DNA Mismatch Repair Protein Immunohistochemistry and MLH1 Promotor Methylation Testing for Practical Molecular Classification and the Prediction of Prognosis in Endometrial Cancer

 , ,
, , 
Abstract
:1. Introduction
2. Results
2.1. Clinicopathologic Characteristics
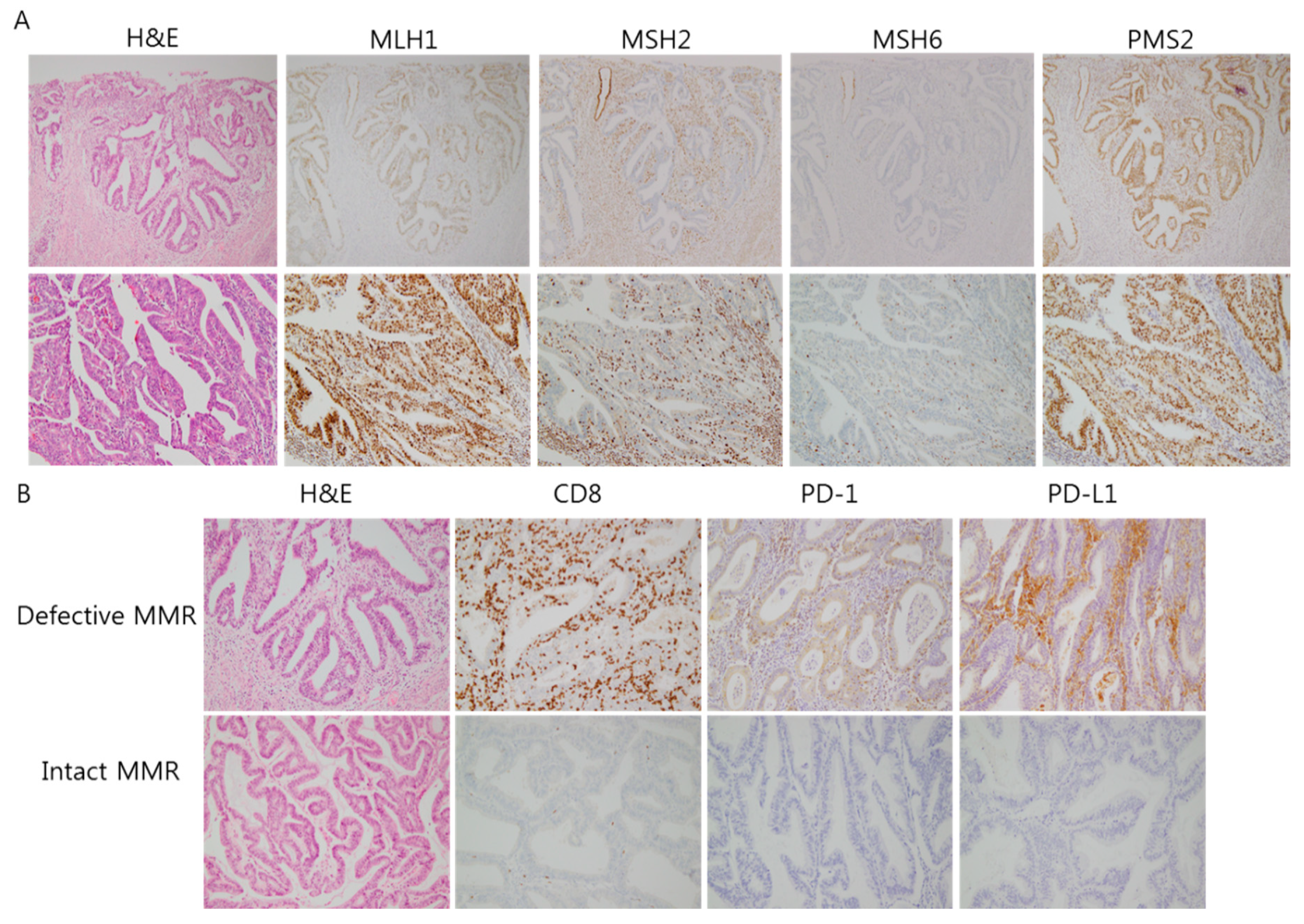
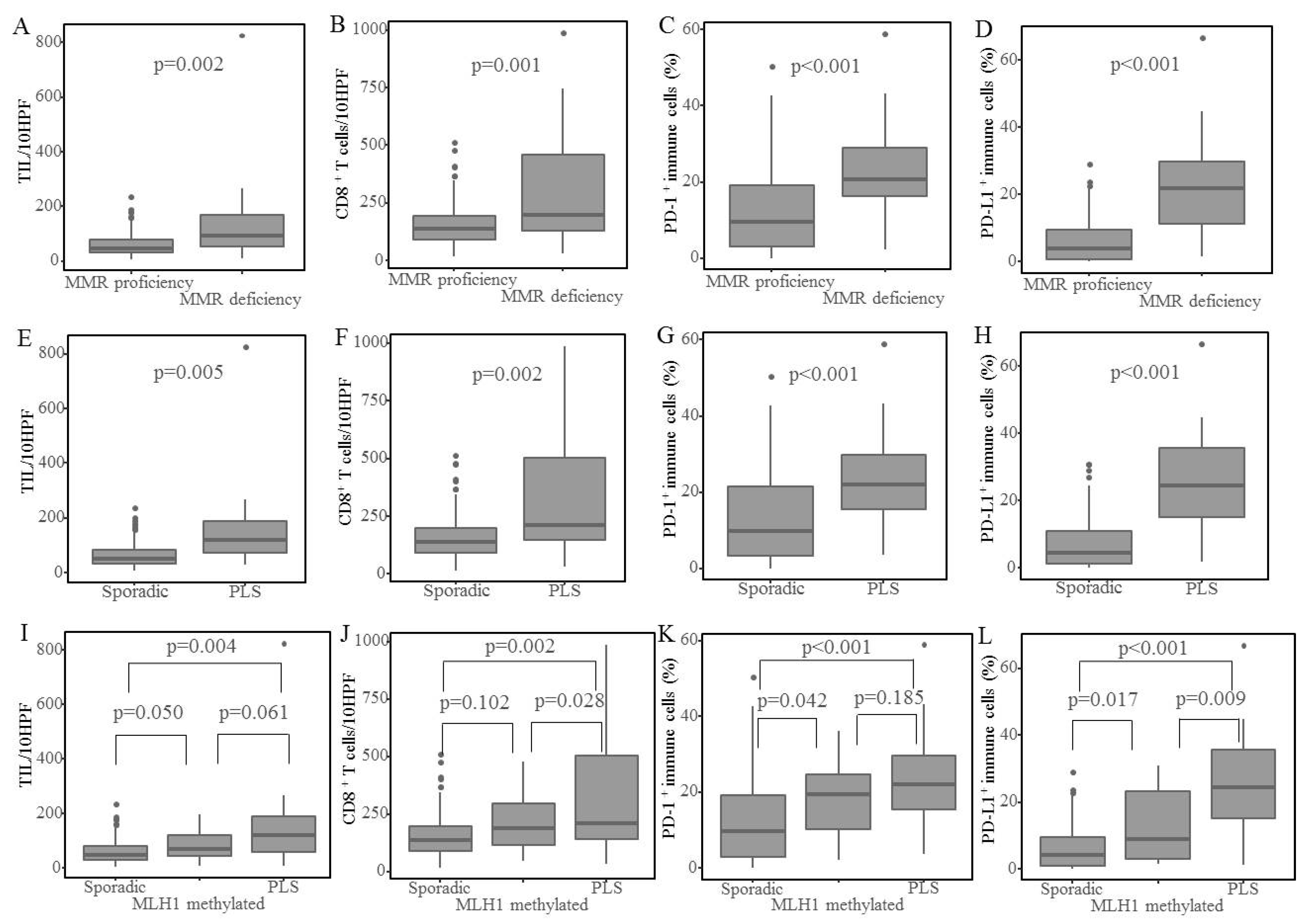
2.2. Peritumoral Immune Marker Expression
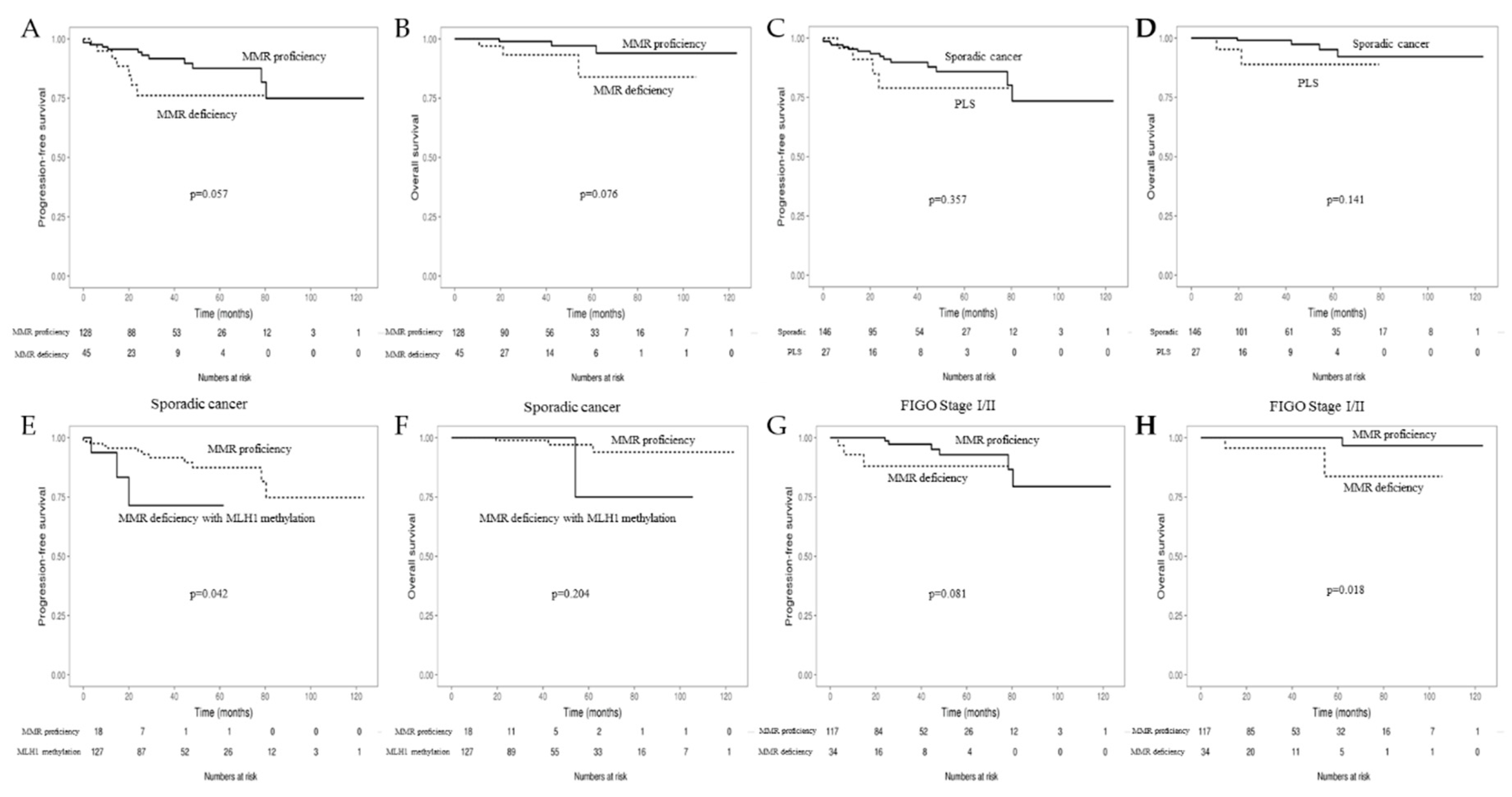
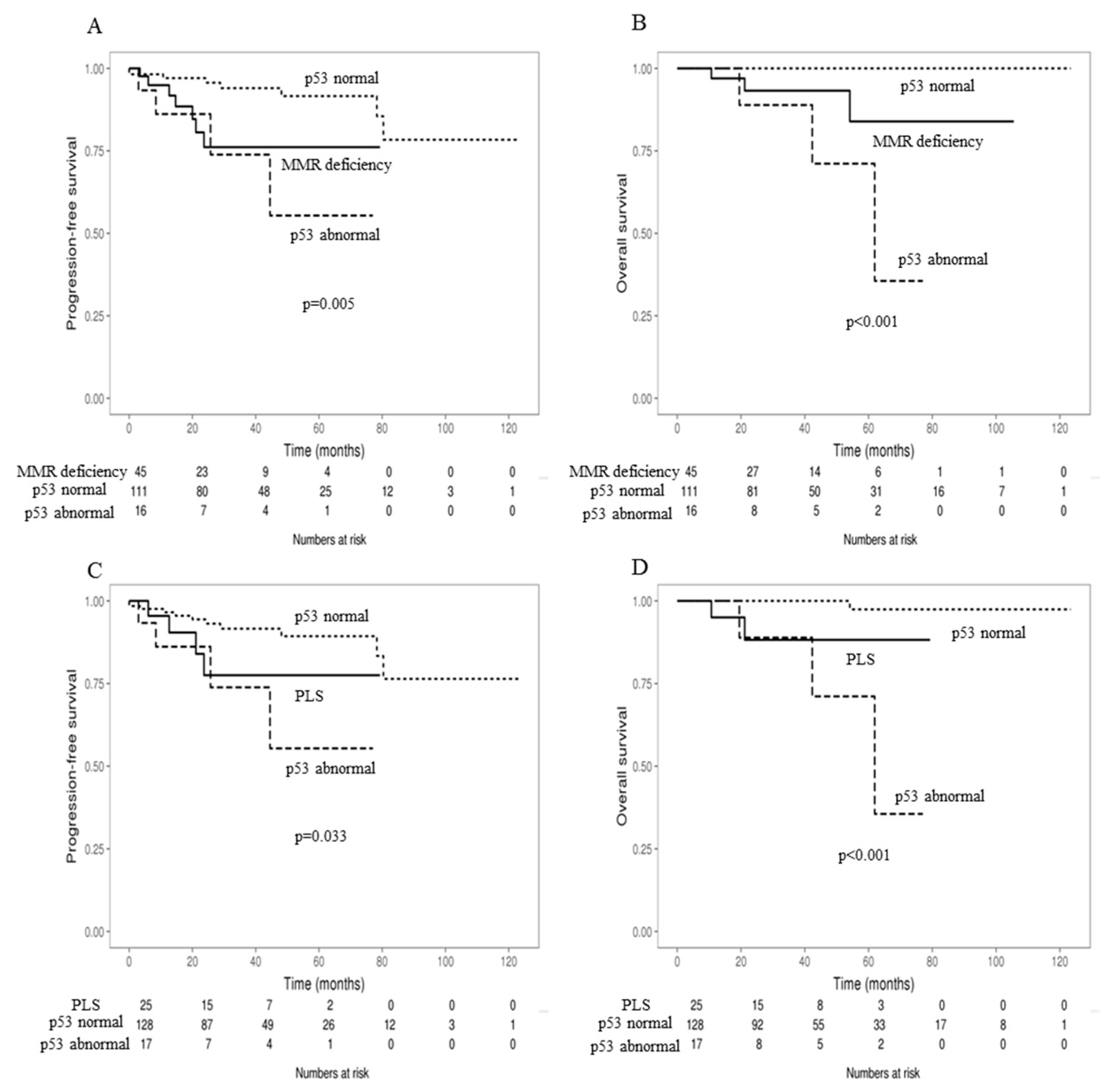
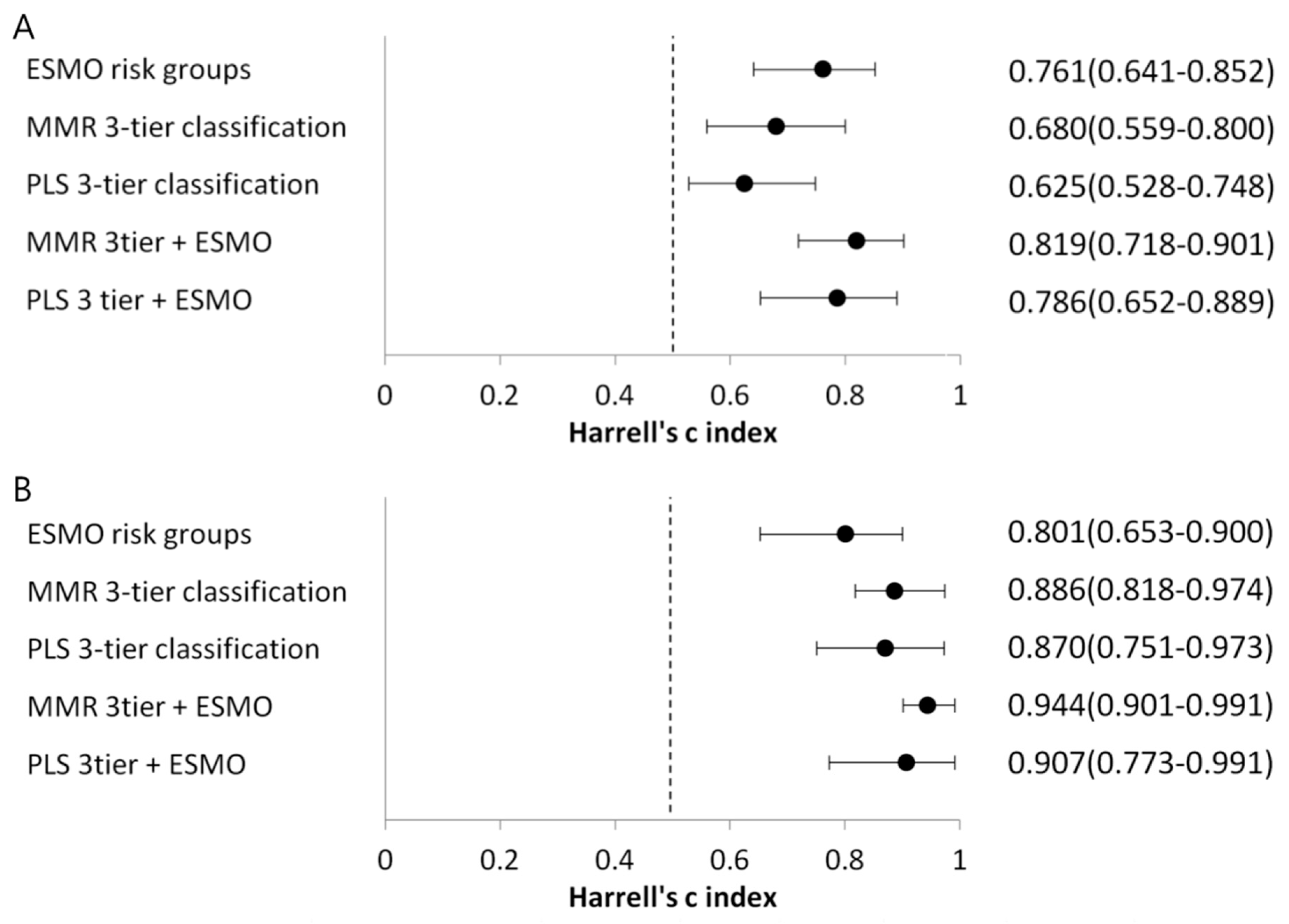
2.3. Prognosis
3. Discussion
4. Materials and Methods
4.1. Patients and Specimens
4.2. Immunohistochemistry
4.3. MLH1 Promoter Methylation Test
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- De Haydu, C.; Black, J.D.; Schwab, C.L.; English, D.P.; Santin, A.D. An update on the current pharmacotherapy for endometrial cancer. Expert Opin. Pharmacother. 2016, 17, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the united states. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Strafford, J.C. Genetic testing for lynch syndrome, an inherited cancer of the bowel, endometrium, and ovary. Rev. Obstet. Gynecol. 2012, 5, 42–49. [Google Scholar] [PubMed]
- Mills, A.M.; Liou, S.; Ford, J.M.; Berek, J.S.; Pai, R.K.; Longacre, T.A. Lynch syndrome screening should be considered for all patients with newly diagnosed endometrial cancer. Am. J. Surg. Pathol. 2014, 38, 1501–1509. [Google Scholar] [CrossRef] [PubMed]
- Goodfellow, P.J.; Billingsley, C.C.; Lankes, H.A.; Ali, S.; Cohn, D.E.; Broaddus, R.J.; Ramirez, N.; Pritchard, C.C.; Hampel, H.; Chassen, A.S.; et al. Combined microsatellite instability, mlh1 methylation analysis, and immunohistochemistry for lynch syndrome screening in endometrial cancers from gog210: An nrg oncology and gynecologic oncology group study. J. Clin. Oncol. 2015, 33, 4301–4308. [Google Scholar] [CrossRef] [PubMed]
- Bokhman, J.V. Two pathogenetic types of endometrial carcinoma. Gynecol. Oncol. 1983, 15, 10–17. [Google Scholar] [CrossRef]
- Murali, R.; Soslow, R.A.; Weigelt, B. Classification of endometrial carcinoma: More than two types. Lancet Oncol. 2014, 15, e268–e278. [Google Scholar] [CrossRef]
- Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; Benz, C.C.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [PubMed] [Green Version]
- Stelloo, E.; Nout, R.A.; Osse, E.M.; Jürgenliemk-Schulz, I.J.; Jobsen, J.J.; Lutgens, L.C.; van der Steen-Banasik, E.M.; Nijman, H.W.; Putter, H.; Bosse, T.; et al. Improved risk assessment by integrating molecular and clinicopathological factors in early-stage endometrial cancer—Combined analysis of the portec cohorts. Clin. Cancer Res. 2016, 22, 4215–4224. [Google Scholar] [CrossRef] [PubMed]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Yang, W.; Lum, A.; Senz, J.; Boyd, N.; Pike, J.; Anglesio, M.; Kwon, J.S.; et al. Confirmation of promise: A simple, genomics-based clinical classifier for endometrial cancer. Cancer 2017, 123, 802–813. [Google Scholar] [CrossRef] [PubMed]
- Billingsley, C.C.; Cohn, D.E.; Mutch, D.G.; Stephens, J.A.; Suarez, A.A.; Goodfellow, P.J. Polymerase varepsilon (pole) mutations in endometrial cancer: Clinical outcomes and implications for lynch syndrome testing. Cancer 2015, 121, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Church, D.N.; Stelloo, E.; Nout, R.A.; Valtcheva, N.; Depreeuw, J.; ter Haar, N.; Noske, A.; Amant, F.; Tomlinson, I.P.; Wild, P.J.; et al. Prognostic significance of pole proofreading mutations in endometrial cancer. J. Natl. Cancer Inst. 2015, 107, 402. [Google Scholar] [CrossRef] [PubMed]
- Howitt, B.E.; Shukla, S.A.; Sholl, L.M.; Ritterhouse, L.L.; Watkins, J.C.; Rodig, S.; Stover, E.; Strickland, K.C.; D’Andrea, A.D.; Wu, C.J.; et al. Association of polymerase e-mutated and microsatellite-instable endometrial cancers with neoantigen load, number of tumor-infiltrating lymphocytes, and expression of pd-1 and pd-l1. JAMA Oncol. 2015, 1, 1319–1323. [Google Scholar] [CrossRef] [PubMed]
- Eggink, F.A.; Van Gool, I.C.; Leary, A.; Pollock, P.M.; Crosbie, E.J.; Mileshkin, L.; Jordanova, E.S.; Adam, J.; Freeman-Mills, L.; Church, D.N.; et al. Immunological profiling of molecularly classified high-risk endometrial cancers identifies pole-mutant and microsatellite unstable carcinomas as candidates for checkpoint inhibition. Oncoimmunology 2017, 6, e1264565. [Google Scholar] [CrossRef] [PubMed]
- Fader, A.N.; Diaz, L.A.; Armstrong, D.K.; Tanner, E.J.; Uram, J.; Eyring, A.; Wang, H.; Fisher, G.; Greten, T.; Le, D. Preliminary results of a phase ii study: Pd-1 blockade in mismatch repair–deficient, recurrent or persistent endometrial cancer. Gynecol. Oncol. 2013, 141, 206–207. [Google Scholar] [CrossRef]
- Ott, P.A.; Bang, Y.J.; Berton-Rigaud, D.; Elez, E.; Pishvaian, M.J.; Rugo, H.S.; Puzanov, I.; Morgan, M.A.; Mehnert, J.M.; Aung, K.L.; et al. Pembrolizumab in advanced endometrial cancer: Preliminary results from the phase ib keynote-028 study. J. Clin. Oncol. 2016, 34, 5581. [Google Scholar]
- Cosgrove, C.M.; Cohn, D.E.; Goodfellow, P.J. Primum non nocere: Are we ready for pole testing in endometrial cancer? Gynecol. Oncol. 2017, 147, 240–242. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E., Jr.; Califf, R.M.; Pryor, D.B.; Lee, K.L.; Rosati, R.A. Evaluating the yield of medical tests. JAMA 1982, 247, 2543–2546. [Google Scholar] [CrossRef] [PubMed]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; Gonzalez-Martin, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. Esmo-esgo-estro consensus conference on endometrial cancer: Diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, 16–41. [Google Scholar] [CrossRef] [PubMed]
- Shikama, A.; Minaguchi, T.; Matsumoto, K.; Akiyama-Abe, A.; Nakamura, Y.; Michikami, H.; Nakao, S.; Sakurai, M.; Ochi, H.; Onuki, M.; et al. Clinicopathologic implications of DNA mismatch repair status in endometrial carcinomas. Gynecol. Oncol. 2016, 140, 226–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruegl, A.S.; Djordjevic, B.; Batte, B.; Daniels, M.; Fellman, B.M.; Urbauer, D.L.; Luthra, R.; Sun, C.; Lu, K.; Broaddus, R.R. Evaluation of clinical criteria for the identification of lynch syndrome among unselected patients with endometrial cancer. Cancer Prev. Res. 2014, 7, 686–697. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, D.D.; Tan, Y.Y.; Walsh, M.D.; Clendenning, M.; Metcalf, A.M.; Ferguson, K.; Arnold, S.T.; Thompson, B.A.; Lose, F.A.; Parsons, M.T.; et al. Tumor mismatch repair immunohistochemistry and DNA mlh1 methylation testing of patients with endometrial cancer diagnosed at age younger than 60 years optimizes triage for population-level germline mismatch repair gene mutation testing. J. Clin. Oncol. 2014, 32, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Takano, M.; Miyamoto, M.; Sasaki, N.; Goto, T.; Tsuda, H.; Furuya, K. DNA mismatch repair-related protein loss as a prognostic factor in endometrial cancers. J. Gynecol. Oncol. 2015, 26, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Black, D.; Soslow, R.A.; Levine, D.A.; Tornos, C.; Chen, S.C.; Hummer, A.J.; Bogomolniy, F.; Olvera, N.; Barakat, R.R.; Boyd, J. Clinicopathologic significance of defective DNA mismatch repair in endometrial carcinoma. J. Clin. Oncol. 2006, 24, 1745–1753. [Google Scholar] [CrossRef] [PubMed]
- Mackay, H.J.; Gallinger, S.; Tsao, M.S.; McLachlin, C.M.; Tu, D.; Keiser, K.; Eisenhauer, E.A.; Oza, A.M. Prognostic value of microsatellite instability (msi) and pten expression in women with endometrial cancer: Results from studies of the ncic clinical trials group (ncic ctg). Eur. J. Cancer 2010, 46, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Zighelboim, I.; Goodfellow, P.J.; Gao, F.; Gibb, R.K.; Powell, M.A.; Rader, J.S.; Mutch, D.G. Microsatellite instability and epigenetic inactivation of mlh1 and outcome of patients with endometrial carcinomas of the endometrioid type. J. Clin. Oncol. 2007, 25, 2042–2048. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, I.; Martin-Arruti, M.; Lopez-Lopez, E.; Garcia-Orad, A. Lack of association between deficient mismatch repair expression and outcome in endometrial carcinomas of the endometrioid type. Gynecol. Oncol. 2014, 134, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, C.M.; Cohn, D.E.; Hampel, H.; Frankel, W.L.; Jones, D.; McElroy, J.P.; Suarez, A.A.; Zhao, W.; Chen, W.; Salani, R.; et al. Epigenetic silencing of mlh1 in endometrial cancers is associated with larger tumor volume, increased rate of lymph node positivity and reduced recurrence-free survival. Gynecol. Oncol. 2017, 146, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Matei, D.; Fang, F.; Shen, C.; Schilder, J.; Arnold, A.; Zeng, Y.; Berry, W.A.; Huang, T.; Nephew, K.P. Epigenetic resensitization to platinum in ovarian cancer. Cancer Res. 2012, 72, 2197–2205. [Google Scholar] [CrossRef] [PubMed]
- Miladi-Abdennadher, I.; Abdelmaksoud-Damak, R.; Ayadi, L.; Khabir, A.; Frikha, F.; Kallel, L.; Frikha, M.; Sellami-Boudawara, T.; Gargouri, A.; Mokdad-Gargouri, R. Aberrant methylation of hmlh1 and p16ink4a in tunisian patients with sporadic colorectal adenocarcinoma. Biosci. Rep. 2011, 31, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Rivlin, N.; Brosh, R.; Oren, M.; Rotter, V. Mutations in the p53 tumor suppressor gene: Important milestones at the various steps of tumorigenesis. Genes Cancer 2011, 2, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Pakish, J.B.; Zhang, Q.; Chen, Z.; Liang, H.; Chisholm, G.B.; Yuan, Y.; Mok, S.C.; Broaddus, R.R.; Lu, K.H.; Yates, M.S. Immune microenvironment in microsatellite-instable endometrial cancers: Hereditary or sporadic origin matters. Clin. Cancer Res. 2017, 23, 4473–4481. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Riella, L.V.; Chock, S.; Liu, T.; Zhao, X.; Yuan, X.; Paterson, A.M.; Watanabe, T.; Vanguri, V.; Yagita, H.; et al. The novel costimulatory programmed death ligand 1/b7.1 pathway is functional in inhibiting alloimmune responses in vivo. J. Immunol. 2011, 187, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Alsaab, H.O.; Sau, S.; Alzhrani, R.; Tatiparti, K.; Bhise, K.; Kashaw, S.K.; Iyer, A.K. Pd-1 and pd-l1 checkpoint signaling inhibition for cancer immunotherapy: Mechanism, combinations, and clinical outcome. Front. Pharmacol. 2017, 8, 561. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Soria, J.-C.; Kowanetz, M.; Fine, G.D.; Hamid, O.; Gordon, M.S.; Sosman, J.A.; McDermott, D.F.; Powderly, J.D.; Gettinger, S.N.; et al. Predictive correlates of response to the anti-pd-l1 antibody mpdl3280a in cancer patients. Nature 2014, 515, 563. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. Pd-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [PubMed]
- Vanderstraeten, A.; Luyten, C.; Verbist, G.; Tuyaerts, S.; Amant, F. Mapping the immunosuppressive environment in uterine tumors: Implications for immunotherapy. Cancer Immunol. Immunother. 2014, 63, 545–557. [Google Scholar] [CrossRef] [PubMed]
- Ott, P.A.; Bang, Y.J.; Berton-Rigaud, D.; Elez, E.; Pishvaian, M.J.; Rugo, H.S.; Puzanov, I.; Mehnert, J.M.; Aung, K.L.; Lopez, J.; et al. Safety and antitumor activity of pembrolizumab in advanced programmed death ligand 1-positive endometrial cancer: Results from the keynote-028 study. J. Clin. Oncol. 2017, 35, 2535–2541. [Google Scholar] [CrossRef] [PubMed]
- Yemelyanova, A.; Vang, R.; Kshirsagar, M.; Lu, D.; Marks, M.A.; Shih, I.M.; Kurman, R.J. Immunohistochemical staining patterns of p53 can serve as a surrogate marker for tp53 mutations in ovarian carcinoma: An immunohistochemical and nucleotide sequencing analysis. Mod. Pathol. 2011, 24, 1248–1253. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Number | % |
|---|---|---|
| Age (mean ± SD) | 54.0 ± 9.8 | |
| BMI (kg/m2) (mean ± SD) | 25.1 ± 4.9 | |
| Menopausal status | ||
| Pre-menopause | 74 | 43.0 |
| Post-menopause | 98 | 57.0 |
| Parity status | ||
| Nulliparous | 31 | 18.0 |
| Parous | 141 | 82.0 |
| FIGO Stage | ||
| I | 139 | 80.3 |
| II | 12 | 6.9 |
| III | 17 | 9.8 |
| IV | 5 | 2.9 |
| Histology | ||
| Endometrioid | 173 | 100 |
| Tumor grade | ||
| 1 | 89 | 51.7 |
| 2 | 55 | 32.0 |
| 3 | 28 | 16.3 |
| Myometrial invasion | ||
| <1/2 | 117 | 68.4 |
| ≥1/2 | 54 | 31.6 |
| Lymphovascular invasion | ||
| Absent | 139 | 82.7 |
| Present | 29 | 17.3 |
| Lymph node metastasis | ||
| Absent | 159 | 93.0 |
| Present | 12 | 7.0 |
| Tumor size | ||
| ≤2 cm | 35 | 27.6 |
| >2 cm | 92 | 72.4 |
| Postoperative adjuvant therapy | ||
| Not performed | 123 | 71.1 |
| Performed | 50 | 28.9 |
| P53 staining | ||
| Normal (IHC 1+) | 149 | 87.6 |
| Abnormal (IHC 0 or 2+) | 21 | 12.4 |
| Clinicopathologic Variables | MMR Status | PLS or Sporadic Cancer | ||||
|---|---|---|---|---|---|---|
| Proficiency | Deficiency | p-Value * | Sporadic | PLS | p-Value * | |
| n = 128 | n = 45 | n = 146 | n = 27 | |||
| Age | 0.258 | 0.974 | ||||
| <50 | 49(38.3) | 13(28.9) | 53(36.3) | 9(33.3) | ||
| ≥50 | 79(61.7) | 32(71.1) | 93(63.7) | 18(66.7) | ||
| BMI | 0.051 | 0.015 | ||||
| <25 | 64(52.0) | 31(68.9) | 74(52.5) | 21(77.8) | ||
| ≥25 | 59(48.0) | 14(31.1) | 67(47.5) | 6(22.2) | ||
| Menopausal status | 0.010 | 0.051 | ||||
| Pre-menopause | 62(48.8) | 12(26.7) | 67(46.2) | 7(25.9) | ||
| Post-menopause | 65(51.2) | 33(73.3) | 78(53.8) | 20(74.1) | ||
| Parity status | 0.064 | 0.052 | ||||
| Nulliparous | 27(21.3) | 4(8.9) | 30(20.7) | 1(3.7) | ||
| Parous | 100(78.7) | 41(91.1) | 115(79.3) | 26(96.3) | ||
| FIGO Stage | 0.014 | 0.028 | ||||
| I | 108(84.4) | 31(68.9) | 121(82.9) | 18(66.7) | ||
| II | 9(7.0) | 3(6.7) | 10(6.8) | 2(7.4) | ||
| III | 8(6.3) | 9(20.0) | 12(8.2) | 5(18.5) | ||
| IV | 3(2.3) | 2(4.4) | 3(2.1) | 2(7.4) | ||
| Tumor grade | 0.011 | 0.213 | ||||
| 1 | 73(57.5) | 16(35.6) | 78(53.8) | 11(40.7) | ||
| 2–3 | 54(42.5) | 29(64.4) | 67(46.2) | 16(59.3) | ||
| Myometrial invasion | 0.157 | 0.264 | ||||
| <1/2 | 90(71.4) | 27(60.0) | 101(70.1) | 16(59.3) | ||
| ≥1/2 | 36(28.6) | 18(40.0) | 43(29.9) | 11(40.7) | ||
| Lymphovascular invasion | 0.003 | 0.055 | ||||
| Absent | 109(87.9) | 30(68.2) | 121(85.2) | 18(69.2) | ||
| Present | 15(12.1) | 14(31.8) | 21(14.8) | 8(30.8) | ||
| Lymph node metastasis | 0.083 | 0.407 | ||||
| Absent | 120(95.2) | 39(86.7) | 135(93.8) | 24(88.9) | ||
| Present | 6(4.8) | 6(13.3) | 9(6.3) | 3(11.1) | ||
| Tumor size | 0.539 | 0.242 | ||||
| ≤2 cm | 27(29.0) | 8(23.5) | 28(25.5) | 7(41.2) | ||
| >2 cm | 66(71.0) | 26(76.5) | 82(74.5) | 10(58.8) | ||
| Postoperative adjuvant therapy | 0.007 | 0.016 | ||||
| Not performed | 98(76.6) | 25(5.6) | 109(74.7) | 14(51.9) | ||
| Performed | 30(23.4) | 20(44.4) | 37(25.3) | 13(48.1) | ||
| P53 staining | 0.867 | 0.743 | ||||
| Normal (IHC 1+) | 111(87.4) | 38(88.4) | 128(88.3) | 21(84.0) | ||
| Abnormal (IHC 0 or 2+) | 16(12.6) | 5(11.6) | 17(11.7) | 4(16.0) | ||
| Variable | MMR Status | ||
|---|---|---|---|
| Proficiency Mean ± SD (n = 128) | Deficiency Mean ± SD (n = 45) | p-Value | |
| Tumor-infiltrating lymphocytes/10HPFs | 59.62 ± 44.55 | 125.52 ± 127 | 0.002 |
| Peritumoral CD8+ T lymphocytes/10FPFs | 157.55 ± 101.68 | 295.69 ± 221.73 | 0.001 |
| Peritumoral PD-1+ immune cells (%) | 12.17 ± 11.39 | 22.22 ± 12.23 | <0.001 |
| Peritumoral PD-L1+ immune cells (%) | 6.21 ± 6.85 | 21.89 ± 14.44 | <0.001 |
| Tumor cell PD-L1+ cells (%) | 1.19 ± 4.81 | 2.79 ± 7.69 | 0.256 |
| Variable | PLS or Sporadic Cancer | ||
| Sporadic Mean ± SD (n = 146) | PLS Mean ± SD (n = 27) | p-Value | |
| Tumor-infiltrating lymphocytes/10HPFs | 62.55 ± 46.49 | 155.27 ± 152.98 | 0.005 |
| Peritumoral CD8+ T lymphocytes/10FPFs | 163.9 ± 105.44 | 352.14 ± 252.75 | 0.002 |
| Peritumoral PD-1+ immune cells (%) | 13.02 ± 11.49 | 24.48 ± 12.82 | <0.001 |
| Peritumoral PD-L1+ immune cells (%) | 7.24 ± 7.92 | 26.93 ± 14.47 | <0.001 |
| Tumor cell PD-L1+ cells (%) | 1.11 ± 4.51 | 4.29 ± 9.7 | 0.155 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Kong, J.K.; Yang, W.; Cho, H.; Chay, D.B.; Lee, B.H.; Cho, S.J.; Hong, S.; Kim, J.-H. DNA Mismatch Repair Protein Immunohistochemistry and MLH1 Promotor Methylation Testing for Practical Molecular Classification and the Prediction of Prognosis in Endometrial Cancer. Cancers 2018, 10, 279. https://doi.org/10.3390/cancers10090279
Kim J, Kong JK, Yang W, Cho H, Chay DB, Lee BH, Cho SJ, Hong S, Kim J-H. DNA Mismatch Repair Protein Immunohistochemistry and MLH1 Promotor Methylation Testing for Practical Molecular Classification and the Prediction of Prognosis in Endometrial Cancer. Cancers. 2018; 10(9):279. https://doi.org/10.3390/cancers10090279
Chicago/Turabian StyleKim, Jisup, Jin Kyoung Kong, Wookyeom Yang, Hanbyoul Cho, Doo Byung Chay, Bang Hyun Lee, Seong Jin Cho, Soonwon Hong, and Jae-Hoon Kim. 2018. "DNA Mismatch Repair Protein Immunohistochemistry and MLH1 Promotor Methylation Testing for Practical Molecular Classification and the Prediction of Prognosis in Endometrial Cancer" Cancers 10, no. 9: 279. https://doi.org/10.3390/cancers10090279
APA StyleKim, J., Kong, J. K., Yang, W., Cho, H., Chay, D. B., Lee, B. H., Cho, S. J., Hong, S., & Kim, J.-H. (2018). DNA Mismatch Repair Protein Immunohistochemistry and MLH1 Promotor Methylation Testing for Practical Molecular Classification and the Prediction of Prognosis in Endometrial Cancer. Cancers, 10(9), 279. https://doi.org/10.3390/cancers10090279