
Predictive and Prognostic Biomarker Identification in a Large Cohort of Androgen Receptor-Positive Salivary Duct Carcinoma Patients Scheduled for Combined Androgen Blockade

 , ,
, ,  , ,
, , 
Abstract
:Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Cohort Description
2.2. Tumor Material Used for RNA Extraction, Immunohistochemistry and HER2 FISH
2.3. RNA Isolation
2.4. Pathway Activity Scores Measurement
2.5. cDNA Synthesis and SRD5A1 Expression Quantification
2.6. Statistical Analysis
2.6.1. Univariable Analysis
2.6.2. Multivariable Analysis
3. Results
3.1. Patient Cohort Description and Treatment Outcome
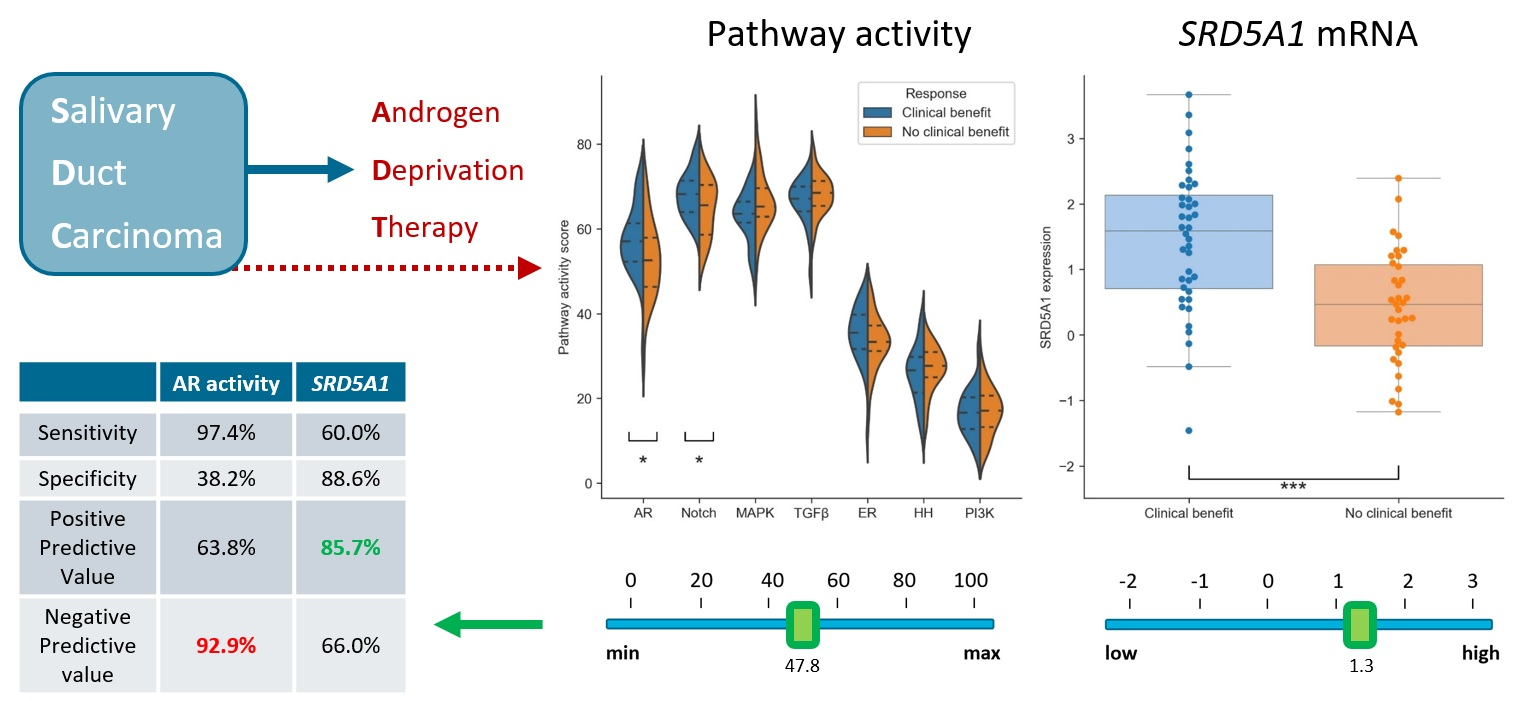
3.2. Predictive Value of Pathway Activity Scores and SRD5A1 Expression
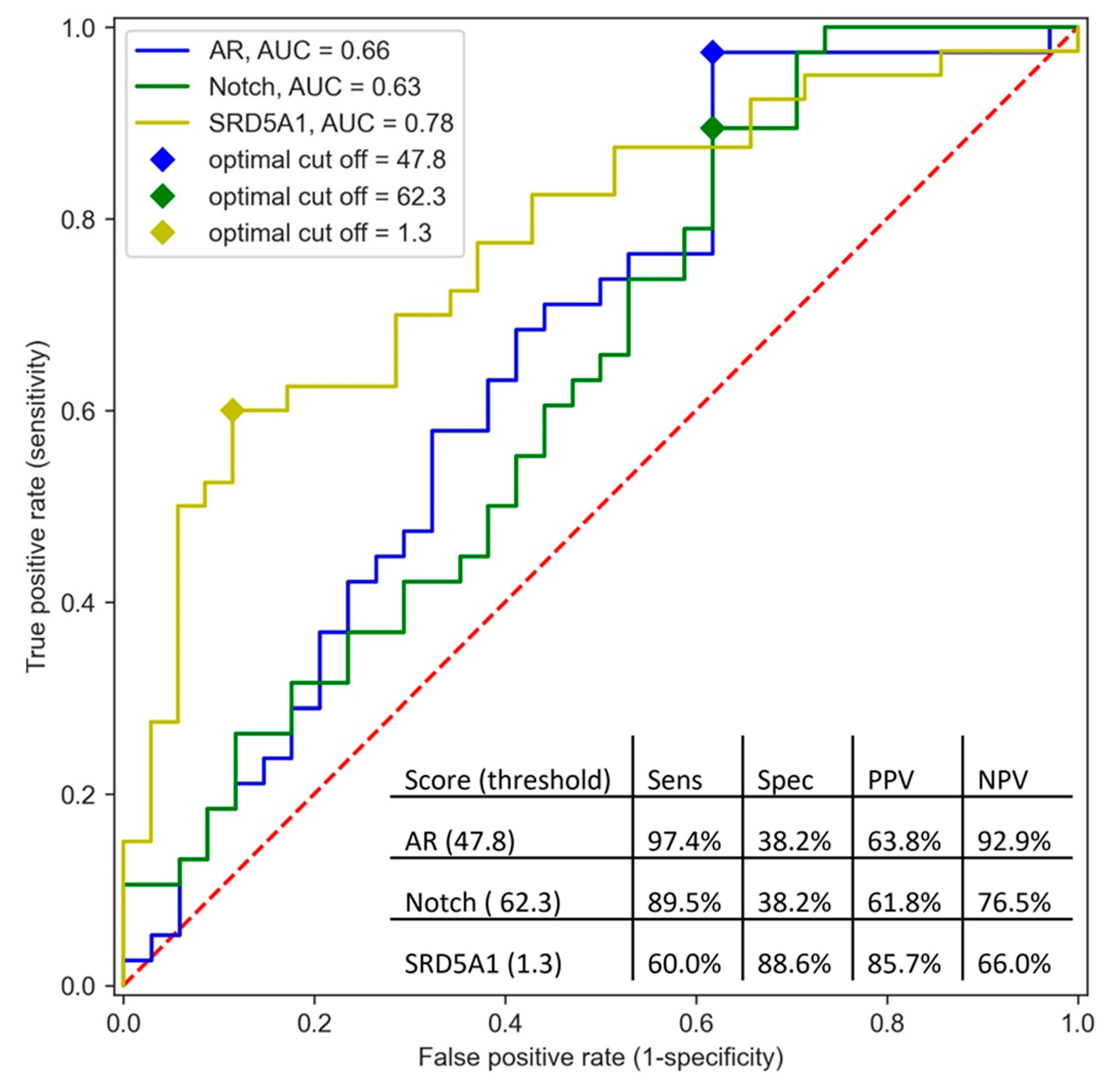
3.3. Clinical Benefit Prediction Using Multiple Pathways and SRD5A1 Expression
3.4. Optimizing Cut-Offs of AR Pathway Activity Score and SRD5A1 Expression to Prevent False Negatives
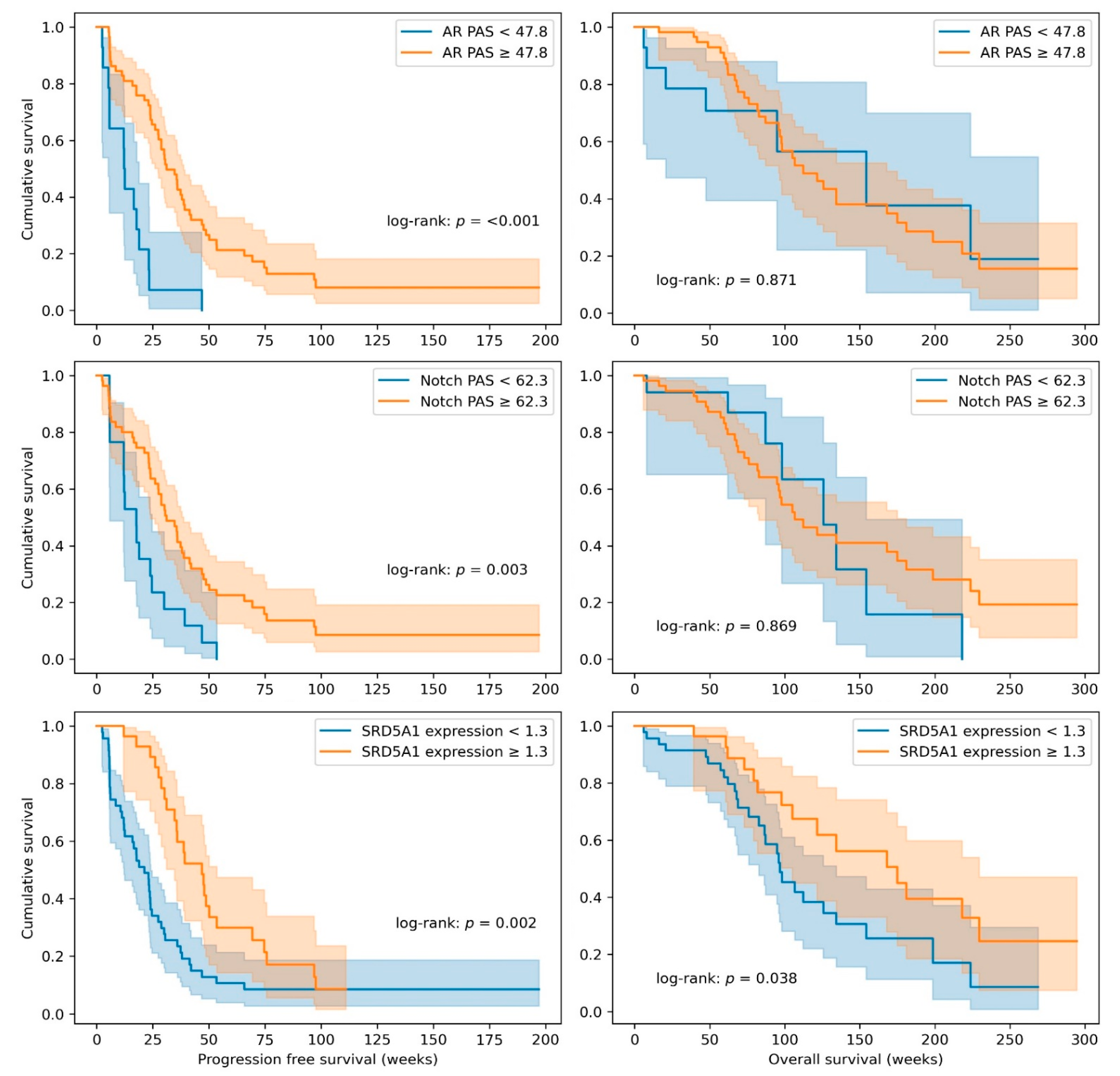
3.5. Prognostic Value of Pathway Activity Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours, 4th ed.; IARC: Lyon, France, 2017. [Google Scholar]
- Boon, E.; Bel, M.; van Boxtel, W.; van der Graaf, W.T.A.; van Es, R.J.J.; Eerenstein, S.E.J.; Baatenburg de Jong, R.J.; van den Brekel, M.W.M.; van der Velden, L.A.; Witjes, M.J.H.; et al. A clinicopathological study and prognostic factor analysis of 177 salivary duct carcinoma patients from The Netherlands. Int. J. Cancer 2018, 143, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, K.; Imanishi, Y.; Tada, Y.; Kawakita, D.; Kano, S.; Tsukahara, K.; Shimizu, A.; Ozawa, H.; Okami, K.; Sakai, A.; et al. Clinical Outcomes and Prognostic Factors for Salivary Duct Carcinoma: A Multi-Institutional Analysis of 141 Patients. Ann. Surg. Oncol. 2016, 23, 2038–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakaguro, M.; Tada, Y.; Faquin, W.C.; Sadow, P.M.; Wirth, L.J.; Nagao, T. Salivary duct carcinoma: Updates in histology, cytology, molecular biology, and treatment. Cancer Cytopathol. 2020, 128, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Boon, E.; van Boxtel, W.; Buter, J.; Baatenburg de Jong, R.J.; van Es, R.J.J.; Bel, M.; Fiets, E.; Oosting, S.F.; Slingerland, M.; Hoeben, A.; et al. Androgen deprivation therapy for androgen receptor-positive advanced salivary duct carcinoma: A nationwide case series of 35 patients in The Netherlands. Head Neck 2018, 40, 605–613. [Google Scholar] [CrossRef]
- Lassche, G.; van Boxtel, W.; Ligtenberg, M.J.L.; van Engen-van Grunsven, A.C.H.; van Herpen, C.M.L. Advances and challenges in precision medicine in salivary gland cancer. Cancer Treat. Rev. 2019, 80, 101906. [Google Scholar] [CrossRef]
- Schmitt, N.C.; Kang, H.; Sharma, A. Salivary duct carcinoma: An aggressive salivary gland malignancy with opportunities for targeted therapy. Oral Oncol. 2017, 74, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Uijen, M.J.M.; Lassche, G.; van Engen-van Grunsven, A.C.H.; Tada, Y.; Verhaegh, G.W.; Schalken, J.A.; Driessen, C.M.L.; van Herpen, C.M.L. Systemic therapy in the management of recurrent or metastatic salivary duct carcinoma: A systematic review. Cancer Treat. Rev. 2020, 89, 102069. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Tada, Y.; Saotome, T.; Akazawa, K.; Ojiri, H.; Fushimi, C.; Masubuchi, T.; Matsuki, T.; Tani, K.; Osamura, R.Y.; et al. Phase II Trial of Trastuzumab and Docetaxel in Patients With Human Epidermal Growth Factor Receptor 2-Positive Salivary Duct Carcinoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 125–134. [Google Scholar] [CrossRef]
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; den Broeck, T.V.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2020. [Google Scholar] [CrossRef]
- Fushimi, C.; Tada, Y.; Takahashi, H.; Nagao, T.; Ojiri, H.; Masubuchi, T.; Matsuki, T.; Miura, K.; Kawakita, D.; Hirai, H.; et al. A prospective phase II study of combined androgen blockade in patients with androgen receptor-positive metastatic or locally advanced unresectable salivary gland carcinoma. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2018, 29, 979–984. [Google Scholar] [CrossRef] [Green Version]
- Locati, L.D.; Perrone, F.; Cortelazzi, B.; Lo Vullo, S.; Bossi, P.; Dagrada, G.; Quattrone, P.; Bergamini, C.; Potepan, P.; Civelli, E.; et al. Clinical activity of androgen deprivation therapy in patients with metastatic/relapsed androgen receptor-positive salivary gland cancers. Head Neck 2016, 38, 724–731. [Google Scholar] [CrossRef]
- Viscuse, P.V.; Price, K.A.; Garcia, J.J.; Schembri-Wismayer, D.J.; Chintakuntlawar, A.V. First Line Androgen Deprivation Therapy vs. Chemotherapy for Patients With Androgen Receptor Positive Recurrent or Metastatic Salivary Gland Carcinoma-A Retrospective Study. Front. Oncol. 2019, 9, 701. [Google Scholar] [CrossRef] [Green Version]
- van Boxtel, W.; Verhaegh, G.W.; van Engen-van Grunsven, I.A.; van Strijp, D.; Kroeze, L.I.; Ligtenberg, M.J.; van Zon, H.B.; Hendriksen, Y.; Keizer, D.; van de Stolpe, A.; et al. Prediction of clinical benefit from androgen deprivation therapy in salivary duct carcinoma patients. Int. J. Cancer 2020, 146, 3196–3206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Stolpe, A.; Holtzer, L.; van Ooijen, H.; Inda, M.A.; Verhaegh, W. Enabling precision medicine by unravelling disease pathophysiology: Quantifying signal transduction pathway activity across cell and tissue types. Sci. Rep. 2019, 9, 1603. [Google Scholar] [CrossRef] [Green Version]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2018, 36, 2105–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Stolpe, A.; Verhaegh, W.; Blay, J.Y.; Ma, C.X.; Pauwels, P.; Pegram, M.; Prenen, H.; De Ruysscher, D.; Saba, N.F.; Slovin, S.F.; et al. RNA Based Approaches to Profile Oncogenic Pathways From Low Quantity Samples to Drive Precision Oncology Strategies. Front. Genet. 2020, 11, 598118. [Google Scholar] [CrossRef] [PubMed]
- van Ooijen, H.; Hornsveld, M.; Dam-de Veen, C.; Velter, R.; Dou, M.; Verhaegh, W.; Burgering, B.; van de Stolpe, A. Assessment of Functional Phosphatidylinositol 3-Kinase Pathway Activity in Cancer Tissue Using Forkhead Box-O Target Gene Expression in a Knowledge-Based Computational Model. Am. J. Pathol. 2018, 188, 1956–1972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verhaegh, W.; van Ooijen, H.; Inda, M.A.; Hatzis, P.; Versteeg, R.; Smid, M.; Martens, J.; Foekens, J.; van de Wiel, P.; Clevers, H.; et al. Selection of personalized patient therapy through the use of knowledge-based computational models that identify tumor-driving signal transduction pathways. Cancer Res. 2014, 74, 2936–2945. [Google Scholar] [CrossRef] [Green Version]
- Canté-Barrett, K.; Holtzer, L.; van Ooijen, H.; Hagelaar, R.; Cordo, V.; Verhaegh, W.; van de Stolpe, A.; Meijerink, J.P.P. A Molecular Test for Quantifying Functional Notch Signaling Pathway Activity in Human Cancer. Cancers 2020, 12, 3142. [Google Scholar] [CrossRef] [PubMed]
- Inda, M.A.; Blok, E.J.; Kuppen, P.J.K.; Charehbili, A.; den Biezen-Timmermans, E.C.; van Brussel, A.; Fruytier, S.E.; Meershoek-Klein Kranenbarg, E.; Kloet, S.; van der Burg, B.; et al. Estrogen Receptor Pathway Activity Score to Predict Clinical Response or Resistance to Neoadjuvant Endocrine Therapy in Primary Breast Cancer. Mol. Cancer Ther. 2020, 19, 680–689. [Google Scholar] [CrossRef] [Green Version]
- Sieuwerts, A.M.; Inda, M.A.; Smid, M.; van Ooijen, H.; van de Stolpe, A.; Martens, J.W.M.; Verhaegh, W.F.J. ER and PI3K Pathway Activity in Primary ER Positive Breast Cancer Is Associated with Progression-Free Survival of Metastatic Patients under First-Line Tamoxifen. Cancers 2020, 12, 802. [Google Scholar] [CrossRef] [Green Version]
- van de Stolpe, A. Quantitative Measurement of Functional Activity of the PI3K Signaling Pathway in Cancer. Cancers 2019, 11, 293. [Google Scholar] [CrossRef] [Green Version]
- van Lieshout, L.; van de Stolpe, A.; van der Ploeg, P.; Bowtell, D.; de Hullu, J.; Piek, J. Signal Transduction Pathway Activity in High-Grade, Serous Ovarian Carcinoma Reveals a More Favorable Prognosis in Tumors with Low PI3K and High NF-κB Pathway Activity: A Novel Approach to a Long-Standing Enigma. Cancers 2020, 12, 2660. [Google Scholar] [CrossRef]
- van Weelden, W.J.; van der Putten, L.J.M.; Inda, M.A.; van Brussel, A.; Snijders, M.; Schriever, L.M.M.; Bulten, J.; Massuger, L.; van de Stolpe, A.; Pijnenborg, J.M.A. Oestrogen receptor pathway activity is associated with outcome in endometrial cancer. Br. J. Cancer 2020, 123, 785–792. [Google Scholar] [CrossRef]
- Akaike, H. A new look at the statistical model identification. IEEE Trans. Autom. Control. 1974, 19, 716–723. [Google Scholar] [CrossRef]
- Heinlein, C.A.; Chang, C. Androgen receptor in prostate cancer. Endocr. Rev. 2004, 25, 276–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandrasekar, T.; Yang, J.C.; Gao, A.C.; Evans, C.P. Mechanisms of resistance in castration-resistant prostate cancer (CRPC). Transl. Androl. Urol. 2015, 4, 365–380. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.A.; Arora, V.K.; Sawyers, C.L. Emerging mechanisms of resistance to androgen receptor inhibitors in prostate cancer. Nat. Rev. Cancer 2015, 15, 701–711. [Google Scholar] [CrossRef] [Green Version]
- Hamid, A.R.; Verhaegh, G.W.; Smit, F.P.; van Rijt-van de Westerlo, C.; Armandari, I.; Brandt, A.; Sweep, F.C.; Sedelaar, J.P.; Schalken, J.A. Dutasteride and enzalutamide synergistically suppress prostate tumor cell proliferation. J. Urol. 2015, 193, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Orozco, M.; Valdez, R.A.; Ramos, L.; Cabeza, M.; Segovia, J.; Romano, M.C. Dutasteride combined with androgen receptor antagonists inhibit glioblastoma U87 cell metabolism, proliferation, and invasion capacity: Androgen regulation. Steroids 2020, 164, 108733. [Google Scholar] [CrossRef]
- Ferrarotto, R.; Mitani, Y.; Diao, L.; Guijarro, I.; Wang, J.; Zweidler-McKay, P.; Bell, D.; William, W.N., Jr.; Glisson, B.S.; Wick, M.J.; et al. Activating NOTCH1 Mutations Define a Distinct Subgroup of Patients With Adenoid Cystic Carcinoma Who Have Poor Prognosis, Propensity to Bone and Liver Metastasis, and Potential Responsiveness to Notch1 Inhibitors. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 352–360. [Google Scholar] [CrossRef]
- Ho, A.S.; Ochoa, A.; Jayakumaran, G.; Zehir, A.; Valero Mayor, C.; Tepe, J.; Makarov, V.; Dalin, M.G.; He, J.; Bailey, M.; et al. Genetic hallmarks of recurrent/metastatic adenoid cystic carcinoma. J. Clin. Investig. 2019, 129, 4276–4289. [Google Scholar] [CrossRef] [PubMed]
- Bray, S.J. Notch signalling in context. Nat. Rev. Mol. Cell Biol. 2016, 17, 722–735. [Google Scholar] [CrossRef] [PubMed]
- Ferrarotto, R.; Mitani, Y.; McGrail, D.J.; Li, K.; Karpinets, T.V.; Bell, D.; Frank, S.J.; Song, X.; Kupferman, M.E.; Liu, B.; et al. Proteogenomic Analysis of Salivary Adenoid Cystic Carcinomas Defines Molecular Subtypes and Identifies Therapeutic Targets. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2021, 27, 852–864. [Google Scholar] [CrossRef] [PubMed]
- Aldahl, J.; Yu, E.J.; He, Y.; Hooker, E.; Wong, M.; Le, V.; Olson, A.; Lee, D.H.; Kim, W.K.; Murtaugh, C.L.; et al. A pivotal role of androgen signaling in Notch-responsive cells in prostate development, maturation, and regeneration. Differentiation 2019, 107, 1–10. [Google Scholar] [CrossRef]
- Farah, E.; Li, C.; Cheng, L.; Kong, Y.; Lanman, N.A.; Pascuzzi, P.; Lorenz, G.R.; Zhang, Y.; Ahmad, N.; Li, L.; et al. NOTCH signaling is activated in and contributes to resistance in enzalutamide-resistant prostate cancer cells. J. Biol. Chem. 2019, 294, 8543–8554. [Google Scholar] [CrossRef]
- Bai, S.; Cao, S.; Jin, L.; Kobelski, M.; Schouest, B.; Wang, X.; Ungerleider, N.; Baddoo, M.; Zhang, W.; Corey, E.; et al. A positive role of c-Myc in regulating androgen receptor and its splice variants in prostate cancer. Oncogene 2019, 38, 4977–4989. [Google Scholar] [CrossRef]
- Alame, M.; Cornillot, E.; Cacheux, V.; Tosato, G.; Four, M.; De Oliveira, L.; Gofflot, S.; Delvenne, P.; Turtoi, E.; Cabello-Aguilar, S.; et al. The molecular landscape and microenvironment of salivary duct carcinoma reveal new therapeutic opportunities. Theranostics 2020, 10, 4383–4394. [Google Scholar] [CrossRef]
- Gargano, S.M.; Senarathne, W.; Feldman, R.; Florento, E.; Stafford, P.; Swensen, J.; Vranic, S.; Gatalica, Z. Novel therapeutic targets in salivary duct carcinoma uncovered by comprehensive molecular profiling. Cancer Med. 2019, 8, 7322–7329. [Google Scholar] [CrossRef] [Green Version]
- Ballman, K.V. Biomarker: Predictive or Prognostic? J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 3968–3971. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic, N (%) | N (%) | Number of Patients (n = 76) | ||
|---|---|---|---|---|
| Clinical Benefit 1 (n = 40) | No Clinical Benefit 1 (n = 36) | Difference | ||
| Age at diagnosis | p = 0.53 | |||
| Median (range) | 66.3 (46–83) | 65.2 (42–81) | ||
| Gender | p = 0.18 | |||
| Male | 39 (97.5) | 32 (88.9) | ||
| Female | 1 (2.5) | 4 (11.1) | ||
| Location primary tumor | p = 0.84 | |||
| Parotid | 28 (70.0) | 24 (66.7) | ||
| Sublingual | 0 (0) | 0 (0) | ||
| Submandibular | 9 (22.5) | 10 (27.8) | ||
| Minor | 3 (7.5) | 2 (5.6) | ||
| HER2 status 2 | p = 0.075 | |||
| Positive | 7 (17.5) | 13 (36.1) | ||
| Negative | 33 (82.5) | 23 (63.9) | ||
| HER2 IHC | p = 0.071 | |||
| 0 | 9 (22.5) | 9 (25.0) | ||
| 1+ | 17 (42.5) | 9 (25.0) | ||
| 2+ | 9 (22.5) | 5 (13.9) | ||
| 3+ | 5 (12.5) | 13 (36.1) | ||
| T-stage at diagnosis | p = 1.0 | |||
| 1–2 | 18 (45.0) | 15 (41.7) | ||
| 3–4 | 22 (55.0) | 20 (55.6) | ||
| Unknown | 0 (0) | 1 (2.7) | ||
| N-stage at diagnosis | p = 0.34 | |||
| 0 | 16 (40.0) | 10 (27.8) | ||
| 1–2 | 24 (60.0) | 26 (72.2) | ||
| M-stage at diagnosis | p = 0.36 | |||
| 0 | 32 (80.0) | 32 (88.9) | ||
| 1 | 8 (20.0) | 4 (11.1) | ||
| R/M | p = 0.41 | |||
| Locally advanced/recurrent | 7 (17.5) | 3 (8.3) | ||
| Metastatic | 27 (67.5) | 27 (75.0) | ||
| Both | 6 (15.0) | 6 (16.7) | ||
| Underwent surgery | p = 1.0 | |||
| Yes | 34 (85.0) | 31 (86.1) | ||
| No | 6 (15.0) | 5 (13.9) | ||
| Postoperative radiotherapy | p = 1.0 | |||
| Yes | 16 (40.0) | 15 (41.7) | ||
| No | 24 (60.0) | 21 (58.3) | ||
| CAB as first line | p = 0.43 | |||
| Yes | 28 (70.0) | 29 (80.6) | ||
| No | 12 (30.0) | 7 (19.4) | ||
| Post-CAB systemic treatment | p = 0.094 | |||
| Yes | 22 (55.0) | 27 (75.0) | ||
| No | 18 (45) | 9 (25.0) | ||
| Post-CAB anti-HER2 | p = 0.01 | |||
| Yes | 2 (5.0) | 10 (27.8) | ||
| No | 38 (95.0) | 26 (72.2) | ||
| Post-CAB chemotherapy | p < 0.001 | |||
| Yes | 9 (22.5) | 24 (66.7) | ||
| No | 31 (77.5) | 12 (33.3) | ||
| Post-CAB platinum- based treatment | p = 0.10 | |||
| Yes | 6 (15.0) | 12 (33.3) | ||
| No | 34 (85.0) | 24 (66.7) | ||
| Pathway | Clinical Benefit (Mean (Range)) | No Clinical Benefit (Mean (Range)) | Difference |
|---|---|---|---|
| AR | 57.5 (31.7–71.9) | 52.8 (29.6–71.9) | p = 0.02 |
| Notch | 68.1 (58.8–79.3) | 64.8 (52.2–76.0) | p = 0.05 |
| MAPK | 63.0 (47.8–73.2) | 66.4 (50.7–84.9) | p = 0.051 |
| TGFβ | 66.2 (49.2–74.5) | 68.2 (57.5–78.5) | p = 0.26 |
| ER | 35.3 (11.3–45.3) | 33.3 (16.7–44.9) | p = 0.097 |
| HH | 25.9 (11.3–38.9) | 26.8 (13.4–35.0) | p = 0.44 |
| PI3K 1 | 16.7 (6.5–32.9) | 16.7 (6.5–28.8) | p = 0.88 |
| SRD5A1 expression 2 | 1.45 (−1.46–3.67) | 0.42 (−1.18–2.39) | p < 0.001 |
| Pathway | Median PFS in Weeks (95% CI) | ||
|---|---|---|---|
| Below Median Score | Above Median Score | Difference 1 | |
| AR | 23 (19–28) | 36 (24–47) | p = 0.035 |
| Notch | 24 (19–28) | 31 (19–43) | p = 0.035 |
| MAPK | 30 (20–40) | 23 (13–33) | p = 0.41 |
| TGFβ | 30 (20–41) | 23 (17–30) | p = 0.40 |
| ER | 24 (22–26) | 35 (27–43) | p = 0.039 |
| HH | 30 (18–42) | 24 (18.0–30) | p = 0.007 |
| PI3K 2 | 29 (23–35) | 24 (16–32) | p = 0.995 |
| SRD5A1 | 18 (5–31) | 38 (34–42) | p = 0.003 |
| Below ROC cut-off | Above ROC cut-off | ||
| AR | 12 (11–13) | 31 (24–38) | p < 0.001 |
| Notch | 18 (10–25) | 31 (24–39) | p = 0.003 |
| SRD5A1 | 21 (13–29) | 47 (32–62) | p = 0.002 |
| Median OS in weeks [95% CI] | |||
| Below median score | Above median score | ||
| AR | 107 (66–147) | 122 (81–163) | p = 0.57 |
| Notch | 122 (93–151) | 112 (15–209) | p = 0.84 |
| MAPK | 112 (85–139) | 126 (76–175) | p = 0.74 |
| TGFβ | 122 (72–172) | 112 (71–154) | p = 0.27 |
| ER | 126 (87–165) | 112 (75–149) | p = 0.59 |
| HH | 154 (68–241) | 107 (83–130) | p = 0.16 |
| PI3K 2 | 121 (76–167) | 105 (93–117) | p = 0.73 |
| SRD5A1 | 97 (83–111) | 168 (99–237) | p = 0.11 |
| Below ROC cut-off | Above ROC cut-off | ||
| AR | 154 (39–270) | 112 (82–143) | p = 0.87 |
| Notch | 126 (85–166) | 107 (79–135) | p = 0.87 |
| SRD5A1 | 97 (82–111) | 175 (96–254) | p = 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lassche, G.; Tada, Y.; van Herpen, C.M.L.; Jonker, M.A.; Nagao, T.; Saotome, T.; Hirai, H.; Saigusa, N.; Takahashi, H.; Ojiri, H.; et al. Predictive and Prognostic Biomarker Identification in a Large Cohort of Androgen Receptor-Positive Salivary Duct Carcinoma Patients Scheduled for Combined Androgen Blockade. Cancers 2021, 13, 3527. https://doi.org/10.3390/cancers13143527
Lassche G, Tada Y, van Herpen CML, Jonker MA, Nagao T, Saotome T, Hirai H, Saigusa N, Takahashi H, Ojiri H, et al. Predictive and Prognostic Biomarker Identification in a Large Cohort of Androgen Receptor-Positive Salivary Duct Carcinoma Patients Scheduled for Combined Androgen Blockade. Cancers. 2021; 13(14):3527. https://doi.org/10.3390/cancers13143527
Chicago/Turabian StyleLassche, Gerben, Yuichiro Tada, Carla M. L. van Herpen, Marianne A. Jonker, Toshitaka Nagao, Takashi Saotome, Hideaki Hirai, Natsuki Saigusa, Hideaki Takahashi, Hiroya Ojiri, and et al. 2021. "Predictive and Prognostic Biomarker Identification in a Large Cohort of Androgen Receptor-Positive Salivary Duct Carcinoma Patients Scheduled for Combined Androgen Blockade" Cancers 13, no. 14: 3527. https://doi.org/10.3390/cancers13143527
APA StyleLassche, G., Tada, Y., van Herpen, C. M. L., Jonker, M. A., Nagao, T., Saotome, T., Hirai, H., Saigusa, N., Takahashi, H., Ojiri, H., van Engen-Van Grunsven, A. C. H., Schalken, J. A., Fushimi, C., & Verhaegh, G. W. (2021). Predictive and Prognostic Biomarker Identification in a Large Cohort of Androgen Receptor-Positive Salivary Duct Carcinoma Patients Scheduled for Combined Androgen Blockade. Cancers, 13(14), 3527. https://doi.org/10.3390/cancers13143527