1. Introduction
Family members share similar eating habits that are affected by individual factors and the family food environment [
1]. Parental role modeling and perception of adequacy of their child’s diet are important predictors for the child’s current dietary behavior [
2] and watching the parents eat raises the children’s awareness of their parents’ eating behaviors [
3,
4]. Despite the fact that fathers and mothers were found to influence the child’s eating behavior [
5,
6], the influence differs for mothers compared to fathers [
7,
8]. Paternal dietary influence was identified for fruit but also for fat-and energy-dense, nutrient-poor foods [
9,
10], whereas positive child–mother correlations have been reported for fruit and vegetable intake [
11] and soft drinks [
12]. Thus, parents build their children’s food environment by making healthy foods [
13] or unhealthy foods [
14] available. Accordingly the children’s food consumption was associated with healthy foods (so-called core foods, e.g., cereals, dairy, fruit, and vegetables) or with unhealthy non-core foods (e.g., snack foods, fats, and oils) [
5]. As an example, adolescents were more likely to consume fruit and vegetables when parents made those foods available [
15,
16]. It has been observed that the person who prepares the majority of family meals largely influences the consumption of fruit and vegetables but also high-fat foods; this association increases with increasing numbers of shared meals [
17].
Previous research has demonstrated that the association between parental and child intake increased with an increasing number of family meals at home [
18] and that the number of family meals was positively associated with the consumption of healthier foods [
19]. Family mealtimes provide structure and a regular opportunity for developing emotional connections among family members and therefore help children to monitor their mood and learn healthy dietary behaviors [
20]. Accordingly, higher family meal frequency was found to be associated with significantly fewer weekly servings of sweets and sugar-sweetened beverages [
21]; however, the consumption of those non-core foods (e.g., sugar sweetened beverages) was found to be higher when their home availability was higher [
5]. Consumption of sugar-sweetened beverages is one epidemiological key health indicator of the European Core Health Indicators [
22] and is frequently used in public health monitoring, especially when addressing socioeconomic determinants of eating behavior in European children and adolescents [
23,
24]. Investigations in low-income parent–child dyads found that soft drink availability at home was a strong influencing factor for the children’s soft drink intake [
25], identifying parents as gatekeepers for the family food environment.
Apart from this literature, it is striking that there is little knowledge about the resemblance of entire dietary patterns among children and their parents across Europe, which was described in the present study. The previous literature mainly investigated parental influence on the children’s intake of particular food groups such as fruit and vegetables or sugar-sweetened beverages. We therefore aimed at adding knowledge on the influence of the entire parental DP on the children’s DP. Besides parental intake, home availability has also been found to predict children’s intake of core-food and non-core foods. Thus, we aimed at determining whether the family food environment (operationalized as the number of shared meals and availability of soft drinks during meals) moderated the association between children’s DP and parental DP. Understanding to what extent the family food environment, along with the parental DP, influences children’s eating behavior has important public health implications, because in this age children and adolescents mostly still live with their parents and potentially eat up to three meals a day at home. Development of intervention strategies to improve children’s dietary patterns is likely to be more successful if supported by an understanding not only healthy but also unhealthy food intake.
2. Materials and Methods
2.1. Study Participants
Data from this investigation were obtained from the I.Family cohort. In 2013/2014 the I.Family study cross-sectionally examined children and parents from Sweden, Germany, Hungary, Italy, Cyprus, Spain, Belgium, and Estonia in order to investigate associations between eating habits and lifestyle factors leading to overweight and obesity [
26]. For this investigation children and adolescents from six years to approximately 16 years who lived with their families were invited to the examination, together with the person having the care and custody of the child (hereinafter named parents). In the present analysis we included children and parents providing at least one 24HDR (
N = 4816). In the final mixed effects logistic regression model, we included 1662 child–mother dyads (with 1269 mothers) and 789 child–father dyads (with 566 fathers); of those, 516 families provided information from siblings and 362 families provided information from the mother and father. Information on the availability of soft drinks during meals was provided for 1607 child–mother dyads and 763 child–father dyads.
Parents and children older than 16 years provided written informed consent. Younger children gave oral consent for examinations and sample collection. Study subjects and their parents could consent to single components of the study while abstaining from others. Study participants did not undergo any procedures unless they (and their parents) had given consent for examinations, collection of samples, subsequent analysis, and storage of personal data and collected samples. All applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during this research. Each participating center obtained ethical approval from the local responsible authorities in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
2.2. Questionnaires and Anthropometric Measurements
Questionnaires were developed in English, translated into local languages, and then back-translated to check for translation errors. Parents reported the age and sex of their children and themselves in addition to their highest educational level according to the International Standard Classification of Education (ISCED) [
27], which was used as a proxy indicator for the socioeconomic status (SES) of the family. Additionally, parents reported if soft drinks are available at home during meals (answer options: Yes, often or always; No or rarely).
The field methods comprised anthropometric measurements of standing height (cm) using a Seca 225 stadiometer (Seca GmbH & KG, Birmingham, UK) in accordance with international standards for anthropometric assessment and weight (kg) [
28]. Body weight was assessed in fasting status using a prototype of the TANITA BC 420 SMA digital scale for children and a TANITA BC 418 MA for adolescents and adults (TANITA Europe GmbH, Sindelfingen, Germany). All measurements were performed in light clothing (e.g., underwear) [
29].
The BMI of the participants was calculated by dividing body weight in kilograms by squared body height in meters. The BMI of children was transformed to an age- and sex-specific
z-score according to Cole et al. [
30]. Weight groups (thin/normal and overweight/obese) of children were categorized using age- and sex-specific cutoff values based on the extended IOTF criteria [
31]. Weight groups of adolescents and parents above 18 years were calculated using WHO cutoffs [
32]. Even though weight status was not a focus of this investigation, it was calculated for a better characterization of the study population.
2.3. Dietary Information
Dietary intake of the previous 24 h was assessed using an online 24-h dietary recall (24HDR) assessment program, called ‘Self-Administered Children, Adolescents and Adult Nutrition Assessment’ (SACANA), based on the validated SACINA offline version [
33]. The instrument has been validated and results supported the validity of SACANA as a self-reporting instrument for assessing intakes in children (publications in progress).
Children and parents were asked to recall their diet and to enter the type and amount (g) of all drinks and foods consumed during the previous day, starting with the first intake after waking up in the morning. Children under 11 years were advised to ask their parents for help [
34]. Study participants above 11 years of age could ask for assistance from a dietician or trained study nurse during the survey examinations, but the majority of participants had no questions since they already participated in the IDEFICS study and were therefore familiar with the recall procedures and software structure used. Standardized photographs were used to assist with accurate estimation of portion size [
35]. In the present study, participants were asked to complete at least three 24HDR during the upcoming four weeks. However, the availability of repeated 24HDR varied among individuals from one to four recalls. For 43% of parents (39% of children), three repeated 24HDR were available.
The total number of main meals (breakfast, lunch, and dinner) per participant was calculated. Breakfast was defined as “shared” if the total number of shared breakfasts (parent with child) divided by the number of all reported breakfasts of the respective parent was at least 0.5. Shared lunches and dinners were categorized accordingly. The sum of all shared main meals per parent was calculated and the following categories were derived: (1) <1 shared meal per day and (2) ≥1 shared meal per day.
2.4. Dietary Data Analysis
Missing or implausible values for intake of single food items that could not be corrected were imputed by country, food group, and age-specific median intakes (0.15% of the entries). Incomplete 24HDR (recalls that have not been completed throughout) and those with more than four imputed values were excluded from the analysis.
Age- and sex-specific Goldberg cutoffs were applied to classify each recall day as under-reported, plausibly reported, and over-reported energy intake, as described elsewhere [
36].
In total, we excluded 955 participants classified as misreporters from the analysis: 484 children and 471 adults; among those 95% and 99% were under-reporters, and 5% and 1% were over-reporters, respectively.
Each food recorded by SACANA was assigned to one of 15 dietary categories: healthy and unhealthy cereals and cereal products, unhealthy sugar and sugar products, healthy and unhealthy fat and fat savory sauces, healthy fruit and vegetables, healthy and unhealthy meat and meat products, healthy meat alternatives, healthy and unhealthy milk and dairy products, healthy and unhealthy non-alcoholic beverages, healthy and unhealthy mixed dishes (
Table 1). Foods were categorized as “healthy” when they contained less energy, less sugar, less (unhealthy) fat, or more fiber than the unhealthy food alternative, e.g., table water (healthy beverage) vs. juice (unhealthy beverage), plain yogurt (healthy) vs. full fat and sweetened yogurt (unhealthy). Consumption of unhealthy mixed dishes was so rare that this category was not included in further analysis.
After food categorization, individual usual daily energy intake (EI, kcal/day) and individual usual intakes of dietary categories (kcal/day, healthy non-alcoholic beverages: g/day) were estimated based on the U.S. National Cancer Institute Method [
37,
38]. This method allows the inclusion of covariates like age and additional food frequency information, accounts for different intake on weekend vs. work days, and corrects for the variance inflation caused by the daily variation in diet. Usual intakes were estimated for children as well as for their parents, stratified by sex (all participants with at least one plausible 24HDR). Age was considered as a covariate in all models. When estimating usual food intakes, the corresponding food consumption frequency obtained from the I.Family food frequency questionnaire was also used as a covariate to improve estimates (except for mixed dishes, as this food group was not queried in the food frequency questionnaire but was a generic category in SACANA food groups). The I.Family food frequency questionnaire was built on the valid and reproducible IDEFICS study food frequency questionnaire, which was described in detail previously [
39,
40,
41]. The FFQ contained 59 food items comparable to those in the SACANA web tool, thus allowing categorizing the food items according to the 15 dietary categories mentioned above. The answer possibilities in the FFQ were “never/less than once a week”, “1–3 times a week”, “4–6 times a week”, “1 time/day”, “2 times a day”, “3 times a day”, and “I have no idea”. All participants were asked to complete one FFQ for the four weeks prior to the survey examination.
The individual percentage of energy contribution from all dietary categories was calculated to correct for individual total EI. For children and adults separately, these percentages were transformed into
z-scores using sample means and sample standard deviations. The
z-score represents the distance between the percentage of energy contribution and the corresponding population mean in units of the standard deviation. This procedure was not applied for usual EI and usual intake of non-alcoholic beverages (g/day) since EI correction is neither reasonable for EI itself nor for the calorie-free dietary category. Therefore, age-dependent
z-scores were derived for these variables with the Generalized Additive Models for Location, Scale, and Shape (this procedure is described in detail in
Appendix A).
2.5. Statistical Analysis
K-means clustering was applied for children and parents separately to identify distinct clusters of participants with similar dietary patterns. In this procedure the previously derived
z-scores were taken into account. Details of this procedure are described in
Appendix A. As clusters were comparable between children and parents, the same cluster names were used. Three clusters representing the DP (
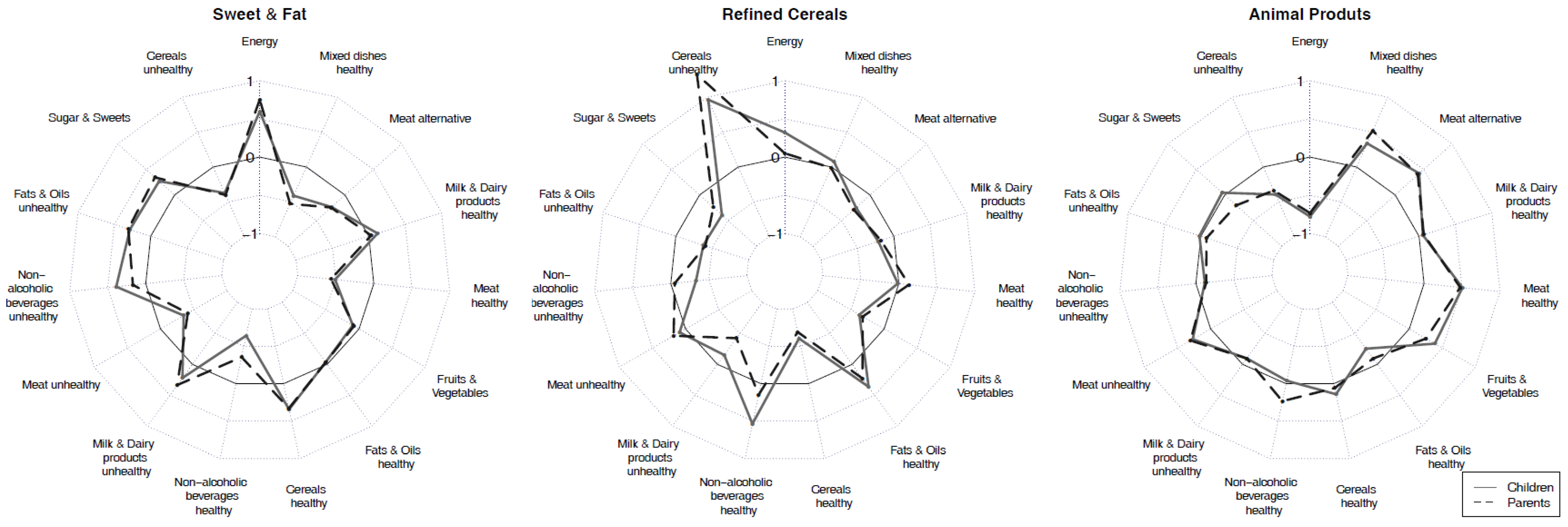
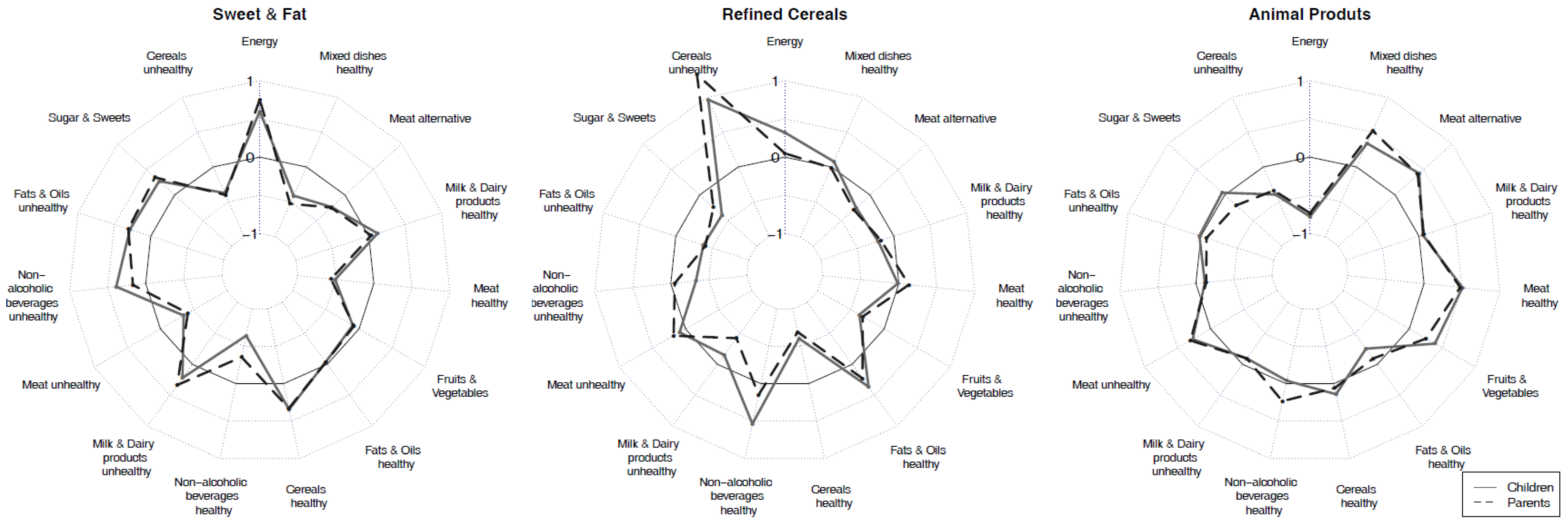
Figure 1) were obtained: Sweet and Fat cluster, Refined Cereals cluster, and Animal Products cluster. Each participant was allocated to exactly one DP and corresponding indicator variables were derived (participant is in the respective cluster versus participant is not in the respective cluster).
Family food environment was operationalized using the number of shared meals (<1 or ≥1 shared meal per day) as an indicator of parental role modeling and the availability of soft drinks during meals as an indicator of home food availability. As a first step, we investigated associations between the outcome children’s DP (indicator variable) and the exposure parental DP (indicator variable) and the number of shared meals using mixed effects logistic regression. To examine whether the number of shared meals strengthened the associations between parental and children’s DP, an interaction term was included (number of shared meal × parental DP). For each of the three DP, we conducted a regression analysis separately for fathers and mothers (six models). Accordingly, we investigated in a second step the associations between children’s DP and the exposure parental DP and availability of soft drinks during meals. To examine whether the availability of soft drinks during meals strengthened the associations between parental DP and children’s DP, an interaction term (availability of soft drinks during meals × parental DP) was included. The models were adjusted for sex, age and BMI z-score of the children, ISCED, country, and BMI of the respective parent. In order to account for dependencies between siblings, a random effect was added for family membership. Based on the mixed effects logistic regression models, odds ratios (OR) and confidence intervals (95%CI) were calculated for a child being allocated to the DP corresponding to the parental DP depending on the number of shared meals and availability of soft drinks during meals. The analysis was performed using the procedure PROC GLIMMIX of the statistical software SAS (version 9.3; SAS Institute, Cary, NC, USA).
3. Results
The aims of the present study were to investigate the resemblance of children’s DP and their parents’ DP as well as to determine whether structural conditions of the family food environment moderated the association between children’s DP and parental DP.
3.1. Dietary Clusters
Based on dietary categories (
Table 1) and usual EI, the three-cluster solutions were derived. For comparable clusters of children and parents, the following labels were assigned: Sweet and Fat (
N = 697 for children and
N = 728 for parents), Refined Cereals (
N = 563 for children and
N = 410 for parents), and Animal Products (
N = 716 for children and
N = 747 for parents).
Table 2 presents the mean
z-scores and standard deviations of usual intake for all dietary categories in the three clusters for children and parents.
In general, we observed a resemblance of children’s dietary patterns to parents’ dietary pattern; details of these analyses can be found in
Appendix A. The overall agreement between cluster allocation of children and mothers was 52% (for fathers, 53%).
In particular, we observed the following characteristics for the three clusters representing dietary patterns (DP).
Sweet and Fat: Children and adults allocated to this cluster reported higher-than-mean intake of sugar and sweets (children’s mean 0.27; parents’ mean 0.34), unhealthy fats and oils (children’s mean 0.29; parents’ mean 0.31), unhealthy (sweetened) non-alcoholic beverages (children’s mean 0.39; parents’ mean 0.17) and unhealthy milk and dairy products (children’s mean 0.22; parents’ mean 0.34) (
Figure 1). Cereals were categorized as healthy in case of low sugar content and low fat content and high fiber content (
Table 1), such as whole-grain breads, plain breakfast cereals, or crispbread (children’s mean 0.34; parents’ mean 0.33). Family members allocated to this DP reported the highest EI (children’s mean 0.60; parents’ mean 0.75).
Refined Cereals: Children and parents from this cluster reported higher-than-mean intake of unhealthy cereals (e.g., white breads, refined and/or sugared breakfast cereals, pasta from refined wheat, refined rice, sweet and/or fatty bakery products (biscuits, cakes, fritters, etc.; children’s mean 0.96; parents’ mean 1.32) and healthy fats and oils (children’s mean 0.36; parents’ mean 0.23). Both children and parents also consumed more healthy non-alcoholic beverages (children’s mean 0.54; parents’ mean 0.15).
Animal Products: Children and parents who were allocated to this cluster reported higher intake of all types of meat (children’s mean for meat unhealthy 0.27, meat healthy 0.51; parents’ mean 0.30 and 0.48, respectively) and meat alternatives (children’s mean 0.42; parents’ mean 0.40) as well as of healthy mixed dishes (children’s mean 0.34; parents’ mean 0.52). Healthy mixed dishes were mainly based on cereals, legumes, and vegetables/potatoes, with small proportions of fish, egg, or dairy. Children and parents further reported higher-than-mean intakes of fruit and vegetables (children’s mean 0.39; parents’ mean 0.25). Parents reported a higher-than-mean intake for healthy non-alcoholic beverages (mean 0.23). The energy intake of children and parents was lowest in this DP (children’s mean −0.78; parents’ mean −0.73).
3.2. Participant Characteristics
The largest proportion of children (36%) and parents (40%) was allocated to the Animal Products cluster (
Table 3). The mean age of children (11.4 years) and parents (44.2 years) was highest in the Refined Cereals cluster. Girls (39%) and mothers (44%) were mainly found in the Sweet and Fat cluster, whereas most boys and men were found in the Animal Products cluster (38% and 44%, respectively).
Most normal weight children were allocated to the Animal Products cluster (38%), whereas most overweight (39%) and obese (56%) children were allocated to the Refined Cereals cluster. Most normal weight adults (43%) were in the Sweet and Fat cluster; most overweight (41%) and obese (38%) adults were found in the Animal Products cluster.
Children and adults from low SES families mainly belonged to the Refined Cereals cluster (76% and 71%, respectively). Children from high SES families were equally allocated to the Sweet and Fat and the Animal Products clusters (both 39%).
In all countries—except Belgium—those cluster memberships with the highest proportion of children and parents were comparable. In Italy and Hungary most children and parents shared the Refined Cereals cluster; in Estonia, Sweden and Germany most shared the Sweet and Fat cluster; and in Cyprus and Spain most shared the Animal Products cluster. In Belgium 47% of children were found in the Animal Products cluster, but 55% of their parents in the Sweet and Fat cluster.
3.3. Family Food Environment
Shared meals: Resemblance was observed between parental DP and children’s DP: the chance of the child being allocated to the Sweet and Fat DP, the Refined Cereals DP, and the Animal Products DP is higher if the mother was allocated to the same DP, independently of the number of shared meals, compared to the chance if the mother was in a different DP (
Table 4). Overall, children were more likely to be allocated to the Sweet and Fat DP if the father was allocated to the same DP; the odds ratio increased with an increase in the number of shared meals from <1 to ≥1 (OR 2.30; 95% CI 1.15; 4.57 or OR 3.18; 95% CI 1.84; 5.47, respectively).
Soft drink availability during meals: The child was more likely to be allocated to the Sweet and Fat DP if soft drinks were available during meals, even if the mother was not allocated to the Sweet and Fat DP (OR 1.97; 95% CI 1.20; 3.25,
Table 5). The chance of being allocated to the Sweet and Fat DP was highest if the mother was allocated to the Sweet and Fat DP and soft drinks were available during meals (OR 2.78; 95% CI 1.80; 4.28). The child was more likely to be allocated to the Refined Cereals DP or the Animal Products DP if the mother was allocated to the same DPs and if no soft drinks were available during meals (OR 2.48; 95% CI 1.43 and 4.27; OR 2.16;1.59; 2.92, respectively). The child was most likely to be allocated to the Sweet and Fat DP, the Refined Cereals DP, and the Animal Products DP if the father was allocated to the respective DP and if soft drinks were not available during meals (OR 2.48; 95% CI 1.58; 3.87, OR 2.05; 95% CI 1.22; 3.45 and OR 2.48; 95% CI 1.62; 3.79, respectively). The chance of the child sharing the father’s Sweet and Fat DP is higher if soft drinks are available during meals (OR 4.26; 95% CI 2.16; 8.41).
4. Discussion
The present study suggests important similarities between children’s and parental DP. Three DP were obtained in this multi-country study: Animal Products, Refined Cereals, and Sweet and Fat. To our knowledge, this is the first study presenting the resemblance of the DP of pan-European children and their parents using cluster analysis. The study was further able to describe how the family food environment (operationalized as the number of shared meals and the availability of soft drinks during meals) moderated the association between children’s DP and parental DP.
Resemblance of dietary patterns between children and parents: Previously, maternal consumption of core foods (e.g., cereals, dairy, fruit, and vegetables) and non-core foods (e.g., snack foods, fats, and oils) has been shown to be associated with a child’s higher intake of the same foods [
5]. Mothers tend to be the person habitually preparing the family meals [
17] and mothers reported greater perceived responsibility for feeding their children [
18]. Women are known to exert positive influence on children’s food consumption [
42] because they are more likely to adhere to dietary guidelines [
43]. This is in line with our findings that identified the influencing nature of the maternal Animal Products DP per se and when the mother was eating with the child: in our study the Animal Products DP was characterized through the above-the-mean intake of healthy food alternatives such as fruit vegetables, healthy alternatives for meat, meat substitutes, milk and dairy products, cereals, and mixed dishes (
Figure 1). Reported EIs were lowest in the Animal Products DP and we observed the highest proportion of normal weight children in this DP but the highest proportion of overweight parents. Fathers’ influence on the child’s food choices was highest for the foods of the Sweet and Fat DP including all types of sugar and sweets, unhealthy fats and oils, unhealthy beverages, and unhealthy milk and dairy products. In particular, the
z-scores for non-alcoholic unhealthy beverages (including also soft drinks) were highest in the Sweet and Fat DP compared to the other two DP. Likewise, previous studies have reported that fathers have primary influence on the children’s intake of non-core foods [
8].
Dietary patterns and shared meals: In our study associations were found between children’s DP and maternal DP independently of the number of shared meals and in particular between children’s DP and fathers’ Sweet and Fat DP if ≥1 meal was eaten together. Also in previous studies, paternal influence has been found to predict child’s food intake in that fathers used pressure tactics whereas mothers praised children for eating certain things [
44]. In particular, Robinson et al. [
7] observed strong correlations for foods typically eaten at breakfast such as grains and fruit in child–father dyads for families with working mothers, indicating that fathers have breakfast with their children when mothers leave home early. Children and adolescents sharing three or more meals per week with the family had healthier dietary patterns compared to those who share fewer than three family meals [
45]. This is in contrast to our findings, where children who eat together with their fathers at least once a day were more likely to share the Sweet and Fat DP with their fathers than sharing the generally healthier Animal Products DP.
Dietary patterns and the availability of soft drinks during meals: Although the mechanisms for how family meals facilitate healthy eating behaviors have not been empirically explained, different approaches are currently discussed. Eating together is an important ritual for interacting with family members and offers opportunities for children to learn about eating by watching others [
3]. Also, low availability and consumption of convenient foods or sodas during family meals can contribute to healthy dietary intake patterns [
46]. On the other hand, the availability of soft drinks during shared meals and parental soft drink consumption were associated with the child’s soft drink consumption (Sweet and Fat DP) in our study. This is in line with earlier findings from U.S. studies where parental food choices [
3] and soft drink availability were strong influencing factors for the children’s intake [
25], identifying parents as gatekeepers for the family food environment and as role models. Those foods (preferred and) consumed by the parents were the foods to which children were routinely exposed and shaped the children’s food preferences and consumption [
47,
48]. It is not surprising that the availability of soft drinks and chips has been observed to be greater in families who frequently consumed fast food during family meals [
49]. We therefore suggest that home availability of foods is an important predictor for children’s preferences, even more so if parents choose the same foods during meals [
50]. Making healthy foods available and also eating those foods may enhance children’s understanding and acceptance of a healthy diet [
51].
Limitations and Strengths
In the I.Family study dietary information was mainly given by self-respondents. Self-reporting can be susceptible to reporting bias [
52]. We therefore followed a rigorous approach in order to reduce errors due to portion size estimation, incomplete recalls, misreporting, or daily variations in intake. Firstly, the development of the SACANA computer-assisted assessment tool with standardized photographs, multiple plausibility checks, and reminding questions facilitated the reporting of accurate portion sizes and complete recall. Secondly, as a first step in the data analysis, the exclusion of incomplete recalls and recalls with implausible energy reporting helped to correct for reporting bias. Individuals with misreported EI (under-reporters: 462 children, 465 adults; over-reporters: 22 children, six adults) were more likely to be female, from medium educated families, and from Estonia or Germany. They were more often overweight and obese (66% of adults; 36% of children) compared to plausible reporters (16% adults, 4% children). In a separate analysis we derived the clusters including the 955 misreporters in order to compare cluster memberships of the plausible reporters sample (1662 child–mother dyads and 789 child–father dyads) with the cluster memberships of the full study sample (2269 child–mother dyads and 1058 child–father dyads). After comparing the cluster membership of the full sample (also including misreporters) with the final study sample (plausible reporters only) we observed that the three DP remained comparable, except that EI was found to be lower in the Animal Products cluster when misreporters were included. As the Animal Products cluster included 58% of misreporting children and 83% of misreporting parents, including misreporters would overestimate intake (particularly in the Animal Product cluster) and underestimate the intake of plausible reporters (particularly in the Refined Cereals and Sweet and Fat clusters), given that we consider the percentage of energy contribution from dietary categories. We therefore decided to exclude the misreporters from the analysis. However, the question of how to handle possibly implausible interviews has not been answered conclusively: the inclusion of misreports may obscure or even inverse diet–disease relationships, as recently reported, and adjustment for the reporting group may also lead to bias [
53]. Finally, deriving the usual intake based on the NCI method [
37] and accounting for day-to-day variation in intake is a clear strength of this study.
As might be expected, we observed a resemblance between the parental DP and children’s DP. These improved relations do not reflect reporting bias (due to proxy-reporting of dietary intake), as reported in other studies [
18]. In the present study, participants personally reported dietary intake; thus the strength of association between child–mother dyads and child–father dyads truly reflect the environmental influence of parents on the child’s DP and can be seen as an additional strength of this study. In general, the I.Family study allows a deep insight into the resemblance of DP among family members across Europe and the influence of parental DP on their child’s DP when eating together or not. The large sample size comprises data from eight European countries; the strictly standardized data assessment, documentation, and data cleaning processing guarantee the highest possible data quality.

 ,
, 

{kind=link}