1. Introduction
Excess dietary salt intake is associated with elevated blood pressure, a major risk factor for cardiovascular diseases [
1,
2]. In 2010, an estimated 1.65 million cardiovascular deaths worldwide—or 1 out of every 10 cardiovascular deaths—were attributed to salt consumption above the World Health Organization (WHO) recommended intake of 5 g per day [
3,
4]. Salt reduction has been described by the WHO as one of the best investments to improve public health and an efficient and cost-effective way to decrease the burden of elevated blood pressure and cardiovascular diseases [
5].
In 2013, WHO Member States adopted the global target of a 30% reduction of mean population intake of salt by 2025, as part of a broader set of strategies to reduce premature mortality from non-communicable diseases by 25% in 2025 [
6]. A growing number of countries are developing and implementing strategies to reduce salt intake, including, but not limited to, food supply reformulations, front of package labelling, taxation, consumer education, and interventions in public institutions [
7,
8]. For many countries, these strategies are voluntary or restricted to a limited number of food products [
9].
The Republic of South Africa was the first country globally to develop comprehensive, mandatory legislation to reduce sodium levels across a wide range of processed food categories, which involved the co-operation of many food industry members from various sectors [
10,
11]. It is estimated that about half of daily salt intake in South Africa derives from processed foods, with bread being the greatest contributor to non-discretionary salt intake [
12,
13]. The South African sodium legislation was passed by the Department of Health in 2013 and set restrictions regarding the maximum levels of sodium allowed in several commonly consumed foods which, in addition to bread, include breakfast cereals, margarines, meat products, snack foods, and soup mixes [
10]. A few products that are high in sodium, such as biltong (“jerky”) and soy sauce, were exempted due to their relatively low contribution to sodium in the South African diet. The legislation aims to reduce the amount of sodium in specific foods in two waves; the first came into force in June 2016 and the second, with lower sodium targets, will come into effect in June 2019. If successful, this new strategy to reduce sodium in the food supply is expected to save thousands of lives annually and to yield substantial cost savings to the South African health service [
14,
15].
To measure progress in reducing the sodium levels of foods, identify challenges, and track changes over time, an assessment of the current sodium levels of processed foods in South Africa is needed. In the present study, we used data from nutrition information panels on food labels to evaluate the sodium levels of packaged foods in South Africa during the one-year period leading up to the implementation date for the legislation.
3. Results
After removing duplicates and products with ineligible or insufficient information on nutritional composition on the NIPs, 11,065 foods were included in the analyses. Of these, 20% were beverages, 16% were processed fruits and vegetable products, 10% were sauces and spreads, 9% were dairy products, 8% were cereal and cereal products, 8% were bread and bakery products, 6% were confectionery, 5% were convenience foods, 5% were meat or meat products, 3% were fish and fish products, and 3% were snack foods.
3.1. Median Sodium Level
There was substantial variation in the sodium level of processed foods within and between food categories (
Table A1). The food groups with the highest median sodium level were snack foods (746 mg/100 g), followed by meat and meat products (734 mg/100 g), and sauces and spreads (673 mg/100 g). Cereal and cereal products (70 mg/100 g), fruit and vegetable products (22 mg/100 g), confectionery (66 mg/100 g), and dairy (50 mg/100 g) had relatively lower median sodium levels. Within food groups, food categories with the highest median sodium levels were soups (2017 mg/100 g), sauces (999 mg/100 g), meal kits (939 mg/100 g), cheeses (554 mg/100 g), breads (476 mg/100 g), and noodles (470 mg/100 g). Food categories with the lowest sodium levels included several cereal products (e.g., pasta, maize, rice, couscous; all <10 mg/100 g) and dairy products, excluding cheeses (all <100 mg/100 g).
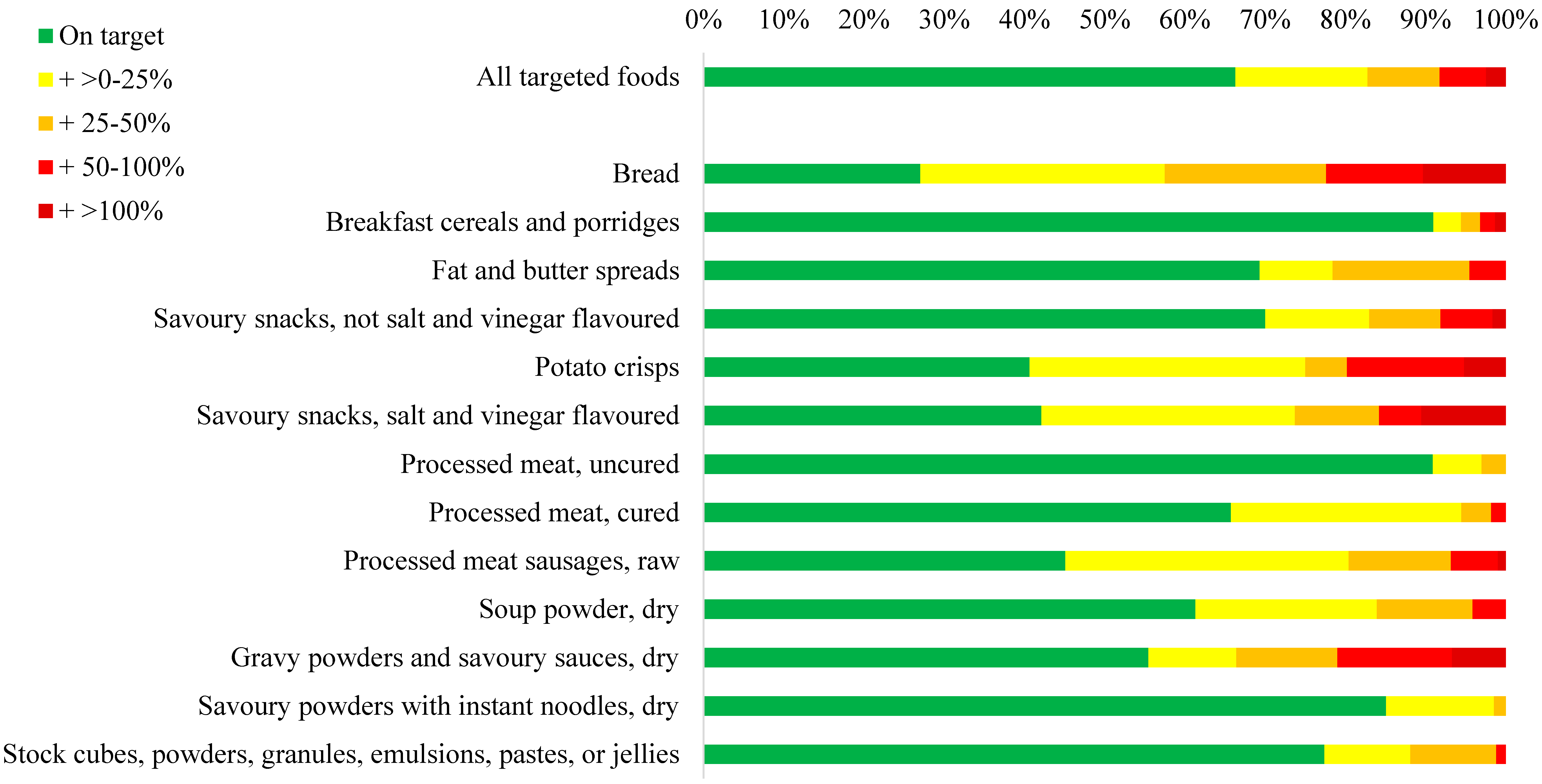
3.2. Sodium Levels of Foods Targeted by the Sodium Legislation
The median sodium level of foods targeted by the sodium legislation ranged from 171 mg/100 g for breakfast cereals and porridges to 4782 mg/100 g for dry soup powders (
Table 2). Other targeted food groups with very high median sodium levels (i.e., >1000 mg/100 g) were stock (3075 mg/100 g), gravy powders and savoury sauces (3029 mg/100 g), instant savoury powders with noodles (1123 mg/100 g), and salt and vinegar flavoured snacks (1094 mg/100 g). Overall, 67% of all targeted foods had a sodium level below the legislated maximum (
Figure 1). Categories with less than 50% of all products achieving the legislated maximum sodium level were bread (27%), potato crisps (41%), salt and vinegar flavoured snacks (42%), and raw processed sausages (45%) (
Figure 1). Over 90% of breakfast cereals and porridges and uncured processed meats had sodium levels below the legislated maximum allowed.
3.3. Sodium Reductions Needed to Meet the Sodium Target
Of targeted foods exceeding the legislated limits, sodium levels would need to be reduced by a quarter or less for 49% of these foods, by 25%–50% for 26% of foods, by 50%–100% for 17% of foods, and by more than 100% for 7% of foods (
Figure 1 and
Table A2). In absolute terms, the median reductions in sodium levels required to meet the limits were 110 mg/100 g for breads, 136 mg/100 g for potato crisps, 236 mg/100 g for salt and vinegar flavoured snacks, and 108 mg/100 g for raw processed sausages. Almost 50% of all gravy powders and savoury sauces exceeding the sodium limit, did so by 50% of the limit or more, equating to a median excess sodium level of 1700 mg/100 g.
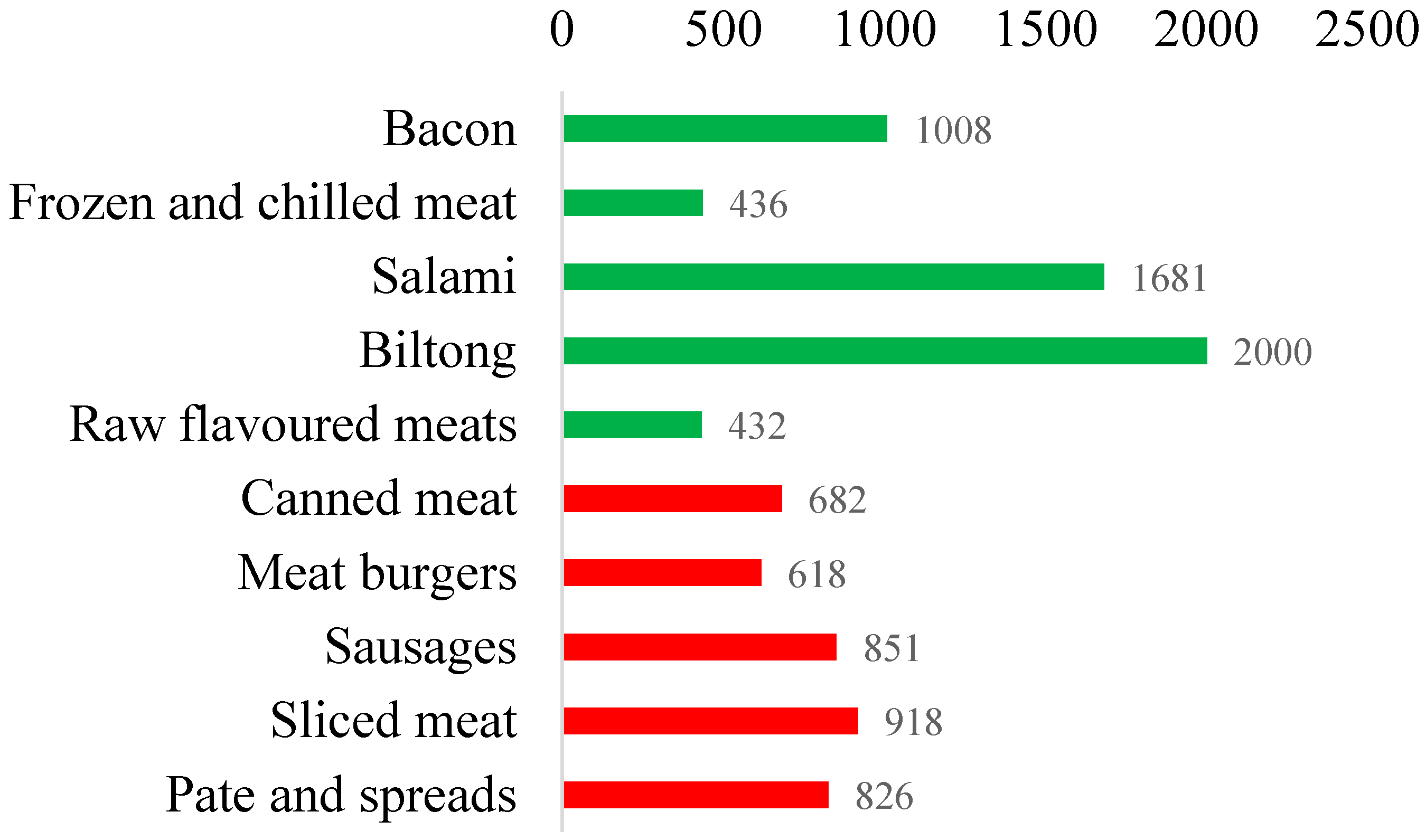
3.4. Sodium Levels within Categories Partially Targeted by the Sodium Legislation
The sodium legislation only targets a subset of meats and only dry (i.e., powdered) mixes for soups, sauces, stocks, and gravy. The median sodium levels of meat products targeted by the legislation was 638 mg/100 g for uncured processed meats, 864 mg/100 g for cured processed meats, and 826 mg/100 g for raw processed sausages. Sodium levels were higher in meats not targeted by the legislation; bacon, salami, and biltong, had a median sodium level of 1070 mg/100 g, 1674 mg/100 g, and 2079 mg/100 g, respectively (
Figure 2 and
Table A3). Canned and chilled soups, also not targeted by the legislation, had median sodium levels of 373 mg/100 g, and 303 mg/100 g, respectively. Stocks and gravy sold as liquid contained a median of 4000 mg and 429 mg of sodium per 100 g, respectively. Sauces not covered by the legislation that were high in sodium were curry pastes (2400 mg/100 g), Asian sauces (2499 mg/100 g), mustard (1760 mg/100 g), and table sauces (988 mg/100 g) (
Table 3).
4. Discussion
South Africa is the first country to adopt mandatory legislation for the reduction of sodium levels across a wide range of processed foods. Findings from this study indicate that two-thirds of targeted food items already met the maximum sodium limits during early stages of policy implementation. However, there was variation in the percentage of foods on target across legislated categories; while over 90% of breakfast cereals and uncured processed meats met the sodium targets, just over 40% of all crisps, salt and vinegar flavoured snacks, and raw processed sausages, and fewer than 30% of breads contained less sodium than the current maximum sodium limit.
Reduction of sodium intake is a global health priority. In 2014, 75 countries representing all WHO regions had national sodium reduction strategies, include food reformulation (81% of countries), front of package labelling (41%), consumer education (95%), and initiatives in public institutions [
7,
8]. Targets for food reformulation are often voluntary and, in most countries, are only for bread, which is often a large contributor to dietary sodium from processed foods [
7]. South Africa, and now also Argentina, are currently the only two countries with mandatory sodium limits for a range of food products across several different food industries. Several other countries have been successful in developing partnerships with the food industry to negotiate voluntary sodium reduction targets for processed foods [
9,
20]. In the UK, these voluntary sodium reduction targets have led to an estimated 7% decrease in the sodium levels in processed foods and there has been an 8 to 10% decrease in mean population salt consumption between 2006 and 2011 [
21,
22]. More challenging voluntary sodium targets were set for 2017 in order to achieve further reductions [
23,
24]. It will be important for the South African government to ensure that the regulated sodium limits are updated regularly to reflect the levels in the current food supply and global best practice. It will also be important to periodically check that the scope of the regulation is adequately capturing all products important to dietary salt consumption in the country.
The ultimate impact of the sodium legislation will be measured by its effect on reducing the burden of cardiovascular disease and associated health care expenditures. A modelling study that informed the development of the sodium legislation in South Africa estimated that a reduction of daily sodium intake of 0.85 g per person per day could avert 7400 cardiovascular deaths; 6400 of which would be due to reducing the sodium levels of bread alone [
14]. The additional 4300 non-fatal strokes that could be prevented are projected to save the strained South African health care system 40 million USD a year. An extended cost effectiveness analysis supported these findings and reported that the South African population salt reduction programme could also avert poverty and reduce household out of pocket expenditures, particularly for the middle class, at minimal cost [
15]. The impact of the sodium legislation on the burden of cardiovascular disease in South Africa will only become apparent some years after it is implemented. To attribute change in the burden of cardiovascular disease to the sodium legislation, assessment of each step between policy implementation and the anticipated health outcomes is needed, including evaluation of its impact on changes in the sodium levels of foods, population salt intake, and blood pressure levels [
25,
26,
27]. The HealthyFood Switch technologies used in this study provide an objective, practical, transferable, and scalable approach to assess the nutritional composition of packaged foods, to assess whether targeted food products comply with the legislation, and to facilitate global benchmarking.
This study has some limitations. First, the HealthyFood Switch database mainly comprises foods available from large retailers that predominantly serve the middle to higher socioeconomic urban population. While additional food items were added through crowdsourcing, our data are not necessarily representative of all packaged foods in South Africa. Second, we evaluated the sodium levels of foods available in-store and did not examine actual food purchases or consumption, nor market share of brands. However, there are data from the UK indicating that crude mean sodium levels of product ranges are broadly comparable to the weighted mean sodium levels of products actually sold [
28]. Third, since nutritional data were collected between the notification and early implementation period of the sodium legislation, we were unable to determine whether food manufacturers had already commenced reformulating, withdrawing, or replacing high-sodium products before the legislation came into effect. Fourth, sodium levels collected were derived from NIPs of packaged foods, which, although mostly deemed to be accurate [
29], are not necessarily derived from chemical analyses. Fifth, in some cases, the availability of ‘as prepared’ nutrition values alone (<15% of products) limited the capacity for robust comparison because mean sodium levels can be influenced by the recommended method of preparation for which there no agreed standards.
In conclusion, sodium levels of two-thirds of foods covered by the sodium legislation in South Africa already met the sodium target during early stages of policy implementation. Further, only moderate reductions in sodium content will be required to bring many of the currently products in line with the regulation. This represents an excellent opportunity for the South African food industry to make rapid improvements to the national food supply. The high sodium levels of nearly three-quarters of breads, the main contributor to non-discretionary sodium intake in South Africa, will require particular attention and should be an early focus of activity. Continued monitoring of sodium levels in foods is required to support industry action and ensure compliance with the legislation is achieved. Monitoring data will also enable modelled evaluation of the impact of the sodium legislation on dietary sodium intake and its downstream effects on population blood pressure levels and cardiovascular diseases.

 ,
, 



{kind=link}
{kind=link}

