
Advancements in Wearable and Implantable Intraocular Pressure Biosensors for Ophthalmology: A Comprehensive Review




Abstract
1. Introduction
2. Overview of Glaucoma
2.1. Understanding the Importance of Intraocular Pressure and Its Role in Glaucoma
2.2. Global Prevalence of Glaucoma
2.3. Classifications of Adult Glaucoma
2.4. The Dynamics of Aqueous Humor: Production, Outflow, and Their Role in Intraocular Pressure
3. Measurement of IOP
- Mackay–Marg–type tonometers: these flatten a small area of the cornea and measure the pressure in the center of the ring; devices like Tono-Pen are portable and useful for patients with corneal scars or edema, as well as those who can only be in a supine position, despite possible inaccuracies at high and low IOP levels (i.e., overestimate low IOPs and underestimate high IOPs) [17,25,26].
- Indentation tonometry (Schiøtz): measures corneal indentation produced by a known weight, accuracy is highly dependent on ocular biomechanical properties, and does not require electrical power [17].
4. Intraocular Pressure (IOP) Fluctuation
4.1. Instantaneous IOP Fluctuation
4.2. Diurnal-Nocturnal IOP Fluctuation
4.3. Short-Term IOP Fluctuation
4.4. Long-Term IOP Fluctuation
4.5. Beyond IOP Reduction: The Importance of Stability in Glaucoma Management
5. Principles and Engineering Aspects of IOP Biosensors
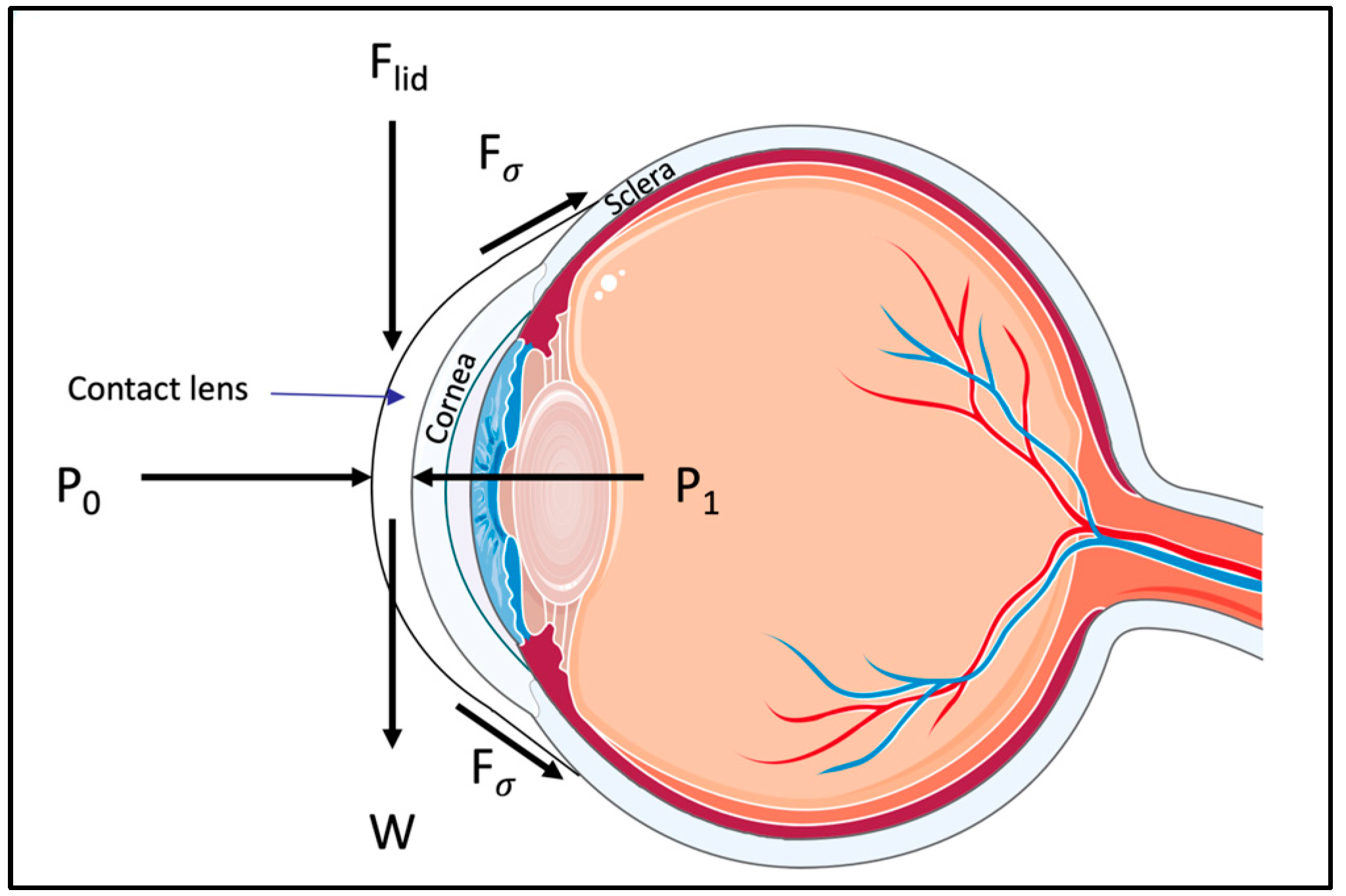
5.1. Engineering of Contact-Lens-Based Sensors
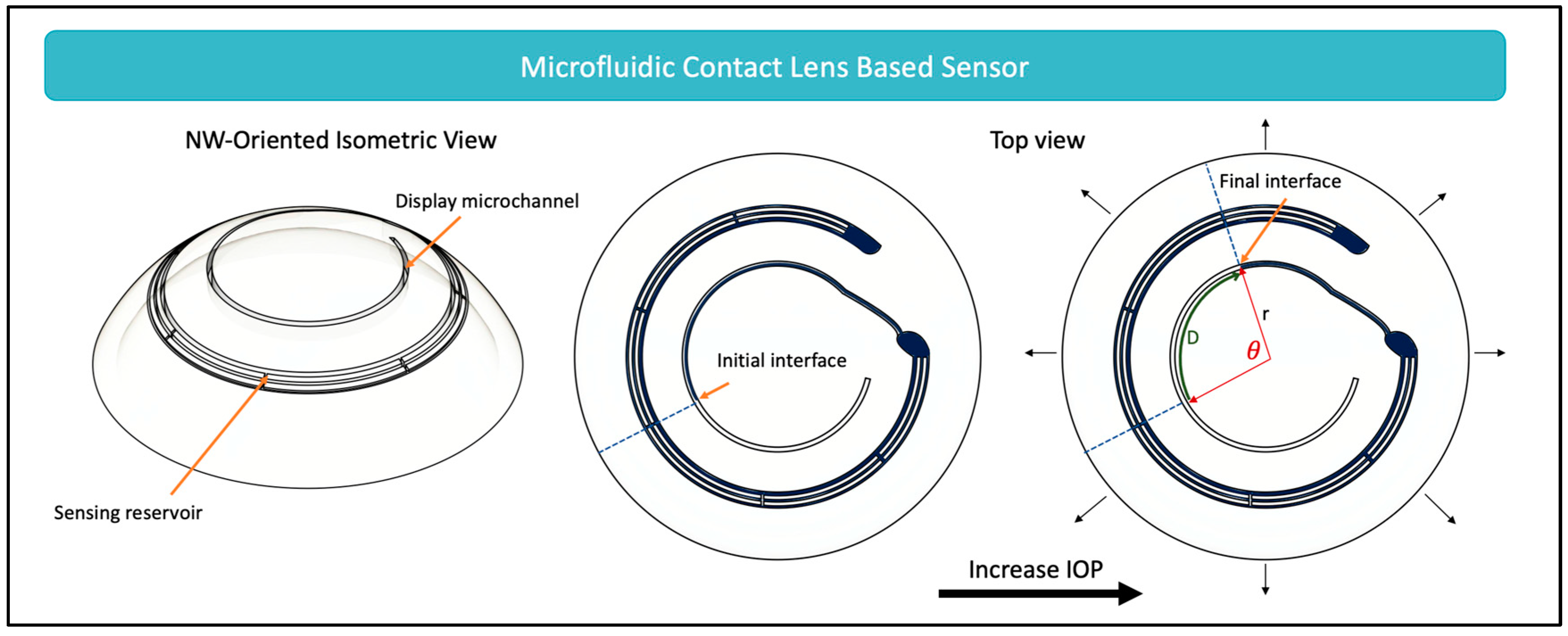
5.1.1. Microfluidic Dilatometer-Based Wearable Sensors
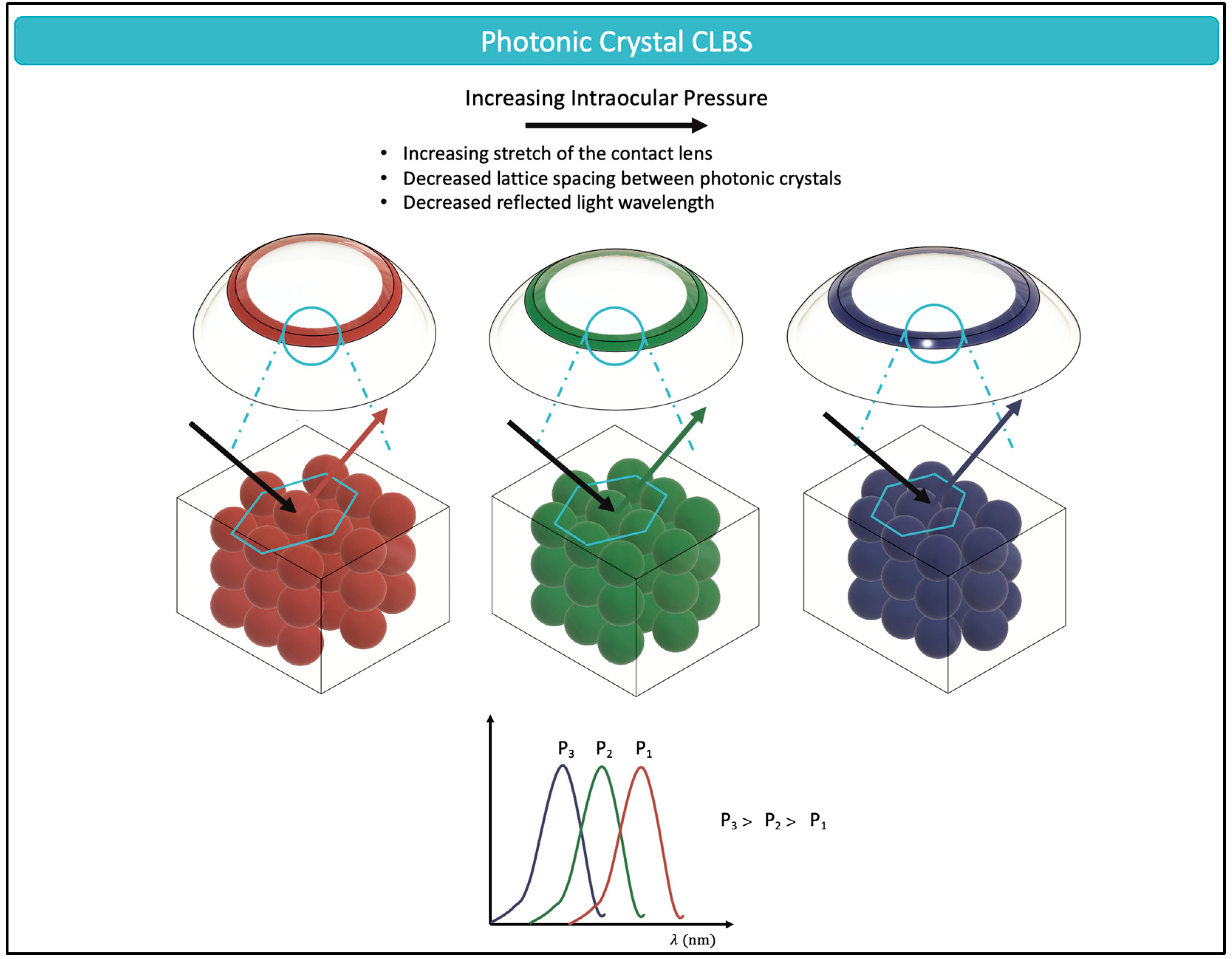
5.1.2. Optical (Phototonic Crystal) Wearable Sensors
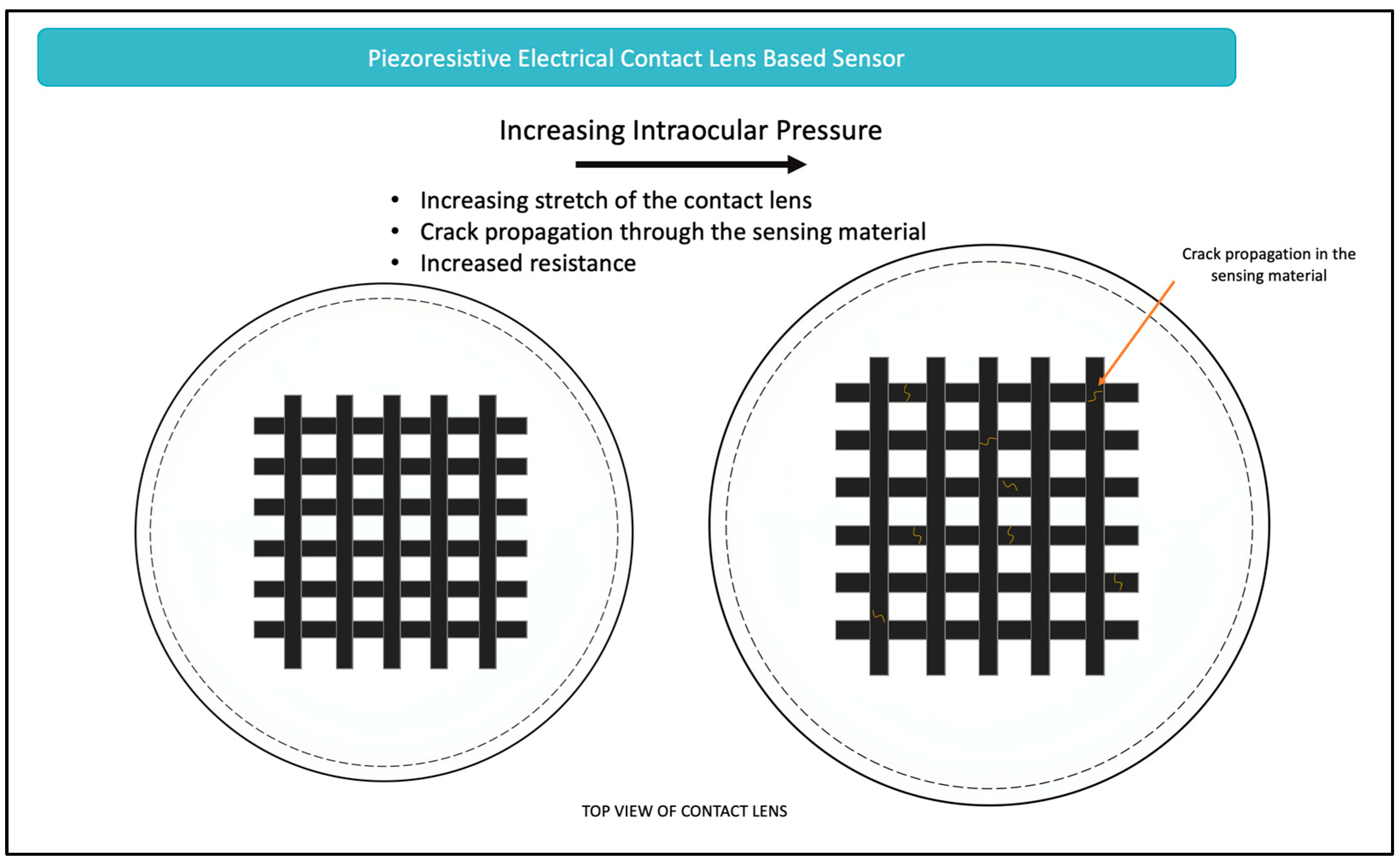
5.1.3. Electrical Wearable Sensor
Piezoresistive Sensors
Inductive Couple Telemetry Sensors
5.2. Engineering of Glasses-Based Sensors
5.3. Engineering of Implantable Sensor
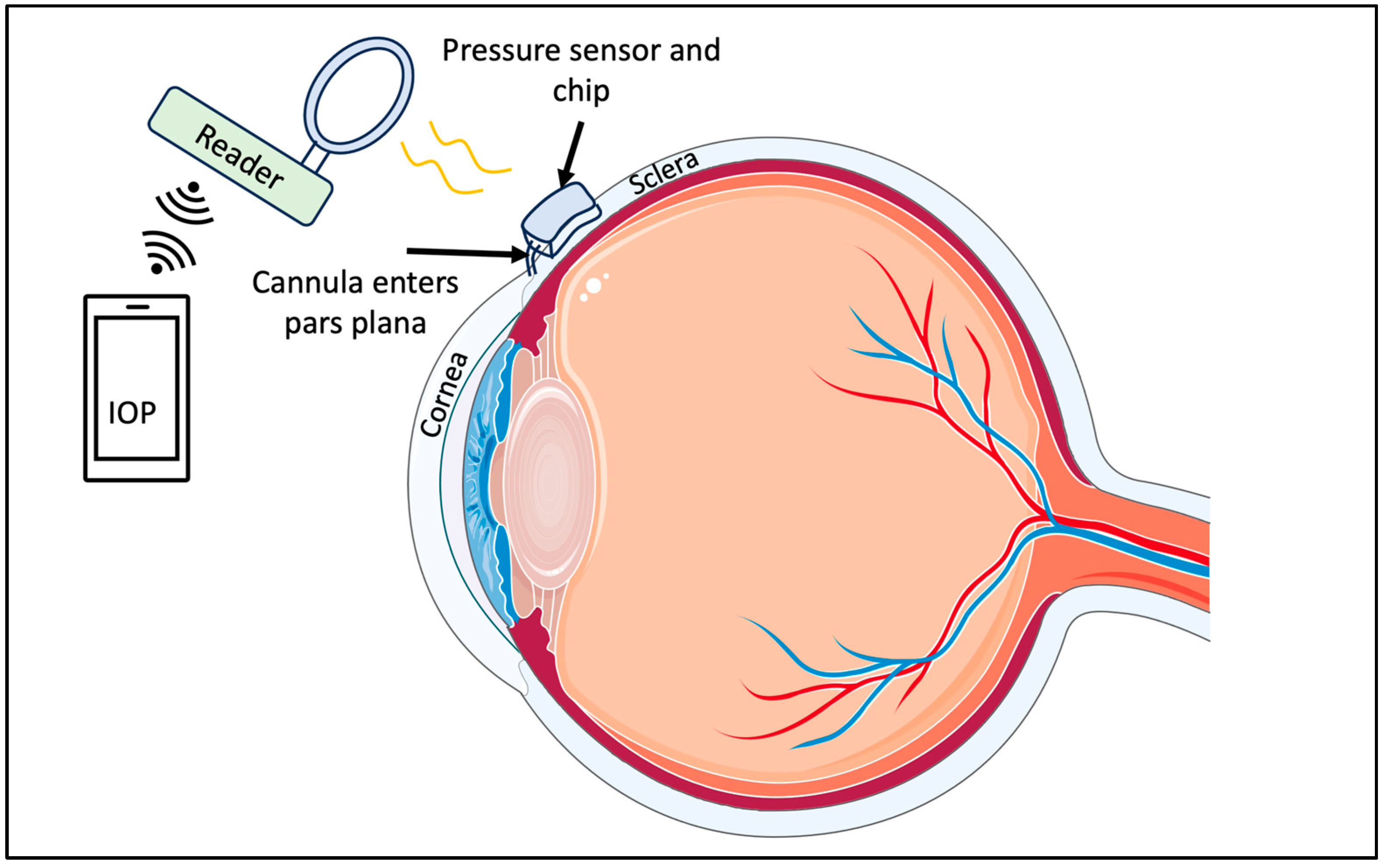
5.3.1. Capacitor-Based Sensors
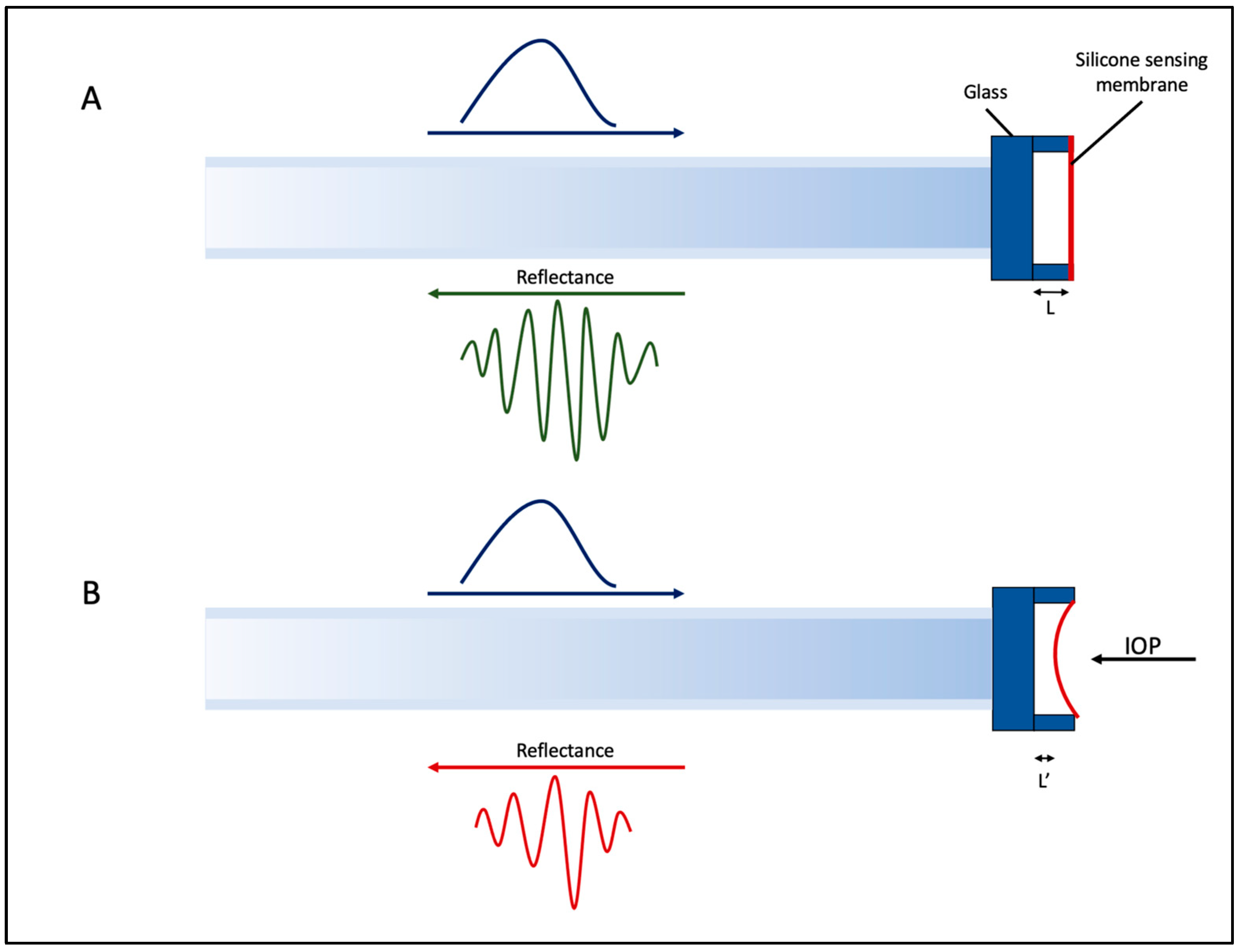
5.3.2. Implantable Fabry–Perot Pressure Sensor for Keratoprosthesis
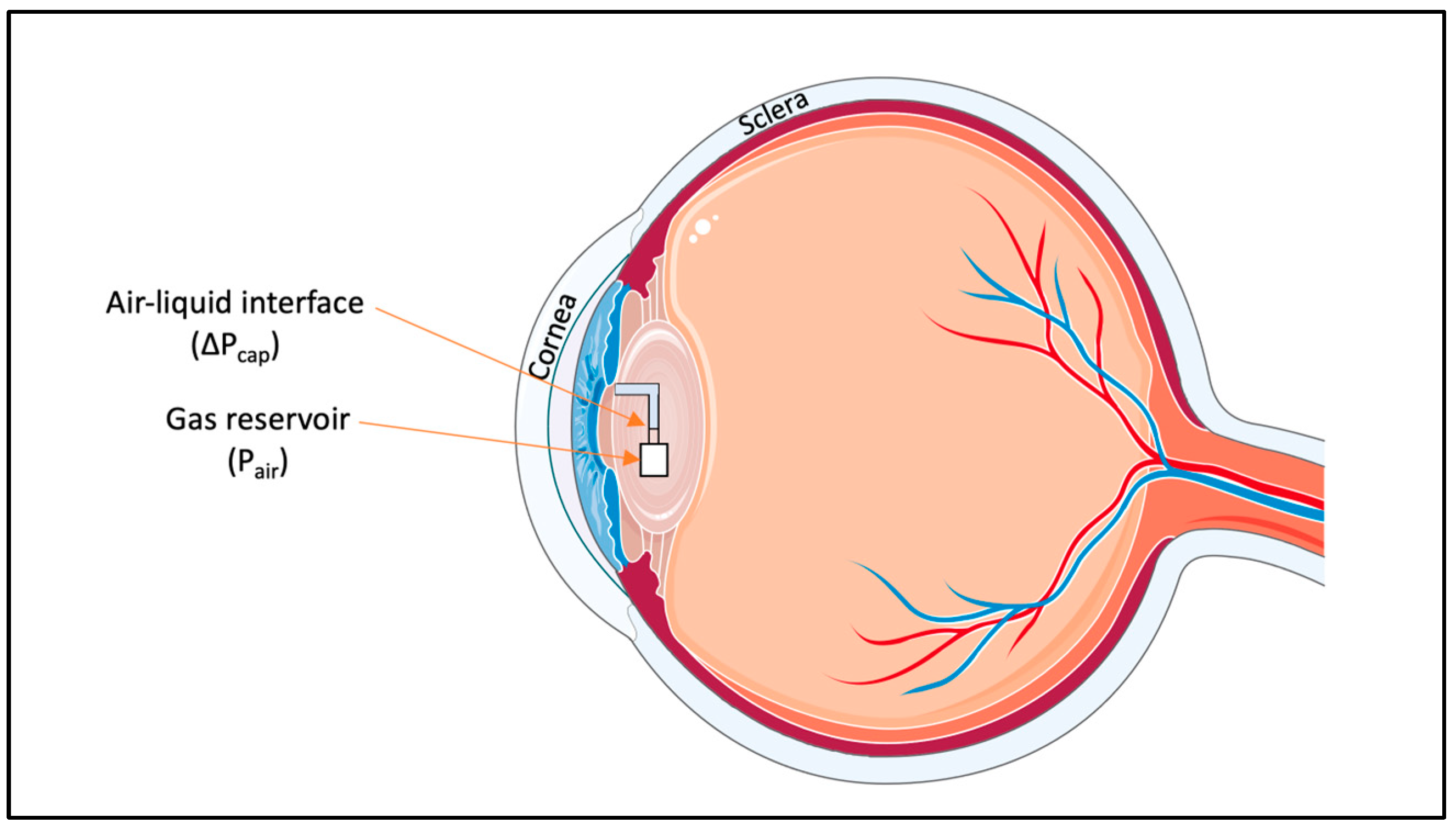
5.3.3. Microfluidic-Implantable Sensors
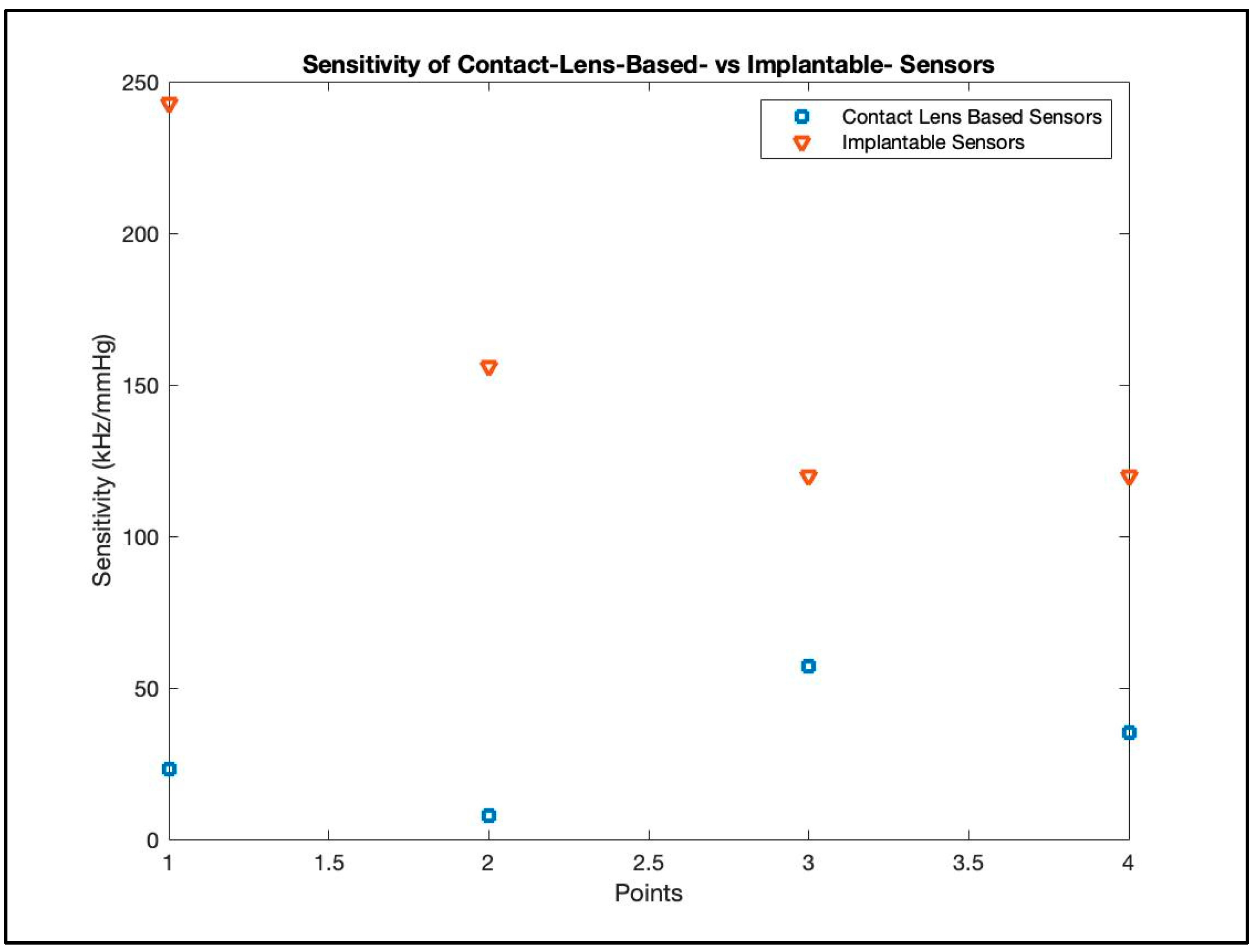
6. Comparison of the Different Sensors
7. Clinical Trials, Commercialization, and Advancements in the Field
7.1. Contact Lens-Based Sensors
7.1.1. Sensimed Triggerfish (Triggerfish CLS, Sensimed AG, Lausanne, Switzerland)
7.1.2. Glakolens Inc.
7.2. Implantable IOP Sensors
7.2.1. EYEMATE, Implandata
7.2.2. IOP Connect (Injectsense, Inc.; Emeryville, CA, USA)
8. Clinical Integration of Advanced IOP Biosensors
8.1. Advantages of Adopting Advanced IOP Biosensors
8.2. Potential Indications of Advanced IOP Biosensors—The “When”
8.3. Integrating IOP Biosensors into Clinical Workflow—The “How”
8.4. Impact on Prognostic Outcomes and Patient Follow-Up—The “What”
8.5. Challenges
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morrison, J.C.; Johnson, E.C.; Cepurna, W.; Jia, L. Understanding Mechanisms of Pressure-Induced Optic Nerve Damage. Prog. Retin. Eye Res. 2005, 24, 217–240. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.S.; Wilson, M.R.; Liebmann, J.M.; Fechtner, R.D.; Weinreb, R.N. An Evidence-Based Assessment of Risk Factors for the Progression of Ocular Hypertension and Glaucoma. Am. J. Ophthalmol. 2004, 138, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, D. Under Pressure: A Review of Normal-Tension Glaucoma. Can. J. Optom. 2012, 74, 33–44. [Google Scholar] [CrossRef]
- Sihota, R.; Angmo, D.; Ramaswamy, D.; Dada, T. Simplifying “Target” Intraocular Pressure for Different Stages of Primary Open-Angle Glaucoma and Primary Angle-Closure Glaucoma. Indian J. Ophthalmol. 2018, 66, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Hollows, F.C.; Graham, P.A. Intra-Ocular Pressure, Glaucoma, and Glaucoma Suspects in a Defined Population. Br. J. Ophthalmol. 1966, 50, 570–586. [Google Scholar] [CrossRef]
- Bonomi, L.; Marchini, G.; Marraffa, M.; Morbio, R. The Relationship between Intraocular Pressure and Glaucoma in a Defined Population: Data from the Egna-Neumarkt Glaucoma Study. Ophthalmologica 2000, 215, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Noecker, R.J. The Management of Glaucoma and Intraocular Hypertension: Current Approaches and Recent Advances. Ther. Clin. Risk Manag. 2006, 2, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Havens, S.J.; Ghate, D.A.; Gulati, V. Glaucoma. In Neuroimmune Pharmacology; Ikezu, T., Gendelman, H.E., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 533–552. ISBN 978-3-319-44022-4. [Google Scholar]
- Tham, Y.-C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.-Y. Global Prevalence of Glaucoma and Projections of Glaucoma Burden through 2040: A Systematic Review and Meta-Analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Bourne, R.R.A.; Taylor, H.R.; Flaxman, S.R.; Keeffe, J.; Leasher, J.; Naidoo, K.; Pesudovs, K.; White, R.A.; Wong, T.Y.; Resnikoff, S.; et al. Number of People Blind or Visually Impaired by Glaucoma Worldwide and in World Regions 1990–2010: A Meta-Analysis. PLoS ONE 2016, 11, e0162229. [Google Scholar] [CrossRef]
- Dietze, J.; Blair, K.; Havens, S.J. Glaucoma. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Leske, M.C.; Heijl, A.; Hyman, L.; Bengtsson, B.; Dong, L.; Yang, Z. Predictors of Long-Term Progression in the Early Manifest Glaucoma Trial. Ophthalmology 2007, 114, 1965–1972. [Google Scholar] [CrossRef]
- Primary Open-Angle Glaucoma PPP 2020. Available online: https://www.aao.org/education/preferred-practice-pattern/primary-open-angle-glaucoma-ppp (accessed on 15 August 2023).
- Cho, H.; Kee, C. Population-Based Glaucoma Prevalence Studies in Asians. Surv. Ophthalmol. 2014, 59, 434–447. [Google Scholar] [CrossRef]
- American Academy of Ophthalmology Basic and Clinical Science Course, Section 02: Fundamentals and Principles of Ophthalmology. Available online: https://store.aao.org/basic-and-clinical-science-course-section-02-fundamentals-and-principles-of-ophthalmology.html (accessed on 15 August 2023).
- Johnson, M. What Controls Aqueous Humour Outflow Resistance? Exp. Eye Res. 2006, 82, 545–557. [Google Scholar] [CrossRef] [PubMed]
- 2020–2021 BCSC Basic and Clinical Science CourseTM. Available online: https://www.aao.org/education/bcscsnippetdetail.aspx?id=b879ee48-8b97-4985-a5b9-af8f9125d2c6 (accessed on 4 August 2023).
- Stock, R.A.; Ströher, C.; Sampaio, R.R.; Mergener, R.A.; Bonamigo, E.L. A Comparative Study Between the Goldmann Applanation Tonometer and the Non-Contact Air-Puff Tonometer (Huvitz HNT 7000) in Normal Eyes. Clin. Ophthalmol. 2021, 15, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Zeppieri, M.; Gurnani, B. Applanation Tonometry. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Mark, H.H. Armand Imbert, Adolf Fick, and Their Tonometry Law. Eye 2012, 26, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Stamper, R.L. A History of Intraocular Pressure and Its Measurement. Optom. Vis. Sci. 2011, 88, E16. [Google Scholar] [CrossRef] [PubMed]
- McCafferty, S.J.; Enikov, E.T.; Schwiegerling, J.; Ashley, S.M. Goldmann Tonometry Tear Film Error and Partial Correction with a Shaped Applanation Surface. Clin. Ophthalmol. 2018, 12, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.O.; Beiser, J.A.; Brandt, J.D.; Heuer, D.K.; Higginbotham, E.J.; Johnson, C.A.; Keltner, J.L.; Miller, J.P.; Parrish, R.K., II; Wilson, M.R.; et al. The Ocular Hypertension Treatment Study: Baseline Factors That Predict the Onset of Primary Open-Angle Glaucoma. Arch. Ophthalmol. 2002, 120, 714–720. [Google Scholar] [CrossRef]
- Moseley, M.J.; Evans, N.M.; Fielder, A.R. Comparison of a New Non-Contact Tonometer with Goldmann Applanation. Eye 1989, 3 Pt 3, 332–337. [Google Scholar] [CrossRef]
- Eisenberg, D.L.; Sherman, B.G.; McKeown, C.A.; Schuman, J.S. Tonometry in Adults and Children: A Manometric Evaluation of Pneumatonometry, Applanation, and TonoPen in Vitro and in vivo11The Authors Have No Commercial Interest in Any of the Products Mentioned. Ophthalmology 1998, 105, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Mackay, R.S.; Marg, E. Fast, Automatic, Electronic Tonometers Based on an Exact Theory. Acta Ophthalmol. 1959, 37, 495–507. [Google Scholar] [CrossRef]
- Kapamajian, M.A.; de la Cruz, J.; Hallak, J.A.; Vajaranant, T.S. Correlation Between Corneal and Scleral Pneumatonometry: An Alternative Method for Intraocular Pressure Measurement. Am. J. Ophthalmol. 2013, 156, 902–906.e1. [Google Scholar] [CrossRef] [PubMed]
- Durham, D.G.; Bigliano, R.P.; Masino, J.A. Pneumatic Applanation Tonometer. Trans. Am. Acad. Ophthalmol. Otolaryngol. 1965, 69, 1029–1047. [Google Scholar] [PubMed]
- Medeiros, F.A.; Freitas, D.; Lisboa, R.; Kuang, T.-M.; Zangwill, L.M.; Weinreb, R.N. Corneal Hysteresis as a Risk Factor for Glaucoma Progression: A Prospective Longitudinal Study. Ophthalmology 2013, 120, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Susanna, B.N.; Ogata, N.G.; Daga, F.B.; Susanna, C.N.; Diniz-Filho, A.; Medeiros, F.A. Association between Rates of Visual Field Progression and Intraocular Pressure Measurements Obtained by Different Tonometers. Ophthalmology 2019, 126, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Susanna, C.N.; Diniz-Filho, A.; Daga, F.B.; Susanna, B.N.; Zhu, F.; Ogata, N.G.; Medeiros, F.A. A Prospective Longitudinal Study to Investigate Corneal Hysteresis as a Risk Factor for Predicting Development of Glaucoma. Am. J. Ophthalmol. 2018, 187, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Kontiola, A.I. A New Induction-Based Impact Method for Measuring Intraocular Pressure. Acta Ophthalmol. Scand. 2000, 78, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Kumar, M.; Prakash, B.; Varshney, G. Relationship of Central Corneal Thickness and Intraocular Pressure by iCare Rebound Tonometer. J. Glaucoma 2014, 23, 380. [Google Scholar] [CrossRef]
- Schneider, E.; Grehn, F. Intraocular Pressure Measurement-Comparison of Dynamic Contour Tonometry and Goldmann Applanation Tonometry. J. Glaucoma 2006, 15, 2. [Google Scholar] [CrossRef]
- Kim, J.H.; Caprioli, J. Intraocular Pressure Fluctuation: Is It Important? J. Ophthalmic Vis. Res. 2018, 13, 170–174. [Google Scholar] [CrossRef]
- Gardiner, S.K.; Fortune, B.; Wang, L.; Downs, J.C.; Burgoyne, C.F. Intraocular Pressure Magnitude and Variability as Predictors of Rates of Structural Change in Non-Human Primate Experimental Glaucoma. Exp. Eye Res. 2012, 103, 1–8. [Google Scholar] [CrossRef]
- Strouthidis, N.G.; Fortune, B.; Yang, H.; Sigal, I.A.; Burgoyne, C.F. Effect of Acute Intraocular Pressure Elevation on the Monkey Optic Nerve Head as Detected by Spectral Domain Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2011, 52, 9431–9437. [Google Scholar] [CrossRef]
- Fortune, B.; Choe, T.E.; Reynaud, J.; Hardin, C.; Cull, G.A.; Burgoyne, C.F.; Wang, L. Deformation of the Rodent Optic Nerve Head and Peripapillary Structures during Acute Intraocular Pressure Elevation. Investig. Ophthalmol. Vis. Sci. 2011, 52, 6651–6661. [Google Scholar] [CrossRef] [PubMed]
- Choh, V.; Gurdita, A.; Tan, B.; Prasad, R.C.; Bizheva, K.; Joos, K.M. Short-Term Moderately Elevated Intraocular Pressure Is Associated With Elevated Scotopic Electroretinogram Responses. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2140–2151. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kim, S.H.; Lee, E.J.; Han, J.C.; Sohn, S.W.; Rhee, T.; Kee, C. The Effect of Diurnal Fluctuation in Intraocular Pressure on the Evaluation of Risk Factors of Progression in Normal Tension Glaucoma. PLoS ONE 2016, 11, e0164876. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, K.; Ishida, K.; Sawada, A.; Kawase, K.; Yamamoto, T. Diurnal Variation of Intraocular Pressure in Suspected Normal-Tension Glaucoma. Jpn. J. Ophthalmol. 2006, 50, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Renard, E.; Palombi, K.; Gronfier, C.; Pepin, J.-L.; Noel, C.; Chiquet, C.; Romanet, J.-P. Twenty-Four Hour (Nyctohemeral) Rhythm of Intraocular Pressure and Ocular Perfusion Pressure in Normal-Tension Glaucoma. Investig. Ophthalmol. Vis. Sci. 2010, 51, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, B.; Heijl, A. Diurnal IOP Fluctuation: Not an Independent Risk Factor for Glaucomatous Visual Field Loss in High-Risk Ocular Hypertension. Graefes Arch. Clin. Exp. Ophthalmol. 2005, 243, 513–518. [Google Scholar] [CrossRef]
- De Moraes, C.G.; Jasien, J.V.; Simon-Zoula, S.; Liebmann, J.M.; Ritch, R. Visual Field Change and 24-Hour IOP-Related Profile with a Contact Lens Sensor in Treated Glaucoma Patients. Ophthalmology 2016, 123, 744–753. [Google Scholar] [CrossRef]
- Choi, J.; Kook, M.S. Systemic and Ocular Hemodynamic Risk Factors in Glaucoma. Biomed. Res. Int. 2015, 2015, 141905. [Google Scholar] [CrossRef]
- Tojo, N.; Abe, S.; Miyakoshi, M.; Hayashi, A. Correlation between Short-Term and Long-Term Intraocular Pressure Fluctuation in Glaucoma Patients. Clin. Ophthalmol. 2016, 10, 1713–1717. [Google Scholar] [CrossRef]
- Nouri-Mahdavi, K.; Hoffman, D.; Coleman, A.L.; Liu, G.; Li, G.; Gaasterland, D.; Caprioli, J.; Advanced Glaucoma Intervention Study. Predictive Factors for Glaucomatous Visual Field Progression in the Advanced Glaucoma Intervention Study. Ophthalmology 2004, 111, 1627–1635. [Google Scholar] [CrossRef] [PubMed]
- Caprioli, J.; Coleman, A.L. Intraocular Pressure Fluctuation a Risk Factor for Visual Field Progression at Low Intraocular Pressures in the Advanced Glaucoma Intervention Study. Ophthalmology 2008, 115, 1123–1129.e3. [Google Scholar] [CrossRef] [PubMed]
- Musch, D.C.; Gillespie, B.W.; Lichter, P.R.; Niziol, L.M.; Janz, N.K. Visual Field Progression in the Collaborative Initial Glaucoma Treatment Study: The Impact of Treatment and Other Baseline Factors. Ophthalmology 2009, 116, 200–207. [Google Scholar] [CrossRef]
- Musch, D.; Gillespie, B.; Niziol, L.; Lichter, P.; Varma, R. Intraocular Pressure Control and Long-Term Visual Field Loss in the Collaborative Initial Glaucoma Treatment Study. Ophthalmology 2011, 118, 1766–1773. [Google Scholar] [CrossRef] [PubMed]
- Fujino, Y.; Asaoka, R.; Murata, H.; Miki, A.; Tanito, M.; Mizoue, S.; Mori, K.; Suzuki, K.; Yamashita, T.; Kashiwagi, K.; et al. Evaluation of Glaucoma Progression in Large-Scale Clinical Data: The Japanese Archive of Multicentral Databases in Glaucoma (JAMDIG). Investig. Ophthalmol. Vis. Sci. 2016, 57, 2012–2020. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.C.; Kolker, A.E.; Sharpe, E.D.; Day, D.G.; Holmes, K.T.; Leech, J.N.; Johnson, M.; Cantrell, J.B. Factors Associated with Long-Term Progression or Stability in Primary Open-Angle Glaucoma. Am. J. Ophthalmol. 2000, 130, 274–279. [Google Scholar] [CrossRef]
- Hong, S.; Seong, G.J.; Hong, Y.J. Long-Term Intraocular Pressure Fluctuation and Progressive Visual Field Deterioration in Patients with Glaucoma and Low Intraocular Pressures after a Triple Procedure. Arch. Ophthalmol. 2007, 125, 1010–1013. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.P.; Walt, J.W.; Rosenblatt, L.C.; Siegartel, L.R.; Stern, L.S.; Glaucoma Care Study Group. Association between Intraocular Pressure Variation and Glaucoma Progression: Data from a United States Chart Review. Am. J. Ophthalmol. 2007, 144, 901–907. [Google Scholar] [CrossRef]
- Asrani, S.; Zeimer, R.; Wilensky, J.; Gieser, D.; Vitale, S.; Lindenmuth, K. Large Diurnal Fluctuations in Intraocular Pressure Are an Independent Risk Factor in Patients with Glaucoma. J. Glaucoma 2000, 9, 134–142. [Google Scholar] [CrossRef]
- The Advanced Glaucoma Intervention Study (AGIS): 7. The Relationship between Control of Intraocular Pressure and Visual Field Deterioration.The AGIS Investigators. Am. J. Ophthalmol. 2000, 130, 429–440. [CrossRef]
- Bengtsson, B.; Leske, M.C.; Hyman, L.; Heijl, A.; Early Manifest Glaucoma Trial Group. Fluctuation of Intraocular Pressure and Glaucoma Progression in the Early Manifest Glaucoma Trial. Ophthalmology 2007, 114, 205–209. [Google Scholar] [CrossRef]
- Kass, M.A.; Heuer, D.K.; Higginbotham, E.J.; Johnson, C.A.; Keltner, J.L.; Miller, J.P.; Parrish, R.K.; Wilson, M.R.; Gordon, M.O. The Ocular Hypertension Treatment Study: A Randomized Trial Determines That Topical Ocular Hypotensive Medication Delays or Prevents the Onset of Primary Open-Angle Glaucoma. Arch. Ophthalmol. 2002, 120, 701–713; discussion 829–830 . [Google Scholar] [CrossRef] [PubMed]
- De Moraes, C.G.V.; Juthani, V.J.; Liebmann, J.M.; Teng, C.C.; Tello, C.; Susanna, R.; Ritch, R. Risk Factors for Visual Field Progression in Treated Glaucoma. Arch. Ophthalmol. 2011, 129, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, F.A.; Weinreb, R.N.; Zangwill, L.M.; Alencar, L.M.; Sample, P.A.; Vasile, C.; Bowd, C. Long-Term Intraocular Pressure Fluctuations and Risk of Conversion from Ocular Hypertension to Glaucoma. Ophthalmology 2008, 115, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Campigotto, A.; Campbell, R.J.; Lai, Y. Correlation between Corneal and Contact Lens Deformation with Changes in Intraocular Pressure for Wearable Monitoring Systems. Eye 2023, 37, 2055–2060. [Google Scholar] [CrossRef]
- Bukhari, S.A.R.; Afrin, T.; Floras, C.; Lai, Y. Contact Lens-Based Intraocular Pressure Sensor. In Proceedings of the IECB 2023, MDPI, online, 8–21 May 2023; p. 15. [Google Scholar]
- Blackburn, B.J.; Jenkins, M.W.; Rollins, A.M.; Dupps, W.J. A Review of Structural and Biomechanical Changes in the Cornea in Aging, Disease, and Photochemical Crosslinking. Front. Bioeng. Biotechnol. 2019, 7, 66. [Google Scholar] [CrossRef] [PubMed]
- Campigotto, A.; Ralhan, A.; Helgason, R.; Campbell, R.J.; Lai, Y. Effect of Variations of Corneal Physiology on Novel Non-Invasive Intraocular Pressure Monitoring Soft Contact Lens. Biomed. Microdevices 2021, 23, 16. [Google Scholar] [CrossRef]
- Agaoglu, S.; Diep, P.; Martini, M.; Kt, S.; Baday, M.; Araci, I.E. Ultra-Sensitive Microfluidic Wearable Strain Sensor for Intraocular Pressure Monitoring. Lab. Chip 2018, 18, 3471–3483. [Google Scholar] [CrossRef]
- An, H.; Chen, L.; Liu, X.; Zhao, B.; Zhang, H.; Wu, Z. Microfluidic Contact Lenses for Unpowered, Continuous and Non-Invasive Intraocular Pressure Monitoring. Sens. Actuators A Phys. 2019, 295, 177–187. [Google Scholar] [CrossRef]
- Campigotto, A.; Leahy, S.; Zhao, G.; Campbell, R.J.; Lai, Y. Non-Invasive Intraocular Pressure Monitoring with Contact Lens. Br. J. Ophthalmol. 2019, 104, 1324–1328. [Google Scholar] [CrossRef]
- Campigotto, A.; Lai, Y. A Novel Non-invasive Wearable Sensor for Intraocular Pressure Measurement. Med. Devices Sens. 2020, 3, e10086. [Google Scholar] [CrossRef]
- Yang, W.; Zhang, X.; Wang, Y.; Fan, Q.; Zhang, S.; Chen, Y.; Shen, X.; Xie, M.; Duan, X. Notched-Ring Structured Microfluidic Contact Lens for Intraocular Pressure Monitoring. Appl. Phys. Lett. 2021, 119, 193701. [Google Scholar] [CrossRef]
- Yuan, M.; Liu, Z.; Wu, X.; Gou, H.; Zhang, Y.; Ning, X.; Li, W.; Yao, Z.; Wang, Y.; Pei, W.; et al. High-Sensitive Microfluidic Contact Lens Sensor for Intraocular Pressure Visualized Monitoring. Sens. Actuators A Phys. 2023, 354, 114250. [Google Scholar] [CrossRef]
- Leonardi, M.; Leuenberger, P.; Bertrand, D.; Bertsch, A.; Renaud, P. First Steps toward Noninvasive Intraocular Pressure Monitoring with a Sensing Contact Lens. Investig. Ophthalmol. Vis. Sci. 2004, 45, 3113. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, M.; Leuenberger, P.; Bertrand, D.; Bertsch, A.; Renaud, P. A Soft Contact Lens with a MEMS Strain Gage Embedded for Intraocular Pressure Monitoring. In Proceedings of the TRANSDUCERS ’03 12th International Conference on Solid-State Sensors, Actuators and Microsystems. Digest of Technical Papers (Cat. No.03TH8664), Boston, MA, USA, 8–12 June 2003; IEEE: Boston, MA, USA, 2003; Volume 2, pp. 1043–1046. [Google Scholar]
- Araci, I.E.; Agaoglu, S.; Baday, M.; Pricilla, D. Closed Microfluidic Network for Strain Sensing Embedded in a Contact Lens to Monitor Intraocular Pressure. U.S. Patent No. 10,898,074, 26 January 2021. [Google Scholar]
- Sun, Y.; Wang, Y.; Liu, Y.; Wu, S.; Zhang, S.; Niu, W. Biomimetic Chromotropic Photonic-Ionic Skin with Robust Resilience, Adhesion, and Stability. Adv. Funct. Mater. 2022, 32, 2204467. [Google Scholar] [CrossRef]
- Cao, X.; Du, Y.; Guo, Y.; Hu, G.; Zhang, M.; Wang, L.; Zhou, J.; Gao, Q.; Fischer, P.; Wang, J.; et al. Replicating the Cynandra Opis Butterfly’s Structural Color for Bioinspired Bigrating Color Filters. Adv. Mater. 2022, 34, 2109161. [Google Scholar] [CrossRef]
- Xue, P.; Chen, Y.; Xu, Y.; Valenzuela, C.; Zhang, X.; Bisoyi, H.K.; Yang, X.; Wang, L.; Xu, X.; Li, Q. Bioinspired MXene-Based Soft Actuators Exhibiting Angle-Independent Structural Color. Nano-Micro Lett. 2023, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Tian, H.; Liu, T.; Liu, H.; Zhao, F.; Li, X.; Wang, C.; Chen, X.; Shao, J. Chameleon-Inspired Active Tunable Structural Color Based on Smart Skin with Multi-Functions of Structural Color, Sensing and Actuation. Mater. Horiz. 2023, 10, 2024–2034. [Google Scholar] [CrossRef]
- Hou, X.; Li, F.; Song, Y.; Li, M. Recent Progress in Responsive Structural Color. J. Phys. Chem. Lett. 2022, 13, 2885–2900. [Google Scholar] [CrossRef]
- Xie, Z.; Li, L.; Liu, P.; Zheng, F.; Guo, L.; Zhao, Y.; Jin, L.; Li, T.; Gu, Z. Self-Assembled Coffee-Ring Colloidal Crystals for Structurally Colored Contact Lenses. Small 2015, 11, 926–930. [Google Scholar] [CrossRef]
- Ren, X.; Zhou, Y.; Lu, F.; Zhai, L.; Wu, H.; Chen, Z.; Wang, C.; Zhu, X.; Xie, Y.; Cai, P.; et al. Contact Lens Sensor with Anti-Jamming Capability and High Sensitivity for Intraocular Pressure Monitoring. ACS Sens. 2023, 8, 2691–2701. [Google Scholar] [CrossRef] [PubMed]
- Maeng, B.; Chang, H.; Park, J. Photonic Crystal-Based Smart Contact Lens for Continuous Intraocular Pressure Monitoring. Lab. Chip 2020, 20, 1740–1750. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Ge, Y.; Zhang, Q.; Yuan, M.; Cai, Y.; Li, K.; Li, Y.; Xie, R.; Xu, C.; Jiang, D.; et al. Smart Contact Lens with Dual-Sensing Platform for Monitoring Intraocular Pressure and Matrix Metalloproteinase-9. Adv. Sci. 2022, 9, 2104738. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhao, Q.; Du, X. Structurally Coloured Contact Lens Sensor for Point-of-Care Ophthalmic Health Monitoring. J. Mater. Chem. B 2020, 8, 3519–3526. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Wu, S.-T.; Lei, X.-Q.; Han, X.-L.; Chen, P.; Ding, S.-N. Novel SiO2 Photonic Crystal Microspheres as Inorganic Pigments for Structural Color Contact Lenses. Opt. Mater. 2023, 138, 113705. [Google Scholar] [CrossRef]
- Ziai, Y.; Petronella, F.; Rinoldi, C.; Nakielski, P.; Zakrzewska, A.; Kowalewski, T.A.; Augustyniak, W.; Li, X.; Calogero, A.; Sabała, I.; et al. Chameleon-Inspired Multifunctional Plasmonic Nanoplatforms for Biosensing Applications. NPG Asia Mater. 2022, 14, 18. [Google Scholar] [CrossRef]
- Panfilova, E.V.; Mozer, K.V.; Ibragimov, A.R. The Formation of a Sensitive Structure of a Contact Lens Sensor. J. Phys. Conf. Ser. 2020, 1571, 012005. [Google Scholar] [CrossRef]
- Moreddu, R.; Vigolo, D.; Yetisen, A.K. Contact Lens Technology: From Fundamentals to Applications. Adv. Healthc. Mater. 2019, 8, 1900368. [Google Scholar] [CrossRef]
- Wang, X.; Wang, Y.; Lu, C.; Zhang, J.; Qiu, W.; Yang, S.; Lin, N.; Zhang, Y.; Liu, X.Y. Chameleon-Inspired Flexible Photonic Crystal Lens-Shaped Dynamic Pressure Sensor Based on Structural Color Shift. Cell Rep. Phys. Sci. 2023, 4, 101490. [Google Scholar] [CrossRef]
- Sahay, P.; Rao, A.; Padhy, D.; Sarangi, S.; Das, G.; Reddy, M.M.; Modak, R. Functional Activity of Matrix Metalloproteinases 2 and 9 in Tears of Patients With Glaucoma. Investig. Ophthalmol. Vis. Sci. 2017, 58, BIO106–BIO113. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.Y.; Shin, S.; Choi, H.; Jeong, S.H.; Myung, D.; Hahn, S.K. Smart Contact Lenses with a Transparent Silver Nanowire Strain Sensor for Continuous Intraocular Pressure Monitoring. ACS Appl. Bio Mater. 2021, 4, 4532–4541. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Tu, H.; Zhao, H.; Wei, F.; Yang, Y.; Ren, T. A Wearable Contact Lens Sensor for Noninvasive In-Situ Monitoring of Intraocular Pressure. Nanotechnology 2021, 32, 095106. [Google Scholar] [CrossRef] [PubMed]
- Pang, Y.; Li, Y.; Wang, X.; Qi, C.; Yang, Y.; Ren, T.-L. A Contact Lens Promising for Non-Invasive Continuous Intraocular Pressure Monitoring. RSC Adv. 2019, 9, 5076–5082. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wang, G.; Pei, W.; Wei, C.; Wu, X.; Dou, Z.; Li, Y.; Wang, Y.; Chen, H. Application of Graphene Nanowalls in an Intraocular Pressure Sensor. J. Mater. Chem. B 2020, 8, 8794–8802. [Google Scholar] [CrossRef]
- Helgason, R.; Lai, Y. Increased Sensitivity of Smart Contact Lenses for Continuous Intraocular Pressure Measurement Using Ring-Shaped Design. Flex. Print. Electron. 2022, 7, 024005. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Man, T.; Huang, D.; Li, X.; Zhu, H.; Li, Z. High Resolution Non-Invasive Intraocular Pressure Monitoring by Use of Graphene Woven Fabrics on Contact Lens. Microsyst. Nanoeng. 2019, 5, 39. [Google Scholar] [CrossRef]
- Zhu, H.; Yang, H.; Zhan, L.; Chen, Y.; Wang, J.; Xu, F. Hydrogel-Based Smart Contact Lens for Highly Sensitive Wireless Intraocular Pressure Monitoring. ACS Sens. 2022, 7, 3014–3022. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.-Y.; Jou, J.-J.; Tseng, C.-L.; Yang, C.-L.; Chen, T.-Y.; Shih, T.-T. Design and Analysis of Wireless Passive LC Sensor Prototypes for Intraocular Pressure Monitoring. In Proceedings of the 2023 9th International Conference on Applied System Innovation (ICASI), Chiba, Japan, 21 April 2023; IEEE: Chiba, Japan, 2023; pp. 169–171. [Google Scholar]
- Kouhani, M.H.M.; Wu, J.; Tavakoli, A.; Weber, A.J.; Li, W. Wireless, Passive Strain Sensor in a Doughnut-Shaped Contact Lens for Continuous Non-Invasive Self-Monitoring of Intraocular Pressure. Lab. Chip 2020, 20, 332–342. [Google Scholar] [CrossRef] [PubMed]
- An, H.; Chen, L.; Liu, X.; Wang, X.; Liu, Y.; Wu, Z.; Zhao, B.; Zhang, H. High-Sensitivity Liquid-Metal-Based Contact Lens Sensor for Continuous Intraocular Pressure Monitoring. J. Micromech. Microeng. 2021, 31, 035006. [Google Scholar] [CrossRef]
- Karunaratne, I.K.; Lee, C.H.C.; Or, P.W.; Wei, Y.; Chong, I.T.; Yang, Y.; Yu, M.; Lam, D.C.C. Wearable Dual-Element Intraocular Pressure Contact Lens Sensor. Sens. Actuators A Phys. 2021, 321, 112580. [Google Scholar] [CrossRef]
- Zolfaghari, P.; Yalcinkaya, A.D.; Ferhanoglu, O. Smart Glasses to Monitor Intraocular Pressure Using Optical Triangulation. Opt. Commun. 2023, 546, 129752. [Google Scholar] [CrossRef]
- Zolfaghari, P.; Yalcinkaya, A.D.; Ferhanoglu, O. MEMS Sensor-Glasses Pair for Real-Time Monitoring of Intraocular Pressure. IEEE Photonics Technol. Lett. 2023, 35, 887–890. [Google Scholar] [CrossRef]
- Agarwal, A.; Shapero, A.; Rodger, D.; Humayun, M.; Tai, Y.-C.; Emami, A. A Wireless, Low-Drift, Implantable Intraocular Pressure Sensor with Parylene-on-Oil Encapsulation. In Proceedings of the 2018 IEEE Custom Integrated Circuits Conference (CICC), San Diego, CA, USA, 8–11 April 2018; IEEE: San Diego, CA, USA, 2018; pp. 1–4. [Google Scholar]
- Goins, K.M.; Kitzmann, A.S.; Greiner, M.A.; Kwon, Y.H.; Alward, W.L.M.; Ledolter, J.; Wagoner, M.D. Boston Type 1 Keratoprosthesis: Visual Outcomes, Device Retention, and Complications. Cornea 2016, 35, 1165–1174. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.A.; Manz, S.N.; Shen, L.Q. Glaucoma Management in Patients with Penetrating Keratoplasty or Keratoprosthesis. Curr. Opin. Ophthalmol. 2023, 34, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Enders, P.; Hall, J.; Bornhauser, M.; Mansouri, K.; Altay, L.; Schrader, S.; Dietlein, T.S.; Bachmann, B.O.; Neuhann, T.; Cursiefen, C. Telemetric Intraocular Pressure Monitoring after Boston Keratoprosthesis Surgery Using the Eyemate-IO Sensor: Dynamics in the First Year. Am. J. Ophthalmol. 2019, 206, 256–263. [Google Scholar] [CrossRef]
- Hui, P.; Shtyrkova, K.; Zhou, C.; Chen, X.; Chodosh, J.; Dohlman, C.H.; Paschalis, E.I. Implantable Self-aligning Fiber-optic Optomechanical Devices for in Vivo Intraocular Pressure-sensing in Artificial Cornea. J. Biophotonics 2020, 13, e202000031. [Google Scholar] [CrossRef]
- Araci, I.E.; Su, B.; Quake, S.R.; Mandel, Y. An Implantable Microfluidic Device for Self-Monitoring of Intraocular Pressure. Nat. Med. 2014, 20, 1074–1078. [Google Scholar] [CrossRef]
- Yan, J. An Unpowered, Wireless Contact Lens Pressure Sensor for Point-of-Care Glaucoma Diagnosis. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; IEEE: Boston, MA, USA, 2011; pp. 2522–2525. [Google Scholar]
- Xu, X.; Liu, Z.; Wang, L.; Huang, Y.; Yang, H. High–Accuracy Film–Integrated Optical Sensor for Real–Time Intraocular Pressure Monitoring. Micromachines 2023, 14, 353. [Google Scholar] [CrossRef] [PubMed]
- Shaker, L.M.; Al-Amiery, A.; Takriff, M.S.; Wan Isahak, W.N.R.; Mahdi, A.S.; Al-Azzawi, W.K. The Future of Vision: A Review of Electronic Contact Lenses Technology. ACS Photonics 2023, 10, 1671–1686. [Google Scholar] [CrossRef]
- Dunbar, G.E.; Shen, B.; Aref, A. The Sensimed Triggerfish Contact Lens Sensor: Efficacy, Safety, and Patient Perspectives. OPTH 2017, 11, 875–882. [Google Scholar] [CrossRef]
- FDA Permits Marketing of Device That Senses Optimal Time to Check Patient’s Eye Pressure. Available online: https://www.fda.gov/news-events/press-announcements/fda-permits-marketing-device-senses-optimal-time-check-patients-eye-pressure (accessed on 28 August 2023).
- Chen, X.; Wu, X.; Lin, X.; Wang, J.; Xu, W. Outcome, Influence Factor and Development of CLS Measurement in Continuous IOP Monitoring: A Narrative Review. Contact Lens Anterior Eye 2021, 44, 101376. [Google Scholar] [CrossRef]
- Tan, S.; Yu, M.; Baig, N.; Chan, P.P.; Tang, F.Y.; Cheung, C.Y.; Tham, C.C.Y. Association of Ultra-Short-Term Intraocular Pressure Fluctuation With Disease Progression in Primary Angle Closure Glaucoma: The CUPAL Study. J. Glaucoma 2022, 31, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, K.; Liu, J.H.K.; Weinreb, R.N.; Tafreshi, A.; Medeiros, F.A. Analysis of Continuous 24-Hour Intraocular Pressure Patterns in Glaucoma. Investig. Ophthalmol. Vis. Sci. 2012, 53, 8050. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rabensteiner, D.F.; Rabensteiner, J.; Faschinger, C. The Influence of Electromagnetic Radiation on the Measurement Behaviour of the Triggerfish® Contact Lens Sensor. BMC Ophthalmol. 2018, 18, 338. [Google Scholar] [CrossRef] [PubMed]
- Hoban, K.; Peden, R.; Megaw, R.; Halpin, P.; Tatham, A.J. 24-Hour Contact Lens Sensor Monitoring of Intraocular Pressure-Related Profiles in Normal-Tension Glaucoma and Rates of Disease Progression. Ophthalmic Res. 2017, 57, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Tojo, N.; Hayashi, A.; Otsuka, M. Correlation between 24-h Continuous Intraocular Pressure Measurement with a Contact Lens Sensor and Visual Field Progression. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 175–182. [Google Scholar] [CrossRef]
- Gillmann, K.; Weinreb, R.N.; Mansouri, K. The Effect of Daily Life Activities on Intraocular Pressure Related Variations in Open-Angle Glaucoma. Sci. Rep. 2021, 11, 6598. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.H.; Tsai, J.C. Telehealth and Screening Strategies in the Diagnosis and Management of Glaucoma. J. Clin. Med. 2021, 10, 3452. [Google Scholar] [CrossRef]
- Yadav, M.; Tanwar, M. Impact of COVID-19 on Glaucoma Management: A Review. Front. Ophthalmol. 2022, 2, 1003653. [Google Scholar] [CrossRef]
- Koutsonas, A.; Walter, P.; Roessler, G.; Plange, N. Implantation of a Novel Telemetric Intraocular Pressure Sensor in Patients With Glaucoma (ARGOS Study): 1-Year Results. Investig. Ophthalmol. Vis. Sci. 2015, 56, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Choritz, L.; Mansouri, K.; Van Den Bosch, J.; Weigel, M.; Dick, H.B.; Wagner, M.; Thieme, H.; Thieme, H.; Rüfer, F.; Szurmann, P.; et al. Telemetric Measurement of Intraocular Pressure via an Implantable Pressure Sensor—12-Month Results from the ARGOS-02 Trial. Am. J. Ophthalmol. 2020, 209, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Szurman, P.; Mansouri, K.; Dick, H.B.; Mermoud, A.; Hoffmann, E.M.; Mackert, M.; Weinreb, R.N.; Rao, H.L.; Seuthe, A.-M. Safety and Performance of a Suprachoroidal Sensor for Telemetric Measurement of Intraocular Pressure in the EYEMATE-SC Trial. Br. J. Ophthalmol. 2023, 107, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, I.; Plange, N.; Walter, P.; Koutsonas, A. Telemetric Non-Contact Intraocular Pressure Monitoring with an Implanted Sensor in Patients with Glaucoma: Long-Term Safety Report and Monitoring Data. Br. J. Ophthalmol. 2023, 107, 1098–1103. [Google Scholar] [CrossRef]
- Koutsonas, A.; Walter, P.; Roessler, G.; Plange, N. Long-Term Follow-up after Implantation of a Telemetric Intraocular Pressure Sensor in Patients with Glaucoma: A Safety Report: Long-Term Ocular Pressure Sensor Follow-Up. Clin. Experiment. Ophthalmol. 2018, 46, 473–479. [Google Scholar] [CrossRef]
- Enders, P.; Cursiefen, C. Device Profile of the EYEMATE-IOTM System for Intraocular Pressure Monitoring: Overview of Its Safety and Efficacy. Expert. Rev. Med. Devices 2020, 17, 491–497. [Google Scholar] [CrossRef]
- Enders, P.; Hall, J.; Bornhauser, M.; Mansouri, K.; Altay, L.; Schrader, S.; Dietlein, T.S.; Bachmann, B.O.; Neuhann, T.; Cursiefen, C. Telemetric Intraocular Pressure Monitoring after Boston Keratoprosthesis Surgery. Ophthalmology 2019, 126, 322–324. [Google Scholar] [CrossRef] [PubMed]
- Todani, A.; Behlau, I.; Fava, M.A.; Cade, F.; Cherfan, D.G.; Zakka, F.R.; Jakobiec, F.A.; Gao, Y.; Dohlman, C.H.; Melki, S.A. Intraocular Pressure Measurement by Radio Wave Telemetry. Investig. Ophthalmol. Vis. Sci. 2011, 52, 9573. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, K.; Gillmann, K.; Rao, H.L.; Weinreb, R.N. Weekly and Seasonal Changes of Intraocular Pressure Measured with an Implanted Intraocular Telemetry Sensor. Br. J. Ophthalmol. 2021, 105, 387–391. [Google Scholar] [CrossRef]
- Mariacher, S.; Ebner, M.; Januschowski, K.; Hurst, J.; Schnichels, S.; Szurman, P. Investigation of a Novel Implantable Suprachoroidal Pressure Transducer for Telemetric Intraocular Pressure Monitoring. Exp. Eye Res. 2016, 151, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Szurman, P.; Gillmann, K.; Seuthe, A.-M.; Dick, H.B.; Hoffmann, E.M.; Mermoud, A.; Mackert, M.J.; Weinreb, R.N.; Rao, H.L.; Mansouri, K.; et al. EYEMATE-SC Trial: Twelve-Month Safety, Performance, and Accuracy of a Suprachoroidal Sensor for Telemetric Measurement of Intraocular Pressure. Ophthalmology 2023, 130, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Injectsense Receives Breakthrough Device Program Designation from FDA, Highlights Eye Sensor Performance and Path to Human Studies. Available online: https://www.medical-xprt.com/news/injectsense-receives-breakthrough-device-program-designation-from-fda-highlights-eye-sensor-performa-1070333 (accessed on 27 August 2023).
- Cao, A.; Malaret, E. Methods and Devices for Implantation of Intraocular Pressure Sensors. U.S. Patent 11,202,568, 21 December 2021. [Google Scholar]
- Liu, J.H.K.; Weinreb, R.N. Monitoring Intraocular Pressure for 24 h. Br. J. Ophthalmol. 2011, 95, 599–600. [Google Scholar] [CrossRef] [PubMed]
- Ricur, G.; Reyes, J.; Alfonso, E.; Marino, R.G. Surfing the COVID-19 Tsunami with Teleophthalmology: The Advent of New Models of Eye Care. Curr. Ophthalmol. Rep. 2023, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Baughman, B.D.; Hansemann, B.K.; Shah, M.M.; Weizer, J.S. Drive-through Intraocular Pressure Checks During the COVID-19 Pandemic. J. Glaucoma 2021, 30, 223. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, K.; Kersten-Gomez, I.; Hoffmann, E.M.; Szurman, P.; Choritz, L.; Weinreb, R.N. Intraocular Pressure Telemetry for Managing Glaucoma during the COVID-19 Pandemic. Ophthalmol. Glaucoma 2021, 4, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Alawa, K.A.; Sales, C.S. Alleviating an Increasingly Burdened Healthcare System with Telemedicine: Anterior Segment. Ophthalmol. Ther. 2021, 10, 225–229. [Google Scholar] [CrossRef]
- Al-Nosairy, K.O.; van den Bosch, J.J.O.N.; Pennisi, V.; Mansouri, K.; Thieme, H.; Choritz, L.; Hoffmann, M.B. Use of a Novel Telemetric Sensor to Study Interactions of Intraocular Pressure and Ganglion-Cell Function in Glaucoma. Br. J. Ophthalmol. 2021, 105, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Bhartiya, S.; Gangwani, M.; Kalra, R.B.; Aggarwal, A.; Gagrani, M.; Sirish, K.N. 24-Hour Intraocular Pressure Monitoring: The Way Ahead. Rom. J. Ophthalmol. 2019, 63, 315–320. [Google Scholar] [CrossRef]
- Huang, S.-K.; Ishii, M.; Mizuki, Y.; Kawagoe, T.; Takeuchi, M.; Nomura, E.; Mizuki, N. Circadian Fluctuation Changes in Intraocular Pressure Measured Using a Contact Lens Sensor in Patients with Glaucoma after the Adjunctive Administration of Ripasudil: A Prospective Study. J. Pers. Med. 2023, 13, 800. [Google Scholar] [CrossRef]
- Dubey, S.; Mittal, D.; Mukherjee, S.; Bhoot, M.; Gupta, Y.P. Relationship between Nocturnal Intraocular Pressure-Related Peak Recorded by Contact Lens Sensor and Disease Progression in Treated Glaucomatous Eyes. Indian J. Ophthalmol. 2020, 68, 2427. [Google Scholar] [CrossRef]
- Gaboriau, T.; Dubois, R.; Foucque, B.; Malet, F.; Schweitzer, C. 24-Hour Monitoring of Intraocular Pressure Fluctuations Using a Contact Lens Sensor: Diagnostic Performance for Glaucoma Progression. Investig. Ophthalmol. Vis. Sci. 2023, 64, 3. [Google Scholar] [CrossRef]
- Sharma, R. 24 Hour IOP Diurnal Variation Analysis with Contact Lens Sensor (Triggerfish)-Potential Benefits, Limitations & Future Challenges. Investig. Ophthalmol. Vis. Sci. 2022, 63, 153-A0346. [Google Scholar]
- Zhang, Y.; Wei, Y.; Karunaratne, I.K.; Lee, C.H.C.; Deng, M.; Chen, Z.; Yang, Y.; Chong, I.T.; Lam, D.C.C.; Yu, M. A New Contact Lens Sensor System for Continuous Intraocular Pressure Monitoring: Evaluation of Safety and Tolerability. Eye Contact Lens 2022, 48, 439. [Google Scholar] [CrossRef] [PubMed]
- Tojo, N.; Hayashi, A. Twenty-Four-Hour Intraocular Pressure Indicators Distinguish Normal Tension Glaucoma From Healthy Eyes Measured With a Contact Lens Sensor. J. Glaucoma 2022, 31, 639. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, S.; Li, J.; Falcone, N.; Cui, Q.; Shah, S.; Hartel, M.C.; Yu, N.; Young, P.; de Barros, N.R.; et al. Lab-on-a-Contact Lens: Recent Advances and Future Opportunities in Diagnostics and Therapeutics. Adv. Mater. 2022, 34, 2108389. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Ong, Z.Z. Sensimed Triggerfish® Contact Lens Sensor for 24-Hour Intraocular Pressure Profile-Safety and Validity. Investig. Ophthalmol. Vis. Sci. 2021, 62, 2564. [Google Scholar]
- Kim, Y.W.; Kim, J.-S.; Lee, S.Y.; Ha, A.; Lee, J.; Park, Y.J.; Kim, Y.K.; Jeoung, J.W.; Park, K.H. Twenty-Four–Hour Intraocular Pressure–Related Patterns from Contact Lens Sensors in Normal-Tension Glaucoma and Healthy Eyes: The Exploring Nyctohemeral Intraocular Pressure Related Pattern for Glaucoma Management (ENIGMA) Study. Ophthalmology 2020, 127, 1487–1497. [Google Scholar] [CrossRef]
- Qiao, Y.; Luo, J.; Cui, T.; Liu, H.; Tang, H.; Zeng, Y.; Liu, C.; Li, Y.; Jian, J.; Wu, J.; et al. Soft Electronics for Health Monitoring Assisted by Machine Learning. Nano-Micro Lett. 2023, 15, 66. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, S.R.; Mothilal, M.; Priyadharshini, B.; Damodharan, N. Thermosensitive hydrogels—A potential carrier for the delivery of drugs and macromolecules. Int. J. Appl. Pharm. 2021, 3, 102–109. [Google Scholar] [CrossRef]
- Mansouri, K.; Gillmann, K. Intereye Symmetry of 24-Hour Intraocular Pressure–Related Patterns in Untreated Glaucoma Patients Using a Contact Lens Sensor. J. Glaucoma 2020, 29, 666. [Google Scholar] [CrossRef]
- Dinis, H.; Mendes, P.M. A Comprehensive Review of Powering Methods Used in State-of-the-Art Miniaturized Implantable Electronic Devices. Biosens. Bioelectron. 2021, 172, 112781. [Google Scholar] [CrossRef] [PubMed]
- Gassel, C.J.; Dzhelebov, D.N.; Voykov, B. Detailed Intraocular Pressure Curve by Telemetric Tonometry with an Implanted Pressure Sensor before and after PreserFlo® MicroShunt Implantation: A Case Report. Ophthalmol. Eye Dis. 2023, 15, 25158414221149927. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Park, J.; Park, Y.G.; Cha, E.; Ku, M.; An, H.S.; Lee, K.P.; Huh, M.I.; Kim, J.; Kim, T.S.; et al. A Soft and Transparent Contact Lens for the Wireless Quantitative Monitoring of Intraocular Pressure. Nat. Biomed. Eng. 2021, 5, 772–782. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Cui, T.; Hirtz, T.; Qiao, Y.; Li, X.; Zhong, F.; Han, X.; Yang, Y.; Zhang, S.; Ren, T.-L. Highly Transparent and Sensitive Graphene Sensors for Continuous and Non-Invasive Intraocular Pressure Monitoring. ACS Appl. Mater. Interfaces 2020, 12, 18375–18384. [Google Scholar] [CrossRef] [PubMed]
- Phan, A.; Truong, P.; Camp, A.; Stewart, K.; Suen, B.; Weinreb, R.N.; Talke, F.E. A Wireless Handheld Pressure Measurement System for In Vivo Monitoring of Intraocular Pressure in Rabbits. IEEE Trans. Biomed. Eng. 2020, 67, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Huang, L.; Weinreb, R.N.; Cheng, H. Wearable Electronic Devices for Glaucoma Monitoring and Therapy. Mater. Des. 2021, 212, 110183. [Google Scholar] [CrossRef]
- Esen, F.; Eraslan, M.; Cerman, E.; Celiker, H.; Kazokoglu, H. Diurnal Spikes of Intraocular Pressure in Uveitic Glaucoma: A 24-Hour Intraocular Pressure Monitoring Study. Semin. Ophthalmol. 2020, 35, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Shioya, S.; Higashide, T.; Tsuchiya, S.; Simon-Zoula, S.; Varidel, T.; Cerboni, S.; Mansouri, K.; Sugiyama, K. Using 24-Hr Ocular Dimensional Profile Recorded with a Sensing Contact Lens to Identify Primary Open-Angle Glaucoma Patients with Intraocular Pressure Constantly below the Diagnostic Threshold. Acta Ophthalmol. 2020, 98, e1017–e1023. [Google Scholar] [CrossRef]
- van den Bosch, J.J.O.N.; Pennisi, V.; Mansouri, K.; Weinreb, R.N.; Thieme, H.; Hoffmann, M.B.; Choritz, L. Effect of Eyelid Muscle Action and Rubbing on Telemetrically Obtained Intraocular Pressure in Patients with Glaucoma with an IOP Sensor Implant. Br. J. Ophthalmol. 2023, 107, 1425–1431. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Mansouri, K.; Moghimi, S.; Weinreb, R.N. Nocturnal Variability of Intraocular Pressure Monitored With Contact Lens Sensor Is Associated With Visual Field Loss in Glaucoma. J. Glaucoma 2021, 30, e56. [Google Scholar] [CrossRef]
- Muniesa, M.J.; Benítez, I.; Ezpeleta, J.; Sánchez de la Torre, M.; Pazos, M.; Millà, E.; Barbé, F. Effect of CPAP Therapy on 24-Hour Intraocular Pressure-Related Pattern From Contact Lens Sensors in Obstructive Sleep Apnea Syndrome. Transl. Vis. Sci. Technol. 2021, 10, 10. [Google Scholar] [CrossRef]
- Carnero, E.; Bragard, J.; Urrestarazu, E.; Rivas, E.; Polo, V.; Larrosa, J.M.; Antón, V.; Peláez, A.; Moreno-Montañés, J. Continuous Intraocular Pressure Monitoring in Patients with Obstructive Sleep Apnea Syndrome Using a Contact Lens Sensor. PLoS ONE 2020, 15, e0229856. [Google Scholar] [CrossRef] [PubMed]
- Tojo, N.; Hayashi, A. Can a Contact Lens Sensor Predict the Success of Trabectome Surgery? Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, K.; Shaarawy, T. Continuous Intraocular Pressure Monitoring with a Wireless Ocular Telemetry Sensor: Initial Clinical Experience in Patients with Open Angle Glaucoma. Br. J. Ophthalmol. 2011, 95, 627–629. [Google Scholar] [CrossRef] [PubMed]
- Pajic, B.; Resan, M.; Pajic-Eggspuehler, B.; Massa, H.; Cvejic, Z. Triggerfish Recording of IOP Patterns in Combined HFDS Minimally Invasive Glaucoma and Cataract Surgery: A Prospective Study. J. Clin. Med. 2021, 10, 3472. [Google Scholar] [CrossRef]
- Erras, A.; Shahrvini, B.; Weinreb, R.N.; Baxter, S.L. Review of Glaucoma Medication Adherence Monitoring in the Digital Health Era. Br. J. Ophthalmol. 2023, 107, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, K.; Rao, H.L.; Weinreb, R.N. Short-Term and Long-Term Variability of Intraocular Pressure Measured with an Intraocular Telemetry Sensor in Patients with Glaucoma. Ophthalmology 2021, 128, 227–233. [Google Scholar] [CrossRef]
- Wasilewicz, R.; Varidel, T.; Simon-Zoula, S.; Schlund, M.; Cerboni, S.; Mansouri, K. First-in-Human Continuous 24-Hour Measurement of Intraocular Pressure and Ocular Pulsation Using a Novel Contact Lens Sensor. Br. J. Ophthalmol. 2020, 104, 1519–1523. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Huang, X.; Li, X.; Yang, C.; Zhang, T.; Wu, Q.; Liu, D.; Lin, H.; Chen, W.; Hu, N.; et al. Wearable and Implantable Intraocular Pressure Biosensors: Recent Progress and Future Prospects. Adv. Sci. 2021, 8, 2002971. [Google Scholar] [CrossRef] [PubMed]
- Dou, Z.; Tang, J.; Liu, Z.; Sun, Q.; Wang, Y.; Li, Y.; Yuan, M.; Wu, H.; Wang, Y.; Pei, W.; et al. Wearable Contact Lens Sensor for Non-Invasive Continuous Monitoring of Intraocular Pressure. Micromachines 2021, 12, 108. [Google Scholar] [CrossRef]
- Shin, H.; Seo, H.; Chung, W.G.; Joo, B.J.; Jang, J.; Park, J.-U. Recent Progress on Wearable Point-of-Care Devices for Ocular Systems. Lab Chip 2021, 21, 1269–1286. [Google Scholar] [CrossRef]
- Wang, Y.; Li, T.; Li, Y.; Yang, R.; Zhang, G. 2D-Materials-Based Wearable Biosensor Systems. Biosensors 2022, 12, 936. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Zhang, J. Real-Time Monitoring of Intraocular Pressure in Glaucoma Patients Using Wearable Mobile Medicine Devices. J. Healthc. Eng. 2022, 2022, e2271937. [Google Scholar] [CrossRef] [PubMed]
- Gillmann, K.; Wasilewicz, R.; Hoskens, K.; Simon-Zoula, S.; Mansouri, K. Continuous 24-Hour Measurement of Intraocular Pressure in Millimeters of Mercury (mmHg) Using a Novel Contact Lens Sensor: Comparison with Pneumatonometry. PLoS ONE 2021, 16, e0248211. [Google Scholar] [CrossRef] [PubMed]
- Saxby, E.; Mansouri, K.; Tatham, A.J. Intraocular Pressure Monitoring Using an Intraocular Sensor Before and After Glaucoma Surgery. J. Glaucoma 2021, 30, 941. [Google Scholar] [CrossRef]
- Kim, T.Y.; Mok, J.W.; Hong, S.H.; Jeong, S.H.; Choi, H.; Shin, S.; Joo, C.-K.; Hahn, S.K. Wireless Theranostic Smart Contact Lens for Monitoring and Control of Intraocular Pressure in Glaucoma. Nat. Commun. 2022, 13, 6801. [Google Scholar] [CrossRef] [PubMed]
- Downs, J.C.C.; Kuhn Asif, S.; Rhodes, L.A.; Samuels, B.C.; Jasien, J.V. Comparison of Extraocular (EO) and Intraocular (IO) Pressure Transducers for Measurement of Transient IOP Fluctuations Using Continuous Wireless Telemetry. Investig. Ophthalmol. Vis. Sci. 2020, 61, 4771. [Google Scholar]
- Joseph, A.; Rajendran, A.; Karthikeyan, A.; Nair, B.G. Implantable Microfluidic Device: An Epoch of Technology. Curr. Pharm. Des. 2022, 28, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Kwarteng, E.; Cebe, M. A Survey on Security Issues in Modern Implantable Devices: Solutions and Future Issues. Smart Health 2022, 25, 100295. [Google Scholar] [CrossRef]
- Meduri, E.; Gillmann, K.; Mansouri, K. Intraocular Pressure Variations After Intravitreal Injections Measured With an Implanted Suprachoroidal Telemetry Sensor. J. Glaucoma 2021, 30, e360. [Google Scholar] [CrossRef]
- Gopesh, T.; Camp, A.; Unanian, M.; Friend, J.; Weinreb, R.N. Rapid and Accurate Pressure Sensing Device for Direct Measurement of Intraocular Pressure. Transl. Vis. Sci. Technol. 2020, 9, 28. [Google Scholar] [CrossRef]
- Park, I.; Park, H.S.; Kim, H.K.; Chung, W.K.; Kim, K. Real-Time Measurement of Intraocular Pressure Variation during Automatic Intravitreal Injections: An Ex-Vivo Experimental Study Using Porcine Eyes. PLoS ONE 2021, 16, e0256344. [Google Scholar] [CrossRef] [PubMed]
- Dennyson Savariraj, A.; Salih, A.; Alam, F.; Elsherif, M.; AlQattan, B.; Khan, A.A.; Yetisen, A.K.; Butt, H. Ophthalmic Sensors and Drug Delivery. ACS Sens. 2021, 6, 2046–2076. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Hui, A.; Phan, C.-M.; Read, M.L.; Azar, D.; Buch, J.; Ciolino, J.B.; Naroo, S.A.; Pall, B.; Romond, K.; et al. BCLA CLEAR—Contact Lens Technologies of the Future. Contact Lens Anterior Eye 2021, 44, 398–430. [Google Scholar] [CrossRef] [PubMed]
- Awwad, S.; Ibeanu, N.; Liu, T.; Velentza-Almpani, A.; Chouhan, N.; Vlatakis, S.; Khaw, P.T.; Brocchini, S.; Bouremel, Y. Real-Time Monitoring Platform for Ocular Drug Delivery. Pharmaceutics 2023, 15, 1444. [Google Scholar] [CrossRef] [PubMed]
- Gillmann, K.; Young, C.C.; Stanley, J.; Seibold, L.K.; Hoskens, K.; Midha, N.; Kahook, M.Y.; Mansouri, K. Relationship Between Contact Lens Sensor Output Parameters and Visual Field Progression in Open-Angle Glaucoma: Assessment of a Practical Tool to Guide Clinical Risk-Assessment. J. Glaucoma 2020, 29, 461. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, M.; Hayashi, A.; Tojo, N. Questionnaire Survey on Complications during 24-h Measurement of Intraocular Pressure-Related Patterns with a Contact Lens Sensor. Int. Ophthalmol. 2020, 40, 1963–1968. [Google Scholar] [CrossRef] [PubMed]
- Toshida, H. Topographical Central Island-Like Pattern After 24 Hrs of Continuous Intraocular Pressure Monitoring with a Contact Lens Sensor. Int. Med. Case Rep. J. 2020, 13, 19–26. [Google Scholar] [CrossRef]
- Miki, A.; Kumoi, M.; Maeda, N.; Koh, S.; Matsushita, K.; Nishida, K. Transient Changes in Refractive Error and Corneal Tomography after 24-h Continuous Monitoring of Intraocular Pressure Patterns with a Contact Lens Sensor. Jpn. J. Ophthalmol. 2020, 64, 127–133. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tonometer Type | Working Principle | Contact/Noncontact | Advantages | Disadvantages | Accuracy | Cost | Indication |
|---|---|---|---|---|---|---|---|
| Goldmann applanation tonometer (GAT) | Applanation | Contact |
|
| High | Low | Gold standard for IOP measurement |
| Perkins tonometer | Applanation | Contact |
|
| High | Low | Suitable for patients who can’t sit at the slit-lamp |
| Mackay-Marg–type tonometers (e.g., Tono-Pen) | Applanation | Contact |
|
| Moderate | Low | Patients with corneal scars or edema, supine patients |
| Rebound tonometers (e.g., iCare tonometer) | Ballistic probe (rebound) | Contact |
|
| High | Low | Pediatrics, home tonometry |
| Noncontact tonometers (e.g., air-puff, ORA) | Applanation | Noncontact |
|
| Moderate (Air-Puff), High (ORA) | Medium | Large-scale glaucoma-screening programs |
| Dynamic contour tonometer (DCT, PASCAL) | Contour matching | Contact |
|
| High | Medium | After corneal refractive surgery |
| Pneumotonometer | Applanation | Contact |
|
| Moderate | Expensive | Eyes with corneal scars, edema, or keratoprostheses |
| Schioetz tonometer | Indentation | Contact |
|
| Moderate | Low | Primarily used in developing countries |
| Tactile tension | Manual pressure | Contact |
|
| Low | None (manual) | Uncooperative patients or for detecting large IOP differences between eyes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, K.Y.; Mina, M.; Carbonneau, M.; Marchand, M.; Tran, S.D. Advancements in Wearable and Implantable Intraocular Pressure Biosensors for Ophthalmology: A Comprehensive Review. Micromachines 2023, 14, 1915. https://doi.org/10.3390/mi14101915
Wu KY, Mina M, Carbonneau M, Marchand M, Tran SD. Advancements in Wearable and Implantable Intraocular Pressure Biosensors for Ophthalmology: A Comprehensive Review. Micromachines. 2023; 14(10):1915. https://doi.org/10.3390/mi14101915
Chicago/Turabian StyleWu, Kevin Y., Mina Mina, Marjorie Carbonneau, Michael Marchand, and Simon D. Tran. 2023. "Advancements in Wearable and Implantable Intraocular Pressure Biosensors for Ophthalmology: A Comprehensive Review" Micromachines 14, no. 10: 1915. https://doi.org/10.3390/mi14101915
APA StyleWu, K. Y., Mina, M., Carbonneau, M., Marchand, M., & Tran, S. D. (2023). Advancements in Wearable and Implantable Intraocular Pressure Biosensors for Ophthalmology: A Comprehensive Review. Micromachines, 14(10), 1915. https://doi.org/10.3390/mi14101915