Profiling Physical Activity, Diet, Screen and Sleep Habits in Portuguese Children

 , ,
, , 
Abstract
:1. Introduction
2. Experimental Section
2.1. Material and Methods
2.1.1. Anthropometry
2.1.2. Maturity Offset
2.1.3. Physical Activity and Sleep Time
2.1.4. Fruit, Vegetable and Sugary Drink Consumption
2.1.5. Screen Time
2.1.6. Socio-Demographic Characteristics
2.2. Statistical Analysis
3. Results

{kind=link}
| Variables | Total |
|---|---|
| n (%) or mean ± sd | |
| Anthropometric sample characteristics | |
| Height (cm) | 143.5 ± 6.8 |
| Weight (kg) | 40.4 ± 9.2 |
| Percent body fat (%) | 22.9 ± 7.5 |
| BMI (Kg/m−2) need to footnote this | 19.5 ± 3.4 |
| Maturity offset | −1.90 ± 0.9 |
| Gender | |
| Boys | 305 (44.5%) |
| Girls | 381 (55.5%) |
| Weight Status | |
| Normal weight | 372 (54.2%) |
| Overweight/obese | 314 (45.8%) |
| Maternal education | |
| <Grade 12 | 317 (46.2%) |
| Grade 12/diploma/technical qualification | 191 (27.8%) |
| University | 108 (15.7%) |
| Did not report | 70 (10.2%) |
| Household income | |
| <12.000 € | 270 (39.4%) |
| 12.000 €–29.999 € | 195 (28.4%) |
| ≥30.000 € | 76 (11.1%) |
| Did not report | 145 (21.1%) |
| No. of Risks | MVPA < 60 min | Fruits/Vegs All Days | Sleep < 10 h | Screen ≥ 120 min | Sugar Drinks ≥ 2 days/week | fo | fe | χ2 | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| 0 | 0 | 0 | 0 | 0 | 0 | 1 | 21.44 | 19.48 | <0.001 |
| 1 | 0 | 0 | 0 | 0 | 1 | 2 | 21.44 | 17.62 | <0.001 |
| 1 | 0 | 0 | 0 | 1 | 0 | 2 | 21.44 | 17.62 | <0.001 |
| 1 | 0 | 0 | 1 | 0 | 0 | 19 | 21.44 | 0.28 | 0.598 |
| 1 | 0 | 1 | 0 | 0 | 0 | 1 | 21.44 | 19.48 | <0.001 |
| 1 | 1 | 0 | 0 | 0 | 0 | 2 | 21.44 | 17.62 | <0.001 |
| 2 | 0 | 0 | 0 | 1 | 1 | 2 | 21.44 | 17.62 | <0.001 |
| 2 | 0 | 0 | 1 | 0 | 1 | 11 | 21.44 | 5.08 | 0.024 |
| 2 | 0 | 0 | 1 | 1 | 0 | 18 | 21.44 | 0.55 | 0.457 |
| 2 | 0 | 1 | 0 | 0 | 1 | 3 | 21.44 | 15.86 | <0.001 |
| 2 | 0 | 1 | 0 | 1 | 0 | 3 | 21.44 | 15.86 | <0.001 |
| 2 | 0 | 1 | 1 | 0 | 0 | 38 | 21.44 | 12.80 | <0.001 |
| 2 | 1 | 0 | 0 | 0 | 1 | 0 | 21.44 | 21.48 | <0.001 |
| 2 | 1 | 0 | 0 | 1 | 0 | 3 | 21.44 | 15.86 | <0.001 |
| 2 | 1 | 0 | 1 | 0 | 0 | 43 | 21.44 | 21.69 | <0.001 |
| 2 | 1 | 1 | 0 | 0 | 0 | 5 | 21.44 | 12.60 | <0.001 |
| 3 | 0 | 0 | 1 | 1 | 1 | 14 | 21.44 | 2.58 | 0.108 |
| 3 | 0 | 1 | 0 | 1 | 1 | 3 | 21.44 | 15.86 | <0.001 |
| 3 | 0 | 1 | 1 | 0 | 1 | 25 | 21.44 | 0.59 | 0.442 |
| 3 | 0 | 1 | 1 | 1 | 0 | 52 | 21.44 | 43.57 | <0.001 |
| 3 | 1 | 0 | 0 | 1 | 1 | 3 | 21.44 | 15.86 | <0.001 |
| 3 | 1 | 0 | 1 | 0 | 1 | 4 | 21.44 | 14.18 | <0.001 |
| 3 | 1 | 0 | 1 | 1 | 0 | 56 | 21.44 | 55.72 | <0.001 |
| 3 | 1 | 1 | 0 | 0 | 1 | 1 | 21.44 | 19.49 | <0.001 |
| 3 | 1 | 1 | 0 | 1 | 0 | 9 | 21.44 | 7.22 | 0.007 |
| 3 | 1 | 1 | 1 | 0 | 0 | 72 | 21.44 | 119.26 | <0.001 |
| 4 | 0 | 1 | 1 | 1 | 1 | 56 | 21.44 | 55.72 | <0.001 |
| 4 | 1 | 0 | 1 | 1 | 1 | 17 | 21.44 | 0.92 | 0.338 |
| 4 | 1 | 1 | 0 | 1 | 1 | 10 | 21.44 | 6.10 | 0.014 |
| 4 | 1 | 1 | 1 | 0 | 1 | 24 | 21.44 | 0.31 | 0.580 |
| 4 | 1 | 1 | 1 | 1 | 0 | 120 | 21.44 | 453.16 | <0.001 |
| 5 | 1 | 1 | 1 | 1 | 1 | 67 | 21.44 | 96.84 | <0.001 |
| Fit measures | Number of Classes | ||
|---|---|---|---|
| 2 | 3 | 4 | |
| Pearson χ2 | 18.208 | 8.997 | 4.064 |
| LR χ2 | 18.839 | 9.740 | 4.270 |
| # of parameters | 11 | 17 | 23 |
| AIC | 3851.165 | 3854.065 | 3860.596 |
| BIC | 3901.004 | 3931.090 | 3964.806 |
| LMR LRT | 42.152 | 8.873 | 5.333 |
| 1 class vs. 2 classes | 2 classes vs. 3 classes | 3 classes vs. 4 classes | |
| BLRT probability | <0.001 | 0.280 | 0.614 |

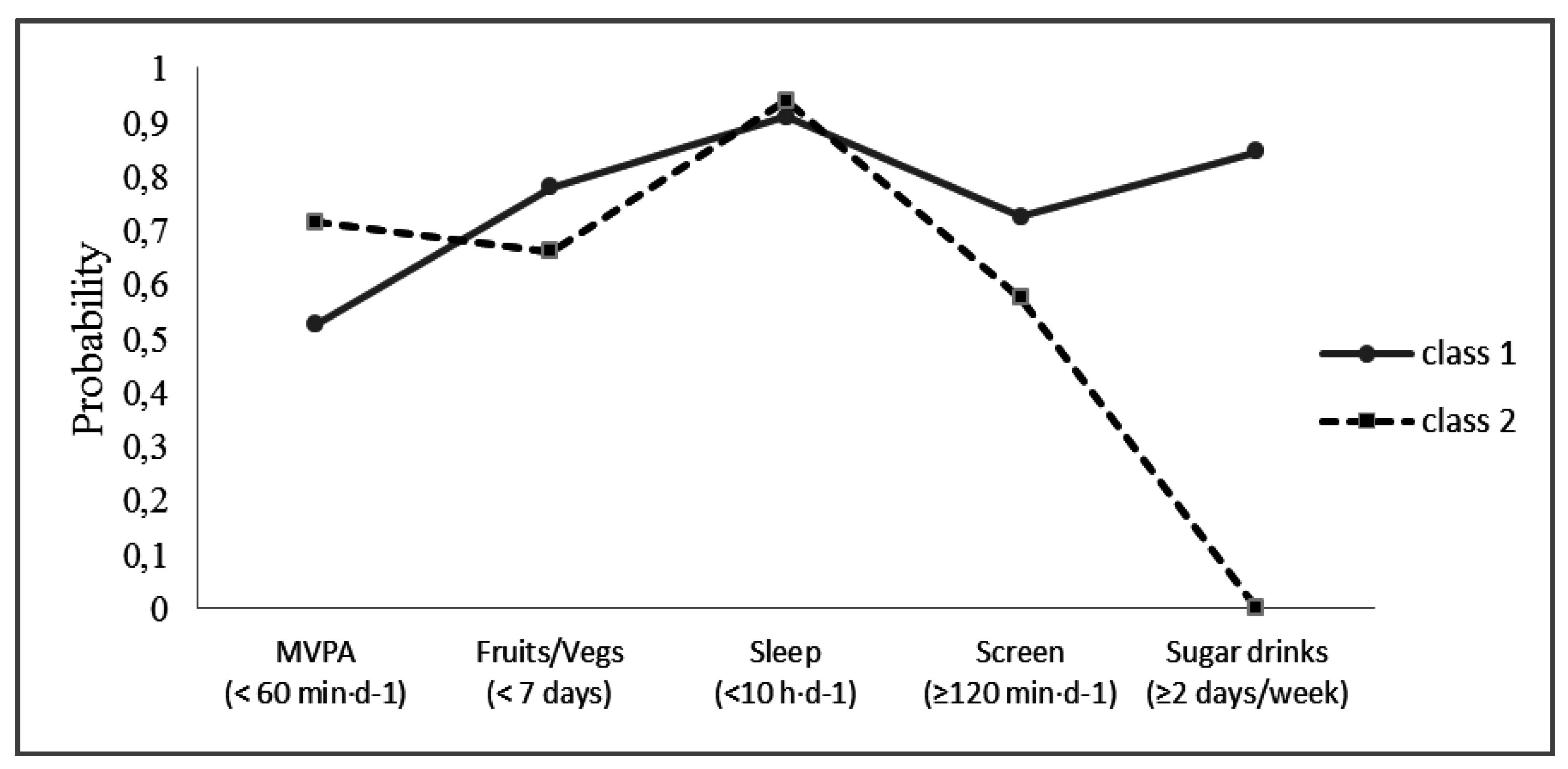
| Class 1 ( n = 242) Sedentary, Poorer Diet Quality | Class 2 ( n = 444) Insufficiently Active, Better Diet Quality | p-Value | ||
|---|---|---|---|---|
| n (%) | n (%) | |||
| MVPA | <0.001 | |||
| ≥60 min·day−1 | 116 (47.9%) | 134 (30.2%) | ||
| <60 min·day−1 | 126 (52.1%) | 310 (69.8%) | ||
| Fruits/Vegetables | 0.004 | |||
| All days | 53 (21.9%) | 144 (32.4%) | ||
| <7 days | 189 (78.1%) | 300 (67.6%) | ||
| Sleep time | 0.051 | |||
| ≥10 h·day−1 | 24 (9.9%) | 26 (5.9%) | ||
| <10 h·day−1 | 218 (90.1%) | 418 (94.1%) | ||
| Screen time | 0.002 | |||
| <120 min·day−1 | 70 (28.9%) | 181 (40.8%) | ||
| ≥120 min·day−1 | 172 (71.1%) | 263 (59.2%) | ||
| Sugary drinks | <0.001 | |||
| <2 days/week | 0 (0.0%) | 444 (100.0%) | ||
| ≥2 days/week | 242 (100.0%) | 0 (0.0%) | ||
| Gender | 0.005 | |||
| Girls | 117 (48.4%) | 264 (59.5%) | ||
| Boys | 125 (51.7%) | 180 (40.5%) | ||
| Weight status | 0.059 | |||
| Normal Weight | 143 (59.1%) | 229 (51.6%) | ||
| Overweight/obese | 99 (40.91%) | 215 (48.4%) | ||
| Maternal education | <0.001 | |||
| <Grade 12 | 120 (49.6%) | 197 (44.4%) | ||
| Grade 12/diploma/technical qualification | 79 (32.6%) | 112 (25.2%) | ||
| University | 20 (8.7%) | 88 (19.8%) | ||
| Did not report | 23 (9.5%) | 47 (10.6%) | ||
| Household income | 0.106 | |||
| <12.000 € | 94 (38.8%) | 176 (39.6%) | ||
| 12.000 €–29.999 € | 77 (31.8%) | 118 (26.6%) | ||
| ≥30.000 € | 18 (7.4%) | 58 (13.1%) | ||
| Did not report | 53 (21.9%) | 92 (20.7%) | ||
| Maturity offset | Mean ± SD | Mean ± SD | 0.292 | |
| −2.02 ± 0.95 | −1.83 ± 0.85 | |||
| Variables | Coefficients(SE) | Odds Ratio | 95%CI | p-Value |
|---|---|---|---|---|
| Sex (Male) | 1.12(0.22) | 3.06 | 1.98–4.72 | <0.001 |
| Maternal Education | ||||
| <12 Grade | Reference | |||
| Grade12/diploma/technical | 0.14(0.26) | 1.15 | 0.70–1.90 | 0.550 |
| University | 0.49(0.35) | 1.632 | 0.83–3.21 | 0.156 |
| Household income | ||||
| <12.000€ | Reference | |||
| 12.000 €–29.999 € | −0.25(0.26) | 0.78 | 0.47–1.30 | 0.339 |
| ≥30.000 € | −0.50(0.32) | 0.61 | 0.32–1.14 | 0.123 |
| Maturity offset | 1.91(0.22) | 6.75 | 4.38–10.41 | <0.001 |
| Latent Classes (iahdq) | −0.51(0.170) | 0.60 | 0.43–0.84 | <0.001 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Carson, V.; Stone, M.; Faulkner, G. Patterns of Sedentary Behavior and Weight Status among Children. Pediatr. Exerc. Sci. 2014, 26, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Kell, K.P.; Cardel, M.I.; Bohan Brown, M.M.; Fernández, J.R. Added sugars in the diet are positively associated with diastolic blood pressure and triglycerides in children. Am. J. Clin. Nutr. 2014, 100, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Beydoun, M.A.; Wang, Y. Is sleep duration associated with childhood obesity? A systematic review and meta-analysis. Obesity 2008, 16, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Knutson, K.L. Sleep duration and cardiometabolic risk: A review of the epidemiologic evidence. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Xi, B.; He, D.; Zhang, M.; Xue, J.; Zhou, D. Clinical review: Short sleep duration predicts risk of metabolic syndrome: A systematic review and meta-analysis. Sleep Med. Rev. 2014, 18, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Stamatakis, E.; Coombs, N.; Jago, R.; Gama, A.; Mourão, I.; Nogueira, H.; Rosado, V.; Padez, C. Associations between indicators of screen time and adiposity indices in Portuguese children. Prev. Med. 2013, 56, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Valente, H.; Teixeira, V.; Padrão, P.; Bessa, M.; Cordeiro, T.; Moreira, A.; Mitchell, V.; Lopes, C.; Mota, J.; Moreira, P. Sugar-sweetened beverage intake and overweight in children from a Medierranean country. Public Health Nutr. 2011, 14, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Gomes, T.N.; Katzmarzyk, P.T.; dos Santos, F.K.; Souza, M.; Pereira, S.; Maia, J.A. Overweight and obesity in Portuguese children: Prevalence and correlates. Int. J. Environ. Res. Public Health 2014, 11, 398–417. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Alvira, J.M.; de Bourdeaudhuij, I.; Singh, A.S.; Vik, F.N.; Manios, Y.; Kovacs, E.; Jan, N.; Brug, J.; Moreno, L.A. Clustering of energy balance-related behaviors and parental education in European children: The ENERGY-project. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 5–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jago, R.; Fox, K.R.; Page, A.S.; Brockman, R.; Thompson, J.L. Physical activity and sedentary behaviour typologies of 10–11 year olds. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Magee, C.A.; Caputi, P.; Iverson, D.C. Patterns of health behaviours predict obesity in Australian children. J. Paediatr. Child. Health 2013, 49, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. The International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE): Design and methods. BMC Public Health 2013, 13, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry: Report of a WHO Expert Committee; WHO: Geneva, Switzerland, 1995. [Google Scholar]
- Mirwald, R.L.; Baxter-Jones, A.D.G.; Bailey, D.A.; Beunen, G.P. An assessment of maturity from anthropometric measurements. Med. Sci. Sports Exerc. 2002, 34, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Tudor-Locke, C.; Barreira, T.V.; Schuna, J.M., Jr.; Mire, E.F.; Katzmarzyk, P.T. Fully automated waist-worn accelerometer algorithm for detecting children’s sleep-period time separate from 24-h physical activity or sedentary behaviors. Appl. Physiol. Nutr. Metab. 2014, 39, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Barreira, T.V.; Schuna, J.M., Jr.; Mire, E.F.; Katzmarzyk, P.T.; Chaput, J.P.; Leduc, G.; Tudor-Locke, C. Identifying children’s nocturnal sleep using 24-h waist accelerometry. Med. Sci. Sports Exerc. 2015, 47, 937–943. [Google Scholar] [CrossRef] [PubMed]
- National Sleep Foundation. Children and Sleep. Available online: http://sleepfoundation.org/sleep-topics/children-and-sleep/page/0%2C2/Suggest (accessed on 20 March 2015).
- Currie, C.; Gabhainn, S.N.; Godeau, E.; Roberts, C.; Smith, R.; Currie, D.; Pickett, W.; Richter, M.; Morgan, A.; Barnekow, V. Inequalities in Young People’s Health: HBSC International Report from the 2005/06 Survey. Health Policy for Children and Adolescents, No. 5; WHO Regional Office for Europe: Copenhagen, Denmark, 2008. [Google Scholar]
- Barlow, S.E. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120 (Suppl. 4), S164–S192. [Google Scholar] [CrossRef] [PubMed]
- Schrepp, M. The use of configural frequency analysis for explorative data analysis. Br. J. Math. Stat. Psychol. 2006, 59, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Geiser, C. Data Analysis with Mplus; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Wang, J.; Wang, X. Structural Equation Modelling: Applications Using Mplus; Wiley/Higher Education Press: Chichester, UK, 2012. [Google Scholar]
- Sanchez, A.; Norman, G.J.; Sallis, J.F.; Calfas, K.J.; Cella, J.; Patrick, K. Patterns and correlates of physical activity and nutrition behaviors in adolescents. Am. J. Prev. Med. 2007, 32, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Grunseit, A.; Khambalia, A.; Bell, C.; Wolfenden, L.; Milat, A.J. Co-occurrence of obesogenic risk factors among adolescents. J. Adolesc. Health 2012, 51, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.W.; Ortiz, C.L.; Lathan, D.; Moore, L.A.; Konzelmann, K.L.; Adolph, A.L.; Simth, E.O.; Butte, N.F. Sleep duration of underserved minority children in a cross-sectional study. BMC Public Health 2013, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Galland, B.C.; Taylor, B.J.; Elder, D.E.; Herbison, P. Clinical Review: Normal sleep patterns in infants and children: A systematic review of observational studies. Sleep Med. Rev. 2012, 16, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Sabbe, D.; de Bourdeaudhuij, I.; Legiest, E.; Maes, L. A cluster-analytical approach towards physical activity and eating habits among 10-year-old children. Health Educ. Res. 2008, 23, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Ottevaere, C.; Huybrechts, I.; Benser, J.; de Bourdeaudhuij, I.; Cuenca-Garcia, M.; Dallongeville, J.; Zaccaria, M.; Gottrand, F.; Kersting, M.; Rey-López, J.P.; et al. Clustering patterns of physical activity, sedentary and dietary behavior among European adolescents: The HELENA study. BMC Public Health 2011, 11 (Suppl. S4), 328–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huh, J.; Riggs, N.R.; Spruijt-Metz, D.; Chou, C.; Huang, Z.; Pentz, M. Identifying Patterns of Eating and Physical Activity in Clildren: A Latent Class Analysis of Obesity Risk. Obesity 2011, 19, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Biddle, S.J.H. Sedentary Behavior and Dietary Intake in Children, Adolescents, and Adults: A Systematic Review. Am. J. Prev. Med. 2011, 41, 178–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, D.; Maia, J.; Seabra, A.; Garganta, R.; Lopes, V.; Katzmarzyk, P.; Beunen, G. Correlates of changes in BMI of children from the Azores islands. Int. J. Obes. (Lond.) 2010, 34, 1487–1493. [Google Scholar] [CrossRef] [PubMed]
- Kanaan, M.N.; Afifi, R.A. Gender differences in determinants of weight-control behaviours among adolescents in Beirut. Public Health Nutr. 2010, 13, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Harter, S. The Self. In Handbook of Child Psychology; Damon, W., Lerner, R.M., Eds.; John Wiley & Sons: New York, NJ, USA, 2006; Volume 3, pp. 505–570. [Google Scholar]
- Jago, R.; Thompson, J.L.; Sebire, S.J.; Wood, L.; Pool, L.; Zahra, J.; Lawlor, D.A. Cross-sectional associations between the screen-time of parents and young children: Differences by parent and child gender and day of the week. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Coelho-E-Silva, M.J.; Vaz, E.R.; Cyrino, E.S.; Fernandes, R.A.; Valente-Dos-Santos, J.; Machado-Rodrigues, A.; Malina, R.M. Nutritional status, biological maturation and cardiorespiratory fitness in Azorean youth aged 11–15 years. BMC Public Health 2013, 13, 495. [Google Scholar] [CrossRef] [PubMed]
- Adair, L.S.; Gordon-Larsen, P. Maturational timing and overweight prevalence in US adolescent girls. Am. J. Public Health 2001, 91, 642–644. [Google Scholar] [PubMed]
- Beunen, G.P.; Malina, R.M.; Lefevre, J.A.; Claessens, A.L.; Renson, R.; Vanreusel, B. Adiposity and biological maturity in girls 6–16 years of age. Int. J. Obes. Relat. Metab. Disord. 1994, 18, 542–546. [Google Scholar] [PubMed]
- Santos, J.R.; Duarte, J.P.; Mota, J. Association between overweight and early sexual maturation in Portuguese boys and girls. Ann. Hum. Biol. 2006, 33, 55–63. [Google Scholar]
- Utter, J.; Scragg, R.; Schaaf, D.; Fitzgerald, E.; Wilson, N. Correlates of body mass index among a nationally representative sample of New Zealand children. Int. J. Pediatr. Obes. 2007, 2, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Gomes, T.N.; dos Santos, F.K.; Santos, D.; Chaves, R.N.; Souza, M.; Katzmarzyk, P.T.; Maia, J. “Fat-But-Active”: Does Physical Activity Play a Significant Role in Metabolic Syndrome Risk among Children of Different BMI Categories? J. Diabetes Metab. 2014, 5, 421. [Google Scholar] [CrossRef]
- Steele, R.M.; van Sluijs, E.M.F.; Sharp, S.J.; Landsbaugh, J.R.; Ekelund, U.; Griffin, S.J. An investigation of patterns of children’s sedentary and vigorous physical activity throughout the week. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Atkin, A.J.; Corder, K.; Ekelund, U.; Wijndaele, K.; Griffin, S.J.; van Sluijs, E.M. Determinants of change in children’s sedentary time. PLoS ONE 2013, 8, e67627. [Google Scholar] [CrossRef] [PubMed]
- Elsenburg, L.K.; Corpeleijn, E.; van Sluijs, E.M.F.; Atkin, A.J. Clustering and Correlates of Multiple Health Behaviours in 9–10 Year Old Children. PLoS ONE 2014, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vasques, C.; Mota, M.; Correia, T.; Lopes, V. Prevalence of overweight/obesity and its association with sedentary behavior in children. Rev. Port. Cardiol. 2012, 31, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Sardinha, L.B.; Santos, R.; Vale, S.; Silva, A.M.; Ferreira, J.P.; Raimundo, A.M.; Moreira, H.; Baptista, F.; Mota, J. Prevalence of overweight and obesity among Portuguese youth: A study in a representative sample of 10–18-year-old children and adolescents. Int. J. Pediatr. Obes. 2011, 6, e124–e128. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Katzmarzyk, P.T.; Boyce, W.F.; Vereecken, C.; Mulvihill, C.; Roberts, C.; Currie, C.; Pickett, W. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes. Rev. 2005, 6, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, M.; Sassi, F.; Lauer, J.A.; Lee, Y.Y.; Guajardo-Barron, V.; Chisholm, D. Tackling of unhealthy diets, physical inactivity, and obesity: Health effects and cost-effectiveness. Lancet 2010, 376, 1775–1784. [Google Scholar] [CrossRef]
- Vereecken, C.A.; Maes, L. A Belgian study on the reliability and relative validity of the Health Behaviour in School-Aged Children food-frequency questionnaire. Public Health Nutr. 2003, 6, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, K.H.; Harnack, L.; Fulton, J.E.; Jacobs, D.R., Jr.; Gao, S.; Lytle, L.A. Reliability and validity of a brief questionnaire to assess television viewing and computer use by middle school children. J. School Health 2004, 74, 370–377. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, S.; Katzmarzyk, P.T.; Gomes, T.N.; Borges, A.; Santos, D.; Souza, M.; Santos, F.K.d.; Chaves, R.N.; Champagne, C.M.; Barreira, T.V.; et al. Profiling Physical Activity, Diet, Screen and Sleep Habits in Portuguese Children. Nutrients 2015, 7, 4345-4362. https://doi.org/10.3390/nu7064345
Pereira S, Katzmarzyk PT, Gomes TN, Borges A, Santos D, Souza M, Santos FKd, Chaves RN, Champagne CM, Barreira TV, et al. Profiling Physical Activity, Diet, Screen and Sleep Habits in Portuguese Children. Nutrients. 2015; 7(6):4345-4362. https://doi.org/10.3390/nu7064345
Chicago/Turabian StylePereira, Sara, Peter T. Katzmarzyk, Thayse Natacha Gomes, Alessandra Borges, Daniel Santos, Michele Souza, Fernanda K. dos Santos, Raquel N. Chaves, Catherine M. Champagne, Tiago V. Barreira, and et al. 2015. "Profiling Physical Activity, Diet, Screen and Sleep Habits in Portuguese Children" Nutrients 7, no. 6: 4345-4362. https://doi.org/10.3390/nu7064345
APA StylePereira, S., Katzmarzyk, P. T., Gomes, T. N., Borges, A., Santos, D., Souza, M., Santos, F. K. d., Chaves, R. N., Champagne, C. M., Barreira, T. V., & Maia, J. A. R. (2015). Profiling Physical Activity, Diet, Screen and Sleep Habits in Portuguese Children. Nutrients, 7(6), 4345-4362. https://doi.org/10.3390/nu7064345