
SEGHI Study: Defining the Best Surveillance Strategy in Hodgkin Lymphoma after First-Line Treatment

 , , , , , ,
, , , , , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Engert, A. ABVD or BEACOPP for Advanced Hodgkin Lymphoma. J. Clin. Oncol. 2016, 34, 1167–1169. [Google Scholar] [CrossRef] [Green Version]
- Radford, J.; Illidge, T.; Counsell, N.; Hancock, B.; Pettengell, R.; Johnson, P.; Wimperis, J.; Culligan, D.; Popova, B.; Smith, P.; et al. Results of a Trial of PET-Directed Therapy for Early-Stage Hodgkin’s Lymphoma. N. Engl. J. Med. 2015, 372, 1598–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connors, J.M.; Jurczak, W.; Straus, D.; Ansell, S.M.; Kim, W.S.; Gallamini, A.; Younes, A.; Alekseev, S.; Illés, Á.; Picardi, M.; et al. Brentuximab Vedotin with Chemotherapy for Stage III or IV Hodgkin’s Lymphoma. N. Engl. J. Med. 2018, 378, 331–344. [Google Scholar] [CrossRef] [PubMed]
- A Radford, J.; Eardley, A.; Woodman, C.; Crowther, D. Follow up policy after treatment for Hodgkin’s disease: Too many clinic visits and routine tests? A review of hospital records. BMJ 1997, 314, 343. [Google Scholar] [CrossRef] [Green Version]
- Elis, A.; Blickstein, D.; Klein, O.; Eliav-Ronen, R.; Manor, Y.; Lishner, M. Detection of relapse in non-Hodgkin’s lymphoma: Role of routine follow-up studies. Am. J. Hematol. 2001, 69, 41–44. [Google Scholar] [CrossRef]
- Guppy, A.; Tebbutt, N.; Norman, A.; Cunningham, D. The Role of Surveillance CT Scans in Patients with Diffuse Large B-cell Non-Hodgkin’s Lymphoma. Leuk. Lymphoma 2003, 44, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, D.C.; Grunfeld, E.; Gunraj, N.; Del Giudice, L. A population-based study of follow-up care for Hodgkin lymphoma survivors: Opportunities to improve surveillance for relapse and late effects. Cancer 2010, 116, 3417–3425. [Google Scholar] [CrossRef]
- Guadagnolo, B.A.; Punglia, R.S.; Kuntz, K.M.; Mauch, P.M.; Ng, A.K. Cost-Effectiveness Analysis of Computerized Tomography in the Routine Follow-Up of Patients After Primary Treatment for Hodgkin’s Disease. J. Clin. Oncol. 2006, 24, 4116–4122. [Google Scholar] [CrossRef]
- El-Galaly, T.C.; Mylam, K.J.; Brown, P.; Specht, L.; Christiansen, I.; Munksgaard, L.; Johnsen, H.E.; Loft, A.; Bukh, A.; Iyer, V.; et al. Positron emission tomography/computed tomography surveillance in patients with Hodgkin lymphoma in first remission has a low positive predictive value and high costs. Haematologica 2011, 97, 931–936. [Google Scholar] [CrossRef] [Green Version]
- Pingali, S.R.; Jewell, S.W.; Havlat, L.; Bast, M.A.; Thompson, J.R.; Eastwood, D.C.; Bartlett, N.L.; Armitage, J.O.; Wagner-Johnston, N.D.; Vose, J.M.; et al. Limited utility of routine surveillance imaging for classical Hodgkin lymphoma patients in first complete remission. Cancer 2014, 120, 2122–2129. [Google Scholar] [CrossRef]
- Burke, L.M.; Bashir, M.R.; Neville, A.M.; Nelson, R.C.; Jaffe, T.A. Current Opinions on Medical Radiation: A Survey of Oncologists Regarding Radiation Exposure and Dose Reduction in Oncology Patients. J. Am. Coll. Radiol. 2014, 11, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Eichenauer, D.A.; Engert, A.; André, M.; Federico, M.; Illidge, T.; Hutchings, M.; Ladetto, M.; ESMO Guidelines Working Group. Hodgkin’s lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014, 25 (Suppl. 3), 70–75. [Google Scholar] [CrossRef]
- Hoppe, R.T.; Advani, R.H.; Ai, W.Z.; Ambinder, R.F.; Aoun, P.; Armand, P.; Bello, C.M.; Benitez, C.M.; Bierman, P.J.; Chen, R.; et al. NCCN Guidelines Insights: Hodgkin Lymphoma, Version 1.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 245–254. [Google Scholar] [CrossRef] [Green Version]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. 2014, 32, 3059–3067. [Google Scholar] [CrossRef] [PubMed]
- Isasi, C.R.; Lu, P.; Blaufox, M.D. A metaanalysis of18F-2-deoxy-2-fluoro-D-glucose positron emission tomography in the staging and restaging of patients with lymphoma. Cancer 2005, 104, 1066–1074. [Google Scholar] [CrossRef] [PubMed]
- Henry-Amar, M.; Friedman, S.; Hayat, M.; Somers, R.; Meerwaldt, J.H.; Carde, P.; Burgers, J.M.; Thomas, J.; Monconduit, M.; Noordijk, E.M. Erythrocyte sedimentation rate predicts early relapse and survival in early-stage Hodgkin disease. The EORTC Lymphoma Cooperative Group. Ann. Intern. Med. 1991, 114, 361–365. [Google Scholar] [CrossRef]
- Friedman, S.; Henry-Amar, M.; Cosset, J.M.; Carde, P.; Hayat, M.; Dupouy, N.; Tubiana, M. Evolution of erythrocyte sedimentation rate as predictor of early relapse in posttherapy early-stage Hodgkin’s disease. J. Clin. Oncol. 1988, 6, 596–602. [Google Scholar] [CrossRef]
- Hartridge-Lambert, S.K.; Schöder, H.; Lim, R.C.; Maragulia, J.C.; Portlock, C.S. ABVD alone and a PET scan complete remission negates the need for radiologic surveillance in early-stage, nonbulky Hodgkin lymphoma. Cancer 2012, 119, 1203–1209. [Google Scholar] [CrossRef]
- Glober, G.; Gunther, J.; Fang, P.; Milgrom, S.; Korivi, B.R.; Jensen, C.T.; Wagner-Bartak, N.A.; Ahmed, S.; Lee, H.J.; Nair, R.; et al. Imaging Surveillance of Limited-stage Classic Hodgkin Lymphoma Patients After PETCT-documented First Remission. Clin. Lymphoma Myeloma Leuk. 2020, 20, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Juweid, M.E. Utility of positron emission tomography (PET) scanning in managing patients with Hodgkin lymphoma. Hematol. Am. Soc. Hematol. Educ. Program 2006, 259–265, 510–511. [Google Scholar] [CrossRef] [Green Version]
- Jochelson, M.; Mauch, P.; Balikian, J.; Rosenthal, D.; Canellos, G. The significance of the residual mediastinal mass in treated Hodgkin’s disease. J. Clin. Oncol. 1985, 3, 637–640. [Google Scholar] [CrossRef]
- Kobe, C.; Kuhnert, G.; Kahraman, D.; Haverkamp, H.; Eich, H.-T.; Franke, M.; Persigehl, T.; Klutmann, S.; Amthauer, H.; Bockisch, A.; et al. Assessment of tumor size reduction im-proves outcome prediction of positron emission tomography/computed tomography after chemotherapy in advanced stage Hodgkin lymphoma. J. Clin. Oncol. 2014, 32, 1776–1781. [Google Scholar] [CrossRef] [PubMed]
- Jerusalem, G.; Beguin, Y.; Fassotte, M.F.; Najjar, F.; Paulus, P.; Rigo, P.; Fillet, G. Wholebody positron emission tomography using 18F-fluorodeoxyglucose for posttreatment evaluation in Hodgkin’s disease and non-Hodgkin’s lymphoma has higher di-agnostic and prognostic value than classical computed tomography scan imaging. Blood 1999, 94, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Fallanca, F.; Giovacchini, G.; Ponzoni, M.; Gianolli, L.; Ciceri, F.; Fazio, F. Cervical thymic hyperplasia after chemotherapy in an adult patient with Hodgkin lymphoma: A potential cause of false-positivity on [18F]FDG PET/CT scanning. Br. J. Haematol. 2007, 140, 477. [Google Scholar] [CrossRef] [PubMed]
- Cardis, E.; Vrijheid, M.; Blettner, M.; Gilbert, E.; Hakama, M.; Hill, C.; Howe, G.; Kaldor, J.; Muirhead, C.R.; Schubauer-Berigan, M.; et al. Risk of cancer after low doses of ionising radiation: Retrospective cohort study in 15 countries. BMJ 2005, 331, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N = 640 Patients |
|---|---|
| Age (median) | 45.5 years (r: 18.2–93.2) |
| Histological Type | NSHL: 434 (67.8%) MCHL: 112 (17.5%) LRHL: 44 (6.9%) LDHL: 5 (0.8%) Not specified: 45 (7%) |
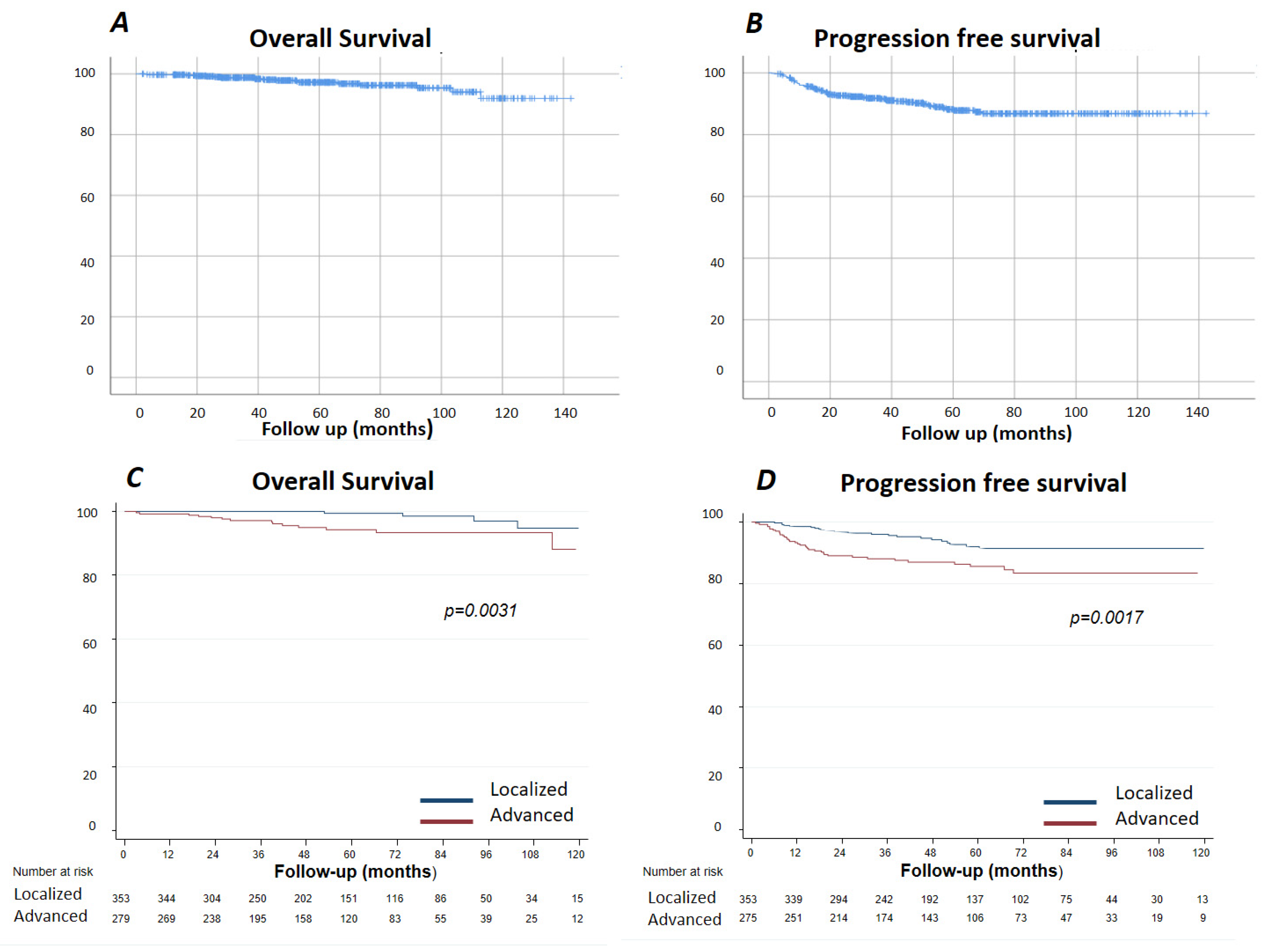
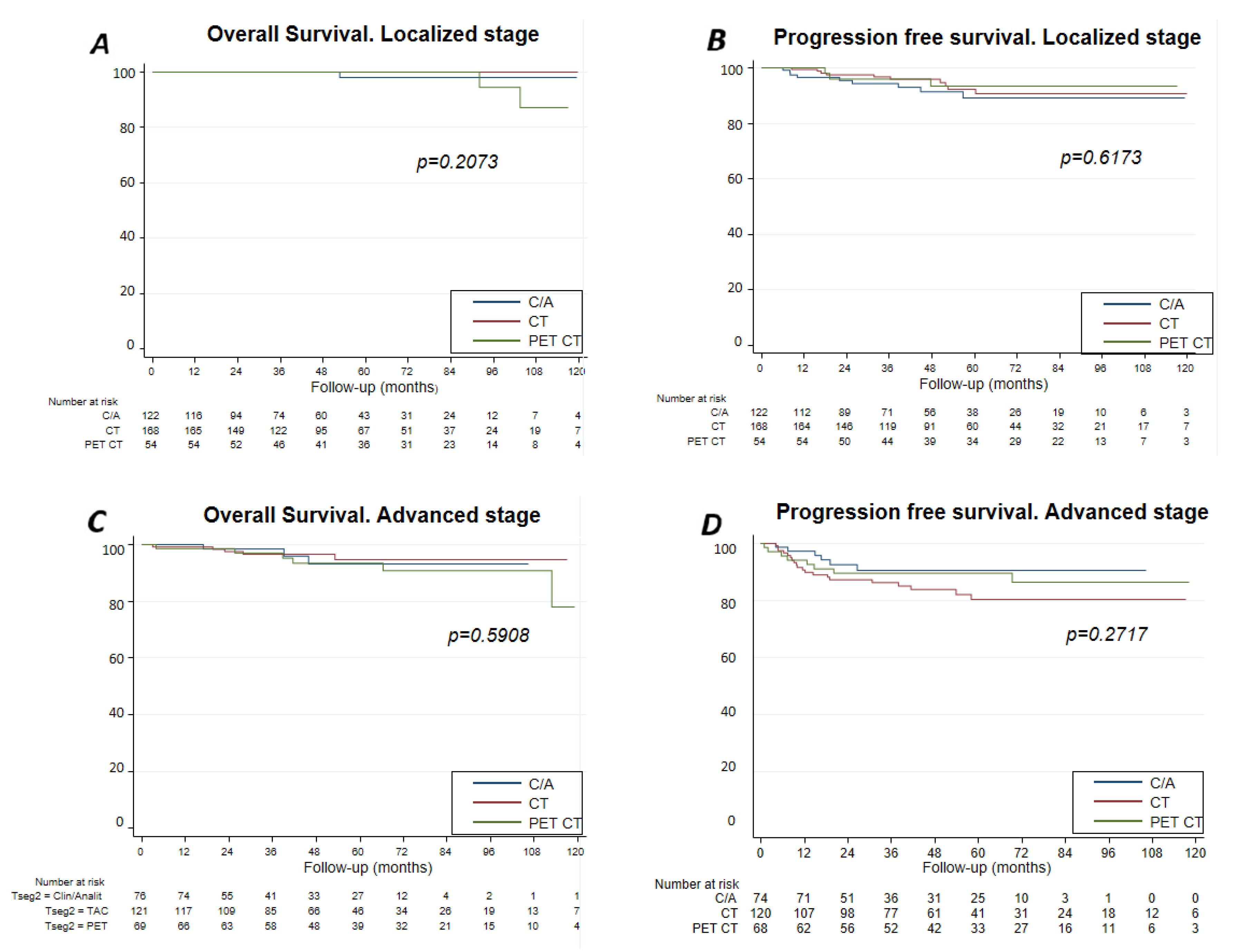
| Stage | I–II: 375 (58.6%) III–IV: 262 (41%) Missing data: 3 (0.4%) |
| Treatment Group | Favorable localized: 178 (27.8%) Unfavorable localized: 179 (28%) Advanced IPS 1–3: 166 (25.9%) Advanced IPS 4–7: 115 (18%) Missing data: 2 (0.3%) |
| Type of treatment | Radiotherapy: 35 (5.5%) Radiotherapy + chemotherapy: 253 (39.5%) Chemotherapy: 350 (54.7%) Missing data: 2 (0.3%) |
| Chemotherapy | ABVD: 564 (88.1%) BEACOPP: 37 (5.8%) Other: 29 (4.5%) Missing data: 10 (1.6%) |
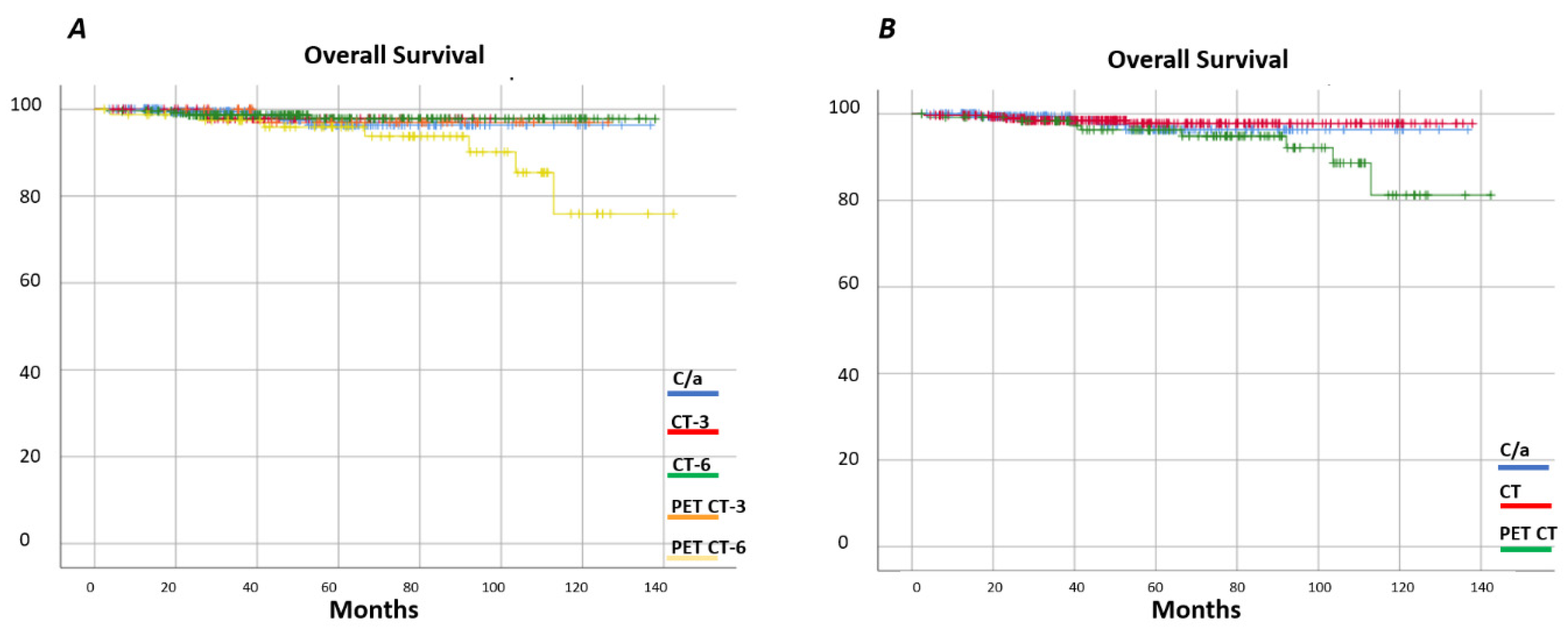
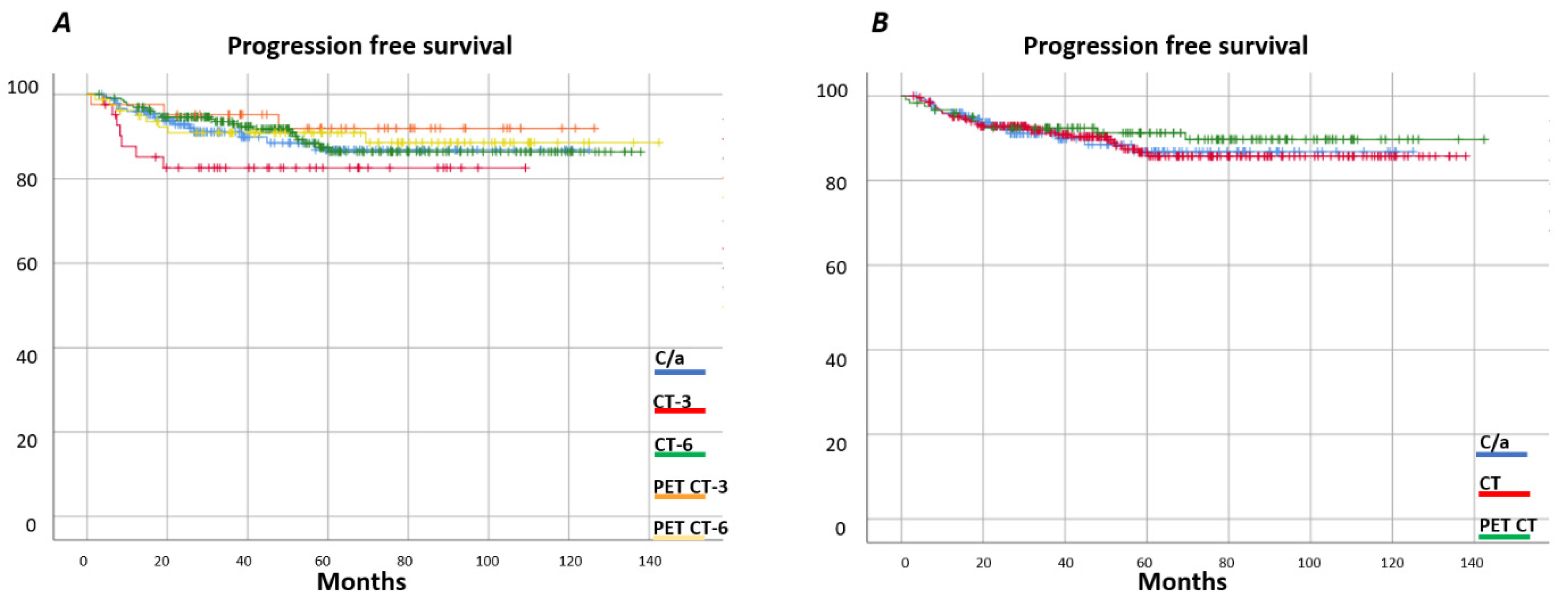
| Follow-up strategies | Clinical/analytical: 202 (31.6%) CT-Scan every 3 months: 58 (9.1%) CT- Scan every 6 months: 232 (36.3%) PET/CT every 3 months: 43 (6.7%) PET/CT every 6 months: 82 (12.8%) Missing data: 23 (3.5%) |
| Follow-Up Strategy | ||||||
|---|---|---|---|---|---|---|
| Clinical/Analytical (n = 202) | CT-Scan Every 3 Months (n = 58) | CT-Scan Every 6 Months (n = 232) | PET/CT Every 3 Months (n = 43) | PET/CT Every 6 Months (n = 82) | ||
| Age (median) | 46.9 (r:18.2–93.2) | 41.2 (r:20.7–84.7) | 45.6 (r:20.4–92.4%) | 44.2 (r:19.8–82.7) | 45.7 (r:20.1–90.2) | |
| Histological Type | NSHL | 125 (63.5%) | 47 (81%) | 149 (64.8%) | 39 (90.7%) | 58 (75.3%) |
| MCHL | 34 (17.3%) | 8 (13.8%) | 49 (21.3%) | 2 (4.7%) | 16 (20.8%) | |
| LRHL | 20(10.2%) | 1 (1.7%) | 17 (7.4%) | 1 (2.3%) | 3 (3.9%) | |
| LDHL | 1 (0.5%) | 0 (0%) | 3 (1.3%) | 0 (0%) | 0 (0%) | |
| Not specified | 17 (8.5%) | 2 (3.4%) | 12 (5.2%) | 1 (2.3%) | 0 (0%) | |
| Stage | I-II | 130 (64.7%) | 32 (55.1%) | 141 (60.8%) | 19 (44.2%) | 44 (54.3%) |
| III-IV | 71 (35.3%) | 26 (44.8%) | 91 (39.2%) | 24 (55.8%) | 37 (45.7%) | |
| Treatment Group | Favorable localized | 68 (33.8%) | 23 (39.7%) | 61 (26.3%) | 3 (7%) | 20 (24.4%) |
| Unfavorable localized | 57 (28.4%) | 8 (13.8%) | 76 (32.8%) | 13 (30.2%) | 19 (23.2%) | |
| Advanced IPI 1–3 | 46 (22.9%) | 10 (17.2%) | 68 (29.3%) | 17 (39.5%) | 17 (20.7%) | |
| Advanced IPI 4–7 | 30 (14.9%) | 17 (29.3%) | 27 (11.6%) | 10 (23.3%) | 26 (31.7%) | |
| Type of treatment | Radiotherapy | 6 (3%) | 13 (22.4%) | 15 (6.5%) | 1 (2.4%) | 0 (0%) |
| Chemo+Radiotherapy | 74 (36.6%) | 28 (48.3%) | 112 (48.3%) | 7 (16.7%) | 24 (29.3%) | |
| Chemotherapy | 122 (60.4%) | 17 (29.3%) | 105 (45.3%) | 34 (81%) | 58 (70.7%) | |
| Type of chemotherapy | ABVD | 171 (86.8%) | 56 (98.2%) | 217 (94.3%) | 39 (92.9%) | 59 (72%) |
| BEACOPP | 12 (6.1%) | 0 (0%) | 3 (1.3%) | 3 (7.1%) | 19 (23.2%) | |
| Other | 14 (7.1%) | 1 (1.8%) | 10 (4.3%) | 0 (0%) | 4 (4.9%) | |
| Follow-Up Strategy | p-Value | |||||
|---|---|---|---|---|---|---|
| Clinical/Analytical (n = 202) | CT-Scan Every 3 Months (n = 58) | CT-Scan Every 6 Months (n = 232) | PET/CT Every 3 Months (n = 43) | PET/CT Every 6 Months (n = 82) | ||
| Visits/year (median) | 4 (0–10) | 4 (2–12) | 4 (1–15) | 6 (2–21) | 4 (1–12) | <0.001 * |
| Median number of CT-scans (2y) (n = 579) | 1 (0–6) | 6 (2–10) | 3 (2–8) | 2 (0–4) | 0 (0–4) | 0.001 * |
| Median number of CT-scans (5y) (n = 319) | 3 (0–17) | 7 (3–14) | 5 (2–11) | 3 (0–7) | 0 (0–5) | <0.001 * |
| Median number of PET/CT (2y) (n = 579) | 0 (0–8) | 1 (1–6) | 0 (0–6) | 6 (1–10) | 3 (1–9) | <0.001 * |
| Median number of PET/CT (5y) (n = 319) | 0 (0–5) | 1 (1–7) | 0 (0–6) | 8 (3–16) | 6 (2–9) | <0.001 * |
| 2-year Cumulative Radiation Exposure (msV) (median) (n = 579) | 19.9 (0–140) | 126.68 (46.68–240.08) | 59.94 (0–200.04) | 80.16 (6.7–187.12) | 20.1 (13.4–140.22) | <0.001 * |
| 5-year Cumulative Radiation Exposure (msV) (median) (n = 319) | 40.1 (0–339.7) | 146.56 (66.64–326.62) | 99.9 (39.9–259.98) | 113.54 (20.1–206.86) | 40.2 (13.4–160.2) | <0.001 * |
| Findings that Identified Relapse | Relapse (n = 68) |
|---|---|
| Clinical History | 9 (13.2%) |
| Physical Examination | 10 (14.7%) |
| Laboratory abnormalities | 2 (2.9%) |
| Clinical History + Physical Examination | 5 (7.4%) |
| Clinical History + Physical Examination + Laboratory abnormalities | 8 (11.8%) |
| Clinical/ analytical + image | 8 (11.8%) |
| 42 (61.7%) | |
| CT-SCAN | 17 (25.1%) |
| PET/CT | 9 (13.1%) |
| 26 (38.2%) | |
| Type of laboratory finding | |
| Blood cell counts | 6 (33.3%) |
| ESR | 7 (38.8%) |
| LDH | 4 (22.2%) |
| Other | 1 (5.6%) |
| Surveillance Strategies | PFS at 12 Months | PFS at 24 Months | PSF at 60 Months | Median Time to Relapse (Month) |
|---|---|---|---|---|
| Clinical/analytical (n = 202) | 96% | 94% | 86% | 16.2 |
| CT-Scan every 3 months (n = 58) | 85% | 82% | 82% | 9.4 |
| CT-Scan every 6 months (n = 232) | 96% | 96% | 87% | 18.4 |
| PET/CT every 3 months (n = 43) | 97% | 92% | 92% | 19.2 |
| PET/CT every 6 months (n = 82) | 95% | 90% | 90% | 13.2 |
| CT-Scan, total (n = 290) | 95% | 92% | 92% | 14.2 |
| PET/CT, total (n = 125) | 95% | 92% | 88% | 16.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bastos Oreiro, M.; Martín, R.; Gomez, P.; López Muñoz, N.; Rodriguez, A.; Liébana, M.; Navarro, B.; Sánchez-González, B.; Marí, P.; Pérez de Oteiza, J.; et al. SEGHI Study: Defining the Best Surveillance Strategy in Hodgkin Lymphoma after First-Line Treatment. Cancers 2021, 13, 2412. https://doi.org/10.3390/cancers13102412
Bastos Oreiro M, Martín R, Gomez P, López Muñoz N, Rodriguez A, Liébana M, Navarro B, Sánchez-González B, Marí P, Pérez de Oteiza J, et al. SEGHI Study: Defining the Best Surveillance Strategy in Hodgkin Lymphoma after First-Line Treatment. Cancers. 2021; 13(10):2412. https://doi.org/10.3390/cancers13102412
Chicago/Turabian StyleBastos Oreiro, Mariana, Reyes Martín, Pilar Gomez, Nieves López Muñoz, Antonia Rodriguez, Marta Liébana, Belén Navarro, Blanca Sánchez-González, Pilar Marí, Jaime Pérez de Oteiza, and et al. 2021. "SEGHI Study: Defining the Best Surveillance Strategy in Hodgkin Lymphoma after First-Line Treatment" Cancers 13, no. 10: 2412. https://doi.org/10.3390/cancers13102412