether they (the patient) should be informed of their weight or if blind weighing (where the patient does not know the number) should be performed. When exact numbers may be triggering, the panelists recommended that the RDN use phrasing like “up, down, the same”, “moving in the right direction”, or “on target”. The panelists also suggested that the RDN convey to the patient that weight is only one component of the overall assessment and not the sole determinant of their health. Individuals, especially those with larger bodies and those who may have a history of weight-related emotional stress, weight bias, and weight shaming or bullying, should be permitted to provide consent for any discussion about weight, shape, size, weight history, and body image.
3.5. Domain 2—General Survey, Cognition, and Neuropsychiatric Symptoms
Domain 2 and its three components were unanimously rated as clinically relevant (100%, n = 22). The panelists recommended having access to other clinicians to provide additional details for the general survey, cognition, and neuropsychiatric symptom assessment. Some panelists suggested that other qualified professionals conduct this domain and that the results be shared with the RDN. The panelists indicated that in addition to asking the patient if they are taking medication regularly and as prescribed, they should ask if they have been prescribed any medication that they may not be taking as prescribed, as this might impact neuropsychiatric symptoms.
Panelist Feedback
The panelists stated that neuropsychiatric symptoms could lead to feelings of being misunderstood and potentially be harmful to some patients, particularly individuals who are neurodivergent. Therefore, this domain would need to be neuro-affirming. Additionally, the panelists suggested that the RDN should observe the patient’s ability to process and respond to questions or statements while asking the patient questions about these symptoms. To be accurately assessed, multiple panelists believed that all components in this domain should consider the involvement of environmental factors like trauma. By considering non-nutrition contributors, the effect of the patient’s nutritional status on cognitive and neuropsychiatric symptoms and changes may be more accurately determined.
3.6. Domain 3—Vital Signs
Vital signs achieved consensus (n = 22), with a 100% frequency rating. Four of the five components were unanimously rated as clinically relevant and achieved a consensus (100%, n = 22). Assessing capillary refill rate was added to the Round Two survey based on the panelist recommendations and additional literature review, and consensus (88.9%) was reached for clinical relevance. In addition to obtaining vital signs in a nutrition examination, several panelists recommended acquiring baseline, historical, or “normal” values from other treatment providers.
Panelist Feedback
The panelists suggested that the patient be informed of each component, how and why it will be performed, and that consent be provided before conducting any vital sign tests. The panelists stressed the importance of assessing the patient’s comfort level and giving reassurance about their autonomy and safety. According to the panelist feedback, blood pressure cuffs should be sized appropriately to accommodate individuals of all sizes and prevent potential traumatization. If preferred, the panelists proposed that the RDN may ask the patient to perform some of these tests independently or have them performed by a medical clinician and shared with the RDN. The panelists mentioned that RDNs who choose not to touch their patients can also ask a medical provider to measure blood pressure and heart rate.
3.7. Domain 4—Bone Loss and Injury, Body Fat, and Muscle Stores
This domain achieved consensus among all panelists (100%, n = 21). All five components achieved consensus, with frequency ratings between 77.3% and 100%. One panelist recommended an additional component, measuring grip strength. This component was added to Round Two and achieved consensus, with a frequency rating of 100% (n = 18).
The panelists recommended that the RDN observe and discuss any concerning changes during each session (e.g., muscle wasting, facial fat loss, etc.), not solely during the examination. The panelists affirmed that grip strength is an easily measured, non-invasive tool to assess malnutrition and can demonstrate muscle loss without emphasizing weight, shape, or body fat.
Panelist Feedback
The panelists recommended only conducting discussions with patients in this domain if relevant to ED recovery. According to the panelists, discussions should honor patients’ experience, autonomy, and safety, approaching each topic with consent and at a pace that meets the person where they can engage in the conversation. Body fat discussions can be re-traumatizing for some individuals with EDs. The clinical relevance of discussions on body fat and muscle should outweigh a patient’s distress. The panelists suggested that the RDN limits feedback on the patient’s body appearance but provides general education about the importance of adequate body stores.
3.8. Domain 5—Hydration Status
Hydration status achieved consensus (n = 21), with a 95.2% frequency rating. The discussion and observation of signs and symptoms of dehydration, overhydration, and abdominal and peripheral edema achieved unanimous consensus (n = 22), with a 100% frequency rating. There was some concern about the panelists’ inexperience in performing edema assessments and when providing telehealth; therefore, the panelists suggested that a medical provider perform the edema assessment. To assess objectivity, the panelists recommended screening for body dysmorphia before inquiring about edema.
Panelist Feedback
The panelists recommended screening for body dysmorphia before inquiring about swelling in the abdomen and ankles. Because “water loading” is common before a patient is weighed, the panelists suggested asking the patient to use the bathroom to urinate just before being weighed.
3.9. Domain 6—Skin, Hands, and Nails
This domain and its four components achieved unanimous consensus (100%, n = 22). Several panelists stated that RDNs could make clinically relevant observations in this domain, but may need additional training to detect signs and symptoms specific to EDs.
Panelist Feedback
Due to skin and nail quality variations among individuals of various races and ethnicities, the panelists suggested that the RDN should not make assumptions about a patient’s “normal” skin and nail quality. According to the panelists, the RDN should initiate a thoughtful discussion of nail and skin changes to ensure cultural competence. To be trauma-informed, the panelists stated that the RDN should be very clear and thoughtful before observing these components so that the patient feels safe and autonomous. The RDN should also discuss the context for the assessment and ask for explicit permission to observe the patient’s skin or hands before the evaluation.
3.10. Domain 7—Hair, Eyelashes, Eyebrows, and Eyes
This domain achieved consensus, with a 95.5% frequency rating. The six components achieved clinical relevance consensus, with frequency ratings between 86.4% and 100%. In addition to the RDN’s assessment, the panelists suggested that the patient’s perception of hair changes (including eyelashes and eyebrows) may also be clinically relevant. The panelists recommended that the RDN ask the patient if they take medications that might impact eye health.
Panelist Feedback
To assess transgender and gender non-conforming (TGNC) patients, the panelists recommended that the RDN be educated on the principles of gender-affirming care and the potential physical changes associated with gender transition. According to the panelist recommendations, for patients who have difficulty making eye contact (neurodiversity or trauma), the RDN should not require the patient to make eye contact during an eye assessment.
3.11. Domain 8—Intraoral, Extraoral, and Neck
The intraoral, extraoral, and neck domain and its six components achieved consensus, with frequency ratings between 86.4% and 100%. The panelists agreed that several critical micronutrient deficiencies are easily visible on the tongue and gingiva and suggested assessing chewing and swallowing issues.
The panelists were more comfortable assessing extraoral versus intraoral changes and more willing to discuss them without observing them. Several panelists stated that medical and dental providers should perform these assessments and share the results with the RDN. RDNs should, however, observe the parotid glands.
Panelist Feedback
The panelists stated that intraoral and extraoral areas are potentially personal and private areas of the body, especially in patients with a trauma history. Therefore, the RDN must be highly skilled and keenly aware of a possible adverse emotional response to this type of assessment. Skin color can impact mucous membrane and gingiva color; therefore, according to the panelists, the RDN should not make assumptions about a patient’s “normal” mucous membrane and gingiva color. The RDN should also ask the patient questions to ensure cultural competence.
3.12. Domain 9—Abdomen (Gastrointestinal)
This domain achieved unanimous consensus (100%, n = 22). The three components within this domain also achieved consensus (86.4–100%). Several panelists stated they would feel comfortable discussing abdominal and gastrointestinal symptoms, but would not observe the abdomen. They would refer the patient to a medical provider and request that they share the results.
Panelist Feedback
The panelists recommended including open-ended questions that permit discussions of race-specific or familial-specific gastrointestinal conditions or predispositions. They also suggested listening sensitively to patients’ concerns about their abdominal or gastrointestinal issues, even if the problem is not physiologically based. According to the panelists, RDNs should be aware that functional gastrointestinal issues are common in patients with EDs, and some patients with functional gastrointestinal disorders may have a history of sexual trauma.
4. Discussion
Individuals with EDs can experience unique, often life-threatening nutrition-related complications [16,20,21,39,57]. The early detection of these complications and a swift nutrition care plan implemented by an RDN are essential components of treatment [27]. Because the traditional NFPE may not thoroughly capture ED-specific nutrition-related complications, an ED-NFPE tool designed to detect these findings could improve the overall nutrition assessment and help to inform treatment [99].
The results of two similar studies indicate the need for disease-specific and population-specific NFPE tools for new and experienced RDNs in various specialties [159,160]. A modified Delphi study was conducted in 2022 by Pike et al. to establish a consensus on the components of the traditional NFPE that would be clinically relevant for detecting the nutrition-related conditions seen explicitly in athletes [159]. In 2023, a modified Delphi study was conducted by Bathgate et al. to examine the need for a modified pediatric NFPE tool specific for infants and children with bronchopulmonary dysplasia (BPD) [160].
In this study, 22 RDN panelists in Round One and 18 in Round Two found the nine ED-NFPE examination domains and 46 of 48 domain components to be clinically relevant for incorporation into an ED-NFPE. Primary ED-NFPE techniques of discussion and observation (with explicit patient permission) were proposed in the place of inspection, palpation, percussion, and auscultation, the traditional NFPE techniques. By conducting a less “invasive” examination, the RDN can assess nutrition-related complications adeptly while ensuring patient autonomy and safety and respecting religious and cultural rules and preferences. The results indicated that the expert panelists predominantly supported these examination techniques.
A unique feature of this study was the qualitative panelist feedback provided for trauma-informed, culturally sensitive practice techniques. The RDN panelists recognized potential trauma and its impact on an individual’s treatment experience. They provided qualitative responses to minimize the risk of inadvertent re-traumatization and optimize treatment adherence and outcomes [9,110,116].
The panelists also provided numerous suggestions for providing a culturally sensitive NFPE, including maintaining a weight-inclusive treatment approach, assessing a patient’s comfort level around weight and body image, and conveying that weight is not the sole determinant of health (state vs. weight) [161].
Although the NFPE is an assessment tool used by RDNs in various clinical settings and performed on numerous patient populations, a common theme in the panelists’ comments was a lack of comfort in performing some examination techniques in several domains. Some panelists stated they would feel comfortable discussing but not observing (i.e., abdominal and intraoral) specific symptoms and observing but not discussing (body fat and muscle) others. They would prefer that a medical provider perform some examination components and share the results with the RDN. The panelists also felt that they needed more training to perform some examination components. Lastly, the panelists who performed telehealth expressed limitations regarding what examination components they could perform.
4.1. Strengths and Limitations
Although the selection of domains and components for the ED-NFPE was based on an extensive literature search, a limitation of this study is that the researchers may have unintentionally introduced bias in statement wording and the choice of ED-specific domains and examination techniques. RDN panelists unfamiliar or uncomfortable with the domains and components may have introduced bias into their survey responses, and their answers may have been influenced by their personal or professional bias [125]. Although all panelists had wide-ranging experience in ED care, it was unclear if they had extensive experience in trauma-informed care or exhibited cultural, racial, or other forms of diversity, possibly introducing bias into their responses. Detailed narratives preceded survey statements. However, the panelists may not have completely understood the statements, and an opportunity for statement clarification was only made available in the following round (Round Two) [65].
Another limitation was that consensus cutoffs included neutral ratings. “Neither agree nor disagree” responses may not have indicated that the panelists supported the statement. Lastly, while panelist group size varies between 10 and 100 in most published Delphi studies, a limitation of this study is the panelist group size of 22 [123].
A significant strength of this study is that consensus was achieved in all nine domains and 46 of the final 48 components. Another strength and core objective of the study is the extensive qualitative feedback that the panelists provided in all domains. The retention rate was high, with 22 panelists in Round One and 18 panelists in Round Two (81.8% retention).
4.2. Implications of Findings
A thorough trauma-informed, culturally sensitive ED-NFPE tool will close the gap in ED patient care by enabling RDNs to skillfully conduct detailed, comprehensive nutrition assessments of individuals in this population. An ED-NFPE could be utilized at the onset and throughout treatment to evaluate changes in nutritional status during the re-nourishment and recovery process. RDNs could use this tool at the individual outpatient level of care through to the acute inpatient treatment level.
RDNs in various clinical and non-clinical settings and those with limited ED expertise could use an ED-NFPE tool as a resource to help identify potential ED-related nutritional findings, provide appropriate treatment referrals, and improve patient care.
Several factors, including a lack of experience or knowledge of the NFPE, time constraints, and a lack of confidence, autonomy, and training, may limit RDNs’ use of the NFPE [162,163]. Formal NFPE training for general practice RDNs, RDNs in ED care, and students enrolled in accredited dietetics programs could provide ample knowledge and hands-on experience to remove potential barriers to conducting comprehensive disease-specific or population-specific nutrition examinations, such as an ED-NFPE [164].
5. Conclusions
In-depth ED-specific assessments and multidisciplinary treatment are vital to reduce or eliminate ED behaviors and minimize, eliminate, or reverse potential nutrition-based medical complications [3]. The RDN is a crucial treatment team member at every level of care [3,27]. To provide optimal ED nutrition care, evidence-based standards and guidelines must be developed for RDNs. The results of this study show that a trauma-informed, culturally competent ED-NFPE tool can not only improve the nutrition assessment of individuals with EDs, but can potentially improve the overall patient experience.
Future studies can build on this study’s results to develop and validate ED-NFPE tool components and evidence-based guidelines for their use, explore the tool’s impact on patient outcomes, and obtain patient feedback on the examination experience. The further development and validation of an ED-NFPE tool and professional NFPE training for RDNs will help to direct nutrition interventions and improve patient outcomes.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu17091449/s1, the “Eating Disorders Nutrition Assessment Tool” Survey.
Author Contributions
D.G., A.B., L.B.-G., D.R.-R. and J.Z. equally contributed to the conceptualization and methodology of the study; D.G. contributed to the curation and analysis of the data, contributed to the interpretation of the data, and drafted the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Rutgers University Institutional Review Board approved the study protocol and consent for panelists’ screening and participation (Pro2023002454, 27 March 2024). The study was conducted by the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting the conclusions of this article will be made available by the corresponding author on request due to privacy reasons.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ED | Eating Disorder |
| NFPE | Nutrition Focused Physical Examination |
| RDN | Registered Dietitian Nutritionist |
| IAEDP | International Association of Eating Disorder Professionals |
| LGBTQ+ | Lesbian, Gay, Bisexual, Transgender, Queer, and Others |
| APA | American Psychiatric Association |
| BMI | Body Mass Index |
| SAMHSA | Substance Abuse and Mental Health Services Administration |
| TGD | Transgender and Gender Diverse |
| AED | Academy for Eating Disorders |
| AND | Academy of Nutrition and Dietetics |
| EDRD Pro | Eating Disorder Registered Dietitians and Professionals |
| IFEDD | International Federation of Eating Disorder Dietitians |
| CREDES | Conducting and Reporting of Delphi Studies |
| SD | Standard Deviation |
| PHP | Partial Hospitalization Program |
| IOP | Intensive Outpatient Program |
| BIPOC | Black, Indigenous, and People of Color |
| BPD | Bronchopulmonary Dysplasia |
References
- Maine, M.; Bunnell, D.W. Chapter 1—A Perfect Biopsychosocial Storm: Gender, Culture, and Eating Disorders. In Treatment of Eating Disorders; Maine, M., McGilley, B.H., Bunnell, D.W., Eds.; Academic Press: San Diego, CA, USA, 2010; pp. 3–16. [Google Scholar]
- National Association of Anorexia Nervosa and Associated Disorders. Eating Disorder Statistics. Available online: https://anad.org/eating-disorder-statistic/ (accessed on 8 June 2024).
- Hackert, A.N.; Kniskern, M.A.; Beasley, T.M. Academy of Nutrition and Dietetics: Revised 2020 Standards of Practice and Standards of Professional Performance for Registered Dietitian Nutritionists (Competent, Proficient, and Expert) in Eating Disorders. J. Acad. Nutr. Diet. 2020, 120, 1902–1919. [Google Scholar] [CrossRef] [PubMed]
- Diemer, E.W.; Grant, J.D.; Munn-Chernoff, M.A.; Patterson, D.A.; Duncan, A.E. Gender Identity, Sexual Orientation, and Eating-Related Pathology in a National Sample of College Students. J. Adolesc. Health 2015, 57, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Halls, D.; Byford, S.; Tchanturia, K. Autistic characteristics in eating disorders: Treatment adaptations and impact on clinical outcomes. Eur. Eat. Disord. Rev. 2022, 30, 671–690. [Google Scholar] [CrossRef] [PubMed]
- Ralph, A.F.; Brennan, L.; Byrne, S.; Caldwell, B.; Farmer, J.; Hart, L.M.; Heruc, G.A.; Maguire, S.; Piya, M.K.; Quin, J.; et al. Management of eating disorders for people with higher weight: Clinical practice guideline. J. Eat. Disord. 2022, 10, 121. [Google Scholar] [CrossRef]
- Solmi, F.; Bentivegna, F.; Bould, H.; Mandy, W.; Kothari, R.; Rai, D.; Skuse, D.; Lewis, G. Trajectories of autistic social traits in childhood and adolescence and disordered eating behaviours at age 14 years: A UK general population cohort study. J. Child Psychol. Psychiatry 2021, 62, 75–85. [Google Scholar] [CrossRef]
- Convertino, A.D.; Morland, L.A.; Blashill, A.J. Trauma exposure and eating disorders: Results from a United States nationally representative sample. Int. J. Eat. Disord. 2022, 55, 1079–1089. [Google Scholar] [CrossRef]
- Brewerton, T.D. An Overview of Trauma-Informed Care and Practice for Eating Disorders. J. Aggress. Maltreatment Trauma 2019, 28, 445–462. [Google Scholar] [CrossRef]
- Backholm, K.; Isomaa, R.; Birgegård, A. The prevalence and impact of trauma history in eating disorder patients. Eur. J. Psychotraumatol. 2013, 4, 22482. [Google Scholar] [CrossRef]
- Mascolo, M.; Geer, B.; Feuerstein, J.; Mehler, P.S. Gastrointestinal comorbidities which complicate the treatment of anorexia nervosa. Eat. Disord. 2017, 25, 122–133. [Google Scholar] [CrossRef]
- Udo, T.; Grilo, C.M. Psychiatric and medical correlates of DSM-5 eating disorders in a nationally representative sample of adults in the United States. Int. J. Eat. Disord. 2019, 52, 42–50. [Google Scholar] [CrossRef]
- Riehl, M.E.; Scarlata, K. Understanding disordered eating risks in patients with gastrointestinal conditions. J. Acad. Nutr. Diet. 2022, 122, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Harvard T.H. Chan—School of Public Health. Strategic Training Initiative for the Prevention of Eating Disorders. Report: Economic Costs of Eating Disorders. Available online: https://www.hsph.harvard.edu/striped/report-economic-costs-of-eating-disorders/ (accessed on 16 July 2024).
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of eating disorders over the 2000–2018 period: A systematic literature review. Am. J. Clin. Nutr. 2019, 109, 1402–1413. [Google Scholar] [CrossRef] [PubMed]
- Mehler, P.S.; Blalock, D.V.; Walden, K.; Kaur, S.; McBride, J.; Walsh, K.; Watts, J. Medical findings in 1,026 consecutive adult inpatient–residential eating disordered patients. Int. J. Eat. Disord. 2018, 51, 305–313. [Google Scholar] [CrossRef]
- Hanachi, M.; Dicembre, M.; Rives-Lange, C.; Ropers, J.; Bemer, P.; Zazzo, J.F.; Poupon, J.; Dauvergne, A.; Melchior, J.C. Micronutrients Deficiencies in 374 Severely Malnourished Anorexia Nervosa Inpatients. Nutrients 2019, 11, 792. [Google Scholar] [CrossRef] [PubMed]
- Westmoreland, P.; Krantz, M.J.; Mehler, P.S. Medical Complications of Anorexia Nervosa and Bulimia. Am. J. Med. 2016, 129, 30–37. [Google Scholar] [CrossRef]
- Wassenaar, E.; Friedman, J.; Mehler, P.S. Medical complications of binge eating disorder. Psychiatr. Clin. 2019, 42, 275–286. [Google Scholar] [CrossRef]
- Forney, K.J.; Buchman-Schmitt, J.M.; Keel, P.K.; Frank, G.K.W. The medical complications associated with purging. Int. J. Eat. Disord. 2016, 49, 249–259. [Google Scholar] [CrossRef]
- Gaudiani, J.L.; Brinton, J.T.; Sabel, A.L.; Rylander, M.; Catanach, B.; Mehler, P.S. Medical outcomes for adults hospitalized with severe anorexia nervosa: An analysis by age group. Int. J. Eat. Disord. 2016, 49, 378–385. [Google Scholar] [CrossRef]
- Lin, J.A.; Woods, E.R.; Bern, E.M. Common and Emergent Oral and Gastrointestinal Manifestations of Eating Disorders. Gastroenterol. Hepatol. 2021, 17, 157–167. [Google Scholar]
- Peebles, R.; Sieke, E.H. Medical complications of eating disorders in youth. Child Adolesc. Psychiatr. Clin. 2019, 28, 593–615. [Google Scholar] [CrossRef]
- Strumia, R. Eating disorders and the skin. Clin. Dermatol. 2013, 31, 80–85. [Google Scholar] [CrossRef]
- Lourenço, M.; Azevedo, Á.; Brandão, I.; Gomes, P.S. Orofacial manifestations in outpatients with anorexia nervosa and bulimia nervosa focusing on the vomiting behavior. Clin. Oral Investig. 2018, 22, 1915–1922. [Google Scholar] [CrossRef] [PubMed]
- Gibson, D.; Workman, C.; Mehler, P.S. Medical complications of anorexia nervosa and bulimia nervosa. Psychiatr. Clin. 2019, 42, 263–274. [Google Scholar] [CrossRef]
- Academy for Eating Disorders Nutrition Working Group. Guidebook for Nutrition Treatment of Eating Disorders. Available online: https://higherlogicdownload.s3.amazonaws.com/AEDWEB/27a3b69a-8aae-45b2-a04c-2a078d02145d/UploadedImages/Publications_Slider/FINAL_AED_Purple_Nutrition_Book.pdf (accessed on 14 July 2024).
- American Psychiatric Association. Feeding and Eating Disorders. In Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2023. [Google Scholar]
- Stamu-O’Brien, C.; Shivakumar, S.; Messas, T.; Kroumpouzos, G. Through the looking glass: Skin signs that help diagnose eating disorders. Clin. Dermatol. 2023, 41, 67–74. [Google Scholar] [CrossRef]
- Johansson, A.-K.; Norring, C.; Unell, L.; Johansson, A. Eating disorders and oral health: A matched case–control study. Eur. J. Oral Sci. 2012, 120, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Paszynska, E.; Dutkiewicz, A.; Osinska, A.; Mozol-Jursza, M.; Smalc, N.; Tyszkiewicz-Nwafor, M.; Dmitrzak-Weglarz, M.; Slopien, A.; Jenerowicz, D. Anorexia Nervosa with Vomiting Episodes: Dermatological and Oral Complications. Eur. J. Dent. 2020, 14, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Uhlen, M.-M.; Tveit, A.B.; Refsholt Stenhagen, K.; Mulic, A. Self-induced vomiting and dental erosion—A clinical study. BMC Oral Health 2014, 14, 92. [Google Scholar] [CrossRef]
- Mehler, P.S.; Brown, C. Anorexia nervosa—Medical complications. J. Eat. Disord. 2015, 3, 11. [Google Scholar] [CrossRef]
- Mehler, P.S.; Rylander, M. Bulimia Nervosa—Medical complications. J. Eat. Disord. 2015, 3, 12. [Google Scholar] [CrossRef]
- Miller, K.K.; Grinspoon, S.K.; Ciampa, J.; Hier, J.; Herzog, D.; Klibanski, A. Medical Findings in Outpatients With Anorexia Nervosa. Arch. Intern. Med. 2005, 165, 561–566. [Google Scholar] [CrossRef]
- Casiero, D.; Frishman, W.H. Cardiovascular complications of eating disorders. Cardiol. Rev. 2006, 14, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Cass, K.; McGuire, C.; Bjork, I.; Sobotka, N.; Walsh, K.; Mehler, P.S. Medical Complications of Anorexia Nervosa. Psychosomatics 2020, 61, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Bahia, A.; Mascolo, M.; Gaudiani, J.L.; Mehler, P.S. PseudoBartter syndrome in eating disorders. Int. J. Eat. Disord. 2012, 45, 150–153. [Google Scholar] [CrossRef]
- Cremonini, F.; Camilleri, M.; Clark, M.M.; Beebe, T.J.; Locke, G.R.; Zinsmeister, A.R.; Herrick, L.M.; Talley, N.J. Associations among binge eating behavior patterns and gastrointestinal symptoms: A population-based study. Int. J. Obes. 2009, 33, 342–353. [Google Scholar] [CrossRef]
- Duriez, P.; Mastellari, T.; Viltart, O.; Gorwood, P. Clinical meaning of body temperatures in anorexia nervosa and bulimia nervosa. Eur. Eat. Disord. Rev. 2022, 30, 124–134. [Google Scholar] [CrossRef] [PubMed]
- El Ghoch, M.; Calugi, S.; Lamburghini, S.; Dalle Grave, R. Anorexia Nervosa and Body Fat Distribution: A Systematic Review. Nutrients 2014, 6, 3895–3912. [Google Scholar] [CrossRef]
- Fischer, M.; JeVenn, A.; Hipskind, P. Evaluation of Muscle and Fat Loss as Diagnostic Criteria for Malnutrition. Nutr. Clin. Pract. 2015, 30, 239–248. [Google Scholar] [CrossRef]
- Holmes, S.R.M.; Sabel, A.L.; Gaudiani, J.L.; Gudridge, T.; Brinton, J.T.; Mehler, P.S. Prevalence and management of oropharyngeal dysphagia in patients with severe anorexia nervosa: A large retrospective review. Int. J. Eat. Disord. 2016, 49, 159–166. [Google Scholar] [CrossRef]
- Quesnel, D.A.; Cooper, M.; Fernandez-del-Valle, M.; Reilly, A.; Calogero, R.M. Medical and physiological complications of exercise for individuals with an eating disorder: A narrative review. J. Eat. Disord. 2023, 11, 3. [Google Scholar] [CrossRef]
- Roerig, J.L.; Steffen, K.J.; Mitchell, J.E.; Zunker, C. Laxative Abuse: Epidemiology, Diagnosis and Management. Drugs 2010, 70, 1487–1503. [Google Scholar] [CrossRef]
- Santangelo, G.; Bursi, F.; Toriello, F.; Tamagni, M.E.; Fior, G.; Massironi, L.; Bertelli, S.; Fanin, A.; Gambini, O.; Carugo, S.; et al. Echocardiographic changes in anorexia nervosa: A pathophysiological adaptation or a disease? Intern. Emerg. Med. 2022, 17, 777–787. [Google Scholar] [CrossRef] [PubMed]
- Sansone, R.A.; Sansone, L.A. Hoarseness: A sign of self-induced vomiting? Innov. Clin. Neurosci. 2012, 9, 37–41. [Google Scholar]
- Silva, V.; Schukow, C.P.; Restini, C.B.A. Striae distensae as a diagnostic indicator for eating disorder pathologies. Int. J. Dermatol. 2023, 62, 715–722. [Google Scholar] [CrossRef]
- Solmi, M.; Veronese, N.; Correll, C.U.; Favaro, A.; Santonastaso, P.; Caregaro, L.; Vancampfort, D.; Luchini, C.; De Hert, M.; Stubbs, B. Bone mineral density, osteoporosis, and fractures among people with eating disorders: A systematic review and meta-analysis. Acta Psychiatr. Scand. 2016, 133, 341–351. [Google Scholar] [CrossRef]
- Tamiya, H.; Ouchi, A.; Chen, R.; Miyazawa, S.; Akimoto, Y.; Kaneda, Y.; Sora, I. Neurocognitive impairments are more severe in the binge-eating/purging anorexia nervosa subtype than in the restricting subtype. Front. Psychiatry 2018, 9, 138. [Google Scholar] [CrossRef]
- Yahalom, M.; Spitz, M.; Sandler, L.; Heno, N.; Roguin, N.; Turgeman, Y. The significance of bradycardia in anorexia nervosa. Int. J. Angiol. 2013, 22, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Mascolo, M.; Chu, E.S.; Mehler, P.S. Abuse and clinical value of diuretics in eating disorders therapeutic applications. Int. J. Eat. Disord. 2011, 44, 200–202. [Google Scholar] [CrossRef]
- Mascolo, M.; Dee, E.; Townsend, R.; Brinton, J.T.; Mehler, P.S. Severe gastric dilatation due to superior mesenteric artery syndrome in anorexia nervosa. Int. J. Eat. Disord. 2015, 48, 532–534. [Google Scholar] [CrossRef] [PubMed]
- Klein, D.A.; Sylvester, J.E.; Schvey, N.A. Eating Disorders in Primary Care: Diagnosis and Management. Am. Fam. Physician 2021, 103, 22–32. [Google Scholar]
- Vall, E.; Wade, T.D. Predictors of treatment outcome in individuals with eating disorders: A systematic review and meta-analysis. Int. J. Eat. Disord. 2015, 48, 946–971. [Google Scholar] [CrossRef]
- Academy for Eating Disorders’ (AED) Medical Care Standards Committee. AED Eating Disorders: A Guide to Medical Care; Academy for Eating Disorders: Wakefield, MA, USA, 2021. [Google Scholar]
- Fichter, M.M.; Quadflieg, N. Mortality in eating disorders—Results of a large prospective clinical longitudinal study. Int. J. Eat. Disord. 2016, 49, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Crone, C.; Fochtmann, L.J.; Attia, E.; Boland, R.; Escobar, J.; Fornari, V.; Golden, N.; Guarda, A.; Jackson-Triche, M.; Manzo, L.; et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Eating Disorders. Am. J. Psychiatry 2023, 180, 167–171. [Google Scholar] [CrossRef]
- Andersen, D.; Baird, S.; Bates, T.; Chapel, D.L.; Cline, A.D.; Ganesh, S.N.; Garner, M.; Grant, B.L.; Hamilton, K.K.; Jablonski, K.; et al. Academy of Nutrition and Dietetics: Revised 2017 Standards of Practice in Nutrition Care and Standards of Professional Performance for Registered Dietitian Nutritionists. J. Acad. Nutr. Diet. 2018, 118, 132–140.e15. [Google Scholar] [CrossRef]
- Fuller, S.J.; Philpot, U.; Group, W. The development of consensus-based guidelines for dietetic practice in nasogastric tube feeding under restraint for patients with anorexia nervosa using a modified Delphi process. J. Hum. Nutr. Diet. 2020, 33, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Garber, A.K.; Sawyer, S.M.; Golden, N.H.; Guarda, A.S.; Katzman, D.K.; Kohn, M.R.; Le Grange, D.; Madden, S.; Whitelaw, M.; Redgrave, G.W. A systematic review of approaches to refeeding in patients with anorexia nervosa. Int. J. Eat. Disord. 2016, 49, 293–310. [Google Scholar] [CrossRef] [PubMed]
- Harrington, B.C.; Jimerson, M.; Haxton, C.; Jimerson, D.C. Initial evaluation, diagnosis, and treatment of anorexia nervosa and bulimia nervosa. Am. Fam. Physician 2015, 91, 46–52. [Google Scholar]
- Hornberger, L.L.; Lane, M.A.; Lane, M.; Breuner, C.C.; Alderman, E.M.; Grubb, L.K.; Powers, M.; Upadhya, K.K.; Wallace, S.B.; Loveless, M. Identification and management of eating disorders in children and adolescents. Pediatrics 2021, 147, e2020040279. [Google Scholar] [CrossRef]
- Linsenmeyer, W.; McGuire, J.; Patel, M.; Theobald, N.; Helein, A. Conducting a Nutrition-Focused Physical Examination on a Transgender Patient: Considerations for Registered Dietitian Nutritionists. J. Acad. Nutr. Diet. 2025, S2212–S2672. [Google Scholar] [CrossRef]
- Mittnacht, A.M.; Bulik, C.M. Best nutrition counseling practices for the treatment of anorexia nervosa: A Delphi study. Int. J. Eat. Disord. 2015, 48, 111–122. [Google Scholar] [CrossRef]
- Peebles, R.; Hardy, K.K.; Wilson, J.L.; Lock, J.D. Are Diagnostic Criteria for Eating Disorders Markers of Medical Severity? Pediatrics 2010, 125, e1193–e1201. [Google Scholar] [CrossRef]
- Setnick, J. Micronutrient Deficiencies and Supplementation in Anorexia and Bulimia Nervosa. Nutr. Clin. Pract. 2010, 25, 137–142. [Google Scholar] [CrossRef]
- Watson, H.J.; Bulik, C.M. Update on the treatment of anorexia nervosa: Review of clinical trials, practice guidelines and emerging interventions. Psychol. Med. 2013, 43, 2477–2500. [Google Scholar] [CrossRef]
- White, J.V.; Guenter, P.; Jensen, G.; Malone, A.; Schofield, M.; Academy Malnutrition Work Group; A.S.P.E.N. Malnutrition Task Force; A.S.P.E.N. Board of Directors. Consensus Statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition. J. Parenter. Enter. Nutr. 2012, 36, 275–283. [Google Scholar] [CrossRef]
- Heruc, G.; Hart, S.; Stiles, G.; Fleming, K.; Casey, A.; Sutherland, F.; Jeffrey, S.; Roberton, M.; Hurst, K. ANZAED practice and training standards for dietitians providing eating disorder treatment. J. Eat. Disord. 2020, 8, 77. [Google Scholar] [CrossRef]
- McCuen-Wurst, C.; Ruggieri, M.; Allison, K.C. Disordered eating and obesity: Associations between binge-eating disorder, night-eating syndrome, and weight-related comorbidities. Ann. N. Y. Acad. Sci. 2018, 1411, 96–105. [Google Scholar] [CrossRef]
- National Eating Disorders Association. Statistics and Research on Eating Disorders. Available online: https://www.nationaleatingdisorders.org/statistics-research-eating-disorders (accessed on 17 July 2024).
- Doyle, E.A.; Quinn, S.M.; Ambrosino, J.M.; Weyman, K.; Tamborlane, W.V.; Jastreboff, A.M. Disordered Eating Behaviors in Emerging Adults With Type 1 Diabetes: A Common Problem for Both Men and Women. J. Pediatr. Health Care 2017, 31, 327–333. [Google Scholar] [CrossRef]
- Send, S. Cultural Competence and Nutrition-focused Physical Exam. Support Line 2023, 45, 14–19. [Google Scholar]
- Smolak, L.; Murnen, S.K.; Ruble, A.E. Female athletes and eating problems: A meta-analysis. Int. J. Eat. Disord. 2000, 27, 371–380. [Google Scholar] [CrossRef]
- Knapp, J.; Aerni, G.; Anderson, J. Eating Disorders in Female Athletes: Use of Screening Tools. Curr. Sports Med. Rep. 2014, 13, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Mulchandani, M.; Shetty, N.; Conrad, A.; Muir, P.; Mah, B. Treatment of eating disorders in older people: A systematic review. Syst. Rev. 2021, 10, 275. [Google Scholar] [CrossRef] [PubMed]
- Chouraqui, J.-P.; Turck, D.; Briend, A.; Darmaun, D.; Bocquet, A.; Feillet, F.; Frelut, M.-L.; Girardet, J.-P.; Guimber, D.; Hankard, R.; et al. Religious dietary rules and their potential nutritional and health consequences. Int. J. Epidemiol. 2020, 50, 12–26. [Google Scholar] [CrossRef]
- Sala, M.; Reyes-Rodríguez, M.L.; Bulik, C.M.; Bardone-Cone, A. Race, ethnicity, and eating disorder recognition by peers. Eat. Disord. 2013, 21, 423–436. [Google Scholar] [CrossRef]
- Kamody, R.C.; Grilo, C.M.; Udo, T. Disparities in DSM-5 defined eating disorders by sexual orientation among U.S. adults. Int. J. Eat. Disord. 2020, 53, 278–287. [Google Scholar] [CrossRef]
- Sato, Y.; Fukudo, S. Gastrointestinal symptoms and disorders in patients with eating disorders. Clin. J. Gastroenterol. 2015, 8, 255–263. [Google Scholar] [CrossRef]
- Elizabeth, J.; Andrea, K.; Aurelia, N. 2016 update on eating disorders in athletes: A comprehensive narrative review with a focus on clinical assessment and management. Br. J. Sports Med. 2016, 50, 154. [Google Scholar] [CrossRef]
- Tu, C.-Y.; Meg Tseng, M.-C.; Chang, C.-H. Night eating syndrome in patients with eating disorders: Is night eating syndrome distinct from bulimia nervosa? J. Formos. Med. Assoc. 2019, 118, 1038–1046. [Google Scholar] [CrossRef]
- Barry, M.R.; Sonneville, K.R.; Leung, C.W. Students with Food Insecurity Are More Likely to Screen Positive for an Eating Disorder at a Large, Public University in the Midwest. J. Acad. Nutr. Diet. 2021, 121, 1115–1124. [Google Scholar] [CrossRef]
- Colton, P.A.; Olmsted, M.P.; Daneman, D.; Farquhar, J.C.; Wong, H.; Muskat, S.; Rodin, G.M. Eating disorders in girls and women with type 1 diabetes: A longitudinal study of prevalence, onset, remission, and recurrence. Diabetes Care 2015, 38, 1212–1217. [Google Scholar] [CrossRef]
- Bahji, A.; Mazhar, M.N.; Hudson, C.C.; Nadkarni, P.; MacNeil, B.A.; Hawken, E. Prevalence of substance use disorder comorbidity among individuals with eating disorders: A systematic review and meta-analysis. Psychiatry Res. 2019, 273, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Durso, L.E.; Latner, J.D. Understanding Self-directed Stigma: Development of the Weight Bias Internalization Scale. Obesity 2008, 16, S80–S86. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L.; White, M.A.; Grilo, C.M. Weight bias internalization, depression, and self-reported health among overweight binge eating disorder patients. Obesity 2014, 22, E142–E148. [Google Scholar] [CrossRef] [PubMed]
- Castellini, G.; Trisolini, F.; Ricca, V. Psychopathology of eating disorders. J. Psychopathol. 2014, 20, 461–470. [Google Scholar]
- Academy of Nutrition and Dietetics. NCP Step 1: Nutrition Assessment. Available online: https://www.ncpro.org/pubs/2020-encpt-en/page-026 (accessed on 26 August 2024).
- Academy of Nutrition and Dietetics. Electronic Nutrition Care Process Terminology. Available online: https://ncpro.org/?set_ga_opt_in_cookie=1&set_ga_opt_in=Save+Settings (accessed on 13 April 2025).
- Esper, D.H. Utilization of Nutrition-Focused Physical Assessment in Identifying Micronutrient Deficiencies. Nutr. Clin. Pract. 2015, 30, 194–202. [Google Scholar] [CrossRef]
- Pogatshnik, C.; Hamilton, C. Nutrition-focused physical examination: Skin, nails, hair, eyes and oral cavity. Support Line 2011, 33, 7–13. [Google Scholar]
- Hammond, M.I.; Myers, E.F.; Trostler, N. Nutrition Care Process and Model: An Academic and Practice Odyssey. J. Acad. Nutr. Diet. 2014, 114, 1879–1894. [Google Scholar] [CrossRef]
- Lebow, J.; Sim, L.A.; Kransdorf, L.N. Prevalence of a History of Overweight and Obesity in Adolescents With Restrictive Eating Disorders. J. Adolesc. Health 2015, 56, 19–24. [Google Scholar] [CrossRef]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut Off Points; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Eiring, K.; Wiig Hage, T.; Reas, D.L. Exploring the experience of being viewed as “not sick enough”: A qualitative study of women recovered from anorexia nervosa or atypical anorexia nervosa. J. Eat. Disord. 2021, 9, 142. [Google Scholar] [CrossRef]
- Forney, K.J.; Brown, T.A.; Holland-Carter, L.A.; Kennedy, G.A.; Keel, P.K. Defining “significant weight loss” in atypical anorexia nervosa. Int. J. Eat. Disord. 2017, 50, 952–962. [Google Scholar] [CrossRef] [PubMed]
- Academy of Nutrition and Dietetics. Nutrition-Focused Physical Findings. Available online: https://www.nutritioncaremanual.org/topic.cfm?ncm_category_id=11&lv1=64571&lv2=273972&lv3=273975&ncm_toc_id=273975&ncm_heading=Resources (accessed on 16 July 2024).
- Detsky, A.; JR, M.; Baker, J.; Johnston, N.; Whittaker, S.; Mendelson, R.; Jeejeebhoy, K. What is subjective global assessment of nutritional status? J. Parenter. Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Kilde, K.; Nitzsche, L. Nutrition-focused Physical Examination: A Head-to-Toe Approach with a Focus on Micronutrient Deficiencies. Support Line 2016, 38, 3–9. [Google Scholar]
- Hummell, A.C.; Cummings, M. Role of the nutrition-focused physical examination in identifying malnutrition and its effectiveness. Nutr. Clin. Pract. 2022, 37, 41–49. [Google Scholar] [CrossRef]
- Radler, D.R.; Lister, T. Nutrient Deficiencies Associated With Nutrition-Focused Physical Findings of the Oral Cavity. Nutr. Clin. Pract. 2013, 28, 710–721. [Google Scholar] [CrossRef]
- Pinhas, L.; Morris, A.; Crosby, R.D.; Katzman, D.K. Incidence and Age-Specific Presentation of Restrictive Eating Disorders in Children: A Canadian Paediatric Surveillance Program Study. Arch. Pediatr. Adolesc. Med. 2011, 165, 895–899. [Google Scholar] [CrossRef]
- Chen, S.T.; Ong, S.H.; Lim, P.Y.; Chong, K.S. Nutrition-Focused Physical Exam in assessing nutritional status of children with neurological impairment. Hum. Nutr. Metab. 2024, 37, 200279. [Google Scholar] [CrossRef]
- Saha, S.; Beach, M.C.; Cooper, L.A. Patient centeredness, cultural competence and healthcare quality. J. Natl. Med. Assoc. 2008, 100, 1275–1285. [Google Scholar] [CrossRef]
- Schwartz, D.B. Integrating Patient-Centered Care and Clinical Ethics Into Nutrition Practice. Nutr. Clin. Pract. 2013, 28, 543–555. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach; HHS Publication No. (SMA) 14-4884; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2014. [Google Scholar]
- Substance Abuse and Mental Health Services Administration; Center for Substance Abuse Treatment. A Treatment Improvement Protocol Trauma-Informed Care in Behavioral Health Services; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2014. [Google Scholar]
- Diemer, E.W.; White Hughto, J.M.; Gordon, A.R.; Guss, C.; Austin, S.B.; Reisner, S.L. Beyond the Binary: Differences in Eating Disorder Prevalence by Gender Identity in a Transgender Sample. Transgend. Health 2018, 3, 17–23. [Google Scholar] [CrossRef]
- Mujallad, A. CNE SERIES. Modesty Among Muslim Women: Implications for Nursing Care. MEDSURG Nurs. 2016, 25, 169–172. [Google Scholar] [PubMed]
- Sabin, J.A.; Riskind, R.G.; Nosek, B.A. Health Care Providers’ Implicit and Explicit Attitudes Toward Lesbian Women and Gay Men. Am. J. Public Health 2015, 105, 1831–1841. [Google Scholar] [CrossRef] [PubMed]
- Riddle, M.C.; Safer, J.D. Medical considerations in the care of transgender and gender diverse patients with eating disorders. J. Eat. Disord. 2022, 10, 178. [Google Scholar] [CrossRef] [PubMed]
- Elliott, D.E.; Bjelajac, P.; Fallot, R.D.; Markoff, L.S.; Reed, B.G. Trauma-informed or trauma-denied: Principles and implementation of trauma-informed services for women. J. Community Psychol. 2005, 33, 461–477. [Google Scholar] [CrossRef]
- Fallot, R.; Harris, M. Creating Cultures of Trauma-Informed Care: A Self-Assessment and Planning Protocol; Community Connections: Washington, DC, USA, 2009. [Google Scholar]
- Academy for Eating Disorders. About AED. Available online: https://www.aedweb.org/about-aed/who-we-are (accessed on 8 July 2024).
- Academy of Nutrition and Dietetics. Behavioral Health Nutrition: A Dietetic Practice Group of the Academy of Nutrition and Dietetics. Available online: https://www.bhndpg.org/bhn-knowledge-basecamp (accessed on 10 July 2024).
- Eating Disorder Registered Dietitians and Professionals. EDRDPRO Eating Disorder Registered Dietitians and Profesionals. Available online: https://edrdpro.com/ (accessed on 26 August 2024).
- International Federation of Eating Disorder Dietitians. Welcome to the International Federation of Eating Disorder Dietitians. Available online: https://ifedd.org/ (accessed on 10 June 2024).
- Nasa, P.; Jain, R.; Juneja, D. Delphi methodology in healthcare research: How to decide its appropriateness. World J. Methodol. 2021, 11, 116–129. [Google Scholar] [CrossRef] [PubMed]
- White, R.E.; Cooper, K. Grounded Theory. In Qualitative Research in the Post-Modern Era: Critical Approaches and Selected Methodologies; White, R.E., Cooper, K., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 339–385. [Google Scholar]
- Humphrey-Murto, S.; Varpio, L.; Gonsalves, C.; Wood, T.J. Using consensus group methods such as Delphi and Nominal Group in medical education research. Med. Teach. 2017, 39, 14–19. [Google Scholar] [CrossRef]
- Jorm, A.F. Using the Delphi expert consensus method in mental health research. Aust. N. Z. J. Psychiatry 2015, 49, 887–897. [Google Scholar] [CrossRef]
- McMaster, C.M.; Wade, T.; Franklin, J.; Hart, S. Development of consensus-based guidelines for outpatient dietetic treatment of eating disorders: A Delphi study. Int. J. Eat. Disord. 2020, 53, 1480–1495. [Google Scholar] [CrossRef]
- Kankam, P.K. The use of paradigms in information research. Libr. Inf. Sci. Res. 2019, 41, 85–92. [Google Scholar] [CrossRef]
- Lee, K.M.; Hunger, J.M.; Tomiyama, A.J. Weight stigma and health behaviors: Evidence from the Eating in America Study. Int. J. Obes. 2021, 45, 1499–1509. [Google Scholar] [CrossRef]
- Giovinazzo, S.; Sukkar, S.G.; Rosa, G.M.; Zappi, A.; Bezante, G.P.; Balbi, M.; Brunelli, C. Anorexia nervosa and heart disease: A systematic review. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2019, 24, 199–207. [Google Scholar] [CrossRef]
- Klinkby Støving, R.; Bennedbæk, F.N.; Hegedüs, L.; Hagen, C. Evidence of diffuse atrophy of the thyroid gland in patients with anorexia nervosa. Int. J. Eat. Disord. 2001, 29, 230–235. [Google Scholar] [CrossRef]
- Fleming, S.; Gill, P.; Jones, C.; Taylor, J.A.; Van den Bruel, A.; Heneghan, C.; Roberts, N.; Thompson, M. The Diagnostic Value of Capillary Refill Time for Detecting Serious Illness in Children: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0138155. [Google Scholar] [CrossRef] [PubMed]
- Bulik, C.M.; Carroll, I.M.; Mehler, P. Reframing anorexia nervosa as a metabo-psychiatric disorder. Trends Endocrinol. Metab. 2021, 32, 752–761. [Google Scholar] [CrossRef]
- Gaudiani, J.L.; Sabel, A.L.; Mascolo, M.; Mehler, P.S. Severe anorexia nervosa: Outcomes from a medical stabilization unit. Int. J. Eat. Disord. 2012, 45, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Frølich, J.; Winkler, L.A.; Abrahamsen, B.; Bilenberg, N.; Hermann, A.P.; Støving, R.K. Fractures in women with eating disorders—Incidence, predictive factors, and the impact of disease remission: Cohort study with background population controls. Int. J. Eat. Disord. 2020, 53, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Legroux, I.; Cortet, B. Factors influencing bone loss in anorexia nervosa: Assessment and therapeutic options. RMD Open 2019, 5, e001009. [Google Scholar] [CrossRef]
- Shi, E.; Oloff, L.M.; Todd, N.W. Stress injuries in the athlete. Clin. Podiatr. Med. Surg. 2023, 40, 181–191. [Google Scholar] [CrossRef]
- Ji, M.-X.; Yu, Q. Primary osteoporosis in postmenopausal women. Chronic Dis. Transl. Med. 2015, 1, 9–13. [Google Scholar] [CrossRef]
- Hembree, W.C.; Cohen-Kettenis, P.T.; Gooren, L.; Hannema, S.E.; Meyer, W.J.; Murad, M.H.; Rosenthal, S.M.; Safer, J.D.; Tangpricha, V.; T’Sjoen, G.G. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 3869–3903. [Google Scholar] [CrossRef]
- El Ghoch, M.; Alberti, M.; Capelli, C.; Calugi, S.; Dalle Grave, R. Resting Energy Expenditure in Anorexia Nervosa: Measured versus Estimated. J. Nutr. Metab. 2012, 2012, 652932. [Google Scholar] [CrossRef]
- Thibault, R.; Genton, L.; Pichard, C. Body composition: Why, when and for who? Clin. Nutr. 2012, 31, 435–447. [Google Scholar] [CrossRef]
- Cass, K.; Blalock, D.; Manwaring, J.; Wesselink, D.; Lundberg, C.; Mehler, P. Changes in Grip Strength, Depression, and Cognitive Functioning During Medical Stabilization for Anorexia Nervosa: Exploring the Utility of Grip Strength as a Marker of Severity. J. Rehabil. Res. Pract. 2024, 5, 14–22. [Google Scholar] [CrossRef]
- Mehler, P.S.; Winkelman, A.B.; Andersen, D.M.; Gaudiani, J.L. Nutritional Rehabilitation: Practical Guidelines for Refeeding the Anorectic Patient. J. Nutr. Metab. 2010, 2010, 625782. [Google Scholar] [CrossRef] [PubMed]
- Glorio, R.; Allevato, M.; De Pablo, A.; Abbruzzese, M.; Carmona, L.; Savarin, M.; Ibarra, M.; Busso, C.; Mordoh, A.; Llopis, C.; et al. Prevalence of cutaneous manifestations in 200 patients with eating disorders. Int. J. Dermatol. 2000, 39, 348. [Google Scholar] [CrossRef] [PubMed]
- Gaudiani, J.L.; Mehler, P.S. Rare medical manifestations of severe restricting and purging: “Zebras,” missed diagnoses, and best practices. Int. J. Eat. Disord. 2016, 49, 331–344. [Google Scholar] [CrossRef]
- Gibson, D.; Watters, A.; Mehler, P.S. The intersect of gastrointestinal symptoms and malnutrition associated with anorexia nervosa and avoidant/restrictive food intake disorder: Functional or pathophysiologic?—A systematic review. Int. J. Eat. Disord. 2021, 54, 1019–1054. [Google Scholar] [CrossRef]
- Atkinson, J.; Kavanagh, G.; McCracken, G. Pica: Recognizing the presentation in primary dental care. Dent. Update 2023, 50, 211–214. [Google Scholar] [CrossRef]
- Jousse-Joulin, S. Chapter 17—Salivary Glands. In Essential Applications of Musculoskeletal Ultrasound in Rheumatology; Wakefield, R.J., D’Agostino, M.A., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2010; pp. 199–206. [Google Scholar]
- Anderson, S.; Gopi-Firth, S. Eating disorders and the role of the dental team. Br. Dent. J. 2023, 234, 445–449. [Google Scholar] [CrossRef]
- Hetterich, L.; Mack, I.; Giel, K.E.; Zipfel, S.; Stengel, A. An update on gastrointestinal disturbances in eating disorders. Mol. Cell. Endocrinol. 2019, 497, 110318. [Google Scholar] [CrossRef]
- Mathenge, N.; Osiro, S.; Rodriguez, I.I.; Salib, C.; Tubbs, R.S.; Loukas, M. Superior mesenteric artery syndrome and its associated gastrointestinal implications. Clin. Anat. 2014, 27, 1244–1252. [Google Scholar] [CrossRef]
- QualtricsXM. Survey Basic Overview. Available online: https://www.qualtrics.com/support/survey-platform/survey-module/survey-module-overview/ (accessed on 10 June 2024).
- QualtricsXM. What Is a Likert Scale. Available online: https://www.qualtrics.com/experience-management/research/likert-scale/ (accessed on 8 July 2024).
- International Association of Eating Disorders Professionals Foundation. About the International Association of Eating Disorders Professionals Foundation. Available online: https://iaedpfoundation.com/about-us/ (accessed on 10 June 2024).
- Trevelyan, E.G.; Robinson, P.N. Delphi methodology in health research: How to do it? Eur. J. Integr. Med. 2015, 7, 423–428. [Google Scholar] [CrossRef]
- Jünger, S.; Payne, S.A.; Brine, J.; Radbruch, L.; Brearley, S.G. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliat. Med. 2017, 31, 684–706. [Google Scholar] [CrossRef] [PubMed]
- Spranger, J.; Homberg, A.; Sonnberger, M.; Niederberger, M. Reporting guidelines for Delphi techniques in health sciences: A methodological review. Z. Evidenz Fortbild. Qual. Gesundheitswesen 2022, 172, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Patricia, S.; Nathan, E.; Juan Sebastian, R.; Paula, M.; Randall, R.L.; Robert, T.; Roberto, V.; Mohit, B.; Michelle, G. Moving forward through consensus: Protocol for a modified Delphi approach to determine the top research priorities in the field of orthopaedic oncology. BMJ Open 2016, 6, e011780. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows; Version 27.0; IBM Corp.: Armonk, NY, USA, 2023. [Google Scholar]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Pike, K.; Rothpletz-Puglia, P.; Byham-Gray, L. Development of a Sports Nutrition Focused Physical Examination Tool: A Delphi Study. Ph.D. Thesis, Rutgers School of Health Professions, Newark, NJ, USA, 2022. [Google Scholar]
- Bathgate, J.R.; Pike, K.; Newkirk, M.; Rigassio Radler, D.; Byham-Gray, L.; Ziegler, J. Development of a bronchopulmonary dysplasia nutrition focused physical examination tool: A modified Delphi study. Pediatr. Pulmonol. 2024, 59, 1695–1707. [Google Scholar] [CrossRef]
- Tylka, T.L.; Annunziato, R.A.; Burgard, D.; Daníelsdóttir, S.; Shuman, E.; Davis, C.; Calogero, R.M. The weight-inclusive versus weight-normative approach to health: Evaluating the evidence for prioritizing well-being over weight loss. J. Obes. 2014, 2014, 983495. [Google Scholar] [CrossRef]
- Stankorb, S.M.; Rigassio-Radler, D.; Khan, H.; Touger-Decker, R. Nutrition Focused Physical Examination Practices of Registered Dietitians. Top. Clin. Nutr. 2010, 25, 335–344. [Google Scholar] [CrossRef]
- MacKle, T.J.; Touger-Decker, R.; Maillet, J.O.S.; Holland, B.K. Registered dietitians’ use of physical assessment parameters in professional practice. J. Am. Diet. Assoc. 2003, 103, 1632–1638. [Google Scholar] [CrossRef]
- Andersen, D.; Baird, S.; Bates, T.; Chapel, D.L.; Cline, A.D.; Ganesh, S.N.; Garner, M.; Grant, B.L.; Hamilton, K.K.; Jablonski, K.; et al. Academy of Nutrition and Dietetics: Revised 2017 Scope of Practice for the Registered Dietitian Nutritionist. J. Acad. Nutr. Diet. 2018, 118, 141–165. [Google Scholar] [CrossRef]
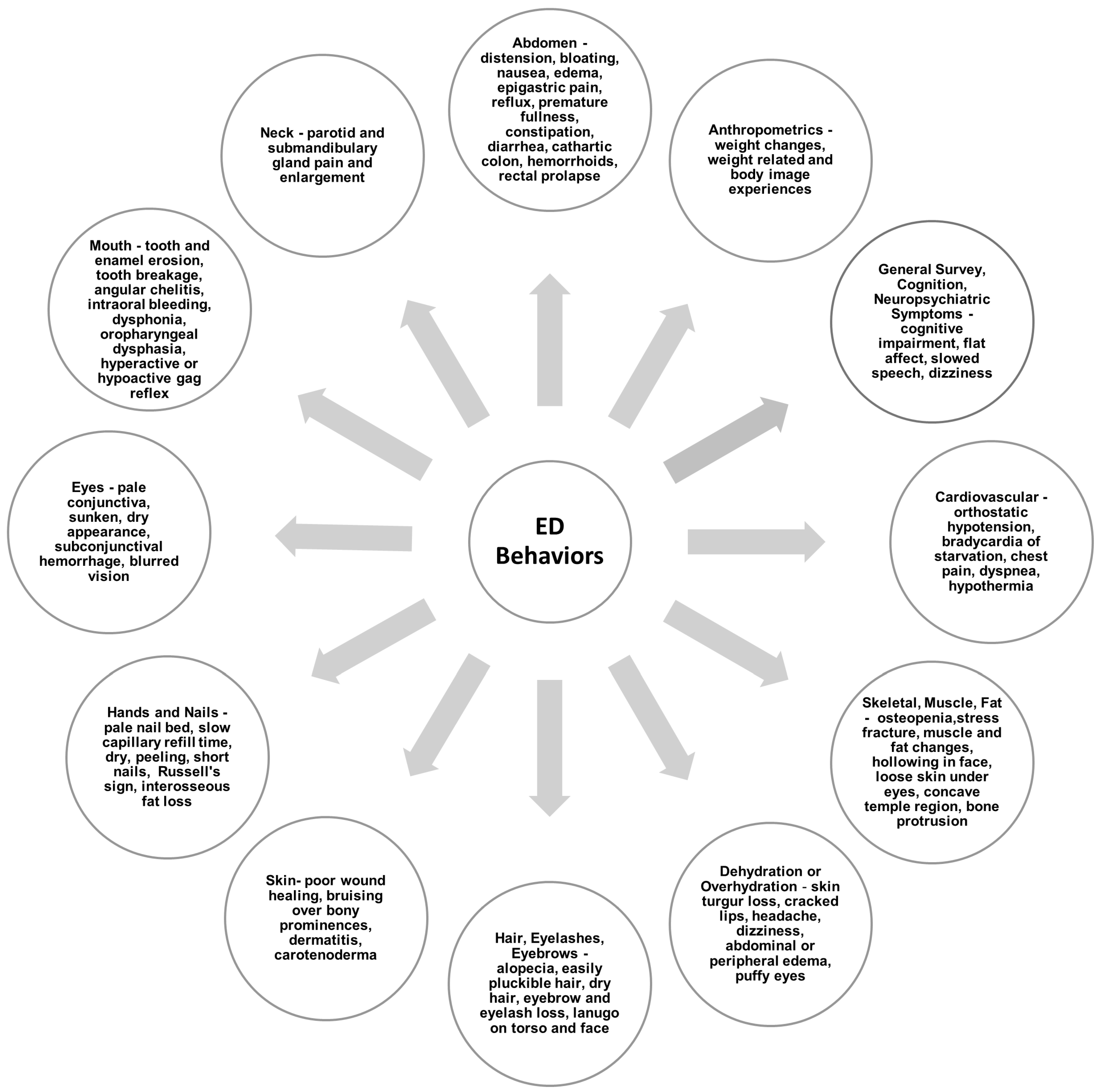
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).