Incidence, Risk Factors, and Outcomes of Arterial Thromboembolism in Patients with Pancreatic Cancer Following Palliative Chemotherapy

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patient Demographics and Clinical Characteristics
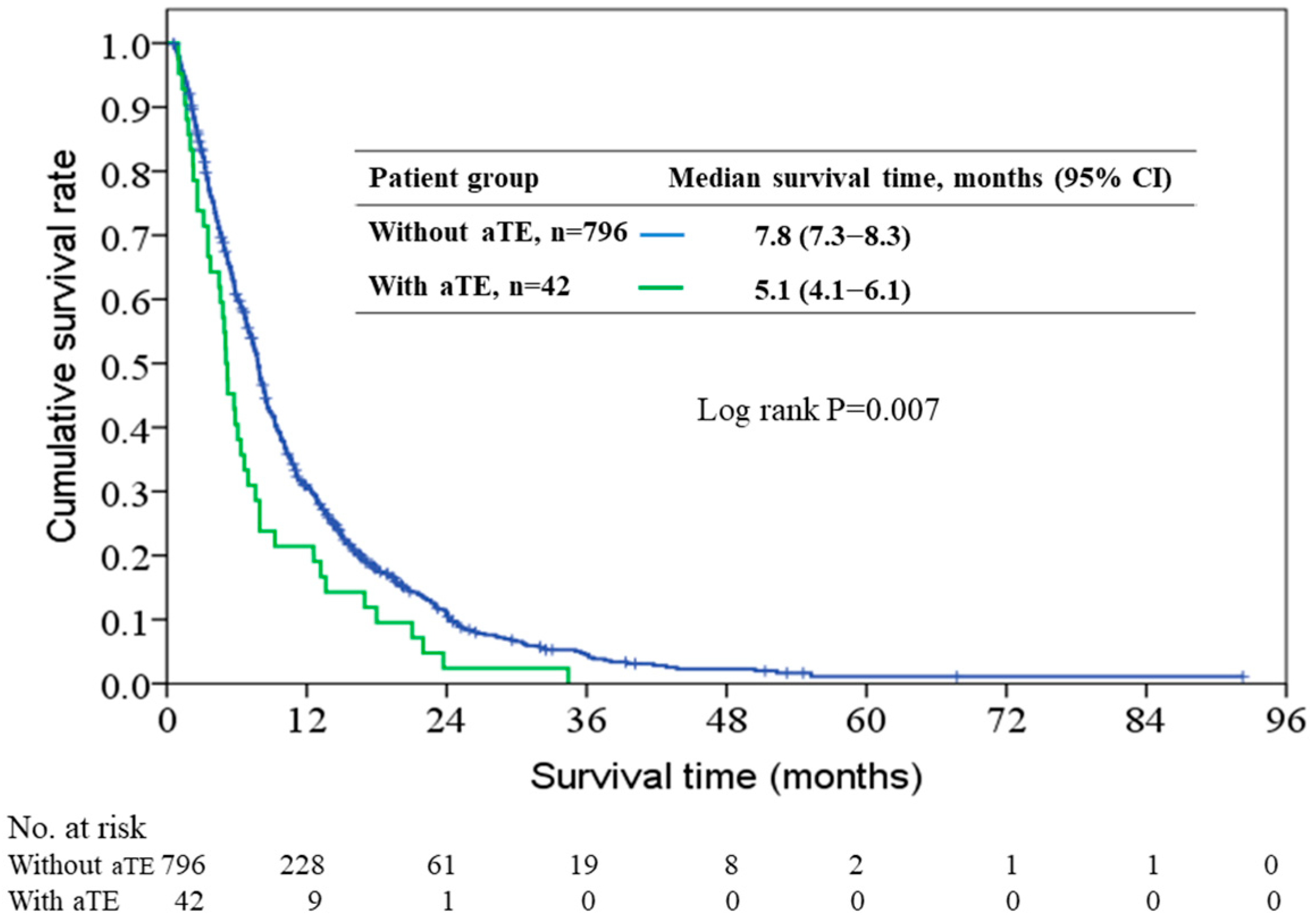
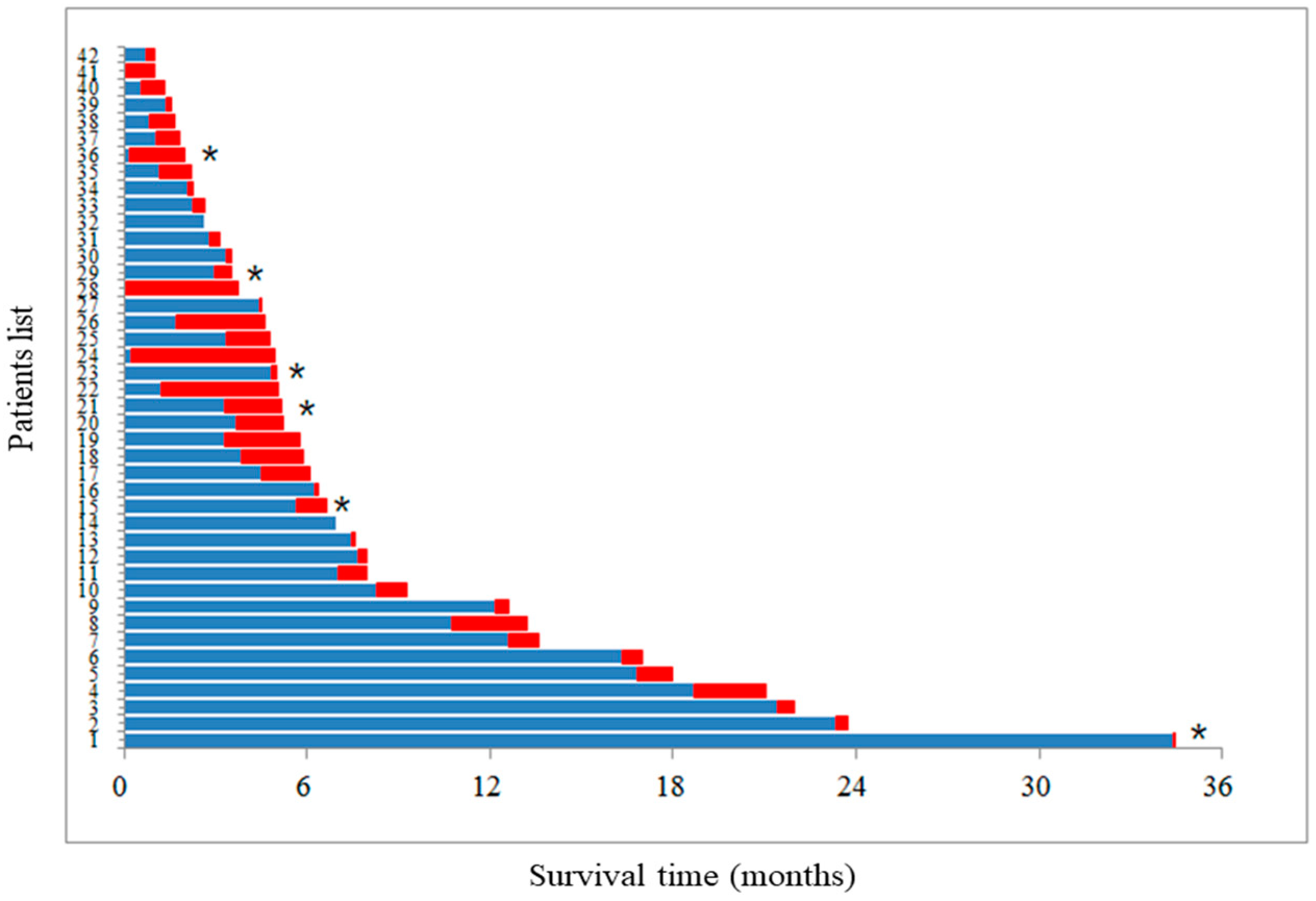
2.2. Patient Outcomes and the Impact of aTE on Overall Survival
2.3. Risk Factors for aTE
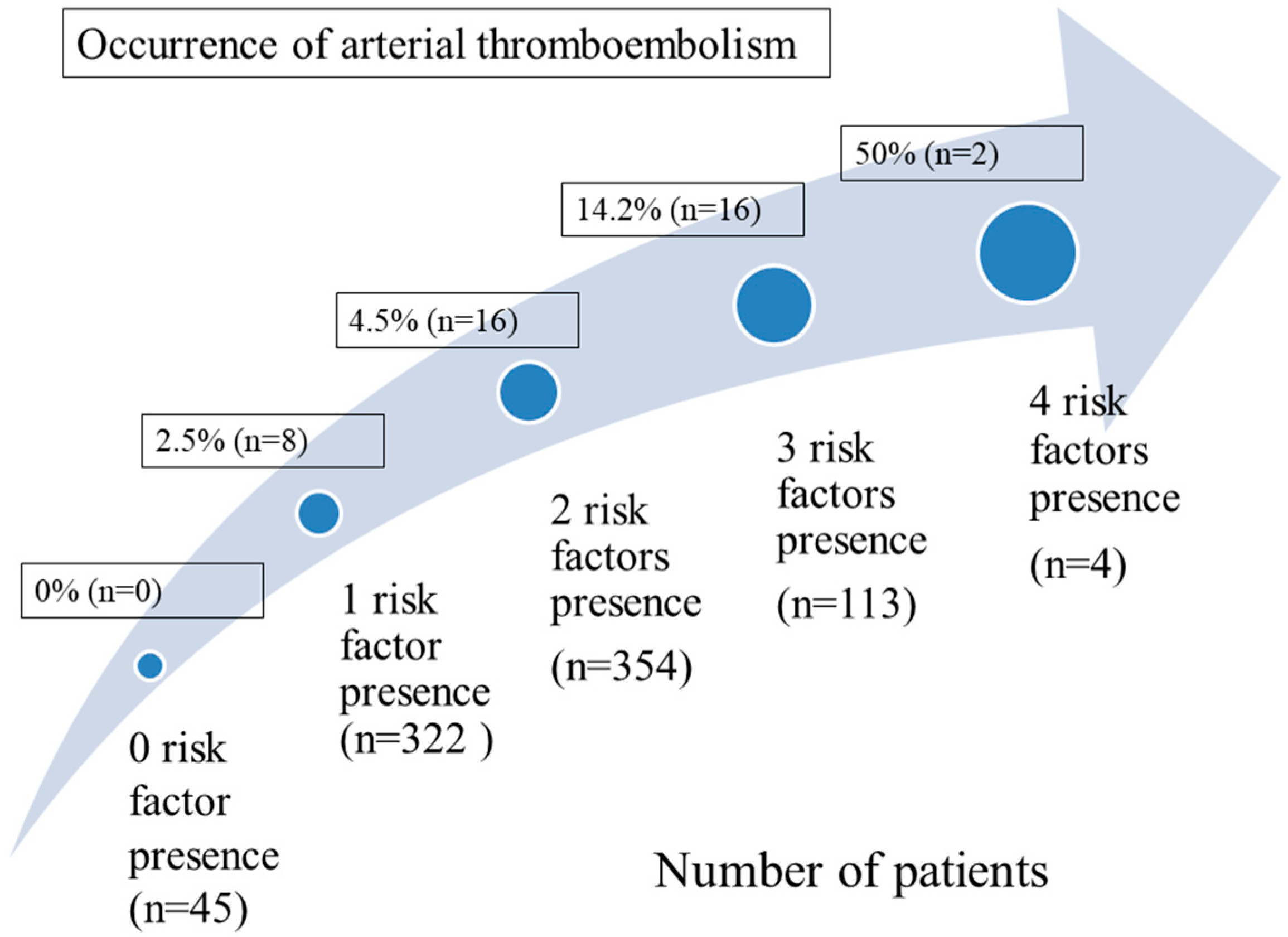
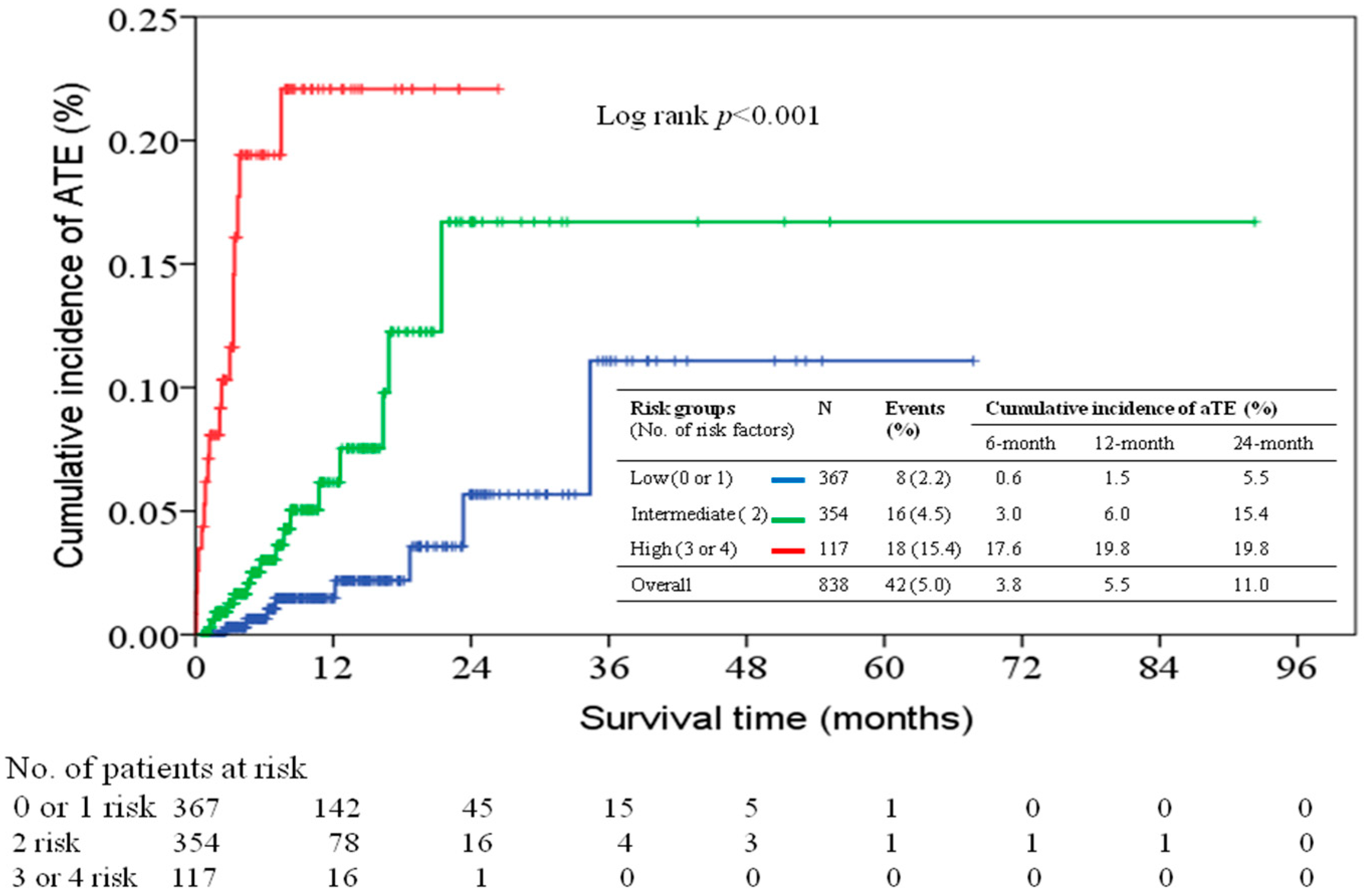
2.4. Predictive Model of aTE Incidence Based on Presence of Numbers of Risk Factor
3. Discussion
4. Patients and Methods
4.1. Patient Selection
4.2. Data Collection
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Falanga, A.; Russo, L.; Verzeroli, C. Mechanisms of thrombosis in cancer. Thromb. Res. 2013, 131, S59–S62. [Google Scholar] [CrossRef]
- Noble, S.; Pasi, J. Epidemiology and pathophysiology of cancer-associated thrombosis. Br. J. Cancer 2010, 102, S2–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, T.H.; Mellemkjaer, L.; Olsen, J.H.; Baron, J.A. Prognosis of cancers associated with venous thromboembolism. N. Engl. J. Med. 2000, 343, 1846–1850. [Google Scholar] [CrossRef] [PubMed]
- Kessler, C.M. The link between cancer and venous thromboembolism: A review. Am. J. Clin. Oncol. 2009, 32, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Connolly, G.C. Assessing risk of venous thromboembolism in the patient with cancer. J. Clin. Oncol. 2009, 27, 4839–4847. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Francis, C.W.; Culakova, E.; Kuderer, N.M.; Lyman, G.H. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer 2007, 110, 2339–2346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood 2008, 111, 4902–4907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraaijpoel, N.; Van Es, N.; Raskob, G.E.; Büller, H.R.; Carrier, M.; Zhang, G.; Lin, M.; Grosso, M.A.; Di Nisio, M. Risk sores for occult cancer in patients with venous thromboembolism: A post Hoc analysis of the Hokusai-VTE study. Thromb. Haemost. 2018, 118, 1270–1278. [Google Scholar] [CrossRef] [PubMed]
- Chew, T.W.; Gau, C.S.; Wen, Y.W.; Shen, L.J.; Mullins, C.D.; Hsiao, F.Y. Epidemiology, clinical profile and treatment patterns of venous thromboembolism in cancer patients in Taiwan: A population-based study. BMC Cancer 2015, 15, 298. [Google Scholar] [CrossRef] [PubMed]
- Navi, B.B.; Reiner, A.S.; Kamel, H.; Iadecola, C.; Okin, P.M.; Elkind, M.S.V.; Panageas, K.S.; DeAngelis, L.M. Risk of arterial thromboembolism in patients with cancer. J. Am. Coll. Cardiol. 2017, 70, 926–938. [Google Scholar] [CrossRef] [PubMed]
- Navi, B.B.; Reiner, A.S.; Kamel, H.; Iadecola, C.; Elkind, M.S.; Panageas, K.S.; DeAngelis, L.M. OC-02-Risk of arterial thromboembolism in patients with breast cancer. Thromb. Res. 2016, 140, S169. [Google Scholar] [CrossRef]
- Lin, S.Y.; Lin, C.L.; Chang, C.H.; Wu, H.C.; Wang, I.K.; Chou, C.Y.; Liang, J.A. Risk of acute myocardial infarction in upper tract urothelial carcinoma patients receiving radical nephroureterectomy: A population-based cohort study. Oncotarget 2017, 8, 79498–79506. [Google Scholar] [CrossRef] [PubMed]
- Navi, B.B.; Reiner, A.S.; Kamel, H.; Iadecola, C.; Elkind, M.S.; Panageas, K.S.; DeAngelis, L.M. Association between incident cancer and subsequent stroke. Ann. Neurol. 2015, 77, 291–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.C.; Muo, C.H.; Lee, Y.T.; Yu, Y.H.; Sung, F.C. Lung cancer and incidence of stroke: A population-based cohort study. Stroke 2011, 42, 3034–3039. [Google Scholar] [CrossRef] [PubMed]
- Li, S.H.; Chen, W.H.; Tang, Y.; Rau, K.M.; Chen, Y.Y.; Huang, T.L.; Liu, J.S.; Huang, C.H. Incidence of ischemic stroke post-chemotherapy: A retrospective review of 10,963 patients. Clin. Neurol. Neurosurg. 2006, 108, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Cestari, D.M.; Weine, D.M.; Panageas, K.S.; Segal, A.Z.; DeAngelis, L.M. Stroke in patients with cancer: Incidence and etiology. Neurology 2004, 62, 2025–2030. [Google Scholar] [CrossRef] [PubMed]
- Grazioli, S.; Paciaroni, M.; Agnelli, G.; Acciarresi, M.; Alberti, A.; D’Amore, C.; Caso, V.; Venti, M.; Guasti, L.; Ageno, W.; et al. Cancer-associated ischemic stroke: A retrospective multicentre cohort study. Thromb. Res. 2018, 165, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Selvik, H.A.; Bjerkreim, A.T.; Thomassen, L.; Waje-Andreassen, U.; Naess, H.; Kvistad, C.E. When to screen ischaemic stroke patients for cancer. Cerebrovasc. Dis. 2018, 45, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Grisold, W.; Oberndorfer, S.; Struhal, W. Stroke and cancer: A review. Acta Neurol. Scand. 2009, 119, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Aarnio, K.; Joensuu, H.; Haapaniemi, E.; Melkas, S.; Kaste, M.; Tatlisumak, T.; Putaala, J. Cancer in young adults with ischemic stroke. Stroke 2015, 46, 1601–1606. [Google Scholar] [CrossRef] [PubMed]
- Castro, H.H.G.; Alencar, A.P.; Benseñor, I.M.; Lotufo, P.A.; Goulart, A.C. Multimorbidities are associated to lower survival in ischaemic stroke: Results from a Brazilian Stroke Cohort (EMMA Study). Cerebrovasc. Dis. 2017, 44, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Trousseau, A. Phlegmasia alba dolens. In Clinique medicale de l‘Hotel–Dieu de Paris; JB Balliere et Fils: Paris, France, 1865; Volume 2, pp. 654–712. [Google Scholar]
- Epstein, A.S.; Soff, G.A.; Capanu, M.; Crosbie, C.; Shah, M.A.; Kelsen, D.P.; Denton, B.; Gardos, S.; O’Reilly, E.M. Analysis of incidence and clinical outcomes in patients with thromboembolic events and invasive exocrine pancreatic cancer. Cancer 2012, 118, 3053–3061. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.C.; Chang, W.L.; Hsu, M.H.; Yeh, C.H.; Muo, C.H.; Chang, K.S.; Hsu, C.Y.; Wu, B.T.; Lai, C.H.; Lee, C.H.; et al. Higher stroke incidence in the patients with pancreatic cancer: A nation-based cohort study in Taiwan. Medicine (Baltimore) 2018, 97, e0133. [Google Scholar] [CrossRef] [PubMed]
- Gong, I.Y.; Yan, A.T.; Ko, D.T.; Earle, C.C.; Cheung, W.Y.; Peacock, S.; Hall, M.; Gale, C.P.; Chan, K.K.W. Temporal changes in treatments and outcomes after acute myocardial infarction among cancer survivors and patients without cancer, 1995 to 2013. Cancer 2018, 124, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Reiner, A.S.; Navi, B.B.; DeAngelis, L.M.; Panageas, K.S. Increased risk of arterial thromboembolism in older men with breast cancer. Breast Cancer Res. Treat. 2017, 166, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Price, A.J.; Wright, F.L.; Green, J.; Balkwill, A.; Kan, S.W.; Yang, T.O.; Floud, S.; Kroll, M.E.; Simpson, R.; Sudlow, C.L.M.; et al. Differences in risk factors for 3 types of stroke: UK prospective study and meta-analyses. Neurology 2018, 90, e298–e306. [Google Scholar] [CrossRef] [PubMed]
- Pokorney, S.D.; Piccini, J.P.; Stevens, S.R.; Patel, M.R.; Pieper, K.S.; Halperin, J.L.; Breithardt, G.; Singer, D.E.; Hankey, G.J.; Hacke, W.; et al. Cause of death and predictors of all-cause mortality in anticoagulated patients with nonvalvular atrial fibrillation: Data from ROCKET AF. J. Am. Heart Assoc. 2016, 5, e002197. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Wang, C.Y.; Li, Y.X.; Pan, Y.; Niu, J.Q.; He, S.M. Determination of the upper cut-off values of serum alanine aminotransferase and aspartate aminotransferase in Chinese. World J. Gastroenterol. 2015, 21, 2419–2424. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.S.; Stagliano, N.E.; Donovan, M.J.; Breitbart, R.E.; Ginsburg, G.S. Atherosclerosis: A cancer of the blood vessels? A. J. Clin. Pathol. 2001, 116, S97–S107. [Google Scholar]
- Heit, J.A.; Silverstein, M.D.; Mohr, D.N.; Petterson, T.M.; O’Fallon, W.M.; Melton, L.J., 3rd. Risk factors for deep vein thrombosis and pulmonary embolism: A population-based case-control study. Arch. Intern. Med. 2000, 160, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Muñoz Martín, A.J.; García Alfonso, P.; Rupérez Blanco, A.B.; Pérez Ramírez, S.; Blanco Codesido, M.; Martín Jiménez, M. Incidence of venous thromboembolism (VTE) in ambulatory patients with pancreatic cancer receiving chemotherapy and analysis of Khorana’s predictive model. Clin. Transl. Oncol. 2014, 16, 927–930. [Google Scholar] [CrossRef] [PubMed]
- Sorgun, M.H.; Kuzu, M.; Ozer, I.S.; Yilmaz, V.; Ulukan, C.; Cotur Levent, H.; Tezcan, S.; Rzayev, S.; Rawandi, A.; Bakırarar, B.; et al. Risk factors, biomarkers, etiology, outcome and prognosis of ischemic stroke in cancer patients. Asian Pac. J. Cancer Prev. 2018, 19, 649–653. [Google Scholar] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; Katus, H.A.; Lindahl, B.; Morrow, D.A.; Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction; et al. Third universal definition of myocardial infarction. Circulation 2012, 126, 2020–2035. [Google Scholar] [CrossRef] [PubMed]
- Newschaffer, C.J.; Bush, T.L.; Penberthy, L.E.; Bellantoni, M.; Helzlsour, K.; Diener-West, M. Does comorbid disease interact with cancer? An epidemiologic analysis of mortality in a cohort of elderly breast cancer patients. J. Gerontol. A Biol. Sci. Med. Sci. 1998, 53, 372–378. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Value |
|---|---|---|
| Age, years (range) | median | 62 (23–89) |
| Gender, n (%) | male | 474 (59.3) |
| female | 364 (40.7) | |
| BMI, kg/m2 (range) | median | 23 (13.0–36.2) |
| ECOG PS | 0–1 | 597 (71.2) |
| 2 | 206 (24.6) | |
| 3 | 35 (4.2) | |
| Smoking history, n (%) | yes | 306 (36.5) |
| Charlson comorbidity index, n (%) | 0 | 227 (27.1) |
| 1 | 292 (34.8) | |
| 2 | 193 (23.0) | |
| 3 | 102 (12.2) | |
| 4 | 19 (2.3) | |
| 5 | 5 (0.6) | |
| Comorbidity, n (%) | diabetic mellitus | 313 (37.4) |
| hypertension | 332 (39.6) | |
| cerebrovascular disease | 30 (3.6) | |
| coronary artery disease | 52 (6.2) | |
| arrhythmia | 13 (1.6) | |
| Tumor site of pancreas, n (%) | head | 343 (40.9) |
| body | 148 (17.7) | |
| tail | 171 (20.4) | |
| overlapping | 176 (21.0) | |
| Tumor stage, n (%) | III | 183 (21.8) |
| IV | 655 (78.2) | |
| Tumor grade, n (%) | well to moderate | 93 (11.1) |
| poorly | 92 (11.0) | |
| unclassified or unknown | 653 (77.9) | |
| Presence with obstructive jaundice under drainage, n (%) | yes | 272 (32.5) |
| no | 566 (67.5) | |
| Metastatic organ, n (%) | liver | 438 (52.3) |
| peritoneum | 239 (28.5) | |
| lymph nodes | 150 (17.9) | |
| lung | 98 (11.7) | |
| Laboratory data, median (range) | Hemoglobin, g/dL | 12.3 (3.6–17.4) |
| Leukocyte count, 109/L | 7600 (1400–77,000) | |
| Platelet count, 109/L | 221 (23–500) | |
| Albumin, g/dL | 3.8 (1.9–4.5) | |
| AST, μ/L | 34 (10–954) | |
| Alkaline phosphatase, IU/L | 110 (10–2688) | |
| CEA, ng/mL | 5.3 (0.3–50,000) | |
| CA19-9, μ/mL | 780 (0.5–50,000) | |
| Use of chemotherapy agent, n (%) | Gemcitabine | 792 (94.5) |
| Platins | 433 (51.7) | |
| S-1 | 335 (40.0) | |
| 5-fluorouracil | 257 (30.7) | |
| Irinotecan | 17 (2.0) | |
| Erlotinib | 14 (1.8) | |
| Nab-paclitaxel | 12 (1.4) | |
| Patients with aTE | 42 (5.0) | |
| Type of aTE | ischemic stroke | 36 (4.3) |
| myocardial infarction | 6 (0.7) |
| Variable | Category | ATE No/Total No (%) | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |||
| BMI, kg/m2 | ≤23 | 17/474 (3.6) | 1 | 1 | ||||
| >23 | 25/364 (6.9) | 1.98 | 1.05–3.73 | 0.037 | 1.69 | 0.87–3.23 | 0.12 | |
| ECOG PS | 0–2 | 38/803 (4.7) | 1 | 1 | ||||
| 3 | 4/35 (11.4) | 2.6 | 0.87–7.73 | 0.086 | 1.76 | 0.52–5.97 | 0.37 | |
| Hypertension | no | 14/506 (2.8) | 1 | 1 | ||||
| yes | 28/332 (8.4) | 3.24 | 1.68–6.25 | <0.001 | 2.74 | 1.37–5.47 | 0.004 | |
| Cerebrovascular disease | no | 37/808 (4.6) | 1 | 1 | ||||
| yes | 5/30 (16.7) | 4.17 | 1.51–11.5 | 0.006 | 1.98 | 0.62–6.34 | 0.25 | |
| Coronary artery disease | no | 38/786 (4.8) | 1 | |||||
| yes | 4/52 (7.7) | 1.64 | 0.56–4.79 | 0.37 | ||||
| Arrhythmia | no | 39/825 (4.7) | 1 | 1 | ||||
| yes | 3/13 (23.1) | 6.05 | 1.60–22.9 | 0.008 | 4.77 | 1.10–20.7 | 0.037 | |
| Tumor stage, 7th AJCC | III | 3/183 (1.6) | 1 | 1 | ||||
| IV | 39/655 (6.0) | 3.80 | 1.16–12.4 | 0.027 | 4.12 | 1.24–13.6 | 0.021 | |
| Aspartate transaminase, μ/L | ≤34 | 16/450 (3.6) | 1 | 1 | ||||
| >34 | 26/388 (6.7) | 1.98 | 1.05–3.75 | 0.036 | 1.97 | 1.02–3.78 | 0.043 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, Y.-S.; Chen, J.-S.; Chen, Y.-Y.; Lu, C.-H.; Chang, P.-H.; Chou, W.-C. Incidence, Risk Factors, and Outcomes of Arterial Thromboembolism in Patients with Pancreatic Cancer Following Palliative Chemotherapy. Cancers 2018, 10, 432. https://doi.org/10.3390/cancers10110432
Hung Y-S, Chen J-S, Chen Y-Y, Lu C-H, Chang P-H, Chou W-C. Incidence, Risk Factors, and Outcomes of Arterial Thromboembolism in Patients with Pancreatic Cancer Following Palliative Chemotherapy. Cancers. 2018; 10(11):432. https://doi.org/10.3390/cancers10110432
Chicago/Turabian StyleHung, Yu-Shin, Jen-Shi Chen, Yen-Yang Chen, Chang-Hsien Lu, Pei-Hung Chang, and Wen-Chi Chou. 2018. "Incidence, Risk Factors, and Outcomes of Arterial Thromboembolism in Patients with Pancreatic Cancer Following Palliative Chemotherapy" Cancers 10, no. 11: 432. https://doi.org/10.3390/cancers10110432
APA StyleHung, Y.-S., Chen, J.-S., Chen, Y.-Y., Lu, C.-H., Chang, P.-H., & Chou, W.-C. (2018). Incidence, Risk Factors, and Outcomes of Arterial Thromboembolism in Patients with Pancreatic Cancer Following Palliative Chemotherapy. Cancers, 10(11), 432. https://doi.org/10.3390/cancers10110432