Abstract
Purpose: Dysfunctional voiding (DV) is not uncommon in women with non-neurogenic voiding dysfunction. Because of its unknown pathophysiology, effective and durable treatment is lacking. This study aimed to analyze the results of treatment and predictive factors for a successful outcome of botulinum toxin A (BoNT-A) treatment in female patients with DV. Methods: In total, 66 women with DV confirmed by a videourodynamic study (VUDS) were treated with a BoNT-A injection into the urethral sphincter once (n = 33) or several times (n = 33). VUDS was performed before (baseline) and after the BoNT-A treatment. Patients with a global response assessment of the voiding condition of 2 or 3 and a voiding efficiency (VE) of >20% than baseline were considered to have a successful outcome. The baseline demographics, VUDS parameters, and VUDS DV subtypes were compared between the successful and failed groups. Predictive factors for a successful outcome were investigated by logistic regression analyses. Results: Successful and failed outcomes were achieved in 27 (40.9%) and 39 (59.1%) women, respectively. After BoNT-A injections, the maximum flow rate (Qmax), voided volume, and VE all significantly increased, and the postvoid residual (PVR) was slightly improved. No significant difference in the number of injections and medical comorbidity was found between the groups. However, the successful group had a higher incidence of previous pelvic surgery. No significant difference in the treatment outcome was found among patients with different urethral obstruction sites. Significant improvements in Qmax, voided volume, PVR, VE, and the bladder outlet obstruction (BOO) index were noted in the successful group. A lower VE at baseline and a history of surgery were identified as predictive factors for a successful outcome of BoNT-A injections for treating DV. Conclusion: BoNT-A injections into the urethral sphincter can effectively improve VE in 40.9% of women with DV. Women with higher BOO grades and previous pelvic surgery are predicted to have a successful treatment outcome.
Key Contribution:
Botulinum toxin A urethral sphincter injection is effective in treating women with dysfunctional voiding; however, the success rate is only 40.9%.
1. Introduction
Dysfunctional voiding (DV) in women is a condition of the lower urinary tract characterized with poor relaxation or dyssynergia of the urethral sphincter during voiding without neurological lesions or anatomical bladder outlet obstruction (BOO) [1]. The prevalence of female DV ranges from approximately 2.7% to 23% [2,3,4]. Although DV is commonly encountered in children with recurrent urinary tract infections (UTIs) and vesicoureteral reflux, the pathophysiology of female DV has not been well elucidated. Among various voiding dysfunctions in women, DV is the most challenging lower urinary tract disorder to treat [5]. Thus, effective treatment is still lacking. Patients with DV may experience difficulty urinating, large postvoid residual (PVR) urine volumes, recurrent UTIs, and bladder storage symptoms [6].
Various treatment modalities have been used to relax the urethral sphincter and pelvic floor muscles, such as training of the pelvic floor muscles, antimuscarinic therapy, sacral nerve neuromodulation, and posterior tibial nerve stimulation [4,7,8]. Given the lack of definitive medical treatment currently available for DV, clinicians have enthusiastically used urethral botulinum toxin A (BoNT-A) for this off-label indication [9]. However, a satisfactory outcome of BoNT-A has not been achievable for all patients with DV [10]. BoNT-A injections into the urethral sphincter are currently advocated for the treatment of female DV, mostly due to the simple and non-invasive procedure. Previous studies revealed that the success rate for improving voiding efficiency (VE) and the global response assessment (GRA) by one scale was approximately 70% in women with different subtypes revealed by videourodynamic study (VUDS). However, only 49.4% of women achieved a very good satisfactory outcome with a GRA of ≥2 [11,12]. Women with definite BOO might have a better successful outcome after BoNT-A injections into the urethral sphincter [13]. However, BoNT-A injections do not provide a durable treatment outcome, and patients need repeated BoNT-A injections to ensure therapeutic efficiency and maintain relief from lower urinary tract symptoms. There could be some pathophysiology underlying the factors that reduces the overall success rate of BoNT-A therapy for DV. This study retrospectively analyzed the treatment results and predictive factors for a successful outcome of BoNT-A treatment in female patients with DV.
2. Results
The study included a total of 66 patients. The mean age was 57.7 ± 15.6 (range, 10.4–85.1) years. Thirty-three (50%) women received only one BoNT-A injection into the urethral sphincter, and the other 33 (50%) received repeat injections. Repeat VUDS was performed 3 months after each BoNT-A injection, and the follow-up time ranged from 6 to 12 months. For patients who had several VUDS during the follow-up period, because the voiding symptoms might change over time, the best result was selected for the post-treatment evaluation, based on the lowest voiding pressure and highest maximum flow rate (Qmax). The results of the baseline and treatment VUDS are shown in Table 1. After BoNT-A injections, there were significant increases in Qmax, voided volume, and voiding efficiency (VE), with a slight improvement in postvoid residual (PVR). The baseline VUDS revealed a narrow bladder outlet at the mid-urethra in 47 women (71.2%) women, the distal urethra in 16 women (24.2%), and both the bladder neck and mid-urethra in 3 women (4.5%).

Table 1.
Baseline and post-treatment (BoNT-A) urodynamic findings.
A successful outcome was achieved in 27 (40.9%) women and a failed outcome in 39 (59.1%). The follow-up periods were 7.7 ± 5.2 and 9.3 ± 6.7 months for the successful and failed groups, respectively. Table 2 shows the patients’ demographics for the successful and failed groups. No significant difference in the number of injections, medical comorbidities, and previous surgery was found between the successful and failed subgroups, except for pelvic surgery, for which the successful group had a higher incidence of previous pelvic surgery. The pelvic surgery included hysterectomy (n = 12), colectomy (n = 2), oophorectomy (n = 2), and cystocele repair (n = 2).
Table 2.
Baseline demographics between successful and failed treatment outcomes.
In the comparison of the baseline VUDS findings between the successful and failed groups, the successful group had significantly older age, lower Qmax, smaller voided volume, greater PVR, and lower VE. However, no significant differences in the treatment outcome was found among patients with BOO at the bladder neck (33.3%), mid-urethra (36.2%), or distal urethra (56.3%) (Table 3).
Table 3.
Comparison of VUDS findings between failure and successful treatment outcomes.
Table 4 shows the changes in the VUDS parameters between the failed and successful groups. As expected, the successful group had significant improvement in Qmax, voided volume, PVR, VE, and BOOI. Interestingly, only the Pdet slightly decreased, and the volume of bladder sensation did not change after BoNT-A injections. On the contrary, none of the measured parameters showed significant changes after BoNT-A injections into the urethral sphincter in the failed group.
Table 4.
Changes in the VUDS parameters between patients with failed or successful treatment outcomes.
Univariate and multivariate logistic regression analyses were conducted to identify the predictors of a successful treatment outcome, based on the baseline characteristics and VUDS parameters. A lower VE at baseline and a history of pelvic surgery were found to be predictive factors for a successful outcome of BoNT-A injections for treating DV (Table 5).
Table 5.
Univariate and multivariate logistic regression analyses of the predictors of a successful treatment outcome for the baseline characteristics and VUDS parameters.
3. Discussion
This study revealed that a successful treatment outcome of BoNT-A injections, defined by a strict criterion of a GRA ≥2 and an improvement in VE by ≥20%, was achieved only in 40.9% of women with DV. The results were similar to our previous large-cohort retrospective analysis, i.e., a very satisfactory outcome could only be achieved in 40.9% of women with DV [11]. Moreover, a successful treatment outcome could be predicted for patients with a significantly lower baseline VE and previous pelvic surgery, suggesting the therapeutic effect of BoNT-A on dysfunction of the urethral sphincter is for true external sphincter spasticity but not other causes of voiding dysfunction in women.
The pathophysiology of non-neurogenic DV in women has not been well elucidated. Pelvic floor muscle overactivity or hypertonicity may be caused by inflammatory conditions of the pelvic organ, denervation and re-innervation of the pelvic floor, or a learned behavior [14,15,16,17]. In severe female DV, severe storage symptoms, recurrent urinary tract infections, chronic urine retention, or upper urinary tract deterioration may ensue [18]. Poor relaxation of the pelvic floor muscles is also commonly encountered in women with DV [14,15]. Dysfunctional pubococcygeal muscles could also contribute to the development of DV [17]. Differential diagnosis between true dysfunction of the urethral sphincter and dysfunction of the pelvic floor muscles is not easy, even by VUDS [12]. Thus, effective and durable treatment of DV has not currently been established. In addition to medical therapy, biofeedback-based pelvic floor muscle exercise, posterior tibial nerve stimulation, and BoNT-A injections into the urethral sphincter have proven effective in some women with DV; however, these are not durable treatment options [4,7,8,9]. Thus, repeated BoNT-A treatment is needed to ensure longer efficacy.
BoNT-A injections into the urethral sphincter have not been licensed for the treatment of voiding dysfunction caused by a dyssynergic urethral sphincter or DV; however, enthusiasm has been aroused because early clinical trials have demonstrated its efficacy and safety [9,10,11,12]. The rates of successful treatment outcomes vary widely, from 40% to 70%, depending on the definition of DV in the patients’ selection criteria and the determination of a successful treatment outcome [10,11,12]. Patients with DV may present with a narrow urethral lumen at the middle or distal portion during voiding. Some patients may present with a tight bladder neck initially and a tight mid-urethra after TUI-BN. These different clinical phenotypes might have different pathophysiologies; therefore, the treatment outcome might vary mildly. Patients who have both BND and DV were the best treated among three DV subgroups [11]. Regarding the pathophysiology of non-neurogenic voiding dysfunction, the dyssynergic urethral sphincter is not likely caused by suprasacral dysregulation between the detrusor and pudendal nucleus, such as in patients with spinal cord injury or multiple sclerosis. The DV might be a result of neurological dysregulation at the sacral cords or pelvic ganglionic level, which would also explain the effectiveness of sacral neuromodulation in modulating the micturition reflex circuit in the CNS and restoring the coordination between the detrusor and urethral sphincter during micturition [19,20].
BoNT-A injections into the urethral sphincter can result in the relaxation of the striated muscle by inhibiting the release of acetylcholine from nerve terminals and might inhibit the release of neuropeptides in the dorsal horn nucleus because of chronic inflammation [21]. With this dual mechanism of action, BoNT-A injections could result in relaxation of the urethral sphincter during voiding and increase the Qmax and VE [10]. A single BoNT-A injection might not resolve the chronic inflammation in the dorsal horn ganglia; therefore, repeated BoNT-A injections into the urethral sphincter might have a chance of long-term efficacy [22,23]. Although the theoretical benefits of BoNT-A injections for the urethral sphincter seem reasonable, the present and previous studies have revealed that this treatment goal is still not achievable in over half of the patients with DV. These patients often still require clean intermittent catheterization to evacuate a large PVR and prevent UTIs [10]. The pathophysiology of the successful and failed groups might be different, which needs further investigation.
Dysregulated urethral function with spastic or a non-relaxing external urethral sphincter has been considered a cause of DV, leading to voiding symptoms, such as slow urinary flow and a large PVR [15,24]. However, the actual mechanism for DV is not well understood. It is possible that different pathophysiologies might exist in hypertonicity of the female urethral sphincter or pelvic floor, which might result in DV with varying degrees of urethral narrowing during voiding. Therefore, the reduction in the urethral sphincter’s hypertonicity by BoNT-A injections and the resumption of spontaneous voiding usually cannot achieve a highly satisfactory rate through a single injection. Many women might have a mild improvement (GRA = 1) and a small increase in VE (10%), and only 40% of the patients achieved good satisfaction. The suboptimal treatment outcome of female DV is also possibly caused by chronic inflammation in the CNS and sensitization, leading to the persistent sensitization and hyperactivity of the urethral sphincter. Under this consideration, we hypothesize that repeat BoNT-A injections into the urethral sphincter might help adequately alleviate the inflammation of the CNS through the sensory nerves of the pudenda, leading to a long-term relaxation of the urethral sphincter. However, in this study, no significant difference was found in the number of BoNT-A injections regarding a successful outcome. Therefore, the exact mechanism for effective BoNT-A injections for treating DV remains unknown.
This study revealed that the successful group had a higher BOO grade, including higher Pdet, lower Qmax, larger PVR, and lower VE during VUDS. This finding was compatible with the results of our previous cohort studies, reporting that a higher BOO grade indicated a successful BoNT-A treatment outcome [11,12,13]. Interestingly, this group also had a higher incidence of previous pelvic surgery. The reason for this association between pelvic surgery and a higher BOO grade is unknown; however, the results imply that a dyssynergic urethral sphincter may be directly or indirectly related to the dysregulation of the sympathetic and parasympathetic nerves in the pelvic nerve plexus after previous pelvic organ surgery. Previous studies have shown that a crosstalk between the pelvic organs is present after long-term sensitization of the pelvic organ between the lower urinary tract and the colon [25]. The inflammation-induced sensory afferent activation from the pelvic organ’s wound may contribute to cross-sensitization, such as in patients with bladder pain syndrome or hypertonicity of the pelvic floor muscles [26]. Spinal cord inflammation may also develop after pelvic organ surgery; therefore, patients might have DV and a higher BOO grade during voiding.
Contrastingly, the pathophysiology of DV has not been fully elucidated. Several theories have accounted for DV in women and children. In addition to the association with encopresis in children, dysregulation of the CNS or learned habits have been considered to cause DV in children and women, which could be effectively treated by biofeedback therapy [27,28]. Because the causes of DV might not only originate from the urethral sphincter’s hypertonicity but also from dysfunctions of the pelvic floor muscles, BoNT-A injections into the urethral sphincter could not effectively decrease the muscular tone and adequately relieve the bladder outlet’s resistance. Therefore, the BOOI in the failed group was relatively lower than that in the successful group, and changes in the BOOI were also not significant after BoNT-A injections into the urethral sphincter in the failed group. The results of this study further emphasize that BoNT-A injections into the urethral sphincter are effective in reducing urethral resistance only in women with evident BOO because of a hypertonic or dyssynergic urethral sphincter [13,29]. Patients who are not likely to have BOO caused by a dysfunctional urethral sphincter, as manifested by a lower Pdet, higher Qmax, and a higher VE, might not benefit from BoNT-A injections into the urethral sphincter.
The limitations of this study include the small number of cases, the retrospective analysis, and the non-randomized design. Additionally, the follow-up period extending beyond 6 months after the latest BoNT-A injection suggested that the effects of BoNT-A injections into the urethral sphincter may not be durable. The possible reason is that the underlying pathophysiology of DV is not adequately resolved by BoNT-A injections into the urethral sphincter. Given the unsatisfactory success rate, the purpose of this study aimed to investigate any predictive factors for selecting appropriate patients for BoNT-A injections in the future. Further investigations into the electrophysiology and autonomic dysregulation of DV might help urologists understand this disease and provide more effective treatment.
4. Conclusions
This study revealed that BoNT-A injections into the urethral sphincter can effectively improve VE and GRA in only 40.9% of women with DV. Women with a successful treatment outcome had higher BOO grades, lower VE, and previous pelvic surgery, whereas patients with treatment failure had lower BOO grades and higher VE.
5. Methods
From September 2020 to September 2023, 66 consecutive women with voiding dysfunction received BoNT-A injections into the urethral sphincter for a clinical and VUDS-confirmed diagnosis of DV. This retrospective study analyzed the treatment outcomes. All patients had undergone a VUDS examination and were found to have high voiding pressure, a low maximum flow rate (Qmax), and a narrow bladder neck, mid-urethra, or distal urethra, as demonstrated by voiding cystourethrography [12]. The participants who had previously been treated with an alpha-blocker and baclofen without success then received BoNT-A injections into the urethral sphincter. Patients who had urodynamic detrusor overactivity (DO) were also treated with antimuscarinics or beta-3 adrenoceptor agonists. Patients with voiding dysfunction due to SCI, a cerebral vascular accident (CVA), multiple sclerosis, or peripheral neuropathy were classified as having neurogenic voiding dysfunctions and were excluded from this study.
This study was approved by the institutional review board of the authors’ hospital (IRB: 110-265-A, dated 1 July 2022). Informed consent was waived due to the retrospective study design. All study procedures were in accordance with the Declaration of Helsinki.
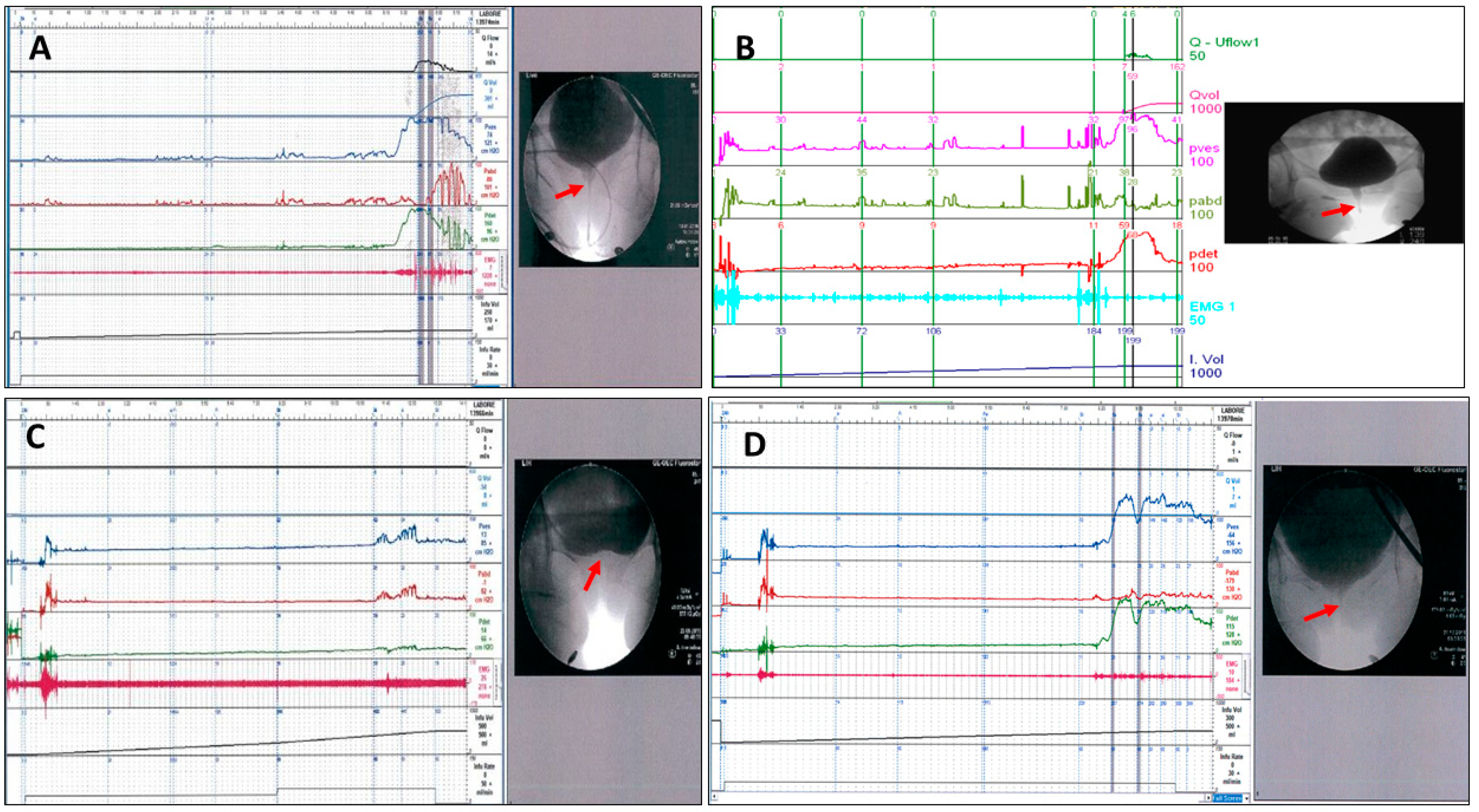
The videourodynamic parameters of the VUDS, including the status of the bladder neck during voiding cystourethrography, first bladder sensation (FSF), cystometric bladder capacity (CBC), detrusor pressure (Pdet), maximum flow rate (Qmax), PVR, and abdominal pressure to void, were recorded and analyzed [6]. The terminologies used in this study were in accordance with the recommendations of the International Continence Society [30]. DO that occurred during the bladder storage phase and before uninhibited voiding were recorded as phasic DO and terminal DO, respectively. The VE (defined as voided volume/CBC), the BOO index (BOOI, defined as Pdet–2 × Qmax), and the bladder contractility index (BCI, defined as Pdet + 5 × Qmax) were calculated from the measured parameters. During voiding, the appearance of the bladder outlet was carefully evaluated. DV was defined by a high voiding Pdet (≥35 cmH2O), a low Qmax < 15 mL/s, and urethral narrowing at the mid-urethra (Figure 1A) or distal urethra (Figure 1B) [1,31]. Patients with a history of transurethral incision for bladder neck dysfunction (BND) (Figure 1C) but who were found to have mid-urethral BOO during a follow-up VUDS were specifically categorized as having BND plus DV. (Figure 1D) Electromyography (EMG) of the urethral sphincter was performed using surface EMG patches to record the pelvic floor muscles’ activity during voiding, which could show intermittency, hyperactivity, or non-relaxation [29]. Repeat VUDS was performed at 6–12 months after the initial diagnosis of DV.
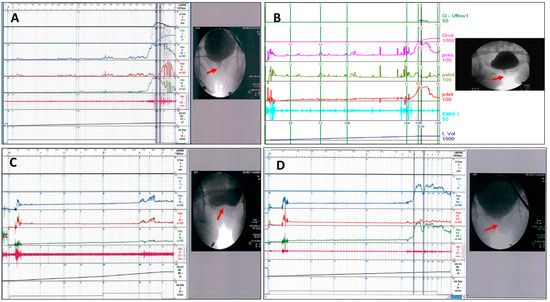
Figure 1.
VUDS characteristics of bladder outlet obstruction in women with dysfunctional voiding (DV), with urethral narrowing (arrow) at the (A) mid-urethra, (B) distal urethra, (C) bladder neck before transurethral incision of the bladder neck (TUI-BN), and (D) DV at the mid-urethra after TUI-BN of the woman shown in Figure 1C.
The procedure of BoNT-A injections into the urethral sphincter followed the protocol outlined in our previous reports [10]. In total, 100 U of onabotulinum toxin A was dissolved into 5 mL of a normal saline solution. Under intravenous general anesthesia, the BoNT-A solution was injected into the urethral sphincter along the urethral lumen at the 2, 5, 7, 10, and 12 o’clock positions by a single author (HCK). The injecting needle was inserted into the urethral sphincter at each injection site to depths of 2.0 cm and 1.0 cm, with 0.5 mL of the BoNT-A solution injected into each site. Following the BoNT-A injections, the urine was drained, and the patients were discharged after they had awakened and were free of adverse events. Patients were then followed up at the outpatient clinic to assess changes in voiding symptoms, Qmax, and PVR. Medical therapy with alpha-blockers with or without baclofen was continued as needed.
When patients still experienced voiding difficulty, low Qmax, and large PVR after the initial BoNT-A injection, repeated BoNT-A injections into the urethral sphincter were recommended at least 6 months after the prior injection Some patients preferred to stay on medical therapy and declined repeat BoNT-A injections. VUDS was repeated to compare the storage and voiding parameters and assess the treatment results of the BoNT-A injections. The treatment outcome was assessed 6 months after the last urethral BoNT-A injection. Improvement in voiding symptoms was evaluated by the GRA, defined as markedly worse (−3), moderately worse (−2), mildly worse (−1), no change (0), mildly improved (+1), moderately improved (+2), and markedly improved (+3) [32]. Patients with a GRA of two or three points and a post-treatment improvement in VE of 20% or more compared with the baseline were considered to have a successful outcome. Otherwise, the treatment was considered a failure. Patients who did not respond to urethral BoNT-A injections were recommended to undergo additional therapy, including sacral neuromodulation (n = 2), pelvic floor muscle biofeedback therapy (n = 5), or transcutaneous tibial nerve stimulation (n = 3). However, these treatments did not yield satisfactory results for all patients. Continuous variables are expressed as means with standard deviations, and categorical data are presented as numbers and percentages. The chi-square test for categorical variables and the Wilcoxon rank-sum test for continuous variables were used to determine p-values between groups for statistical comparisons. All assessments were two-sided and considered significant at p < 0.05. All calculations were performed using SPSS for Windows, version 16.0 (SPSS, Chicago, IL, USA).
Author Contributions
Conceptualization, H.-C.K.; methodology, Y.-H.J. and H.-C.K.; validation, H.-C.K.; formal analysis, Y.-H.J.; investigation, Y.-H.J. and H.-C.K.; resources, H.-C.K.; data curation, H.-C.K.; writing—original draft preparation, C.-C.Y.; writing—review and editing, Y.-H.J.; supervision, H.-C.K.; funding acquisition, H.-C.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the grants of Tzu Chi Mical Foundation, TCMF-SP-112-01, TCMF-IMC 112-01, and TCMF-MP 110-03-01.
Institutional Review Board Statement
110-265-A, dated 1 July 2022.
Informed Consent Statement
Informed consent was waived due to the retrospective study design. All study procedures were in accordance with the Declaration of Helsinki.
Data Availability Statement
Data of this study are available by contacting the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol. Urodyn. 2010, 29, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Massey, J.A.; Abrams, P.H. Obstructed voiding in the female. Br. J. Urol. 1988, 61, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Nitti, V.W.; Fiske, J. Cystometrogram versus cystometrogram plus voiding pressure-flow studies in women with lower urinary tract symptoms. J. Urol. 1999, 161, 201. [Google Scholar] [CrossRef]
- Groutz, A.; Blaivas, J.G.; Pies, C.; Sassone, A.M. Learned voiding dysfunction (non-neurogenic, neurogenic bladder) among adults. Neurourol. Urodyn. 2001, 20, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Kim, J.C.; Lee, K.S.; Seo, J.T.; Kim, H.-J.; Yoo, T.K.; Lee, J.B.; Choo, M.-S.; Lee, J.G.; Lee, J.Y. Analysis of female voiding dysfunction: A prospective, multi-center study. Int. Urol. Nephrol. 2013, 45, 989–994. [Google Scholar] [CrossRef]
- Malde, S.; Solomon, E.; Spilotros, M.; Mukhtar, B.; Pakzad, M.; Hamid, R.; Ockrim, J.; Greenwell, T. Female bladder outlet obstruction: Common symptoms masking an uncommon cause. LUTS Low. Urin. Tract Symptoms 2019, 11, 72–77. [Google Scholar] [CrossRef]
- Minardi, D.; D’Anzeo, G.; Parri, G.; Polito, M.; Piergallina, M.; El Asmar, Z.; Marchetti, M.; Muzzonigro, G. The Role of uroflowmetry biofeedback and biofeedback training of the pelvic floor muscles in the treatment of recurrent urinary tract infections in women with dysfunctional voiding: A randomized controlled prospective study. Urology 2010, 75, 1299–1304. [Google Scholar] [CrossRef]
- Espuña-Pons, M.; Cardozo, L.; Chapple, C.; Sievert, K.; van Kerrebroeck, P.; Kirby, M.G. Overactive bladder symptoms and voiding dysfunction in neurologically normal women. Neurourol. Urodyn. 2012, 31, 422–428. [Google Scholar] [CrossRef]
- Lo, C.-W.; Wu, M.-Y.; Yang, S.S.-D.; Jaw, F.-S.; Chang, S.-J. Comparing the Efficacy of OnabotulinumtoxinA, Sacral Neuromodulation, and Peripheral Tibial Nerve Stimulation as Third Line Treatment for the Management of Overactive Bladder Symptoms in Adults: Systematic Review and Network Meta-Analysis. Toxins 2020, 12, 128. [Google Scholar] [CrossRef]
- Nadeem, M.; Lindsay, J.; Pakzad, M.; Hamid, R.; Ockrim, J.; Greenwell, T. Botulinum toxin A injection to the external urethral sphincter for voiding dysfunction in females: A tertiary center experience. Neurourol. Urodyn. 2022, 41, 1793–1799. [Google Scholar] [CrossRef]
- Lee, C.-L.; Chen, S.-F.; Jiang, Y.-H.; Kuo, H.-C. Effect of videourodynamic subtypes on treatment outcomes of female dysfunctional voiding. Int. Urogynecology J. 2022, 33, 1283–1291. [Google Scholar] [CrossRef]
- Jiang, Y.-H.; Lee, C.-L.; Chen, S.-F.; Kuo, H.-C. Therapeutic Effects of Urethral Sphincter Botulinum Toxin A Injection on Dysfunctional Voiding with Different Videourodynamic Characteristics in Non-Neurogenic Women. Toxins 2021, 13, 362. [Google Scholar] [CrossRef]
- Chow, P.-M.; Hsiao, S.-M.; Kuo, H.-C. Obstructive patterns in videourodynamic studies predict responses of female dysfunctional voiding treated with or without urethral botulinum toxin injection: A long-term follow-up study. Int. Urogynecology J. 2020, 31, 2557–2564. [Google Scholar] [CrossRef]
- Carson, C.; Segura, J.; Osborne, D. Evaluation and treatment of the female urethral syndrome. J. Urol. 1980, 124, 609–610. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, W.E.; Firlit, C.F.; Schoenberg, H.W. The female urethral syndrome: External sphincter spasm as etiology. J. Urol. 1980, 124, 48–49. [Google Scholar] [CrossRef]
- Raz, S.; Smith, R.B. External sphincter spasticity syndrome in female patients. J. Urol. 1976, 115, 443–446. [Google Scholar] [CrossRef] [PubMed]
- Deindl, F.M.; Vodusek, D.B.; Bischoff, C.H.; Hartung, R. Dysfunctional voiding in women: Which muscles are responsible? Br. J. Urol. 1998, 82, 814–819. [Google Scholar] [CrossRef]
- Hinman, F., Jr. Nonneurogenic neurogenic bladder (the Hinmann syndrome)—15 years later. J. Urol. 1986, 136, 769–777. [Google Scholar] [CrossRef]
- Ho, F.C.S.; He, C.; Yao, H.H.; O’Connell, H.E.; Gani, J. Efficacy of sacral neuromodulation and percutaneous tibial nerve stimulation in the treatment of chronic nonobstructive urinary retention: A systematic review. Neurourol. Urodyn. 2021, 40, 1078–1088. [Google Scholar] [CrossRef]
- Agnello, M.; Vottero, M.; Bertapelle, P. Sacral neuromodulation to treat voiding dysfunction in patients with previous pelvic surgery for deep infiltrating endometriosis: Our centre’s experience. Int. Urogynecol. J. 2021, 32, 1499–1504. [Google Scholar] [CrossRef] [PubMed]
- Jhang, J.-F.; Kuo, H.-C. Botulinum Toxin A and Lower Urinary Tract Dysfunction: Pathophysiology and Mechanisms of Action. Toxins 2016, 8, 120. [Google Scholar] [CrossRef] [PubMed]
- Desrosiers, L.; Knoepp, L.R. Botulinum Toxin A: A Review of Potential Uses in Treatment of Female Urogenital and Pelvic Floor Disorders. Ochsner J. 2020, 20, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.P.; Nishiguchi, J.; O’leary, M.; Yoshimura, N.; Chancellor, M.B. Single-institution experience in 110 patients with botulinum toxin A injection into bladder or urethra. Urology 2005, 65, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.C. Dysfunctional voiding in women with lower urinary tract symptoms. Tzu Chi Med. J. 2000, 12, 217–223. [Google Scholar]
- Ustinova, E.E.; Fraser, M.O.; Pezzone, M.A. Cross-talk and sensitization of bladder afferent nerves. Neurourol. Urodyn. 2010, 29, 77–81. [Google Scholar] [CrossRef]
- Yoshikawa, S.; Kawamorita, N.; Oguchi, T.; Funahashi, Y.; Tyagi, P.; Chancellor, M.; Yoshimura, N. Pelvic organ cross-sensitization to enhance bladder and urethral pain behaviors in rats with experimental colitis. Neuroscience 2015, 284, 422–429. [Google Scholar] [CrossRef]
- Kajbafzadeh, A.-M.; Sharifi-Rad, L.; Ghahestani, S.M.; Ahmadi, H.; Kajbafzadeh, M.; Mahboubi, A.H. Animated biofeedback: An ideal treatment for children with dysfunctional elimination syndrome. J. Urol. 2011, 186, 2379–2385. [Google Scholar] [CrossRef]
- Chiang, C.-H.; Jiang, Y.-H.; Kuo, H.-C. Therapeutic efficacy of biofeedback pelvic floor muscle exercise in women with dysfunctional voiding. Sci. Rep. 2021, 11, 13757. [Google Scholar] [CrossRef]
- Brucker, B.M.; Fong, E.; Shah, S.; Kelly, C.; Rosenblum, N.; Nitti, V.W. Urodynamic differences between dysfunctional voiding and primary bladder neck obstruction in women. Urology 2012, 80, 55–60. [Google Scholar] [CrossRef]
- Schäfer, W.; Abrams, P.; Liao, L.; Mattiasson, A.; Pesce, F.; Spangberg, A.; Sterling, A.M.; Zinner, N.R.; van Kerrebroeck, P.; International Continence Society. Good urodynamic practices: Uroflowmetry, filling cystometry, and pressure-flow studies. Neurourol. Urodyn. 2002, 21, 261–274. [Google Scholar] [CrossRef]
- Carlson, K.V.; Rome, S.; Nitti, V.W. Dysfunctional voiding in women. J. Urol. 2001, 165, 143–147. [Google Scholar] [CrossRef]
- Propert, K.; Mayer, R.; Wang, Y.; Sant, G.; Hanno, P.; Peters, K.; Kusek, J.; Interstitial Cystitis Clinical Trials Group. Responsiveness of symptom scales for interstitial cystitis. Urology 2006, 67, 55–59. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).