Novel Model to Predict HCC Recurrence after Liver Transplantation Obtained Using Deep Learning: A Multicenter Study

 , , , ,
, , , ,
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Participants
2.2. Statistical Analysis
2.3. Deep Learning for Development of a Novel Prediction Model
3. Results
3.1. Baseline Characteristics of the Derivation and Validation Cohorts
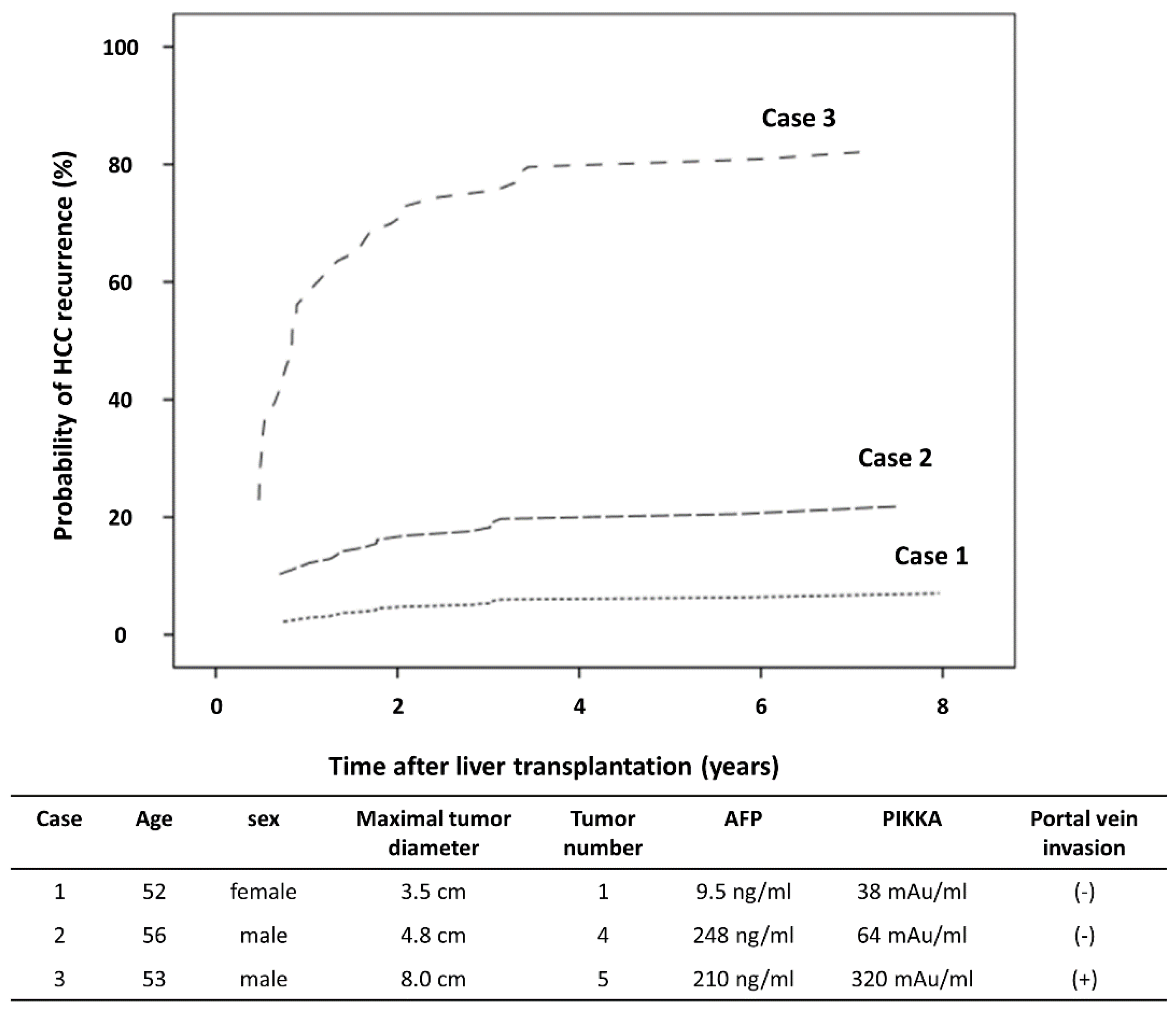
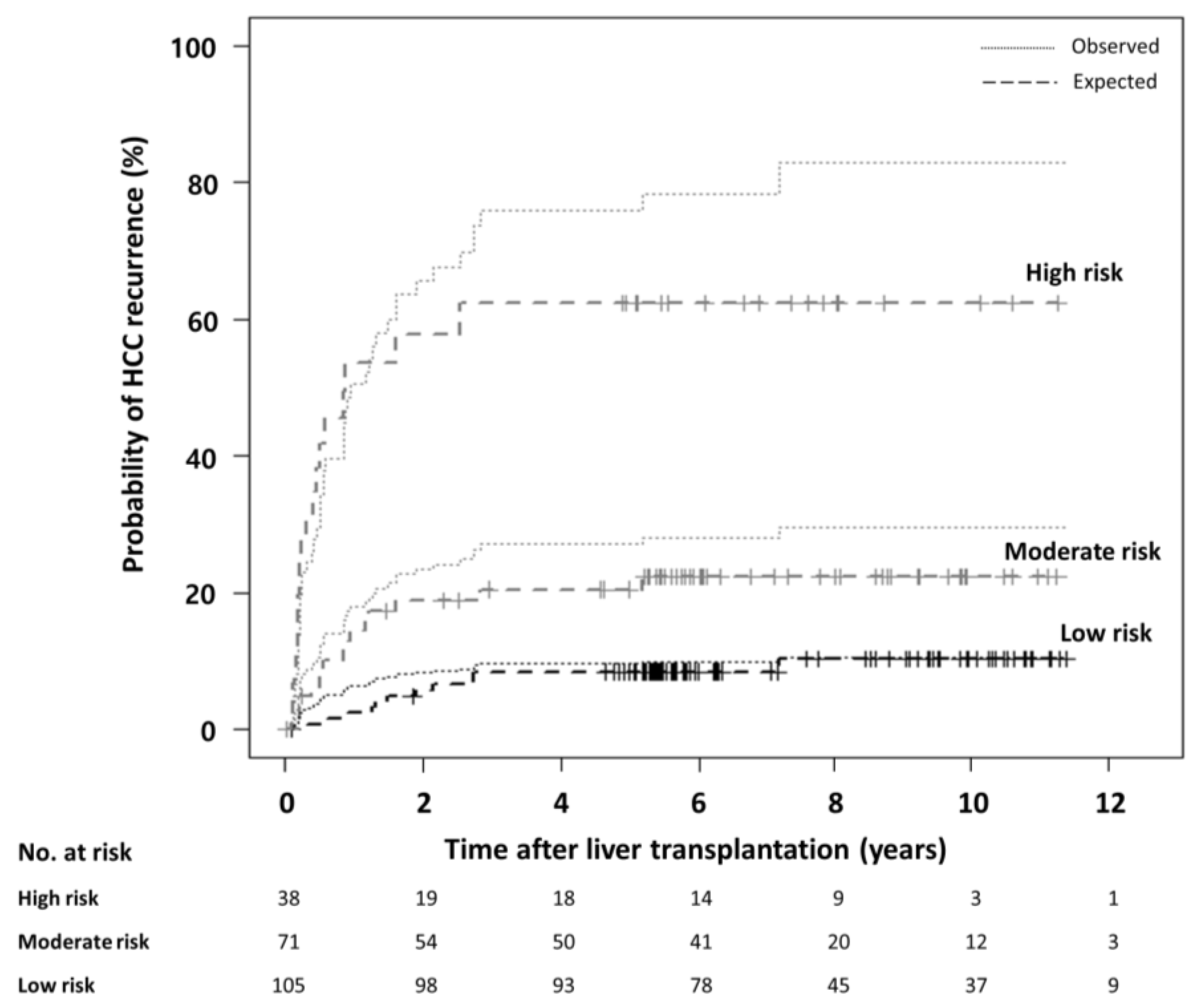
3.2. Deep Learning Based Model
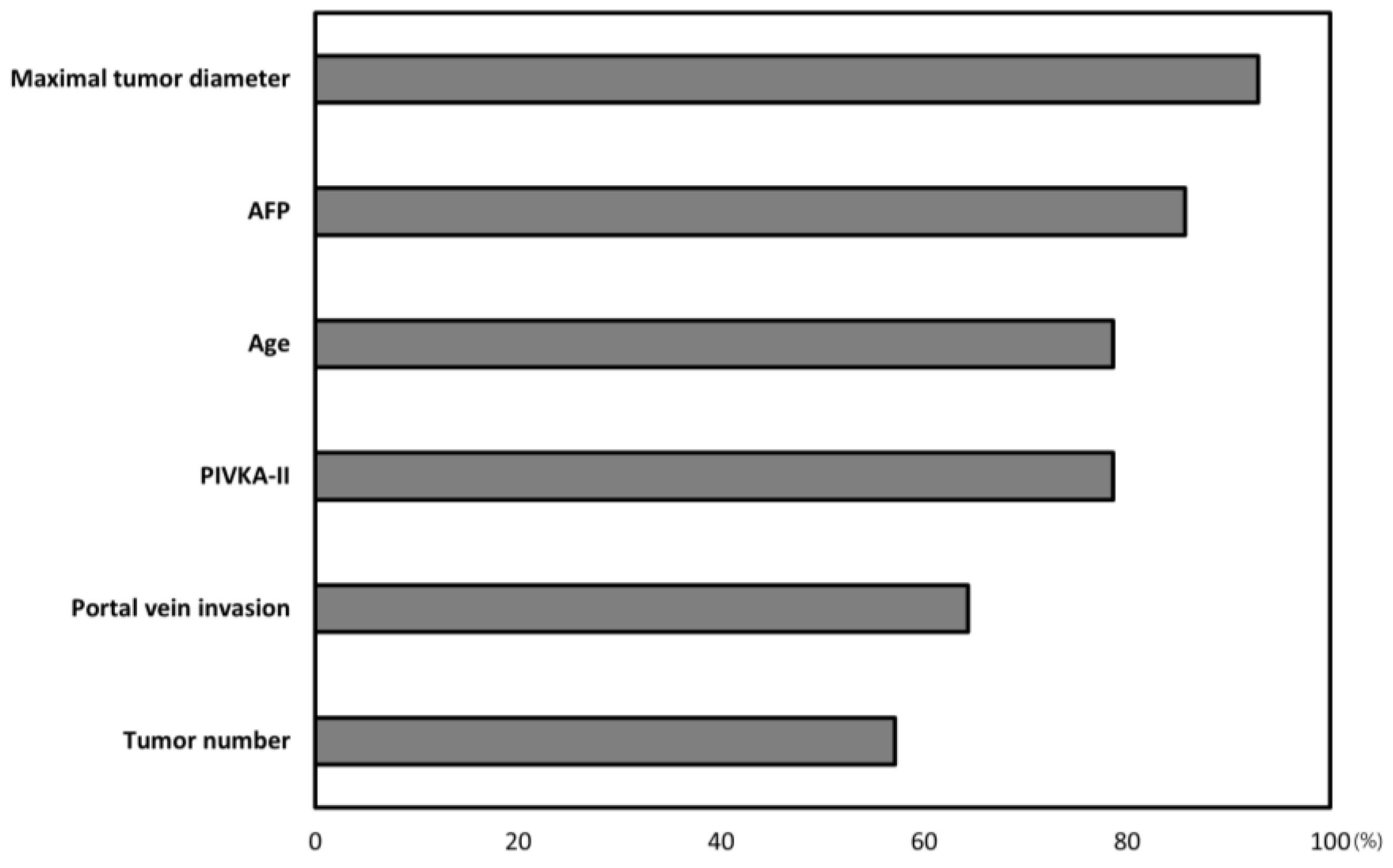
3.3. Evaluation of the Weight of Each Factor in the DNN Model
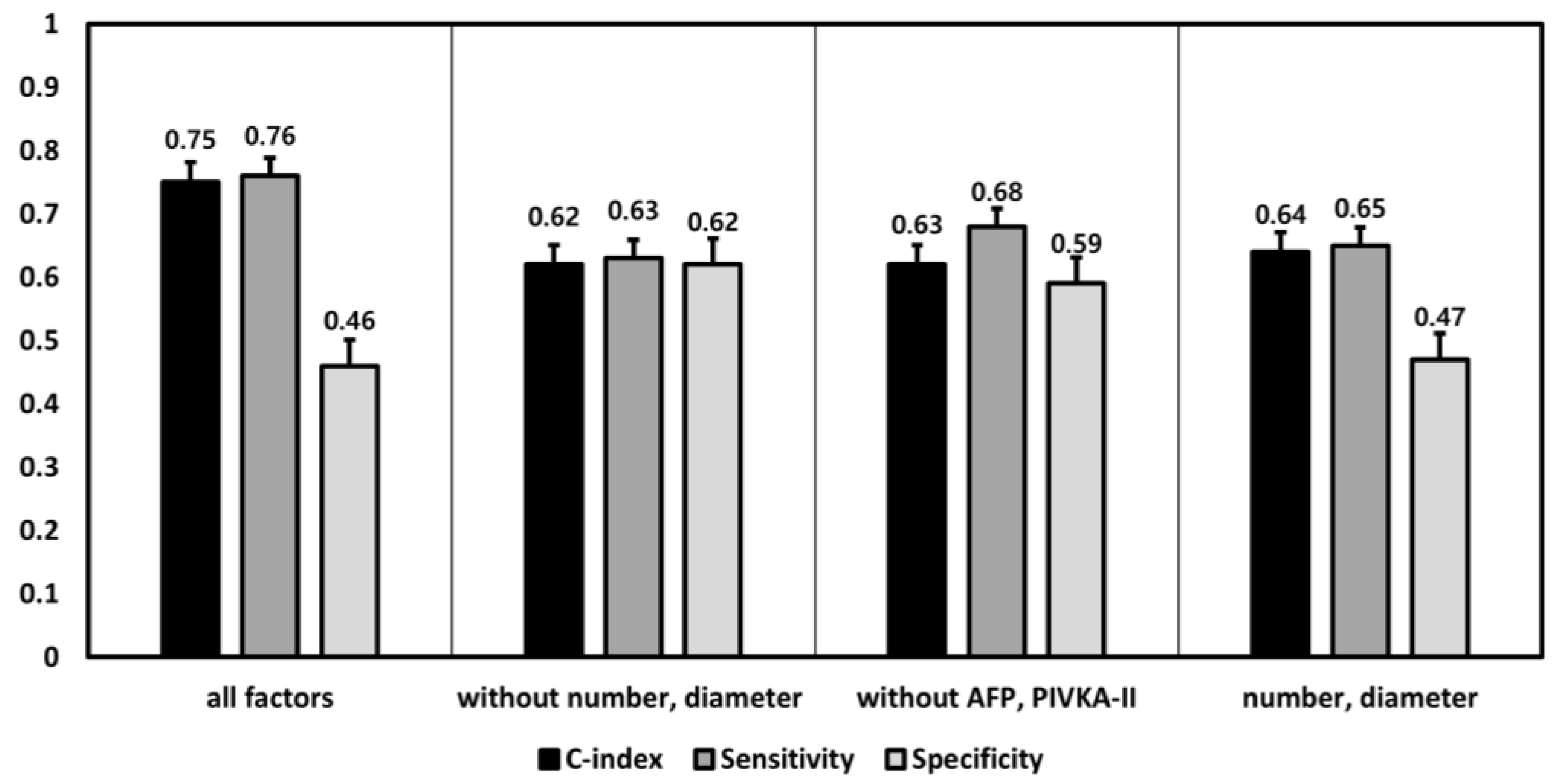
3.4. Performance Differences among the DNN Models according to the Inclusion of Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–700. [Google Scholar] [CrossRef]
- Herrero, J.I.; Sangro, B.; Pardo, F.; Quiroga, J.; Inarrairaegui, M.; Rotellar, F.; Montiel, C.; Alegre, F.; Prieto, J. Liver transplantation in patients with hepatocellular carcinoma across Milan criteria. Liver Transplant. 2008, 14, 272–278. [Google Scholar] [CrossRef]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Watson, J.J.; Bacchetti, P.; Venook, A.; Ascher, N.L.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: Expansion of the tumor size limits does not adversely impact survival. Hepatology 2001, 33, 1394–1403. [Google Scholar] [CrossRef]
- Ito, T.; Takada, Y.; Ueda, M.; Haga, H.; Maetani, Y.; Oike, F.; Ogawa, K.; Sakamoto, S.; Ogura, Y.; Egawa, H. Expansion of selection criteria for patients with hepatocellular carcinoma in living donor liver transplantation. Liver Transplant. 2007, 13, 1637–1644. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: A retrospective, exploratory analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef]
- Lee, J.-H.; Cho, Y.; Kim, H.Y.; Cho, E.J.; Lee, D.H.; Yu, S.J.; Lee, J.W.; Yi, N.-J.; Lee, K.-W.; Kim, S.H. Serum tumor markers provide refined prognostication in selecting liver transplantation candidate for hepatocellular carcinoma patients beyond the Milan criteria. Ann. Surg. 2016, 263, 842–850. [Google Scholar] [CrossRef]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115. [Google Scholar] [CrossRef]
- Loftus, T.J.; Tighe, P.J.; Filiberto, A.C.; Efron, P.A.; Brakenridge, S.C.; Mohr, A.M.; Rashidi, P.; Upchurch, G.R.; Bihorac, A.J.J.S. Artificial intelligence and surgical decision-making. JAMA Surg. 2020, 155, 148–158. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL–EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma. Hepatology 2005, 42, 1208–1236. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M.; Llovet, J.M.; Beaugrand, M.; Lencioni, R.; Burroughs, A.K.; Christensen, E.; Pagliaro, L.; Colombo, M.; Rodés, J. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. J. Hepatol. 2001, 35, 421–430. [Google Scholar] [CrossRef]
- Cho, J.Y.; Suh, K.-S.; Shin, W.Y.; Lee, H.W.; Yi, N.-J.; Lee, K.U. Thrombosis confined to the portal vein is not a contraindication for living donor liver transplantation. World J. Surg. 2008, 32, 1731–1737. [Google Scholar] [CrossRef]
- Marzano, A.; Salizzoni, M.; Debernardi-Venon, W.; Smedile, A.; Franchello, A.; Ciancio, A.; Gentilcore, E.; Piantino, P.; Barbui, A.M.; David, E. Prevention of hepatitis B virus recurrence after liver transplantation in cirrhotic patients treated with lamivudine and passive immunoprophylaxis. J. Hepatol. 2001, 34, 903–910. [Google Scholar] [CrossRef]
- Chun, J.; Kim, W.; Kim, B.G.; Lee, K.L.; Suh, K.S.; Yi, N.J.; Park, K.U.; Kim, Y.J.; Yoon, J.H.; Lee, H. High viremia, prolonged Lamivudine therapy and recurrent hepatocellular carcinoma predict posttransplant hepatitis B recurrence. Am. J. Transpl. 2010, 10, 1649–1659. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 26 June 2016. [Google Scholar]
- Schwartz, M. Liver transplantation for hepatocellular carcinoma. Gastroenterology 2004, 127, S268–S276. [Google Scholar] [CrossRef]
- Xu, X.; Lu, D.; Ling, Q.; Wei, X.; Wu, J.; Zhou, L.; Yan, S.; Wu, L.; Geng, L.; Ke, Q. Liver transplantation for hepatocellular carcinoma beyond the Milan criteria. Gut 2016, 65, 1035–1041. [Google Scholar] [CrossRef]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; Van Der Laak, J.A.; Van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436. [Google Scholar] [CrossRef]
- Korean Network for Organ Sharing. Available online: https://www.konos.go.kr/konosis/common/bizlogic.jsp or https://www.konos.go.kr; (accessed on 8 April 2020).
- Ministry of the Interior and Safety. Available online: http://www.prism.go.kr/homepage/entire/retrieveEntireDetail.do?research_id=1351000-201700153 or http://www.prism.go.kr; (accessed on 8 April 2020).
- Lee, K.W.; Suh, S.W.; Choi, Y.; Jeong, J.; Yi, N.J.; Kim, H.; Yoon, K.C.; Hong, S.K.; Kim, H.S.; Lee, K.B.J.L.T. Macrovascular invasion is not an absolute contraindication for living donor liver transplantation. Liver Transpl. 2017, 23, 19–27. [Google Scholar] [CrossRef]
- Schmidhuber, J. Deep learning in neural networks: An overview. Neural Netw. 2015, 61, 85–117. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics | Derivation Set (n = 349) | Validation Set (n = 214) | p-Value |
|---|---|---|---|
| Age, years | 55.7 ± 7.8 | 53.7 ± 7.6 | 0.004 † |
| Sex, Male, (n, %) | 286 (81.1%) | 182 (85.0%) | 0.229 ‡ |
| Maximal Tumor size, cm | 3.0 ± 2.1 | 2.6 ± 2.1 | 0.021 † |
| Tumor number, no. | 1.0 (1.0–3.0) | 2.0 (1.0–3.0) | 0.046 |
| AFP, ng/mL | 19.0 (7.1–130.5) | 13.9 (5.5–70.6) | 0.060 |
| PIVKA-II, mAU/mL | 29.0 (15.0–137.5) | 31.5 (19.0–111.8) | 0.171 |
| Portal vein invasion, (n, %) | 44 (12.6%) | 39 (18.2%) | 0.068 ‡ |
| BCLC stage | 40/156/65/33/55 | 21/79/34/26/54 | 0.042 ‡ |
| 0/A/B/C/D, (n, %) | 11.5/44.7/18.6/9.5/15.8 | 9.8/36.9/15.9/12.1/25.2 | |
| Type of HCC | 279/25/0 | 192/20/2 | 0.214 ‡ |
| Nodular/diffuse or infiltrative, (n, %) | 91.8/8.2/0.0 | 89.2/9.3/0.9 | |
| Median follow-up, months | 71.4 (12.8–104.3) | 77.3 (56.0–117.7) | 0.004 |
| Proportion of beyond-MC | 114 (32.7%) | 90 (42.1%) | 0.024 ‡ |
| Portal vein invasion, (n, %) | 44 (38.6%) | 39 (43.3%) | 0.494 ‡ |
| Multinodular HCCs (≥4), (n, %) | 53 (46.5%) | 46 (51.1%) | 0.512 ‡ |
| Large HCCs (>5 cm), (n, %) | 38 (33.3%) | 20 (22.2%) | 0.081 ‡ |
| Model | c-Index | 95% Confidence Interval | p-Value † | |
|---|---|---|---|---|
| Lower | Upper | |||
| MoRAL-AI | 0.75 | 0.67 | 0.83 | Ref. |
| Milan criteria | 0.64 | 0.60 | 0.68 | <0.001 † |
| MoRAL | 0.69 | 0.59 | 0.79 | <0.001 † |
| UCSF | 0.62 | 0.52 | 0.72 | <0.001 † |
| Up-to-seven | 0.50 | 0.40 | 0.59 | <0.001 † |
| Kyoto criteria | 0.50 | 0.40 | 0.59 | <0.001 † |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, J.Y.; Lee, J.-H.; Bae, J.; Chang, Y.; Cho, Y.; Sinn, D.H.; Kim, B.H.; Kim, S.H.; Yi, N.-J.; Lee, K.-W.; et al. Novel Model to Predict HCC Recurrence after Liver Transplantation Obtained Using Deep Learning: A Multicenter Study. Cancers 2020, 12, 2791. https://doi.org/10.3390/cancers12102791
Nam JY, Lee J-H, Bae J, Chang Y, Cho Y, Sinn DH, Kim BH, Kim SH, Yi N-J, Lee K-W, et al. Novel Model to Predict HCC Recurrence after Liver Transplantation Obtained Using Deep Learning: A Multicenter Study. Cancers. 2020; 12(10):2791. https://doi.org/10.3390/cancers12102791
Chicago/Turabian StyleNam, Joon Yeul, Jeong-Hoon Lee, Junho Bae, Young Chang, Yuri Cho, Dong Hyun Sinn, Bo Hyun Kim, Seoung Hoon Kim, Nam-Joon Yi, Kwang-Woong Lee, and et al. 2020. "Novel Model to Predict HCC Recurrence after Liver Transplantation Obtained Using Deep Learning: A Multicenter Study" Cancers 12, no. 10: 2791. https://doi.org/10.3390/cancers12102791
APA StyleNam, J. Y., Lee, J.-H., Bae, J., Chang, Y., Cho, Y., Sinn, D. H., Kim, B. H., Kim, S. H., Yi, N.-J., Lee, K.-W., Kim, J. M., Park, J.-W., Kim, Y. J., Yoon, J.-H., Joh, J.-W., & Suh, K.-S. (2020). Novel Model to Predict HCC Recurrence after Liver Transplantation Obtained Using Deep Learning: A Multicenter Study. Cancers, 12(10), 2791. https://doi.org/10.3390/cancers12102791