Clinical Significance of ABCB1 in Acute Myeloid Leukemia: A Comprehensive Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
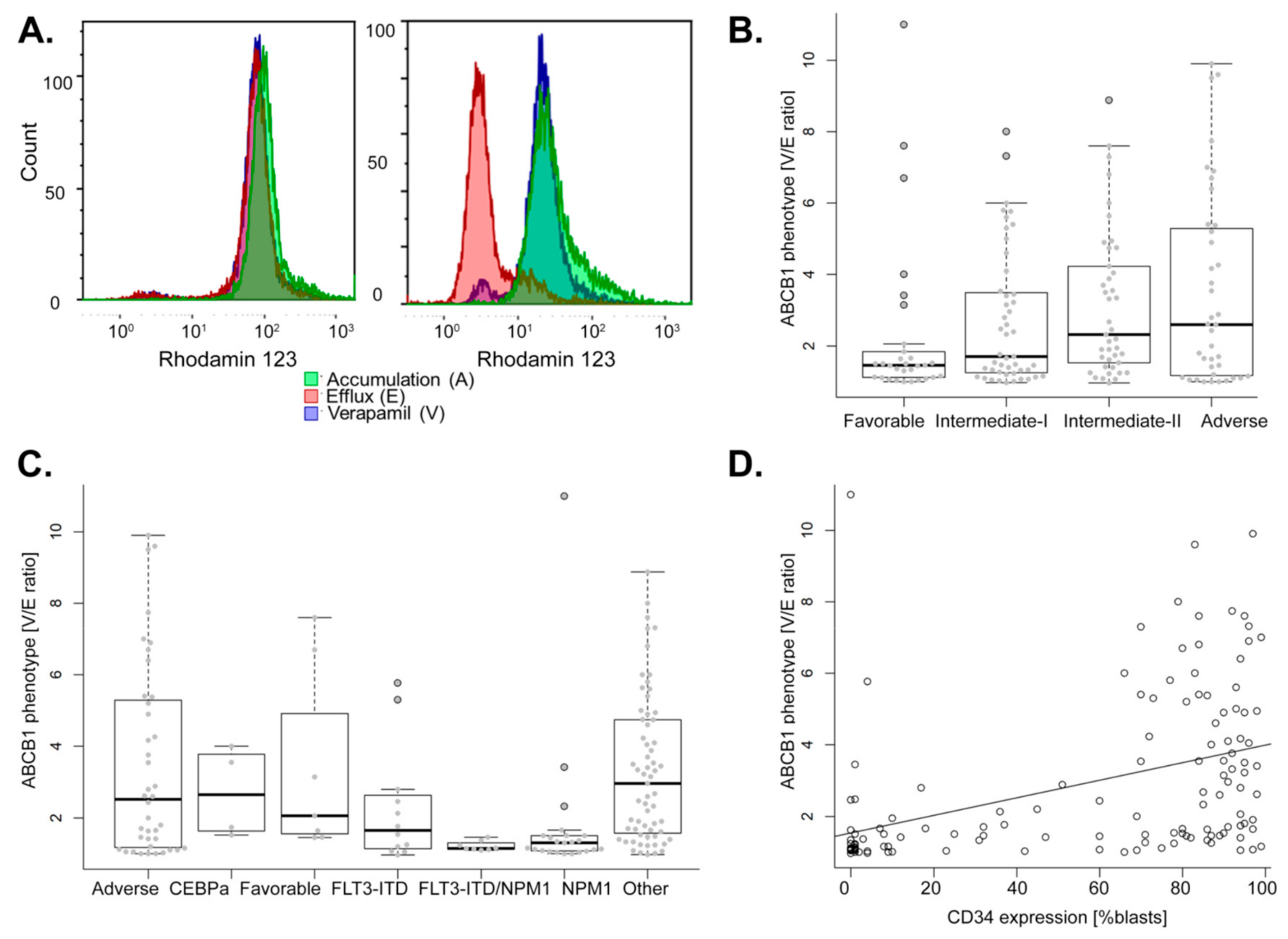
2.1. Association of ABCB1 Activity with Diagnostic Parameters of AML
2.2. Higher ABCB1 Activity Linked to Poor Clinical Outcome of AML Patients Treated with Standard Chemotherapy
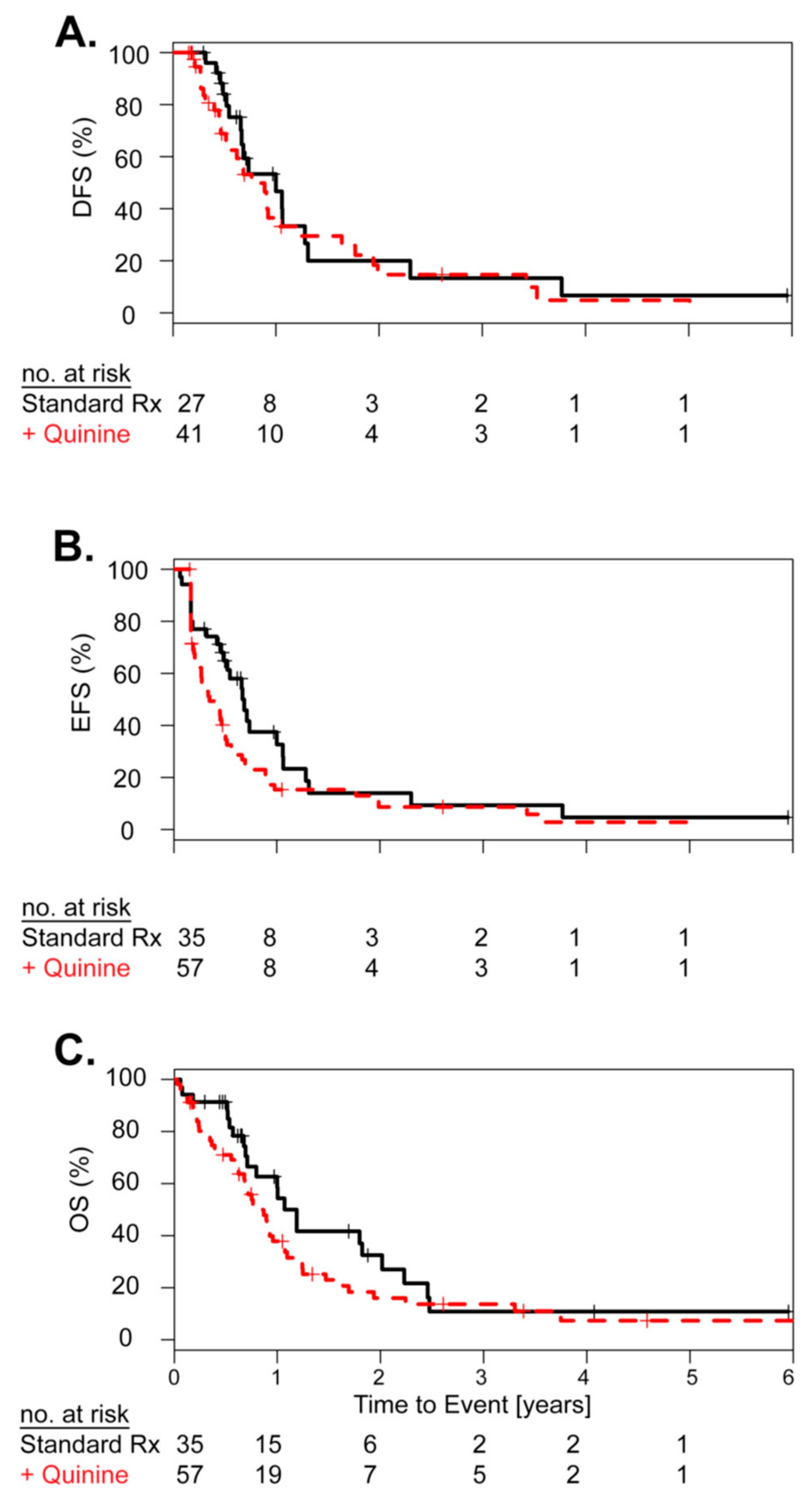
2.3. Concurrent Treatment with the ABCB1 Inhibitor Quinine Did Not Improve Clinical Outcome
2.4. Primary Cell ABCB1 Activity Was Not Linked to Ex Vivo Drug Resistance and Showed a Specific Gene Expression Profile
2.5. Patients with Low ABCB1 Expression Benefit from Addition Ofgemtuzumab Ozogamicin (GO) to Standard Chemotherapy
2.6. ABCB1 Expression Is Related to the Stem Cell Phenotype
3. Discussion
4. Materials and Methods
4.1. Patients’ Samples
4.2. ABCB1 Activity
4.3. Gene Expression Analysis
4.4. Ex Vivo Drug Resistance
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Dohner, H.; Weisdorf, D.J.; Bloomfield, C.D. Acute Myeloid Leukemia. N. Engl. J. Med. 2015, 373, 1136–1152. [Google Scholar] [CrossRef]
- Dohner, H.; Estey, E.H.; Amadori, S.; Appelbaum, F.R.; Buchner, T.; Burnett, A.K.; Dombret, H.; Fenaux, P.; Grimwade, D.; Larson, R.A.; et al. Diagnosis and management of acute myeloid leukemia in adults: Recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood 2010, 115, 453–474. [Google Scholar] [CrossRef]
- Shaffer, B.C.; Gillet, J.P.; Patel, C.; Baer, M.R.; Bates, S.E.; Gottesman, M.M. Drug resistance: Still a daunting challenge to the successful treatment of AML. Drug Resist. Updat. 2012, 15, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Robey, R.W.; Pluchino, K.M.; Hall, M.D.; Fojo, A.T.; Bates, S.E.; Gottesman, M.M. Revisiting the role of ABC transporters in multidrug-resistant cancer. Nat. Rev. Cancer 2018, 18, 452–464. [Google Scholar] [CrossRef]
- Marie, J.P.; Zittoun, R.; Sikic, B.I. Multidrug resistance (mdr1) gene expression in adult acute leukemias: Correlations with treatment outcome and in vitro drug sensitivity. Blood 1991, 78, 586–592. [Google Scholar]
- Campos, L.; Guyotat, D.; Archimbaud, E.; Calmard-Oriol, P.; Tsuruo, T.; Troncy, J.; Treille, D.; Fiere, D. Clinical significance of multidrug resistance P-glycoprotein expression on acute nonlymphoblastic leukemia cells at diagnosis. Blood 1992, 79, 473–476. [Google Scholar]
- Legrand, O.; Simonin, G.; Perrot, J.Y.; Zittoun, R.; Marie, J.P. Pgp and MRP activities using calcein-AM are prognostic factors in adult acute myeloid leukemia patients. Blood 1998, 91, 4480–4488. [Google Scholar]
- Pirker, R.; Wallner, J.; Geissler, K.; Linkesch, W.; Haas, O.A.; Bettelheim, P.; Hopfner, M.; Scherrer, R.; Valent, P.; Havelec, L.; et al. MDR1 gene expression and treatment outcome in acute myeloid leukemia. J. Natl. Cancer Inst. 1991, 83, 708–712. [Google Scholar] [CrossRef]
- Guerci, A.; Merlin, J.L.; Missoum, N.; Feldmann, L.; Marchal, S.; Witz, F.; Rose, C.; Guerci, O. Predictive value for treatment outcome in acute myeloid leukemia of cellular daunorubicin accumulation and P-glycoprotein expression simultaneously determined by flow cytometry. Blood 1995, 85, 2147–2153. [Google Scholar] [Green Version]
- Shi, P.; Zha, J.; Guo, X.; Chen, F.; Fan, Z.; Huang, F.; Meng, F.; Liu, X.; Feng, R.; Xu, B. Idarubicin is superior to daunorubicin in remission induction of de novo acute myeloid leukemia patients with high MDR1 expression. Pharmacogenomics 2013, 14, 17–23. [Google Scholar] [CrossRef]
- Walter, R.B.; Gooley, T.A.; Van Der Velden, V.H.; Loken, M.R.; van Dongen, J.J.; Flowers, D.A.; Bernstein, I.D.; Appelbaum, F.R. CD33 expression and P-glycoprotein-mediated drug efflux inversely correlate and predict clinical outcome in patients with acute myeloid leukemia treated with gemtuzumab ozogamicin monotherapy. Blood 2007, 109, 4168–4170. [Google Scholar] [CrossRef]
- Ford, J.M.; Hait, W.N. Pharmacology of drugs that alter multidrug resistance in cancer. Pharmacol. Rev. 1990, 42, 155–199. [Google Scholar]
- List, A.F.; Kopecky, K.J.; Willman, C.L.; Head, D.R.; Persons, D.L.; Slovak, M.L.; Dorr, R.; Karanes, C.; Hynes, H.E.; Doroshow, J.H.; et al. Benefit of cyclosporine modulation of drug resistance in patients with poor-risk acute myeloid leukemia: A Southwest Oncology Group study. Blood 2001, 98, 3212–3220. [Google Scholar] [CrossRef]
- Wattel, E.; Solary, E.; Hecquet, B.; Caillot, D.; Ifrah, N.; Brion, A.; Mahe, B.; Milpied, N.; Janvier, M.; Guerci, A.; et al. Quinine improves the results of intensive chemotherapy in myelodysplastic syndromes expressing P glycoprotein: Results of a randomized study. Br. J. Haematol. 1998, 102, 1015–1024. [Google Scholar] [CrossRef]
- Solary, E.; Drenou, B.; Campos, L.; De Cremoux, P.; Mugneret, F.; Moreau, P.; Lioure, B.; Falkenrodt, A.; Witz, B.; Bernard, M.; et al. Quinine as a multidrug resistance inhibitor: A phase 3 multicentric randomized study in adult de novo acute myelogenous leukemia. Blood 2003, 102, 1202–1210. [Google Scholar] [CrossRef]
- Solary, E.; Witz, B.; Caillot, D.; Moreau, P.; Desablens, B.; Cahn, J.Y.; Sadoun, A.; Pignon, B.; Berthou, C.; Maloisel, F.; et al. Combination of quinine as a potential reversing agent with mitoxantrone and cytarabine for the treatment of acute leukemias: A randomized multicenter study. Blood 1996, 88, 1198–1205. [Google Scholar]
- Greenberg, P.L.; Lee, S.J.; Advani, R.; Tallman, M.S.; Sikic, B.I.; Letendre, L.; Dugan, K.; Lum, B.; Chin, D.L.; Dewald, G.; et al. Mitoxantrone, etoposide, and cytarabine with or without valspodar in patients with relapsed or refractory acute myeloid leukemia and high-risk myelodysplastic syndrome: A phase III trial (E2995). J. Clin. Oncol. 2004, 22, 1078–1086. [Google Scholar] [CrossRef]
- Kolitz, J.E.; George, S.L.; Marcucci, G.; Vij, R.; Powell, B.L.; Allen, S.L.; DeAngelo, D.J.; Shea, T.C.; Stock, W.; Baer, M.R.; et al. P-glycoprotein inhibition using valspodar (PSC-833) does not improve outcomes for patients younger than age 60 years with newly diagnosed acute myeloid leukemia: Cancer and Leukemia Group B study 19808. Blood 2010, 116, 1413–1421. [Google Scholar] [CrossRef]
- Van der Holt, B.; Lowenberg, B.; Burnett, A.K.; Knauf, W.U.; Shepherd, J.; Piccaluga, P.P.; Ossenkoppele, G.J.; Verhoef, G.E.; Ferrant, A.; Crump, M.; et al. The value of the MDR1 reversal agent PSC-833 in addition to daunorubicin and cytarabine in the treatment of elderly patients with previously untreated acute myeloid leukemia (AML), in relation to MDR1 status at diagnosis. Blood 2005, 106, 2646–2654. [Google Scholar] [CrossRef] [Green Version]
- Kolitz, J.E.; George, S.L.; Dodge, R.K.; Hurd, D.D.; Powell, B.L.; Allen, S.L.; Velez-Garcia, E.; Moore, J.O.; Shea, T.C.; Hoke, E.; et al. Dose escalation studies of cytarabine, daunorubicin, and etoposide with and without multidrug resistance modulation with PSC-833 in untreated adults with acute myeloid leukemia younger than 60 years: Final induction results of Cancer and Leukemia Group B Study 9621. J. Clin. Oncol. 2004, 22, 4290–4301. [Google Scholar] [CrossRef]
- Ng, S.W.; Mitchell, A.; Kennedy, J.A.; Chen, W.C.; McLeod, J.; Ibrahimova, N.; Arruda, A.; Popescu, A.; Gupta, V.; Schimmer, A.D.; et al. A 17-gene stemness score for rapid determination of risk in acute leukaemia. Nature 2016, 540, 433–437. [Google Scholar] [CrossRef]
- Hirsch, P.; Tang, R.; Marzac, C.; Perrot, J.Y.; Fava, F.; Bernard, C.; Jeziorowska, D.; Marie, J.P.; Legrand, O. Prognostic impact of high ABC transporter activity in 111 adult acute myeloid leukemia patients with normal cytogenetics when compared to FLT3, NPM1, CEBPA and BAALC. Haematologica 2012, 97, 241–245. [Google Scholar] [CrossRef]
- Van den Heuvel-Eibrink, M.M.; Van der Holt, B.; Burnett, A.K.; Knauf, W.U.; Fey, M.F.; Verhoef, G.E.; Vellenga, E.; Ossenkoppele, G.J.; Lowenberg, B.; Sonneveld, P. CD34-related coexpression of MDR1 and BCRP indicates a clinically resistant phenotype in patients with acute myeloid leukemia (AML) of older age. Ann. Hematol. 2007, 86, 329–337. [Google Scholar] [CrossRef] [Green Version]
- Leith, C. Multidrug resistance in leukemia. Curr. Opin. Hematol. 1998, 5, 287–291. [Google Scholar] [CrossRef]
- Baldus, C.D.; Tanner, S.M.; Ruppert, A.S.; Whitman, S.P.; Archer, K.J.; Marcucci, G.; Caligiuri, M.A.; Carroll, A.J.; Vardiman, J.W.; Powell, B.L.; et al. BAALC expression predicts clinical outcome of de novo acute myeloid leukemia patients with normal cytogenetics: A Cancer and Leukemia Group B Study. Blood 2003, 102, 1613–1618. [Google Scholar] [CrossRef]
- Coles, S.J.; Wang, E.C.; Man, S.; Hills, R.K.; Burnett, A.K.; Tonks, A.; Darley, R.L. CD200 expression suppresses natural killer cell function and directly inhibits patient anti-tumor response in acute myeloid leukemia. Leukemia 2011, 25, 792–799. [Google Scholar] [CrossRef] [Green Version]
- Martner, A.; Thoren, F.B.; Aurelius, J.; Hellstrand, K. Immunotherapeutic strategies for relapse control in acute myeloid leukemia. Blood Rev. 2013, 27, 209–216. [Google Scholar] [CrossRef]
- Linenberger, M.L.; Hong, T.; Flowers, D.; Sievers, E.L.; Gooley, T.A.; Bennett, J.M.; Berger, M.S.; Leopold, L.H.; Appelbaum, F.R.; Bernstein, I.D. Multidrug-resistance phenotype and clinical responses to gemtuzumab ozogamicin. Blood 2001, 98, 988–994. [Google Scholar] [CrossRef] [Green Version]
- Castaigne, S.; Pautas, C.; Terre, C.; Raffoux, E.; Bordessoule, D.; Bastie, J.N.; Legrand, O.; Thomas, X.; Turlure, P.; Reman, O.; et al. Effect of gemtuzumab ozogamicin on survival of adult patients with de-novo acute myeloid leukaemia (ALFA-0701): A randomised, open-label, phase 3 study. Lancet 2012, 379, 1508–1516. [Google Scholar] [CrossRef]
- Holleman, A.; Cheok, M.H.; den Boer, M.L.; Yang, W.; Veerman, A.J.; Kazemier, K.M.; Pei, D.; Cheng, C.; Pui, C.H.; Relling, M.V.; et al. Gene-expression patterns in drug-resistant acute lymphoblastic leukemia cells and response to treatment. N. Engl. J. Med. 2004, 351, 533–542. [Google Scholar] [CrossRef]
- Nibourel, O.; Guihard, S.; Roumier, C.; Pottier, N.; Terre, C.; Paquet, A.; Peyrouze, P.; Geffroy, S.; Quentin, S.; Alberdi, A.; et al. Copy-number analysis identified new prognostic marker in acute myeloid leukemia. Leukemia 2017, 31, 555–564. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Positive ABCB1 n = 94 (58%) | Negative ABCB1 n = 67 (42%) | p-Value | |
|---|---|---|---|
| Median Age in years (range) | 60.6 (22.3–86.7) | 60.7 (21.3–87.9) | 0.99 |
| Median WBC count as 109/L (range) | 4.7 (0.8–208.0) | 16.2 (0.7–378.0) | 0.011 |
| FAB subtypesn (%) | |||
| M0 | 8 (8) | 4 (6) | <0.001 |
| M1 | 11 (12) | 15(22) | |
| M2 | 31 (33) | 8 (12) | |
| M4 | 8 (9) | 13 (19) | |
| M5 | 3 (3) | 15 (22) | |
| M6 | 2 (2) | 0 | |
| M7 | 2 (2) | 0 | |
| ND | 29 (31) | 12 (18) | |
| Cytogenetics | |||
| Favorable | 6 (6) | 2 (3) | 0.556 |
| Intermediate | 62 (66) | 49 (73) | |
| Adverse | 26 (28) | 16 (24) | |
| Median CD34 expression as % of blasts (range) | 85.0 (0.0–99.0) | 12.0 (0.0–99.0) | <0.001 |
| NPM1 mutationn (%) | |||
| Present | 4 (4) | 29 (43) | <0.001 |
| Absent | 75 (80) | 32 (48) | |
| ND | 15 (16) | 6 (9) | |
| FLT3-ITDn (%) | |||
| Present | 7 (7) | 16 (24) | 0.006 |
| Absent | 77 (82) | 47 (70) | |
| ND | 10 (11) | 4 (6) | |
| CEBPA mutation n (%) | |||
| Present | 6 (6) | 0 (0) | 0.037 |
| Absent | 73 (78) | 60 (90) | |
| ND | 15 (16) | 7 (10) | |
| Characteristics | DFS HR | 95% CI | p-Value | EFS HR | 95% CI | p-Value | OS HR | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| ELN classification | |||||||||
| Favorable | - | - | - | - | - | - | - | - | - |
| Intermediate-I | 2.1 | 0.89–4.94 | 0.091 | 2.6 | 1.15–5.89 | 0.022 | 2.34 | 0.90–6.31 | 0.082 |
| Intermediate-II | 3.71 | 1.48–9.31 | 0.005 | 4.5 | 1.88–10.7 | 0.007 | 4.5 | 1.72–11.8 | 0.002 |
| Adverse | 13.9 | 4.02–48.1 | <0.001 | 12.6 | 4.40–35.9 | <0.001 | 19.9 | 5.91–67.2 | <0.001 |
| WBC count | |||||||||
| <100 | - | - | - | - | - | - | - | - | - |
| >100 | 4.22 | 1.32–13.5 | 0.015 | 2.95 | 1.16–7.49 | 0.023 | 3.68 | 1.40–9.72 | 0.008 |
| ABCB1 activity | |||||||||
| Low | - | - | - | - | - | - | - | - | - |
| High | 1.66 | 0.84–3.28 | 0.146 | 1.84 | 1.02–3.32 | 0.044 | 1.98 | 1.03–3.81 | 0.039 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boyer, T.; Gonzales, F.; Barthélémy, A.; Marceau-Renaut, A.; Peyrouze, P.; Guihard, S.; Lepelley, P.; Plesa, A.; Nibourel, O.; Delattre, C.; et al. Clinical Significance of ABCB1 in Acute Myeloid Leukemia: A Comprehensive Study. Cancers 2019, 11, 1323. https://doi.org/10.3390/cancers11091323
Boyer T, Gonzales F, Barthélémy A, Marceau-Renaut A, Peyrouze P, Guihard S, Lepelley P, Plesa A, Nibourel O, Delattre C, et al. Clinical Significance of ABCB1 in Acute Myeloid Leukemia: A Comprehensive Study. Cancers. 2019; 11(9):1323. https://doi.org/10.3390/cancers11091323
Chicago/Turabian StyleBoyer, Thomas, Fanny Gonzales, Adeline Barthélémy, Alice Marceau-Renaut, Pauline Peyrouze, Soizic Guihard, Pascale Lepelley, Adriana Plesa, Olivier Nibourel, Carole Delattre, and et al. 2019. "Clinical Significance of ABCB1 in Acute Myeloid Leukemia: A Comprehensive Study" Cancers 11, no. 9: 1323. https://doi.org/10.3390/cancers11091323
APA StyleBoyer, T., Gonzales, F., Barthélémy, A., Marceau-Renaut, A., Peyrouze, P., Guihard, S., Lepelley, P., Plesa, A., Nibourel, O., Delattre, C., Wetterwald, M., Pottier, N., Plantier, I., de Botton, S., Dombret, H., Berthon, C., Preudhomme, C., Roumier, C., & Cheok, M. (2019). Clinical Significance of ABCB1 in Acute Myeloid Leukemia: A Comprehensive Study. Cancers, 11(9), 1323. https://doi.org/10.3390/cancers11091323