Validation of Immunohistochemistry for the Detection of BRAF V600E-Mutated Lung Adenocarcinomas

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Clinical and Pathological Characteristics of BRAF V600E Mutation-Positive Patients with Lung ADC
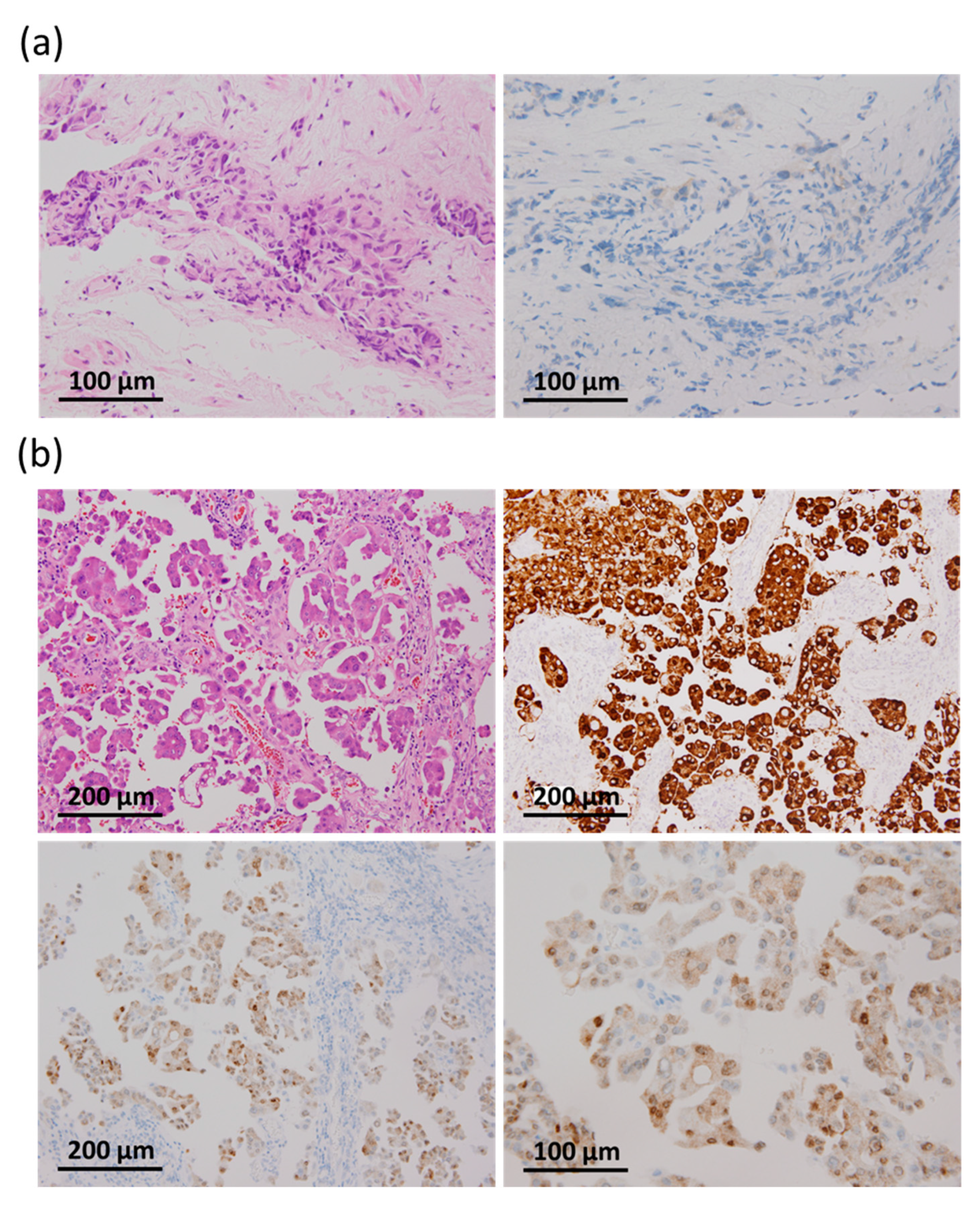
2.2. Sensitivity of BRAF V600E (VE1) IHC: Results from 29 BRAF V600-Mutated Lung Cancers
2.3. Specificity of BRAF V600E (VE1) IHC: Results from 70 Lung Cancers without BRAF V600E Mutations
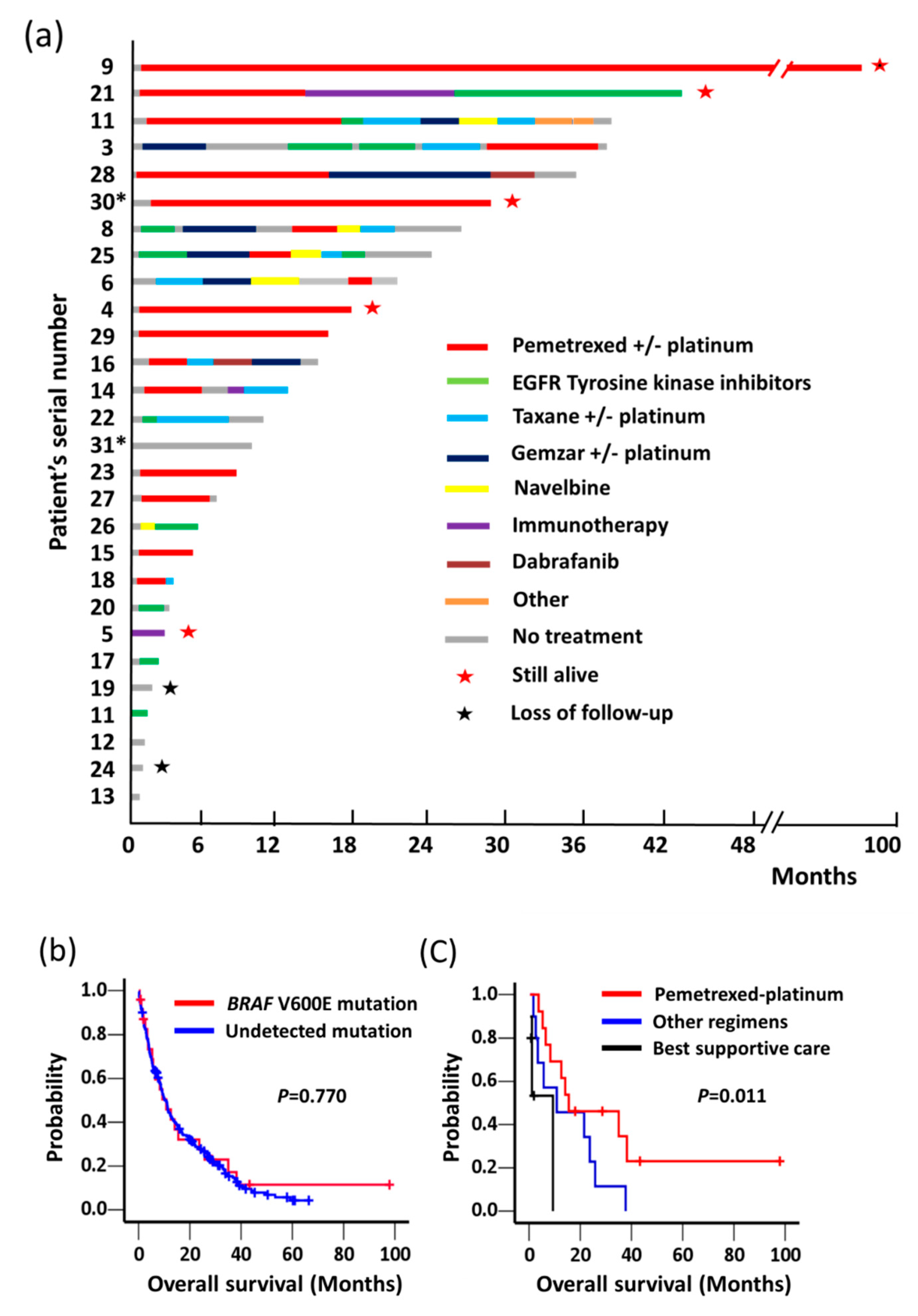
2.4. Clinical Outcomes of BRAF V600E-Mutated Lung ADCs without BRAF-Targeted Therapy
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Mutation Analyses
4.3. Immunohistochemistry
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lynch, T.J.; Bell, D.W.; Sordella, R.; Gurubhagavatula, S.; Okimoto, R.A.; Brannigan, B.W.; Harris, P.L.; Haserlat, S.M.; Supko, J.G.; Haluska, F.G.; et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N. Engl. J. Med. 2004, 350, 2129–2139. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Ou, S.H.; Bang, Y.J.; Camidge, D.R.; Solomon, B.J.; Salgia, R.; Riely, G.J.; Varella-Garcia, M.; Shapiro, G.I.; Costa, D.B.; et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N. Engl. J. Med. 2014, 371, 1963–1971. [Google Scholar] [CrossRef] [PubMed]
- Brose, M.S.; Volpe, P.; Feldman, M.; Kumar, M.; Rishi, I.; Gerrero, R.; Einhorn, E.; Herlyn, M.; Minna, J.; Nicholson, A.; et al. BRAF and RAS mutations in human lung cancer and melanoma. Cancer Res. 2002, 62, 6997–7000. [Google Scholar] [PubMed]
- Cantwell-Dorris, E.R.; O’Leary, J.J.; Sheils, O.M. BRAFV600E: Implications for carcinogenesis and molecular therapy. Mol. Cancer Ther. 2011, 10, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Kris, M.G.; Johnson, B.E.; Berry, L.D.; Kwiatkowski, D.J.; Iafrate, A.J.; Wistuba, I.I.; Varella-Garcia, M.; Franklin, W.A.; Aronson, S.L.; Su, P.F.; et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA 2014, 311, 1998–2006. [Google Scholar] [CrossRef] [PubMed]
- Beeram, M.; Patnaik, A.; Rowinsky, E.K. Raf: A strategic target for therapeutic development against cancer. J. Clin. Oncol. 2005, 23, 6771–6790. [Google Scholar] [CrossRef]
- Mason, C.S.; Springer, C.J.; Cooper, R.G.; Superti-Furga, G.; Marshall, C.J.; Marais, R. Serine and tyrosine phosphorylations cooperate in Raf-1, but not B-Raf activation. EMBO J. 1999, 18, 2137–2148. [Google Scholar] [CrossRef] [Green Version]
- Ji, H.; Wang, Z.; Perera, S.A.; Li, D.; Liang, M.C.; Zaghlul, S.; McNamara, K.; Chen, L.; Albert, M.; Sun, Y.; et al. Mutations in BRAF and KRAS converge on activation of the mitogen-activated protein kinase pathway in lung cancer mouse models. Cancer Res. 2007, 67, 4933–4939. [Google Scholar] [CrossRef]
- Odogwu, L.; Mathieu, L.; Blumenthal, G.; Larkins, E.; Goldberg, K.B.; Griffin, N.; Bijwaard, K.; Lee, E.Y.; Philip, R.; Jiang, X.; et al. FDA Approval Summary: Dabrafenib and Trametinib for the Treatment of Metastatic Non-Small Cell Lung Cancers Harboring BRAF V600E Mutations. Oncologist 2018, 23, 740–745. [Google Scholar] [CrossRef]
- Ritterhouse, L.L.; Barletta, J.A. BRAF V600E mutation-specific antibody: A review. Semin. Diagn. Pathol. 2015, 32, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Wilmott, J.S.; Capper, D.; Preusser, M.; Zhang, Y.E.; Thompson, J.F.; Kefford, R.F.; von Deimling, A.; Scolyer, R.A. Immunohistochemistry is highly sensitive and specific for the detection of V600E BRAF mutation in melanoma. Am. J. Surg. Pathol. 2013, 37, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Koperek, O.; Kornauth, C.; Capper, D.; Berghoff, A.S.; Asari, R.; Niederle, B.; von Deimling, A.; Birner, P.; Preusser, M. Immunohistochemical detection of the BRAF V600E-mutated protein in papillary thyroid carcinoma. Am. J. Surg. Pathol. 2012, 36, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Sinicrope, F.A.; Smyrk, T.C.; Tougeron, D.; Thibodeau, S.N.; Singh, S.; Muranyi, A.; Shanmugam, K.; Grogan, T.M.; Alberts, S.R.; Shi, Q. Mutation-specific antibody detects mutant BRAFV600E protein expression in human colon carcinomas. Cancer 2013, 119, 2765–2770. [Google Scholar] [CrossRef] [PubMed]
- Bledsoe, J.R.; Kamionek, M.; Mino-Kenudson, M. BRAF V600E immunohistochemistry is reliable in primary and metastatic colorectal carcinoma regardless of treatment status and shows high intratumoral homogeneity. Am. J. Surg. Pathol. 2014, 38, 1418–1428. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Shimizu, S.; Tani, Y.; Shitara, M.; Okuda, K.; Hikosaka, Y.; Moriyama, S.; Yano, M.; Fujii, Y. Usefulness of immunohistochemistry for the detection of the BRAF V600E mutation in Japanese lung adenocarcinoma. Lung Cancer 2013, 82, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Long, E.; Hofman, V.; Dadone, B.; Marquette, C.H.; Mouroux, J.; Vignaud, J.M.; Begueret, H.; Merlio, J.P.; Capper, D.; et al. Diagnostic value of immunohistochemistry for the detection of the BRAFV600E mutation in primary lung adenocarcinoma Caucasian patients. Ann. Oncol. 2013, 24, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Litvak, A.M.; Paik, P.K.; Woo, K.M.; Sima, C.S.; Hellmann, M.D.; Arcila, M.E.; Ladanyi, M.; Rudin, C.M.; Kris, M.G.; Riely, G.J. Clinical characteristics and course of 63 patients with BRAF mutant lung cancers. J. Thorac. Oncol. 2014, 9, 1669–1674. [Google Scholar] [CrossRef] [PubMed]
- Leonetti, A.; Facchinetti, F.; Rossi, G.; Minari, R.; Conti, A.; Friboulet, L.; Tiseo, M.; Planchard, D. BRAF in non-small cell lung cancer (NSCLC): Pickaxing another brick in the wall. Cancer Treat. Rev. 2018, 66, 82–94. [Google Scholar] [CrossRef]
- McEvoy, S.H.; Halpenny, D.F.; Viteri-Jusue, A.; Hayes, S.A.; Plodkowski, A.J.; Riely, G.J.; Ginsberg, M.S. Investigation of patterns of nodal metastases in BRAF mutant lung cancer. Lung Cancer 2017, 108, 62–65. [Google Scholar] [CrossRef]
- Capper, D.; Preusser, M.; Habel, A.; Sahm, F.; Ackermann, U.; Schindler, G.; Pusch, S.; Mechtersheimer, G.; Zentgraf, H.; von Deimling, A. Assessment of BRAF V600E mutation status by immunohistochemistry with a mutation-specific monoclonal antibody. Acta Neuropathol. 2011, 122, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Ida, C.M.; Vrana, J.A.; Rodriguez, F.J.; Jentoft, M.E.; Caron, A.A.; Jenkins, S.M.; Giannini, C. Immunohistochemistry is highly sensitive and specific for detection of BRAF V600E mutation in pleomorphic xanthoastrocytoma. Acta Neuropathol. Commun. 2013, 1, 20. [Google Scholar] [CrossRef] [PubMed]
- Brastianos, P.K.; Taylor-Weiner, A.; Manley, P.E.; Jones, R.T.; Dias-Santagata, D.; Thorner, A.R.; Lawrence, M.S.; Rodriguez, F.J.; Bernardo, L.A.; Schubert, L.; et al. Exome sequencing identifies BRAF mutations in papillary craniopharyngiomas. Nat. Genet. 2014, 46, 161–165. [Google Scholar] [CrossRef]
- Tiacci, E.; Trifonov, V.; Schiavoni, G.; Holmes, A.; Kern, W.; Martelli, M.P.; Pucciarini, A.; Bigerna, B.; Pacini, R.; Wells, V.A.; et al. BRAF mutations in hairy-cell leukemia. N. Engl. J. Med. 2011, 364, 2305–2315. [Google Scholar] [CrossRef] [PubMed]
- Brown, N.A.; Rolland, D.; McHugh, J.B.; Weigelin, H.C.; Zhao, L.; Lim, M.S.; Elenitoba-Johnson, K.S.; Betz, B.L. Activating FGFR2-RAS-BRAF mutations in ameloblastoma. Clin. Cancer Res. 2014, 20, 5517–5526. [Google Scholar] [CrossRef] [PubMed]
- Bosmuller, H.; Fischer, A.; Pham, D.L.; Fehm, T.; Capper, D.; von Deimling, A.; Bonzheim, I.; Staebler, A.; Fend, F. Detection of the BRAF V600E mutation in serous ovarian tumors: A comparative analysis of immunohistochemistry with a mutation-specific monoclonal antibody and allele-specific PCR. Hum. Pathol. 2013, 44, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, A.; Felicioni, L.; Malatesta, S.; Grazia Sciarrotta, M.; Guetti, L.; Chella, A.; Viola, P.; Pullara, C.; Mucilli, F.; Buttitta, F. Clinical features and outcome of patients with non-small-cell lung cancer harboring BRAF mutations. J. Clin. Oncol. 2011, 29, 3574–3579. [Google Scholar] [CrossRef]
- Cui, G.; Liu, D.; Li, W.; Fu, X.; Liang, Y.; Li, Y.; Shi, W.; Chen, X.; Zhao, S. A meta-analysis of the association between BRAF mutation and nonsmall cell lung cancer. Medicine 2017, 96, e6552. [Google Scholar] [CrossRef]
- Kamiya, K.; Hayashi, Y.; Douguchi, J.; Hashiguchi, A.; Yamada, T.; Izumi, Y.; Watanabe, M.; Kawamura, M.; Horinouchi, H.; Shimada, N.; et al. Histopathological features and prognostic significance of the micropapillary pattern in lung adenocarcinoma. Mod. Pathol. 2008, 21, 992–1001. [Google Scholar] [CrossRef] [Green Version]
- Yousem, S.A.; Nikiforova, M.; Nikiforov, Y. The histopathology of BRAF-V600E-mutated lung adenocarcinoma. Am. J. Surg. Pathol. 2008, 32, 1317–1321. [Google Scholar] [CrossRef]
- Cardarella, S.; Ogino, A.; Nishino, M.; Butaney, M.; Shen, J.; Lydon, C.; Yeap, B.Y.; Sholl, L.M.; Johnson, B.E.; Janne, P.A. Clinical, pathologic, and biologic features associated with BRAF mutations in non-small cell lung cancer. Clin. Cancer Res. 2013, 19, 4532–4540. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Besse, B.; Groen, H.J.M.; Souquet, P.J.; Quoix, E.; Baik, C.S.; Barlesi, F.; Kim, T.M.; Mazieres, J.; Novello, S.; et al. Dabrafenib plus trametinib in patients with previously treated BRAF(V600E)-mutant metastatic non-small cell lung cancer: An open-label, multicentre phase 2 trial. Lancet Oncol. 2016, 17, 984–993. [Google Scholar] [CrossRef]
- Chen, Q.; Jain, N.; Ayer, T.; Wierda, W.G.; Flowers, C.R.; O’Brien, S.M.; Keating, M.J.; Kantarjian, H.M.; Chhatwal, J. Economic Burden of Chronic Lymphocytic Leukemia in the Era of Oral Targeted Therapies in the United States. J. Clin. Oncol. 2017, 35, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.G.; Biesma, B.; Heigener, D.; von Pawel, J.; Eisen, T.; Bennouna, J.; Zhang, L.; Liao, M.; Sun, Y.; Gans, S.; et al. Phase III, randomized, double-blind, placebo-controlled trial of gemcitabine/cisplatin alone or with sorafenib for the first-line treatment of advanced, nonsquamous non-small-cell lung cancer. J. Clin. Oncol. 2012, 30, 3084–3092. [Google Scholar] [CrossRef] [PubMed]
- Tissot, C.; Couraud, S.; Tanguy, R.; Bringuier, P.P.; Girard, N.; Souquet, P.J. Clinical characteristics and outcome of patients with lung cancer harboring BRAF mutations. Lung Cancer 2016, 91, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Zhang, Z.; Jiang, T.; Li, X.; Zhao, C.; Su, B.; Zhou, C. Clinicopathologic characteristics and outcomes of Chinese patients with non-small-cell lung cancer and BRAF mutation. Cancer Med. 2017, 6, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.; Bauml, J.; Forde, P.M.; Davis, K.L.; Myall, N.J.; Sasane, M.; Dalal, A.; Culver, K.; Wozniak, A.J.; Baik, C.S.; et al. Real-world treatment patterns and survival of patients with BRAF V600-mutated metastatic non-small cell lung cancer. Lung Cancer 2019, 128, 74–90. [Google Scholar] [CrossRef]
- Gautschi, O.; Milia, J.; Cabarrou, B.; Bluthgen, M.V.; Besse, B.; Smit, E.F.; Wolf, J.; Peters, S.; Fruh, M.; Koeberle, D.; et al. Targeted Therapy for Patients with BRAF-Mutant Lung Cancer: Results from the European EURAF Cohort. J. Thorac. Oncol. 2015, 10, 1451–1457. [Google Scholar] [CrossRef]
- Nakanishi, Y.; Nakagawa, Y.; Tsujino, I.; Shimizu, T.; Takahashi, N.; Hashimoto, S.; Masuda, S. Favorable Outcome With Pemetrexed Treatment for Advanced BRAF-V600E-Positive Lung Adenocarcinoma in a Patient Followed up Over 8 Years. J. Thorac. Oncol. 2018, 13, e199–e202. [Google Scholar] [CrossRef] [Green Version]
- Gow, C.H.; Hsieh, M.S.; Wu, S.G.; Shih, J.Y. A comprehensive analysis of clinical outcomes in lung cancer patients harboring a MET exon 14 skipping mutation compared to other driver mutations in an East Asian population. Lung Cancer 2017, 103, 82–89. [Google Scholar] [CrossRef]
- Rami-Porta, R.; Ball, D.; Crowley, J.; Giroux, D.J.; Jett, J.; Travis, W.D.; Tsuboi, M.; Vallieres, E.; Goldstraw, P.; International Staging, C.; et al. The IASLC Lung Cancer Staging Project: Proposals for the revision of the T descriptors in the forthcoming (seventh) edition of the TNM classification for lung cancer. J. Thorac. Oncol. 2007, 2, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.G.; Liu, Y.N.; Yu, C.J.; Yang, J.C.; Shih, J.Y. Driver mutations of young lung adenocarcinoma patients with malignant pleural effusion. Genes Chromosomes Cancer 2018, 57, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Gow, C.H.; Chang, H.T.; Lim, C.K.; Liu, C.Y.; Chen, J.S.; Shih, J.Y. Comparable clinical outcomes in patients with HER2-mutant and EGFR-mutant lung adenocarcinomas. Genes Chromosomes Cancer 2017, 56, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.F.; Hsieh, M.S.; Wu, S.G.; Chang, Y.L.; Yu, C.J.; Yang, J.C.; Yang, P.C.; Shih, J.Y. Efficacy of Pemetrexed-Based Chemotherapy in Patients with ROS1 Fusion-Positive Lung Adenocarcinoma Compared with in Patients Harboring Other Driver Mutations in East Asian Populations. J. Thorac. Oncol. 2016, 11, 1140–1152. [Google Scholar] [CrossRef] [PubMed]
- To, K.F.; Tong, J.H.; Yeung, K.S.; Lung, R.W.; Law, P.P.; Chau, S.L.; Kang, W.; Tong, C.Y.; Chow, C.; Chan, A.W.; et al. Detection of ALK rearrangement by immunohistochemistry in lung adenocarcinoma and the identification of a novel EML4-ALK variant. J. Thorac. Oncol. 2013, 8, 883–891. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristic | BRAF V600E | Non-BRAF V600E | p-Value # |
|---|---|---|---|
| Patients, n | 31 | 700 | |
| Age, years | |||
| Median (range) | 67.0 (33–87) | 65.7 (27–93) | 0.455 |
| >70, n (%) | 14 (45) | 268 (38) | |
| Gender, n (%) | |||
| M | 16 (52) | 381 (54) | |
| F | 15 (48) | 319 (46) | 0.854 |
| Smokers, n (%) | 12 (39) | 267 (38) | |
| Pack-years, average/SD | 40/26 | N/A | 1.000 |
| ECOG PS, n (%) | |||
| 0−1 | 21 (68) | 589 (84) | |
| 2−4 | 10 (32) | 111 (16) | 0.024 * |
| Stage, n (%) | |||
| I−IIIB | 7 (23) | 228 (33) | |
| IV | 24 (77) | 472 (67) | 0.245 |
| Metastatic sites | |||
| 0−1 | 14 (58) | 255 (54) | |
| ≥2 | 10 (42) | 217 (46) | 0.834 |
| Patient’s Serial No. | Age, Years | Sex | Sample | Stage | Histological Pattern | Grade a | IHC Score b | IHC Positive Percentage |
|---|---|---|---|---|---|---|---|---|
| 1 | 61 | F | SUR | IIIA | Acinar | 2 | 2+ | 100% |
| 2 | 80 | F | SUR | IB | Acinar | 2 | 1+ | 70% |
| 3 | 66 | M | SUR | IIIA | Micropapillary | 3 | 1+ | 80% |
| 4 | 61 | F | SUR | IIIA | Micropapillary | 3 | 2+ | 70% |
| 5 | 54 | F | SUR | IIIA | Micropapillary | 3 | 3+ | 100% |
| 6 | 71 | M | SUR | IIIB | Micropapillary | 3 | 3+ | 100% |
| 7 | 59 | F | SUR | IB | Papillary | 2 | 1+ | 60% |
| 8 | 67 | M | Bron B | IV | Micropapillary | 3 | 1+ | 10% |
| 9 | 49 | M | Bron B | IV | Micropapillary | 3 | 2+ | 70% |
| 10 | 67 | M | Bron B | IV | Micropapillary | 3 | 2+ | 75% |
| 11 | 67 | M | Echo B | IV | Micropapillary | 3 | 2+ | 75% |
| 12 | 55 | M | Echo B | IV | Micropapillary | 3 | 3+ | 90% |
| 13 | 85 | F | Echo B | IV | Solid | 3 | 2+ | 95% |
| 14 | 65 | F | LN | IV | Micropapillary | 3 | 1+ | 100% |
| 15 | 67 | M | LN | IV | Micropapillary | 3 | 2+ | 95% |
| 16 | 71 | F | LN | IV | Micropapillary | 3 | 3+ | 100% |
| 17 | 87 | F | LN | IV | Solid | 3 | 3+ | 95% |
| 18 | 65 | F | LN | IV | Solid | 3 | 3+ | 100% |
| 19 | 50 | M | Bone | IV | Acinar | 2 | 3+ | 90% |
| 20 | 69 | F | MPE | IV | Micropapillary | N/A | 1+ | 75% |
| 21 | 78 | F | MPE | IV | Micropapillary | N/A | 2+ | 90% |
| 22 | 74 | F | MPE | IV | Micropapillary | N/A | 1+ | 80% |
| 23 | 85 | M | MPE | IV | Micropapillary | N/A | 1+ | 90% |
| 24 | 85 | M | MPE | IV | Micropapillary | N/A | 2+ | 80% |
| 25 | 40 | M | MPE | IV | Micropapillary | N/A | 2+ | 95% |
| 26 | 78 | F | MPE | IV | Micropapillary | N/A | 3+ | 90% |
| 27 | 78 | M | MPE | IV | Micropapillary | N/A | 3+ | 95% |
| 28 | 78 | M | MPE | IV | Micropapillary | N/A | 3+ | 100% |
| 29 | 67 | M | MPE | IV | Micropapillary | N/A | 3+ | 100% |
| Driver Gene Alteration (Case Numbers) | Gene Alteration (Numbers) | Mutation Detection Methods | BRAF (VE1) IHC Positive * (Numbers) | Positive % |
|---|---|---|---|---|
| BRAF V600E (29) | V600E (29) | Sequencing | 28 a | 97 |
| BRAF non-V600E (8) | G469A (3) G469V (1) K483E (1) D594G (2) L597R (1) | Sequencing | 0 | 0 |
| EGFR (14) | exon 18 G719A (2) exon 19 deletion (4) del L747-A750insP (1) del E746-A750 (2) del E746-S752insV (1) exon 21 L858R (7) exon 21 L861Q (1) | Sequencing | 0 | 0 |
| KRAS (9) | G12A (1) G12C (3) G12D (2) G12V (2) G12R (1) | Sequencing | 0 | 0 |
| ALK fusion (10) | ALK IHC positive (5) EML4-ALK fusion (5) | IHC Sequencing | 1b | 10 |
| ROS1 fusion (5) | ROS1 FISH positive (4) CD74 exon6-ROS1 exon34 (1) | FISH Sequencing | 0c | 0 |
| RET fusion (4) | KIF5B exon15-RET exon12 (2) CCDC exon1-RET exon12 (1) CCDC exon5-RET exon11 (1) | Sequencing | 0 | 0 |
| HER2 (5) | A775_G776insYVMA (4) P780_Y781insGSP (1) | Sequencing | 0 | 0 |
| MET (5) | exon 14 skipping (5) | Sequencing | 0 | 0 |
| Undetected mutation # (10) | No mutation/fusion detected (10) | Sequencing | 0 | 0 |
| Study | Sensitivity | Specificity | Cases for IHC | Assay |
|---|---|---|---|---|
| Sasaki et al. [16] | 5/5 (100%) | 20/21 (95.2%) | BRAF V600E BRAF non-V600E mutations | VE1 Ab, Dako EnVisionTM ELEX detection system |
| Ilie et al. [17] | 19/21 (90.5%) | 19/19 (100%) | BRAF V600E BRAF non-V600E mutations | VE1 Ab, Ventana Medical Systems |
| This study | 28/29 (96.6%) | 69/70 (98.6%) | BRAF V600E BRAF non-V600E mutations EGFR, KRAS, HER2, METΔ14, ALK, ROS1, or RET mutations Undetected mutation # | VE1 Ab, Ventana Medical Systems |
| Total | 52/55 (94.5%) | 108/110 (98.2%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gow, C.-H.; Hsieh, M.-S.; Lin, Y.-T.; Liu, Y.-N.; Shih, J.-Y. Validation of Immunohistochemistry for the Detection of BRAF V600E-Mutated Lung Adenocarcinomas. Cancers 2019, 11, 866. https://doi.org/10.3390/cancers11060866
Gow C-H, Hsieh M-S, Lin Y-T, Liu Y-N, Shih J-Y. Validation of Immunohistochemistry for the Detection of BRAF V600E-Mutated Lung Adenocarcinomas. Cancers. 2019; 11(6):866. https://doi.org/10.3390/cancers11060866
Chicago/Turabian StyleGow, Chien-Hung, Min-Shu Hsieh, Yen-Ting Lin, Yi-Nan Liu, and Jin-Yuan Shih. 2019. "Validation of Immunohistochemistry for the Detection of BRAF V600E-Mutated Lung Adenocarcinomas" Cancers 11, no. 6: 866. https://doi.org/10.3390/cancers11060866
APA StyleGow, C.-H., Hsieh, M.-S., Lin, Y.-T., Liu, Y.-N., & Shih, J.-Y. (2019). Validation of Immunohistochemistry for the Detection of BRAF V600E-Mutated Lung Adenocarcinomas. Cancers, 11(6), 866. https://doi.org/10.3390/cancers11060866