Real-World Outcomes and Prognostic Factors in Patients Receiving Nivolumab Therapy for Recurrent or Metastatic Head and Neck Carcinoma

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Treatment Efficacy in All Patients Based on Histological Type
2.3. Treatment-Related Adverse Events
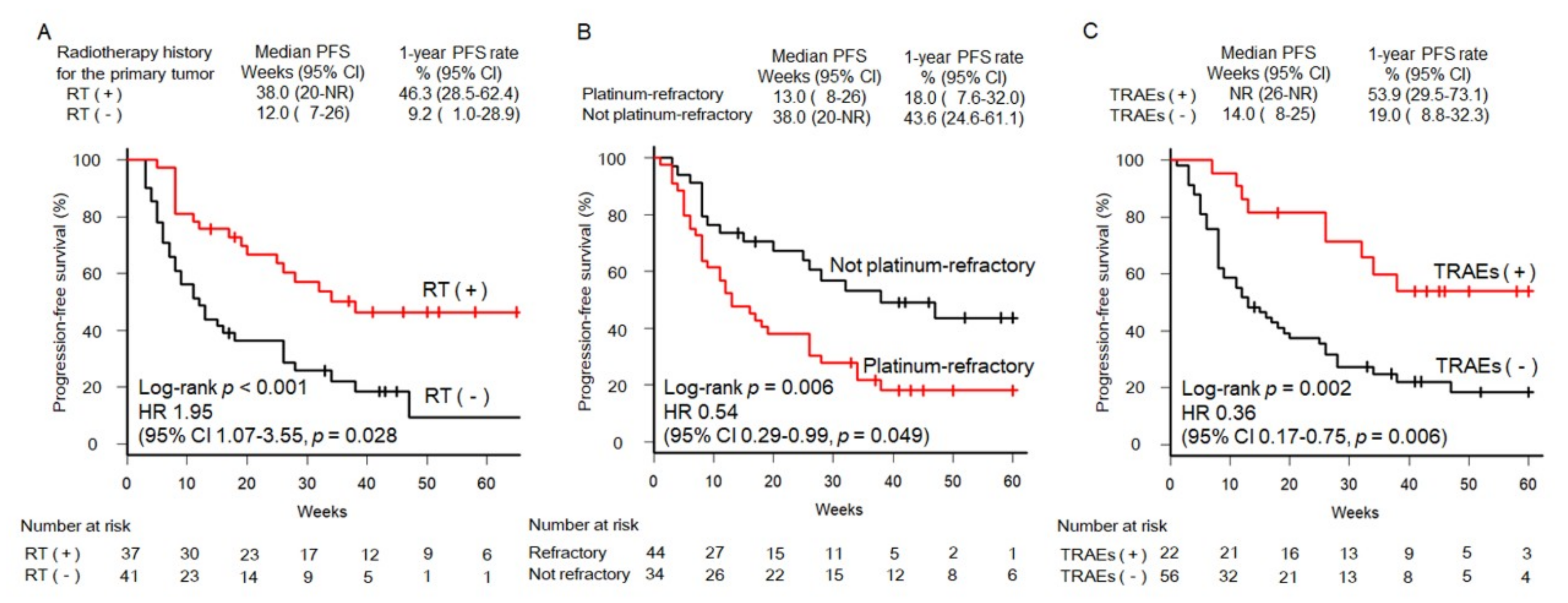
2.4. Association between Prognostic Factors and Treatment Efficacy in Patients with SCCHN
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer. 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Hori, M.; Matsuda, T.; Shibata, A.; Katanoda, K.; Sobue, T.; Nishimoto, H.; Japan Cancer Surveillance Research Group. Cancer incidence and incidence rates in Japan in 2009: A study of 32 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn. J. Clin. Oncol. 2015, 45, 884–891. [Google Scholar] [CrossRef]
- Pignon, J.P.; le Maître, A.; Maillard, E.; Bourhis, J. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefèbvre, J.L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef]
- Cooper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Campbell, B.H.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous cell carcinoma of the head and neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef]
- Ferris, R.L.; Blumenschein, G. Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef]
- Vermorken, J.B.; Mesia, R.; Rivera, F.; Remenar, E.; Kawecki, A.; Rottey, S.; Erfan, J.; Zabolotnyy, D.; Kienzer, H.R.; Cupissol, D.; et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N. Engl. J. Med. 2008, 359, 1116–1127. [Google Scholar] [CrossRef]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Azarnia, N.; Shin, D.M.; Cohen, R.B.; Jones, C.U.; Sur, R.; Raben, D.; Jassem, J.; et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2006, 354, 567–578. [Google Scholar] [CrossRef]
- Takemoto, K.; Miyahara, N.; Chikuie, N.; Hamamoto, T.; Ishino, T.; Ueda, T.; Takeno, S. Efficacy of anti-PD-1 therapy in a patient with brain metastasis of parotid carcinoma: A case report. Auris Nasus Larynx 2018, 46, 813–817. [Google Scholar] [CrossRef]
- Cabezas-Camarero, S.; Puebla, F.; Subhi-Issa, A.I.; Sanz-Ortega, J.; Pérez-Segura, P. Durable response to first-line nivolumab in a patient with oligometastatic PD-L1 positive nasopharyngeal cancer. Oral Oncol. 2018, 87, 204–206. [Google Scholar] [CrossRef]
- Nibu, K.; Hayashi, R.; Asakage, T.; Ojiri, H.; Kimata, Y.; Kodaira, T.; Nagao, T.; Nakashima, T.; Fujii, T.; Fujii, H.; et al. Japanese Clinical Practice Guideline for Head and Neck Cancer. Auris Nasus Larynx 2017, 44, 375–380. [Google Scholar] [CrossRef]
- Gooi, Z.; Fakhry, C.; Goldenberg, D.; Richmon, J.; Kiess, A.P. AHNS Series: Do you know your guidelines? Principles of radiation therapy for head and neck cancer: A review of the National Comprehensive Cancer Network guidelines. Head Neck 2016, 38, 987–992. [Google Scholar] [CrossRef]
- Fulcher, C.D.; Haigentz, M. Jr.; Ow, T.J. Education Committee of the American Head and Neck Society (AHNS). AHNS Series: Do you know your guidelines? Principles of treatment for locally advanced or unresectable head and neck squamous cell carcinoma. Head Neck 2018, 40, 676–686. [Google Scholar] [CrossRef]
- Gill, A.; Vasan, N.; Givi, B.; Joshi, A. AHNS Series: Do you know your guidelines? Evidence-based management of oral cavity cancers. Head Neck 2018, 40, 406–416. [Google Scholar] [CrossRef]
- Byrd, J.K.; Clair, J.M.; El-Sayed, I. AHNS Series: Do you know your guidelines? Principles for treatment of cancer of the paranasal sinuses: A review of the National Comprehensive Cancer Network guidelines. Head Neck 2018, 40, 1889–1896. [Google Scholar] [CrossRef]
- Gooi, Z.; Richmon, J.; Agrawal, N.; Blair, E.; Portugal, L.; Vokes, E.; Seiwert, T.; de Souza, J.; Saloura, V.; Haraf, D.; et al. AHNS Series - Do you know your guidelines? Principles of treatment for nasopharyngeal cancer: A review of the National Comprehensive Cancer Network guidelines. Head Neck 2017, 39, 201–205. [Google Scholar] [CrossRef]
- Guo, T.; Goldenberg, D.; Fakhry, C. AHNS series: Do you know your guidelines? Management of head and neck cancer in the era of human papillomavirus: Educating our patients on human papillomavirus. Head Neck 2017, 39, 833–839. [Google Scholar] [CrossRef]
- Tamaki, A.; Miles, B.A.; Lango, M.; Kowalski, L.; Zender, C.A. AHNS series: Do you know our guidelines? Review of current knowledge on laryngeal cancer. Head Neck 2018, 40, 170–181. [Google Scholar] [CrossRef]
- Mantravadi, A.V.; Moore, M.G.; Rassekh, C.H. AHNS series: Do you know your guidelines? Diagnosis and management of salivary gland tumors. Head Neck 2019, 41, 269–280. [Google Scholar] [CrossRef]
- Eskander, A.; Ghanem, T.; Agrawal, A. Education Committee of American Head and Neck Society (AHNS). AHNS Series: Do you know your guidelines? Guideline recommendations for head and neck cancer of unknown primary site. Head Neck 2018, 40, 614–621. [Google Scholar] [CrossRef]
- Donia, M.; Ellebaek, E.; Øllegaard, T.; Duval, L.; Aaby, J.; Hoejberg, L.; Køhler, U.H.; Schmidt, H.; Bastholt, L.; Svane, I.M. The real-world impact of modern treatments on the survival of patients with metastatic melanoma. Eur. J. Cancer 2018, 108, 25–32. [Google Scholar] [CrossRef]
- Al-Baimani, K.; Jonker, H.; Zhang, T.; Goss, G.D.; Laurie, S.A.; Nicholas, G.; Wheatley-Price, P. Are clinical trial eligibility criteria an accurate reflection of a real-world population of advanced non-small-cell lung cancer patients? Curr. Oncol. 2018, 4, e291–e297. [Google Scholar] [CrossRef]
- Weber, J.S.; D’Angelo, S.P.; Minor, D.; Hodi, F.S.; Gutzmer, R.; Neyns, B.; Hoeller, C.; Khushalani, N.; Miller, W.H.; Lao, C.D.; et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): A randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2015, 16, 375–384. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Accorona, R.; Botti, G.; Farina, D.; Fossati, P.; Gatta, G.; Gogas, H.; Lombardi, D.; Maroldi, R.; Nicolai, P.; et al. Mucosal melanoma of the head and neck. Crit. Rev. Oncol. Hematol. 2017, 112, 136–152. [Google Scholar] [CrossRef]
- Deng, L.; Liang, H.; Burnette, B.; Beckett, M.; Darga, T.; Weichselbaum, R.R.; Fu, X.Y. Irradiation and anti-PD-L1 treatment synergistically promote antitumor immunity in mice. J. Clin. Invest. 2014, 24, 687–695. [Google Scholar] [CrossRef]
- Postow, M.A.; Callahan, M.K.; Barker, C.A.; Yamada, Y.; Yuan, J.; Kitano, S.; Mu, Z.; Rasalan, T.; Adamow, M.; Ritter, E.; et al. Immunologic correlates of the abscopal effect in a patient with melanoma. N. Engl. J. Med. 2012, 366, 925–931. [Google Scholar] [CrossRef]
- Chandra, R.A.; Wilhite, T.J.; Balboni, T.A.; Alexander, B.M.; Spektor, A.; Ott, P.A.; Ng, A.K.; Hodi, F.S.; Schoenfeld, J.D. A systematic evaluation of abscopal responses following radiotherapy in patients with metastatic melanoma treated with ipilimumab. Oncoimmunology 2015, 4, e1046028. [Google Scholar] [CrossRef] [Green Version]
- Grimaldi, A.M.; Simeone, E.; Giannarelli, D.; Muto, P.; Falivene, S.; Borzillo, V.; Giugliano, F.M.; Sandomenico, F.; Petrillo, A.; Curvietto, M.; et al. Abscopal effects of radiotherapy on advanced melanoma patients who progressed after ipilimumab immunotherapy. Oncoimmunology 2014, 3, e28780. [Google Scholar] [CrossRef]
- Ribeiro Gomes, J.; Schmerling, R.A.; Haddad, C.K.; Racy, D.J.; Ferrigno, R.; Gil, E.; Zanuncio, P.; Buzaid, A.C. Analysis of the Abscopal Effect With Anti-PD1 Therapy in Patients With Metastatic Solid Tumors. J. Immunother. 2016, 39, 367–372. [Google Scholar] [CrossRef]
- Kikuchi, M.; Clump, D.A.; Srivastava, R.M.; Sun, L.; Zeng, D.; Diaz-Perez, J.A.; Anderson, C.J.; Edwards, W.; Ferris, R.L. Preclinical immunoPET/CT imaging using Zr-89-labeled anti-PD-L1 monoclonal antibody for assessing radiation-induced PD-L1 upregulation in head and neck cancer and melanoma. Oncoimmunology 2017, 6, e1329071. [Google Scholar] [CrossRef]
- Morisada, M.; Clavijo, P.E.; Moore, E.; Sun, L.; Chamberlin, M.; Van Waes, C.; Hodge, J.W.; Mitchell, J.B.; Friedman, J.; Allen, C.T. PD-1 blockade reverses adaptive immune resistance induced by high-dose hypofractionated but not low-dose daily fractionated radiation. Oncoimmunology 2017, 7, e1395996. [Google Scholar] [CrossRef]
- Sato, K.; Akamatsu, H.; Murakami, E.; Sasaki, S.; Kanai, K.; Hayata, A.; Tokudome, N.; Akamatsu, K.; Koh, Y.; Ueda, H.; et al. Correlation between immune-related adverse events and efficacy in non-small cell lung cancer treated with nivolumab. Lung Cancer 2018, 115, 71–74. [Google Scholar] [CrossRef] [Green Version]
- Haratani, K.; Hayashi, H.; Chiba, Y.; Kudo, K.; Yonesaka, K.; Kato, R.; Kaneda, H.; Hasegawa, Y.; Tanaka, K.; Takeda, M.; et al. Association of immune-related adverse events with nivolumab efficacy in non-small-cell lung cancer. JAMA Oncol. 2018, 4, 374–378. [Google Scholar] [CrossRef]
- Weber, J.S.; Hodi, F.S.; Wolchok, J.D.; Topalian, S.L.; Schadendorf, D.; Larkin, J.; Sznol, M.; Long, G.V.; Li, H.; Waxman, I.M.; et al. Safety Profile of Nivolumab Monotherapy: A Pooled Analysis of Patients With Advanced Melanoma. J. Clin. Oncol. 2017, 35, 785–792. [Google Scholar] [CrossRef]
- Judd, J.; Zibelman, M.; Handorf, E.; O’Neill, J.; Ramamurthy, C.; Bentota, S.; Doyle, J.; Uzzo, R.; Bauman, J.; Borghaei, H.; et al. Immune-Related Adverse Events as a Biomarker in Non-Melanoma Patients Treated with Programmed Cell Death 1 Inhibitors. Oncologist 2017, 22, 1232–1237. [Google Scholar] [CrossRef] [Green Version]
- Rogado, J.; Sánchez-Torres, J.M.; Romero-Laorden, N.; Ballesteros, A.I.; Pacheco-Barcia, V.; Ramos-Leví, A. Immune-related adverse events predict the therapeutic efficacy of anti-PD-1 antibodies in cancer patients. Eur. J. Cancer 2019, 109, 21–27. [Google Scholar] [CrossRef]
- James, D.B.; Mary, K.G.; Christian, W. TNM Classification of Malignant Tumors, 8th ed.; Wiley: Hoboken, NJ, USA, 2017; pp. 17–54. ISBN 978-1-119-26357-9. [Google Scholar]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. American Joint Committee on Cancer (AJCC) Cancer Staging Manual, 8th ed.; Springer: Berlin, Germany, 2017; pp. 55–181. ISBN 978-3-319-40617-6. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (N = 93) | SCCHN Patients a (N = 78) | ||
|---|---|---|---|---|
| Age | ||||
| 75 or higher, n (%) | 15 (16.1) | 11 (14.1) | ||
| <75, n (%) | 78 (83.9) | 67 (85.9) | ||
| Mean ± SD (years) | 64.9 ± 9.9 | 64.9 ± 9.7 | ||
| Sex | ||||
| Male, n (%) | 74 (79.6) | 65 (83.3) | ||
| Female, n (%) | 19 (20.4) | 13 (16.7) | ||
| Smoking status, n (%) | ||||
| (Current or former) Smoker | 58 (62.4) | 49 (62.8) | ||
| Never-smoker | 35 (37.6) | 29 (37.1) | ||
| ECOG PS, n (%) | ||||
| 0 or 1 | 86 (92.5) | 71 (91.0) | ||
| 2 or 3 or 4 | 7 (7.5) | 7 (9.0) | ||
| Primary tumor site, n (%) | ||||
| Pharynx | 45 (48.4) | 39 (50.0) | ||
| 6 (6.5) | 4 (5.1) | 4 (5.0) | ||
| 11 (11.8) | 11 (14.1) | 12 (15.0) | ||
| 26 (28.0) | 24 (30.8) | 25 (31.3) | ||
| Oral cavity | 15 (16.1) | 14 (18.0) | ||
| Larynx | 6 (6.5) | 6 (7.7) | ||
| Salivary gland | 6 (6.5) | - | ||
| Parotid gland | 3 (3.2) | - | ||
| Submandibular gland | 2 (2.2) | - | ||
| Sublingual gland | 1 (1.1) | - | ||
| Nasal cavity and paranasal sinus | 10 (10.8) | 8 (12.8) | ||
| Thyroid gland | 2 (2.2) | 1 (1.3) | ||
| External auditory canal | 3 (3.2) | 3 (3.9) | ||
| Unknown primary | 8 (8.6) | 7 (9.0) | ||
| PD-L1 expression | ||||
| <1% | 5 (5.4) | 5 (6.4) | ||
| 1–10% | 6 (6.5) | 6 (7.7) | ||
| ≥10% | 10 (10.8) | 10 (12.8) | ||
| Not evaluated | 74 (77.9) | 72 (77.4) | ||
| Radiotherapy to the primary tumor, n (%) | ||||
| Radiotherapy (+) | 43 (46.2) | 37 (47.4) | ||
| Radiotherapy (−) | 50 (53.8) | 41 (52.6) | ||
| History of administration of platinum agents for the treatment of primary tumor, n (%) | ||||
| Platinum agents (+) | 60 (64.5) | 52 (66.7) | ||
| Platinum agents (−) | 33 (45.5) | 26 (33.3) | ||
| Site of recurrent or metastatic tumors, n (%) | ||||
| Local primary site | 36 (38.7) | 33 (42.3) | ||
| Lymph nodes | 50 (53.8) | 44 (56.4) | ||
| Lung | 38 (40.9) | 27 (34.6) | ||
| Others | 19 (20.4) | 9 (11.8) | ||
| Treatment of recurrent or metastatic tumors prior to nivolumab therapy, n (%) | ||||
| Chemotherapy | 65 (69.9) | 55 (70.5) | ||
| Number of lines | ||||
| 1 line | 32 (34.4) | 29 (37.2) | ||
| 2 lines | 24 (25.8) | 20 (25.0) | ||
| 3 lines | 9 (9.7) | 6 (7.5) | ||
| 0 line b | 28 (30.1) | 23 (29.5) | ||
| Platinum-containing chemotherapy | 55 (57.9) | 55 (59.1) | ||
| Chemotherapy plus cetuximab | 30 (31.6) | 30 (32.3) | ||
| Surgery | 24 (25.3) | 24 (25.8) | ||
| Local resection | 11 (11.8) | 11 (14.1) | ||
| Neck dissection | 17 (18.3) | 16 (20.5) | ||
| Radiotherapy | 27 (28.4) | 26 (28.0) | ||
| Platinum-refractory carcinoma c, n (%) | ||||
| Platinum-refractory | 48 (51.6) | 44 (56.4) | ||
| Not platinum-refractory | 44 (47.3) | 34 (43.6) | ||
| No history of a platinum-containing regimen d | 1 (1.1) | |||
| Best Overall Response | All Patients (N = 93) | SCCHN Patients a (N = 78) | Non-SCCHN Patients b (N = 15) |
|---|---|---|---|
| Complete Response, n (%) | 4 (4.3) | 4 (5.1) | 0 (0.0) |
| Partial Response, n (%) | 13 (13.9) | 13 (16.7) | 0 (0.0) |
| Stable Disease, n (%) | 11 (11.8) | 10 (12.8) | 1 (6.7) |
| Progressive Disease, n (%) | 60 (64.5) | 49 (62.8) | 11 (73.3) |
| Not Evaluable or Assessed, n (%) | 5 (5.4) | 2 (2.6) | 3 (20.0) |
| ORR (CR + PR), n (%) | 17 (18.3) | 17 (21.8) | 0 (0.0) |
| TRAEs | n (%) | Grade 1 n | Grade 2 n | Grade 3 n |
|---|---|---|---|---|
| Overall | 28 (35.9) | 8 | 14 | 6 |
| Hypothyroidism | 5 (6.4) | 5 | ||
| Pneumonia | 5 (6.4) | 3 | 1 | 1 |
| Skin Toxicity | 5 (6.4) | 1 | 4 | |
| Adrenal Insufficiency | 3 (3.8) | 3 | ||
| Colitis/Diarrhea | 3 (3.8) | 2 | 1 | |
| Stomatitis | 2 (2.6) | 1 | 1 | |
| Liver Dysfunction | 2 (2.6) | 1 | 1 | |
| Arthritis | 1 (1.3) | 1 | ||
| Diabetes Mellitus | 1 (1.3) | 1 | ||
| Renal Dysfunction | 1 (1.3) | 1 |
| Variable | PFS Rate (1 Year) | (95% CI) | p | ||
|---|---|---|---|---|---|
| Age (years) | 0.406 | ||||
| 75 or higher (n = 11) | 39.8% | (11.0–68.0) | |||
| <75 (n = 67) | 27.1% | (15.9–39.4) | |||
| Sex | 0.618 | ||||
| Male (n = 65) | 29.5% | (17.0–43.2) | |||
| Female (n = 13) | 23.1% | (5.6–47.5) | |||
| Smoking statuse | 0.574 | ||||
| Smoker (n = 49) | 33.1% | (19.2–47.7) | |||
| Never-smoker (n = 29) | 25.5% | (11.1–42.6) | |||
| ECOG PS | 0.257 | ||||
| 0 or 1 (n = 71) | 31.4% | (19.8–43.8) | |||
| 2 or 3 or 4 (n = 7) | Not reached | ||||
| PD-L1 expression | 0.82 | ||||
| <1% (n = 5) | 26.7% | (1.0–68.6) | |||
| ≥1% (n = 16) | 24.6% | (4.6–52.8) | |||
| Radiotherapy to the primary tumor | < 0.001 * | ||||
| Radiotherapy (+) (n = 37) | 46.3% | (28.5–62.4) | |||
| Radiotherapy (−) (n = 41) | 9.2% | (1.0–28.9) | |||
| Site of recurrernt or metastatic tumors | |||||
| Local primary site | 0.654 | ||||
| Yes (n = 33) | 27.1% | (10.9–46.4) | |||
| No (n = 45) | 30.2% | (17.1–44.5) | |||
| Lymph nodes | 0.262 | ||||
| Yes (n = 44) | 25.5% | (12.8–40.3) | |||
| No (n = 34) | 33.2% | (15.9–51.6) | |||
| Lung | 0.061 | ||||
| Yes (n = 27) | 19.3% | (6.7–36.6) | |||
| No (n = 51) | 33.6% | (18.9–48.9) | |||
| Treatment of recurrent or metastatic tumors prior to nivolumab therapy | |||||
| Chemotherapy | 0.899 | ||||
| Yes (n = 55) | 32.0% | (19.7–44.9) | |||
| No (n = 23) | 14.8% | (1.3–43.4) | |||
| Platinum-containing chemotherapy | 0.598 | ||||
| Yes (n = 48) | 30.0% | (17.2–44.0) | |||
| No (n = 30) | 25.8% | (8.9–46.9) | |||
| Chemotherapy plus cetuximab | 0.071 | ||||
| Yes (n = 27) | 23.3% | (9.1–41.2) | |||
| No (n = 51) | 32.6% | (18.8–47.1) | |||
| Surgery | 0.419 | ||||
| Yes (n = 22) | 24.5% | (8.7–44.6) | |||
| No (n = 56) | 30.4% | (17.1–44.8) | |||
| Radiotherapy | 0.154 | ||||
| Yes (n = 22) | 25.5% | (9.3–45.4) | |||
| No (n = 56) | 30.3% | (17.2–44.3) | |||
| Platinum-refractory carcinoma a | 0.006 * | ||||
| Platinum-refractory (n = 44) | 18.4% | (7.6–32.0) | |||
| Not platinum-refractory (n = 34) | 43.6% | (24.6–61.1) | |||
| Occurrence of TRAEs | 0.002 * | ||||
| TRAEs (+) (n = 22) | 53.9% | (29.5–73.1) | |||
| TRAEs (−) (n = 56) | 19.0% | (8.8–32.3) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hori, R.; Shinohara, S.; Kojima, T.; Kagoshima, H.; Kitamura, M.; Tateya, I.; Tamaki, H.; Kumabe, Y.; Asato, R.; Harada, H.; et al. Real-World Outcomes and Prognostic Factors in Patients Receiving Nivolumab Therapy for Recurrent or Metastatic Head and Neck Carcinoma. Cancers 2019, 11, 1317. https://doi.org/10.3390/cancers11091317
Hori R, Shinohara S, Kojima T, Kagoshima H, Kitamura M, Tateya I, Tamaki H, Kumabe Y, Asato R, Harada H, et al. Real-World Outcomes and Prognostic Factors in Patients Receiving Nivolumab Therapy for Recurrent or Metastatic Head and Neck Carcinoma. Cancers. 2019; 11(9):1317. https://doi.org/10.3390/cancers11091317
Chicago/Turabian StyleHori, Ryusuke, Shogo Shinohara, Tsuyoshi Kojima, Hiroki Kagoshima, Morimasa Kitamura, Ichiro Tateya, Hisanobu Tamaki, Yohei Kumabe, Ryo Asato, Hiroyuki Harada, and et al. 2019. "Real-World Outcomes and Prognostic Factors in Patients Receiving Nivolumab Therapy for Recurrent or Metastatic Head and Neck Carcinoma" Cancers 11, no. 9: 1317. https://doi.org/10.3390/cancers11091317
APA StyleHori, R., Shinohara, S., Kojima, T., Kagoshima, H., Kitamura, M., Tateya, I., Tamaki, H., Kumabe, Y., Asato, R., Harada, H., Kitani, Y., Tsujimura, T., Honda, K., Ichimaru, K., & Omori, K. (2019). Real-World Outcomes and Prognostic Factors in Patients Receiving Nivolumab Therapy for Recurrent or Metastatic Head and Neck Carcinoma. Cancers, 11(9), 1317. https://doi.org/10.3390/cancers11091317