1. Introduction
Acute Kidney Injury (AKI) is now considered a major clinical health problem [
1,
2]. In fact, its incidence is increasing, especially among ICU patients, and the syndrome still remains associated with highly negative outcomes [
3,
4]. Severe malnutrition has been documented in up to 40% of patients with AKI, and is associated with a further increase in the mortality risk and complications [
5].
Accurate determination of protein and energy needs is obviously important in this clinical setting, because both over- and underfeeding may occur and are associated with poor outcomes [
6,
7]. In particular, significant underfeeding has been recently documented in a recent re-analysis of data from a large cohort of patients with AKI from the RENAL study, whose average daily calorie and protein intake was respectively 867 kcal and 34.8 g [
8].
The gold standard for measuring individual caloric needs is represented by indirect calorimetry (IC), a noninvasive method allowing resting energy expenditure (REE) assessment based on oxygen consumption and carbon dioxide production measurements in the exhaled air [
9]. In critically ill patients, REE measured by IC is in general considered for nutritional prescription. However, during the very early phase (2–3 days) of an acute illness the body produces enough amount of energy to cover most of energy needs, increasing the risk for early overfeeding [
9]. Regarding proteins, the daily protein catabolic rate (PCR as g/24 h) reflects the amount of protein undergoing catabolism and could be considered the target for protein prescription. PCR can be derived from cumulative nitrogen excretion and urea kinetics, in the case of Renal Replacement Therapy (RRT), and can also be expressed as normalized PCR (nPCR, as g/kg of BW/24 h) [
10]. Unfortunately, IC measurements and nPCR are not widely used in daily ICU routine [
9], due to time constraints, reduced equipment availability, staffing scarcity, and costs [
9]. On the other hand, the important limitations and the lack of accuracy of conventional predictive equations for EE estimation in critically ill are well known [
11,
12,
13,
14,
15]. Moreover, data on their validity when applied to patients with AKI are scanty [
16]. Regarding proteins, while PCR of patients on RRT has been investigated in the past by urea kinetic methods [
10,
17,
18,
19,
20,
21], no data are currently available on PCR in patients with AKI not on RRT.
Thus, the purpose of our study in patients with AKI with or without RRT need was:
- (a)
to evaluate the validity of conventional predictive formulas and equations for the calculation of energy expenditure and protein needs, by using IC and the nPCR as gold standards;
- (b)
to compare prescribed and actually received nutrients with estimated and measured needs.
4. Discussion
Our study suggests that in critically ill patients with AKI none of the conventional equations and formulas used to predict REE is in good agreement with actual EE measured by IC, nor protein needs were correctly estimated. Moreover, actual nutrients intakes were significantly lower as compared to both the prescribed and the measured needs.
The most ancient and widely used equation is the Harris-Benedict, developed from healthy caucasic subjects in the beginning of the 20th century [
25]. In the present study, this equation was able to correctly predict EE over only 38% of time. In a very recent study on AKI patients, the same equation was the least precise, with only about 18% of cases predicting EE within 10% of the measured EE [
16]. In a systematic review of the literature on the accuracy of predictive equations for critically ill patients, the Harris-Benedict equation underestimated EE and the use of correction factors was suggested to adjust EE to the current individual situation [
13]. In the present study, the widely applied stress factor of 1.3 was used [
31]. The use of this factor unfortunately worsened the precision of the equation when applied to patients with AKI, with only 26% of estimates between 90–110% of EE measured by IC and 69% of estimates >110% of IC. An important factor likely to have increased the estimation error could be represented by the body weight value used for the calculations. In the case of patients undergoing RRT, the BW at the end of RRT was used, while for patients not on RRT the most recent BW before the IC measurement was considered for calculations. Other studies in critically ill patients also showed a low grade of agreement between Harris-Benedict equation—with and without injury factor correction—and EE measured by IC [
11,
12,
15,
16,
32,
33,
34,
35]. In addition, review studies do not recommend the use of Harris-Benedict equation, with or without injury factor, for critically ill patients [
13,
36].
Guidelines on renal and ICU patients [
23,
24,
37] recommend 20–25 kcal/kg/day during the acute phase of the disease, and 25–30 kcal/kg/day during recovery. However, in many cases it is not mentioned if the actual, pre-admission or ideal BW should be considered. In the present study, the use of 25 kcal/kg/day calculation overestimated EE in 67% of estimates; this very fact could be explained by the use of actual BW, however, when we performed the analysis excluding measurements during fluid overload, the same equation continued to overestimate the REE of patients. In accordance with this finding, a recent study on critically ill elderly patients also showed that estimate EE based only on the relationship of Kcal per Kg of BW likely overestimated EE [
38]. Thus, despite being a very simple way to predict EE, this approach is likely to increase the risk of overfeeding in ICU patients with AKI.
Unlike previous equations, the Faisy-Fagon [
12] and Penn-State [
13] equations were developed from EE measured in mechanically ventilated critically ill patients, and dynamic variables, such as body temperature and minute ventilation that may better reflect the metabolic state of the patient were included in the predictive formulas. In our study, the equations specific for ventilated patients had different performances. The Faisy-Fagon equation was the least precise, with 64% of estimates on the overfeeding category, while Penn-State had 40% of estimates between 90–110% of values obtained by IC. In a recent study on AKI patients that used the admission BW for the calculations, those equations underestimated EE [
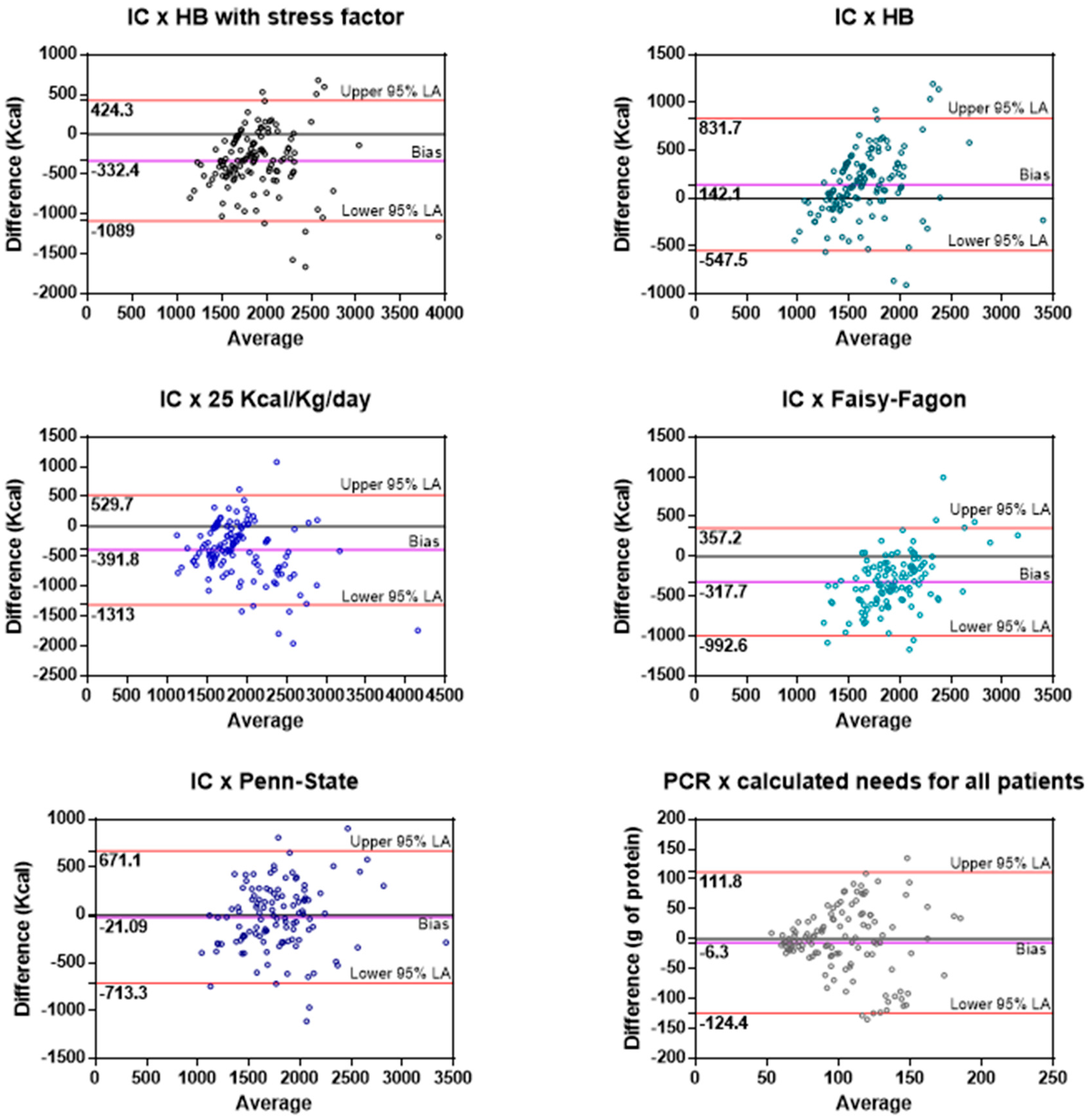
16], again underscoring the importance of the reference BW chosen for estimation. Although the Penn-State was more accurate in our patients, it is not precise enough and its wide limits of agreement highlight the potential to under or overfeed individual patients (
Figure 1). Therefore, it cannot be recommended for mechanically ventilated critically ill patients with AKI. A major problem is that no consensus exist on which BW should be utilized for EE estimation, thus explaining at least in part the differences observed in our study between measured and calculated needs, and also the dysomogeneity found among different studies. In our study, the actual BW after RRT was used; however, in some cases the patient’s weight at admission was used due to lack of BW availability during ICU stay. Nevertheless, also the analysis of the IC measurements that occurred in days with no fluid overload did not change our results. A very recent study on 205 critically ill patients compared REE measured by IC with Harris-Benedict equation calculated with 3 different reference weights (actual, ideal and predicted BW) [
39]. The use of actual BW resulted in the most accurate predicted REE; however, the limits of agreement between the equation and IC measurements were very wide [
39].
Finally, whether only one IC measurement at the beginning of recovery is enough to tailor nutritional prescriptions during ICU stay is still an open question. In our study there was no difference between energy measurements performed at the beginning of ICU stay and within one week, nor within 48 h, despite a vast majority of patients (68%) presenting with differences greater than ±10%, which could be clinically relevant. A retrospective study on 1171 critically ill patients found a significant (
p < 0.0001) between-day difference, however the difference lost significance after excluding the first 2 days of hospitalization [
40]. An expert position paper on IC in critically ill patients [
9] states that energy expenditure of critically ill patients is very dynamic and depends on the phase and the severity of illness, treatment and extended bedrest. The same concept holds true for AKI patients [
23,
24]. Thus, it is recommended that, whenever the clinical condition of the patient is changing, IC should be repeated.
In our study, the formulas used for the estimation of protein needs had different performances in patients on RRT and in patients not on RRT. Because patients undergoing RRT are likely to have more fluid overload, and since BW at the end of RRT was used for the calculations, protein catabolic rate values in these patients were lower than the estimated ones. However, excluding measurements obtained during fluid overload, the results were unchanged (all patients, patients not needing RRT, and patients undergoing RRT). Normalized PCR of 1.5–2.1 g/kg/day have been obtained by the urea kinetic method in small groups of patients with AKI on different modalities of RRT [
10,
17,
18,
19,
20,
21]. However, different BW were considered for protein intake normalization in these studies. In two studies the lowest BW measured during ICU stay was used [
19,
21], in another the actual BW [
20], and in the remaining 3 studies no information was available on which was the reference BW [
10,
17,
18]. Even Guidelines not always clearly specify which BW should be considered for protein needs estimation in critically ill patients with AKI (23–24). In the present study, actual BW was preferably used, and it was the same weight used for the EE estimation. Thus, the use of different BW could explain most of the differences in protein needs estimation, underlying the importance to obtain PCR in critically ill patients. As a matter of fact, recent studies suggest that adequate protein intake correlates to better outcomes in critically ill [
26,
41,
42,
43] and AKI patients [
21]; in addition, negative nitrogen balance was identified as a predictor of death in AKI patients [
44].
The present study has some limitations. First of all, the sample size was relatively small, however the number of measurements performed was high, which increased the accuracy of the Bland-Altman analysis. Second, the reference BW used to estimate REE and protein needs was the actual BW. The use of the actual BW might have influenced the calculated protein and energy needs since AKI patients frequently suffer from fluid overload, however different studies used different BW, and there is no clear recommendation regarding which BW should be considered when prescribing artificial nutrition in critically ill patients with AKI. Third, the RRT modality that was used more frequently was SLED (84% of the computed treatments). In our unit, SLED protocol is based on trisodium citrate as anticoagulant [
45]. It is well known that the use of trisodium citrate can provide hidden non nutritional calories (NNC) that should be considered during artificial nutrition prescription, in this study we did not consider the amount of calories provided by citrate during SLED. However, in a previous study published by our group that investigated the safety of citrate as anticoagulant for SLED, the average amount of NNC provided with our protocol was 90 kcal/SLED session of 8 h [
45]. Probably, the statistical significance of the difference between received and measured energy needs would have been lost for the RRT subgroup if we had considered the NNC from citrate anticoagulation during SLED. One last consideration that should be made regarding the limitations of our study is that we did not measure the amount of amino acids lost during RRT to be considered in the actual protein needs in addition to the PCR. A recent study on five patients undergoing SLED identified a median loss of 15.7 g of amino acids per treatment [
46]. This information in our study would probably not change the statistical significance of the difference between actual protein needs and estimated protein needs, and would increase the gap between actually received and protein need, only reinforcing the need for accurate protein need determination and prescription in the clinical practice.

 ,
, 

{kind=link}