
Quantitative Multiplexed Proteomics Could Assist Therapeutic Decision Making in Non-Small Cell Lung Cancer Patients with Ambiguous ALK Test Results
by

Ho Jung An
1, 
Eunkyung An
2,
Shahrooz Rabizadeh
2,
Wei-Li Liao
2,
Jon Burrows
3,
Todd Hembrough
3,
Jin Hyung Kang
4,
Chan Kwon Park
5 and
Tae-Jung Kim
6,*
1
Department of Medical Oncology, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Seoul 06591, Korea
2
NantOmics, Culver City, CA 90232, USA
3
OncoPlex Diagnostics, Rockville, MD 20850, USA
4
Department of Medical Oncology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul 06591, Korea
5
Division of Pulmonology, Department of Internal Medicine, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul 06591, Korea
6
Department of Hospital Pathology, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul 06591, Korea
*
Author to whom correspondence should be addressed.
Cancers 2021, 13(10), 2337; https://doi.org/10.3390/cancers13102337
Submission received: 6 April 2021
/
Revised: 5 May 2021
/
Accepted: 5 May 2021
/
Published: 12 May 2021
(This article belongs to the Special Issue Update in Lung Cancer Molecular Pathology: Technological Advances and Clinical Practice)
Simple Summary
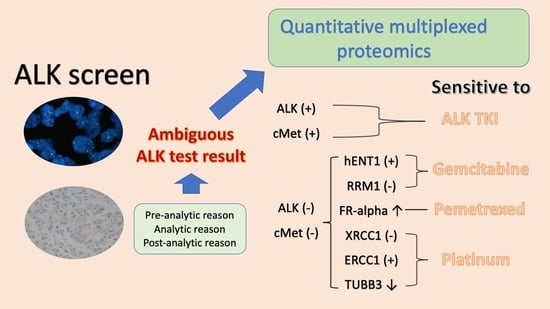
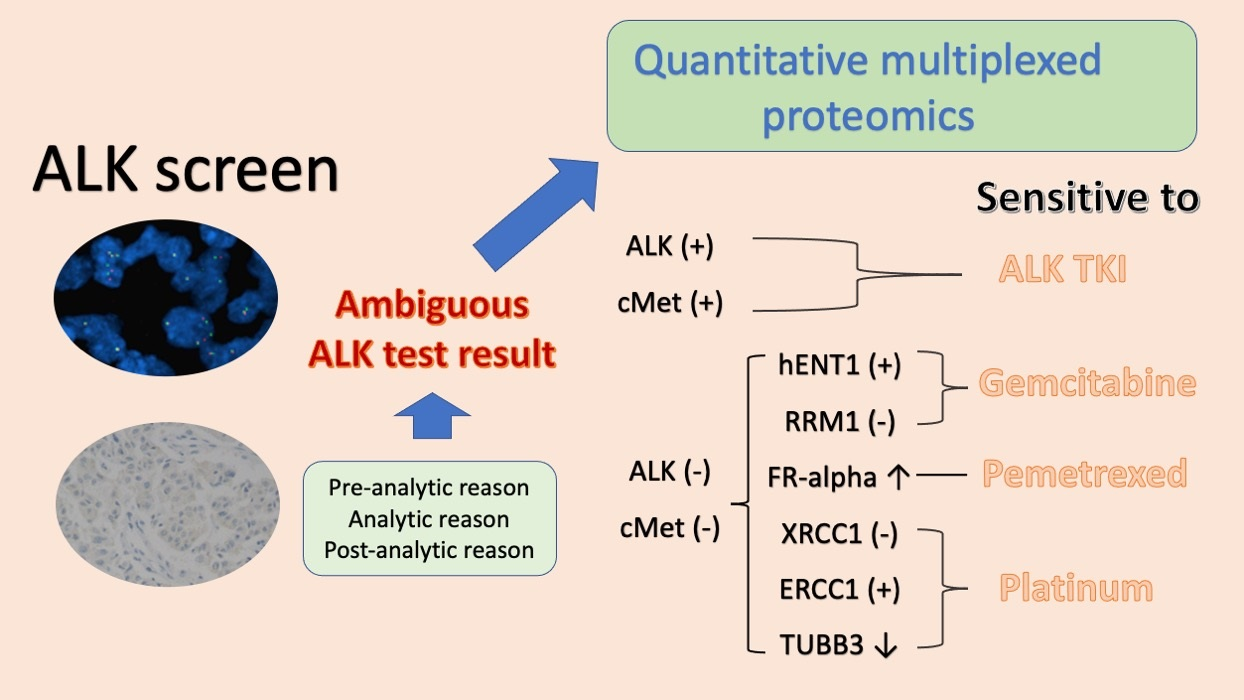
Therapeutic guidance in non-small cell lung cancer (NSCLC) patients with discordant anaplastic lymphoma kinase (ALK) fluorescent in situ hybridization (+) where immunohistochemistry (IHC) (−) results are challenging. Selected reaction monitoring (SRM) quantitative multiplexed proteomics could detect ALK protein in NSCLC samples with delayed fixation where a conventional IHC method failed. ALK protein detection by the SRM method was associated with good responses on ALK inhibitors. It also could detect various predictive proteins for conventional chemotherapy at the same time, and combined results were related to clinical outcomes in this population. The SRM may provide additional information for therapeutic decision making in NSCLC patients with ambiguous ALK test results.
Abstract
Therapeutic guidance in non-small cell lung cancer (NSCLC) tumors that are positive for anaplastic lymphoma kinase (ALK) fluorescent in situ hybridization (FISH), but negative for ALK immunohistochemistry, is still challenging. Parallel routine screening of 4588 NSCLC cases identified 22 discordant cases. We rechecked these samples using ALK antibodies and selected reaction monitoring (SRM) quantitative multiplexed proteomics screening multiple protein targets, including ALK and MET for the ALK tyrosine kinase inhibitor (TKI), and FR-alpha, hENT1, RRM1, TUBB3, ERCC1, and XRCC1 for chemotherapy. The presence of ALK (31.8%), MET (36.4%), FR-alpha (72.7%), hENT1 (18.2%), RRM1 (31.8%), TUBB3 (72.9%), ERCC1 (4.5%), and a low level of XRCC1 (54.4%) correlated with clinical outcomes. SRM was more sensitive than the ALK D5F3 assay. Among the eight cases receiving ALK TKI, four cases with ALK or MET detected by SRM had complete or partial responses, whereas four cases without ALK or MET showed progression. Twenty-seven treatment outcomes from 20 cases were assessed and cases expressing more than half of the specific predictive proteins were sensitive to matching therapeutic agents and showed longer progression-free survival than the other cases (p < 0.001). SRM showed a potential role in therapeutic decision making in NSCLC patients with ambiguous ALK test results.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}