



Towards a Point-of-Care Test of CD4+ T Lymphocyte Concentrations for Immune Status Monitoring with Magnetic Flow Cytometry


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
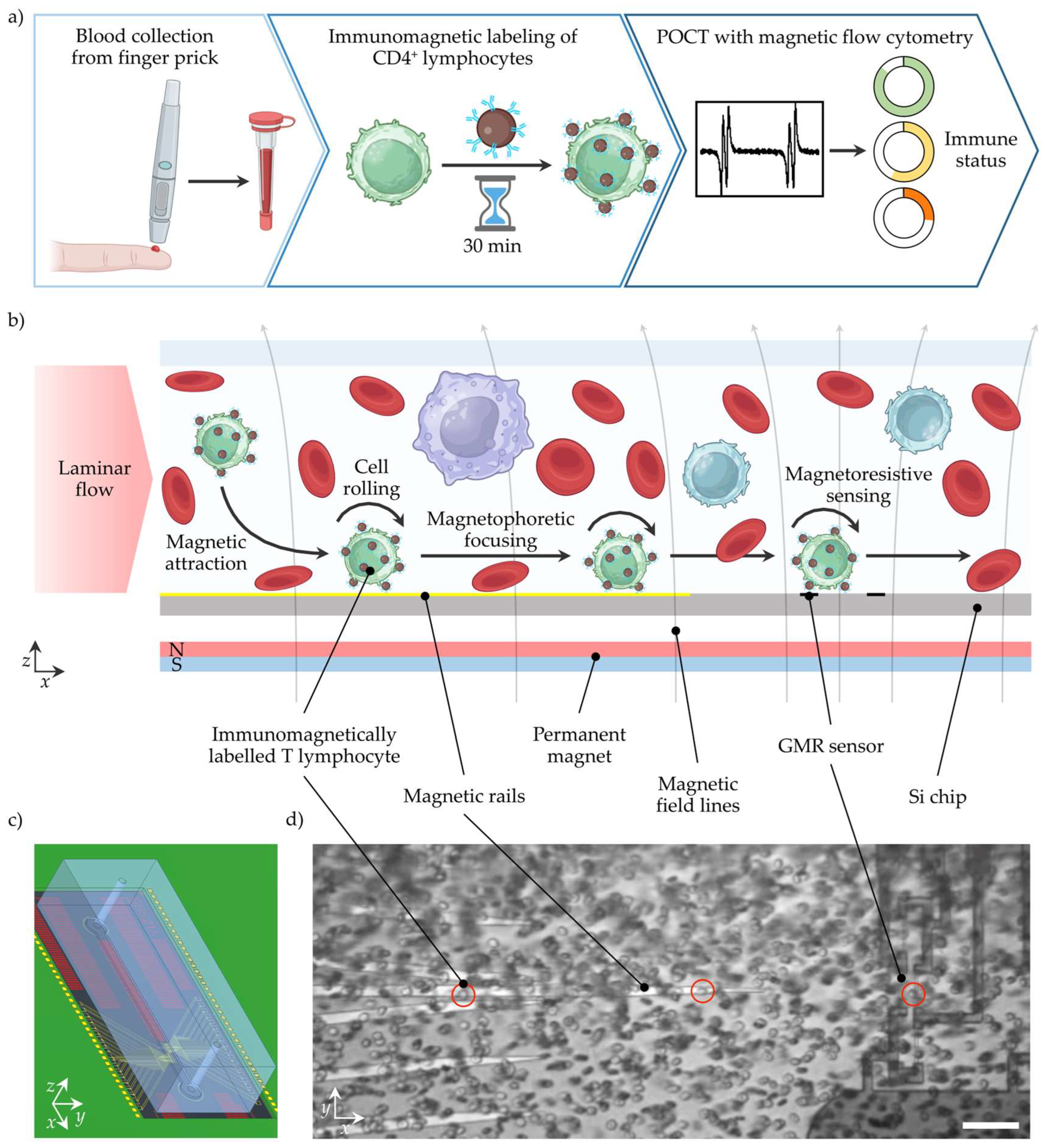
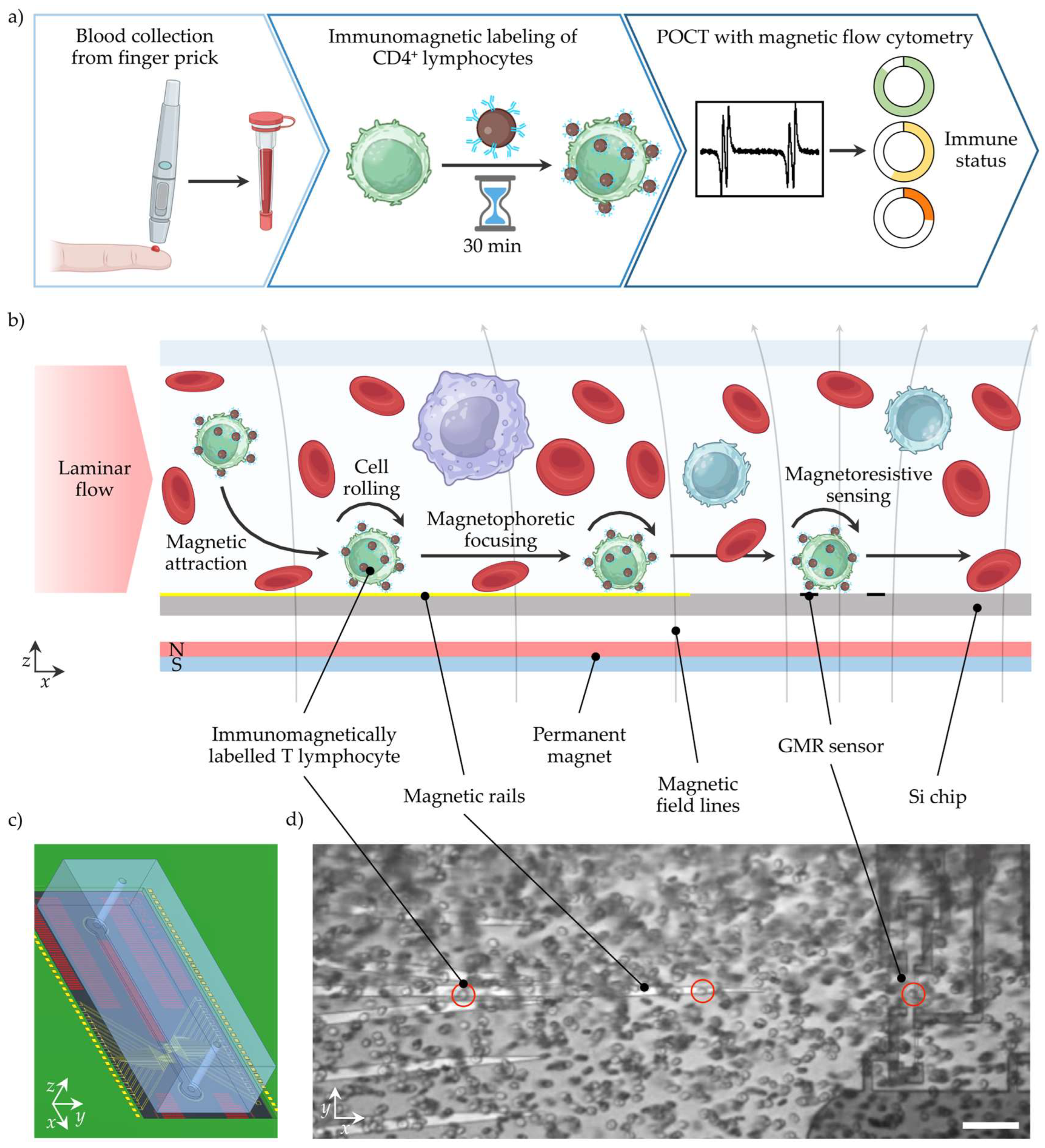
2. POCT Workflow Concept for Immune Status Assessment with MFC
3. Materials and Methods
3.1. Magnetic Flow Cytometer
3.2. Immunomagnetic Cell Labeling and Magnetic Flow Cytometry Measurements
3.3. Optical Reference Measurements
4. Results and Discussion
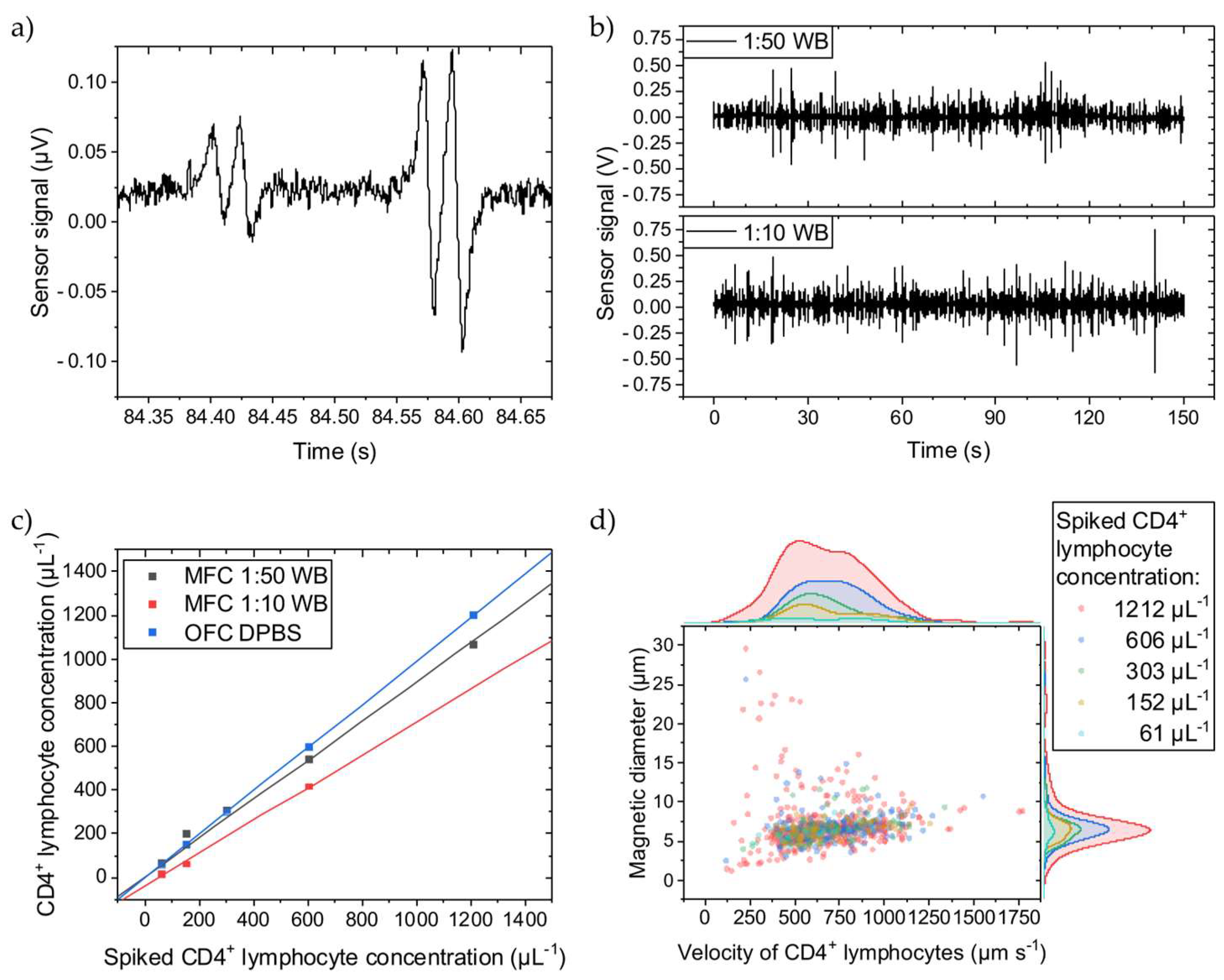
4.1. Cellular Background Impact on Determined Cell Concentrations with MFC
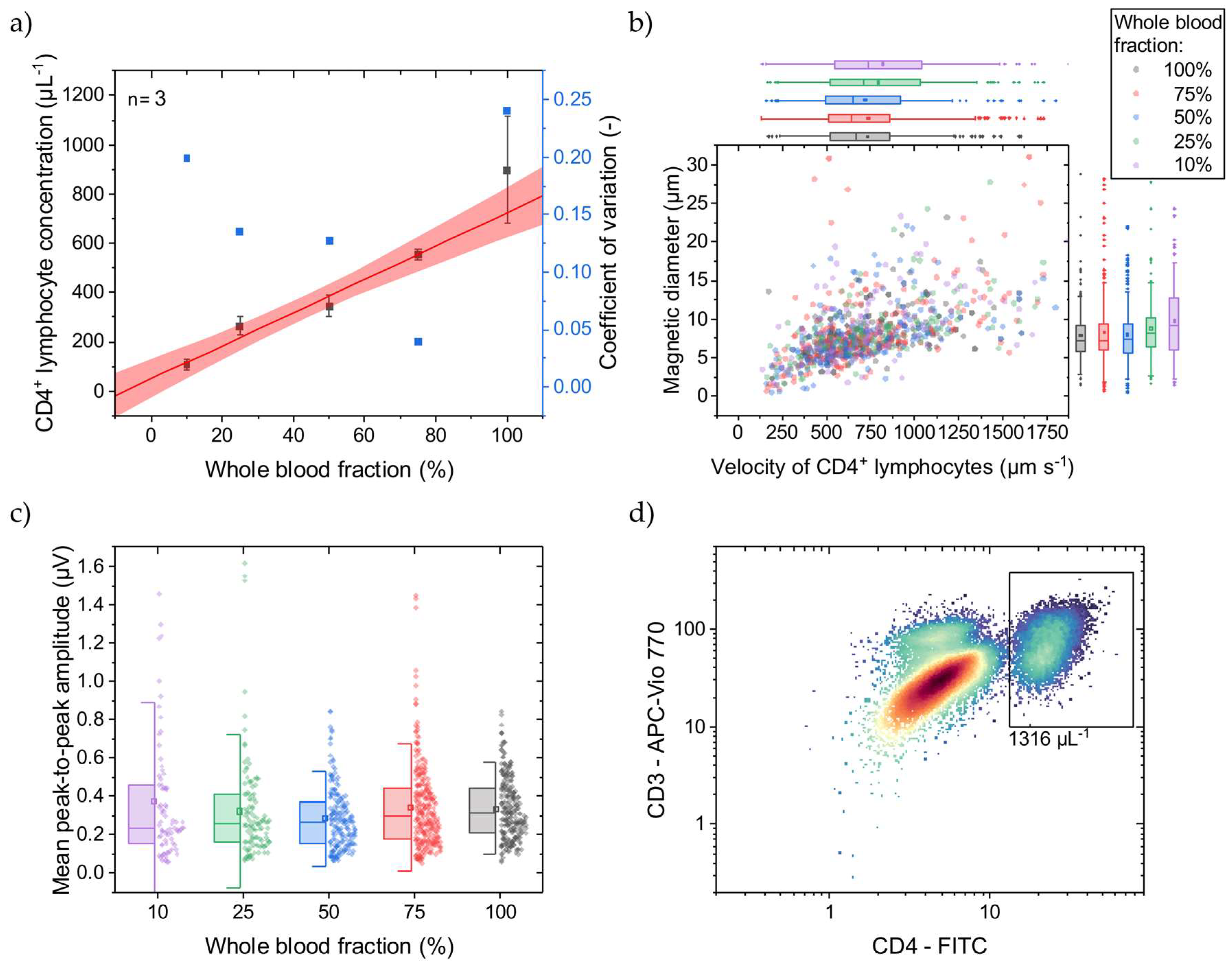
4.2. Simulating HIV Patient’s CD4+ T Lymphocyte Concentrations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manz, A.; Graber, N.; Widmer, H.M. Miniaturized Total Chemical Analysis Systems: A Novel Concept for Chemical Sensing. Sens. Actuators B Chem. 1990, 1, 244–248. [Google Scholar] [CrossRef]
- Lee, A.P. 2020 vision: Celebrating the 20th year of Lab on a Chip. Lab Chip 2020, 20, 1889–1890. [Google Scholar] [CrossRef]
- Touloumi, G.; Pantazis, N.; Pillay, D.; Paraskevis, D.; Chaix, M.L.; Bucher, H.C.; Kücherer, C.; Zangerle, R.; Kran, A.M.B.; Porter, K. Impact of HIV-1 Subtype on CD4 Count at HIV Seroconversion, Rate of Decline, and Viral Loads Set Point in European Seroconverter Cohorts. Clin. Infect. Dis. 2013, 56, 888–897. [Google Scholar] [CrossRef]
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV; Department of Health and Human Services: Washington, DC, USA, 2024. Available online: https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv (accessed on 13 February 2024).
- McCune, J.M. The dynamics of CD4+ T-cell depletion in HIV disease. Nature 2001, 410, 974–979. [Google Scholar] [CrossRef]
- Mellors, J.W.; Munoz, A.; Giorgi, J.V.; Margolick, J.B.; Tassoni, C.J.; Gupta, P.; Kingsley, L.A.; Todd, J.A.; Saah, A.J.; Detels, R.; et al. Plasma Viral Load and CD4+ Lymphocytes as Prognostic Markers of HIV-1 Infection. Ann. Intern. Med. 1997, 126, 946–954. [Google Scholar] [CrossRef]
- Egger, M.; May, M.; Chêne, G.; Phillips, A.N.; Ledergerber, B.; Dabis, F.; Costagliola, D.; Monforte, A.D.A.; De Wolf, F.; Reiss, P.; et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: A collaborative analysis of prospective studies. Lancet 2002, 360, 119–129. [Google Scholar] [CrossRef]
- Kaufmann, G.R.; Perrin, L.; Pantaleo, G. CD4 T-Lymphocyte Recovery in Individuals With Advanced HIV-1 Infection Receiving Potent Antiretoviral Therapy for 4 Years. Arch. Intern. Med. 2003, 163, 2187–2195. [Google Scholar] [CrossRef]
- De Rosa, S.C.; Brenchley, J.M.; Roederer, M. Beyond six colors: A new era in flow cytometry. Nat. Med. 2003, 9, 112–117. [Google Scholar] [CrossRef]
- Dorn-Beineke, A.; Sack, U. Quality control and validation in flow cytometry. J. Lab. Med. 2016, 40, 1–13. [Google Scholar] [CrossRef]
- Robinson, J.P.; Roederer, M. Flow cytometry strikes gold. Science 2015, 350, 739–740. [Google Scholar] [CrossRef]
- Göhde, W.; Cassens, U.; Lehman, L.G.; Traoré, Y.; Göhde jun, W.; Berkes, P.; Westerberg, C.; Greve, B. Individual Patient-Dependent Influence of Erythrocyte Lysis Procedures on Flow-Cytometric Analysis of Leukocyte Subpopulations. Transfus. Med. Hemother. 2003, 30, 165–170. [Google Scholar] [CrossRef]
- Greve, B.; Beller, C.; Cassens, U.; Sibrowski, W.; Severin, E.; Göhde, W. High-Grade Loss of Leukocytes and Hematopoietic Progenitor Cells Caused by Erythrocyte-Lysing Procedures for Flow Cytometric Analyses. J. Hematother. Stem Cell Res. 2003, 12, 321–330. [Google Scholar] [CrossRef]
- Greve, B.; Beller, C.; Cassens, U.; Sibrowski, W.; Göhde, W. The Impact of Erythrocyte Lysing Procedures on the Recovery of Hematopoietic Progenitor Cells in Flow Cytometric Analysis. Stem Cells 2006, 24, 793–799. [Google Scholar] [CrossRef]
- Ateya, D.A.; Erickson, J.S.; Howell, P.B.; Hilliard, L.R.; Golden, J.P.; Ligler, F.S. The good, the bad, and the tiny: A review of microflow cytometry. Anal. Bioanal. Chem. 2008, 391, 1485–1498. [Google Scholar] [CrossRef]
- Chicharo, A.; Martins, M.; Barnsley, L.C.; Taouallah, A.; Fernandes, J.; Silva, B.F.; Cardoso, S.; Diéguez, L.; Espiña, B.; Freitas, P.P. Enhanced magnetic micrometer with 3D flow focusing for cell enumeration. Lab Chip 2018, 18, 2593–2603. [Google Scholar] [CrossRef]
- Reisbeck, M.; Helou, M.J.; Richter, L.; Kappes, B.; Friedrich, O.; Hayden, O. Magnetic fingerprints of rolling cells for quantitative flow cytometry in whole blood. Sci. Rep. 2016, 6, 32838. [Google Scholar] [CrossRef]
- Helou, M.J.; Reisbeck, M.; Tedde, S.F.; Richter, L.; Bär, L.; Bosch, J.J.; Stauber, R.H.; Quandt, E.; Hayden, O. Time-of-flight magnetic flow cytometry in whole blood with integrated sample preparation. Lab Chip 2013, 13, 1035. [Google Scholar] [CrossRef]
- Issadore, D.; Chung, J.; Shao, H.; Liong, M.; Ghazani, A.A.; Castro, C.M.; Weissleder, R.; Lee, H. Ultrasensitive Clinical Enumeration of Rare Cells ex Vivo Using a Micro-Hall Detector. Sci. Transl. Med. 2012, 4, 141ra92. [Google Scholar] [CrossRef]
- Fernandes, A.C.; Duarte, C.M.; Cardoso, F.A.; Bexiga, R.; Cardoso, S.; Freitas, P.P. Lab-on-Chip Cytometry Based on Magnetoresistive Sensors for Bacteria Detection in Milk. Sensors 2014, 14, 15496–15524. [Google Scholar] [CrossRef]
- Duarte, C.M.; Fernandes, A.C.; Cardoso, F.A.; Bexiga, R.; Cardoso, S.F.; Freitas, P.J.P. Magnetic Counter for Group B Streptococci Detection in Milk. IEEE Trans. Magn. 2015, 51, 5100304. [Google Scholar] [CrossRef]
- Loureiro, J.; Andrade, P.Z.; Cardoso, S.; da Silva, C.L.; Cabral, J.M.; Freitas, P.P. Magnetoresistive chip cytometer. Lab Chip 2011, 11, 2255–2261. [Google Scholar] [CrossRef]
- Reisbeck, M.; Richter, L.; Helou, M.J.; Arlinghaus, S.; Anton, B.; van Dommelen, I.; Nitzsche, M.; Baßler, M.; Kappes, B.; Friedrich, O.; et al. Hybrid integration of scalable mechanical and magnetophoretic focusing for magnetic flow cytometry. Biosens. Bioelectron. 2018, 109, 98–108. [Google Scholar] [CrossRef]
- Drain, P.K.; Hyle, E.P.; Noubary, F.; Freedberg, K.A.; Wilson, D.; Bishai, W.R.; Rodriguez, W.; Bassett, I.V. Evaluating Diagnostic Point-of-Care Tests in Resource-Limited Settings. Lancet Infect. Dis. 2014, 14, 239–249. [Google Scholar] [CrossRef]
- Benjamin, E. Self-Monitoring of Blood Glucose: The Basics. Clin. Diabetes 2002, 20, 45–47. [Google Scholar] [CrossRef]
- Huang, W.; Omana-Zapata, I.; Bornheimer, S.; Kirakossian, H.; Wu, A.H.B. CD4 Counts in Capillary and Venous Blood Samples. J. HIV AIDS 2017, 3. [Google Scholar]
- Xia, Y.; Whitesides, G.M. Soft Lithography. Angew. Chem. 1998, 37, 550–575. [Google Scholar] [CrossRef]
- Rosen, R. Optimality Principles in Biology; Butterwoth & Co (Publishers) Ltd.: London, UK, 1967; p. 56. [Google Scholar]
- Cohen, E.; Kramer, M.; Shochat, T.; Goldberg, E.; Krause, I. Relationship between hematocrit levels and intraocular pressure in men and women. Medicine 2017, 96, e8290. [Google Scholar] [CrossRef]
- WHO HIV Treatment and Care Team. Point-of-Care CD4 Tests to Support the Identification of Individuals with Advanced HIV Disease; World Health Organization: Geneva, Switzerland, 2020; Available online: https://iris.who.int/bitstream/handle/10665/331681/WHO-UCN-HHS-19.56-eng.pdf?sequence=1 (accessed on 13 March 2024).
- Leuthner, M.; Hayden, O. Grease the gears: How lubrication of syringe pumps impacts microfluidic flow precision. Lab Chip 2024, 24, 56–62. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leuthner, M.; Reisbeck, M.; Helou, M.; Hayden, O. Towards a Point-of-Care Test of CD4+ T Lymphocyte Concentrations for Immune Status Monitoring with Magnetic Flow Cytometry. Micromachines 2024, 15, 520. https://doi.org/10.3390/mi15040520
Leuthner M, Reisbeck M, Helou M, Hayden O. Towards a Point-of-Care Test of CD4+ T Lymphocyte Concentrations for Immune Status Monitoring with Magnetic Flow Cytometry. Micromachines. 2024; 15(4):520. https://doi.org/10.3390/mi15040520
Chicago/Turabian StyleLeuthner, Moritz, Mathias Reisbeck, Michael Helou, and Oliver Hayden. 2024. "Towards a Point-of-Care Test of CD4+ T Lymphocyte Concentrations for Immune Status Monitoring with Magnetic Flow Cytometry" Micromachines 15, no. 4: 520. https://doi.org/10.3390/mi15040520
APA StyleLeuthner, M., Reisbeck, M., Helou, M., & Hayden, O. (2024). Towards a Point-of-Care Test of CD4+ T Lymphocyte Concentrations for Immune Status Monitoring with Magnetic Flow Cytometry. Micromachines, 15(4), 520. https://doi.org/10.3390/mi15040520