
Satisfaction with Fertility Preservation Decisions among Adolescent Males with Cancer: A Mixed Methods Study

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Procedure
2.2. Quantitative Analysis
2.3. Qualitative Analysis
2.4. Mixed Methods Approach
3. Results
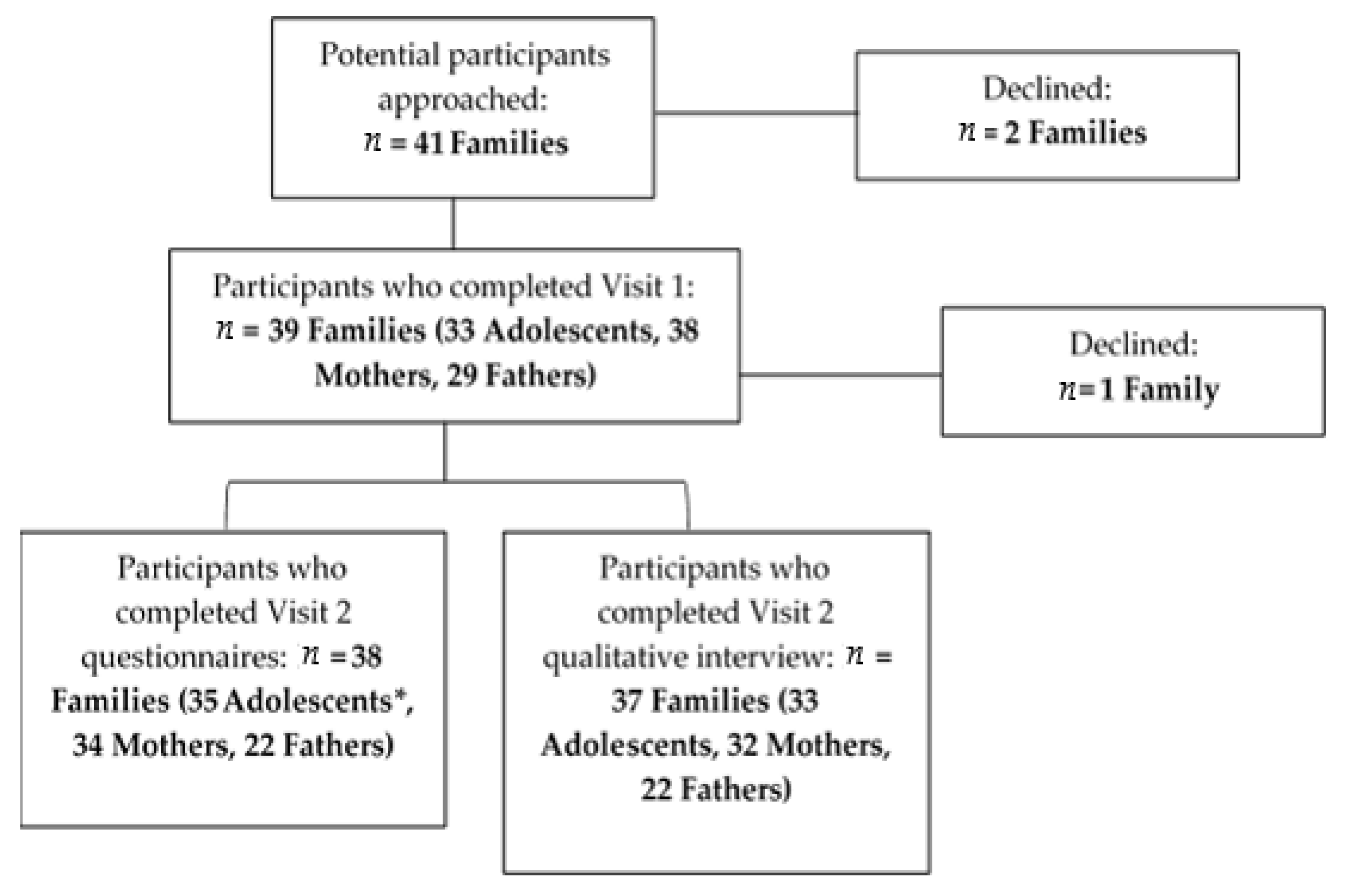
3.1. Participants
3.2. Quantitative Results
3.3. Qualitative Results
3.3.1. Non-Attempter Group Themes
Potential for Future Regret
Acceptance of the Decision
Satisfaction with the Decision
3.3.2. Attempter Group Themes
Satisfaction with the Decision
3.4. Mixed Methods Results
4. Discussion
Limitations
5. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abram McBride, J.; Lipshultz, L.I. Male Fertility Preservation. Curr. Urol. Rep. 2018, 19, 49. [Google Scholar] [CrossRef]
- National Cancer Institute: Surveillance E, a.E.R.P., Cancer Stat Facts: Cancer Among Adolescents and Young Adults (AYAs) (Ages 15–39). 2020. Available online: https://seer.cancer.gov/statfacts/html/aya.html (accessed on 6 June 2021).
- Green, D.M.; Liu, W.; Kutteh, W.H.; Ke, R.W.; Shelton, K.C.; Sklar, C.A.; Chemaitilly, W.; Pui, C.H.; Klosky, J.L.; Spunt, S.L.; et al. Cumulative alkylating agent exposure and semen parameters in adult survivors of childhood cancer: A report from the St Jude Lifetime Cohort Study. Lancet Oncol. 2014, 15, 1215–1223. [Google Scholar] [CrossRef] [Green Version]
- Armuand, G.M.; Wettergren, L.; Rodriguez-Wallberg, K.A.; Lampic, C. Desire for children, difficulties achieving a pregnancy, and infertility distress 3 to 7 years after cancer diagnosis. Support Care Cancer 2014, 22, 2805–2812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehmann, V.; Keim, M.C.; Nahata, L.; Shultz, E.L.; Klosky, J.L.; Tuinman, M.A.; Gerhardt, C.A. Fertility-related knowledge and reproductive goals in childhood cancer survivors: Short communication. Hum. Reprod. 2017, 32, 2250–2253. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.M.; Victorson, D.E.; Choy, J.T.; Waimey, K.E.; Pearman, T.P.; Smith, K.; Dreyfuss, J.; Kinahan, K.E.; Sadhwani, D.; Woodruff, T.K.; et al. Fertility Preservation Preferences and Perspectives Among Adult Male Survivors of Pediatric Cancer and Their Parents. J. Adolesc. Young Adult Oncol. 2014, 3, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Ellis, S.J.; Wakefield, C.E.; McLoone, J.K.; Robertson, E.G.; Cohn, R.J. Fertility concerns among child and adolescent cancer survivors and their parents: A qualitative analysis. J. Psychosoc. Oncol. 2016, 34, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Klosky, J.L.; Simmons, J.L.; Russell, K.M.; Foster, R.H.; Sabbatini, G.M.; Canavera, K.E.; Hodges, J.R.; Schover, L.R.; McDermott, M.J. Fertility as a priority among at-risk adolescent males newly diagnosed with cancer and their parents. Support Care Cancer 2015, 23, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Burns, K.C.; Hoefgen, H.; Strine, A.; Dasgupta, R. Fertility preservation options in pediatric and adolescent patients with cancer. Cancer 2018, 124, 1867–1876. [Google Scholar] [CrossRef] [Green Version]
- Moravek, M.B.; Appiah, L.C.; Anazodo, A.; Burns, K.C.; Gomez-Lobo, V.; Hoefgen, H.R.; Jaworek Frias, O.; Laronda, M.M.; Levine, J.; Meacham, L.R.; et al. Development of a Pediatric Fertility Preservation Program: A Report From the Pediatric Initiative Network of the Oncofertility Consortium. J. Adolesc. Health 2019, 64, 563–573. [Google Scholar] [CrossRef]
- Tam, S.; Puri, N.; Stephens, D.; Mitchell, L.; Giuliani, M.; Papadakos, J.; Gupta, A.A. Improving Access to Standardized Fertility Preservation Information for Older Adolescents and Young Adults with Cancer: Using a User-Centered Approach with Young Adult Patients, Survivors, and Partners to Refine Fertility Knowledge Transfer. J. Cancer. Educ. 2018, 33, 528–535. [Google Scholar] [CrossRef]
- Saraf, A.J.; Stanek, J.; Audino, A.; DaJusta, D.; Hansen-Moore, J.; McCracken, K.; Whiteside, S.; Yeager, N.; Nahata, L. Examining predictors and outcomes of fertility consults among children, adolescents, and young adults with cancer. Pediatr. Blood Cancer 2018, 65, e27409. [Google Scholar] [CrossRef]
- von Bertalanffy, L.; Sutherland, J.W. General Systems Theory: Foundations, Developments, Applications. IEEE Trans. Syst. Man Cybern. 1974, SMC-4, 592. [Google Scholar] [CrossRef]
- Cox, M.J.; Paley, B. Understanding Families as Systems. Curr. Dir. Psychol. Sci. 2003, 12, 193–196. [Google Scholar] [CrossRef]
- Flynn, J.S.; Russell, K.M.; Lehmann, V.; Schenck, L.A.; Klosky, J.L. Parent recommendation to bank sperm among at-risk adolescent and young adult males with cancer. Pediatr. Blood Cancer 2020, e28217. [Google Scholar] [CrossRef] [PubMed]
- Klosky, J.L.; Flynn, J.S.; Lehmann, V.; Russell, K.M.; Wang, F.; Hardin, R.N.; Eddinger, J.R.; Zhang, H.; Schenck, L.A.M.; Schover, L.R. Parental influences on sperm banking attempts among adolescent males newly diagnosed with cancer. Fertil. Steril. 2017, 108, 1043–1049. [Google Scholar] [CrossRef] [Green Version]
- Klosky, J.L.; Wang, F.; Russell, K.M.; Zhang, H.; Flynn, J.S.; Huang, L.; Wasilewski-Masker, K.; Landier, W.; Leonard, M.; Albritton, K.H.; et al. Prevalence and Predictors of Sperm Banking in Adolescents Newly Diagnosed With Cancer: Examination of Adolescent, Parent, and Provider Factors Influencing Fertility Preservation Outcomes. J. Clin. Oncol. 2017, 35, 3830–3836. [Google Scholar] [CrossRef] [PubMed]
- Nurmi, J.-E.; Poole, M.E.; Kalakoski, V. Age differences in adolescent future-oriented goals, concerns, and related temporal extension in different sociocultural contexts. J. Youth Adolesc. 1994, 23, 471–487. [Google Scholar] [CrossRef]
- Logan, S.; Perz, J.; Ussher, J.M.; Peate, M.; Anazodo, A. Systematic review of fertility-related psychological distress in cancer patients: Informing on an improved model of care. Psychooncology 2019, 28, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Olsavsky, A.L.; Theroux, C.I.; Dattilo, T.M.; Klosky, J.L.; O’Brien, S.H.; Quinn, G.P.; Gerhardt, C.A.; Nahata, L. Family communication about fertility preservation in adolescent males newly diagnosed with cancer. Pediatr. Blood Cancer 2021, 68, e28978. [Google Scholar] [CrossRef]
- Becerra Pérez, M.M.; Menear, M.; Brehaut, J.C.; Légaré, F. Extent and Predictors of Decision Regret about Health Care Decisions: A Systematic Review. Med. Decis. Mak. 2016, 36, 777–790. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.A.; Wray, N.P.; Ashton, C.M. Living with treatment decisions: Regrets and quality of life among men treated for metastatic prostate cancer. J. Clin. Oncol. 2001, 19, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Müller, M.; Urech, C.; Boivin, J.; Ehrbar, V.; Moffat, R.; Daellenbach, R.Z.; Rochlitz, C.; Tschudin, S. Addressing decisional conflict about fertility preservation: Helping young female cancer survivors’ family planning decisions. BMJ Sex. Amp Reprod. Health 2018, 44, 175–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastings, L.; Baysal, Ö.; Beerendonk, C.C.; IntHout, J.; Traas, M.A.; Verhaak, C.M.; Braat, D.D.; Nelen, W.L. Deciding about fertility preservation after specialist counselling. Hum. Reprod. 2014, 29, 1721–1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedict, C.; Thom, B.; Kelvin, J.F. Young Adult Female Cancer Survivors’ Decision Regret About Fertility Preservation. J. Adolesc. Young Adult. Oncol. 2015, 4, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Chan, C.H.Y.; Lau, H.P.B.; Tam, M.Y.J.; Ng, E.H.Y. A longitudinal study investigating the role of decisional conflicts and regret and short-term psychological adjustment after IVF treatment failure. Hum. Reprod. 2016, 31, 2772–2780. [Google Scholar] [CrossRef] [PubMed]
- October, T.W.; Jones, A.H.; Greenlick Michals, H.; Hebert, L.M.; Jiang, J.; Wang, J. Parental Conflict, Regret, and Short-term Impact on Quality of Life in Tracheostomy Decision-Making. Pediatr. Crit. Care Med. 2020, 21, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Jokisaari, M. Regret appraisals, age, and subjective well-being. J. Res. Pers. 2003, 37, 487–503. [Google Scholar] [CrossRef]
- Campbell, A.G.; Hillemeier, M. Fertility counseling information adequacy as a moderator of regret among adolescent and young adult breast cancer survivors. Support Care Cancer 2021, 29, 2689–2697. [Google Scholar] [CrossRef]
- Letourneau, J.M.; Ebbel, E.E.; Katz, P.P.; Katz, A.; Ai, W.Z.; Chien, A.J.; Melisko, M.E.; Cedars, M.I.; Rosen, M.P. Pretreatment fertility counseling and fertility preservation improve quality of life in reproductive age women with cancer. Cancer 2012, 118, 1710–1717. [Google Scholar] [CrossRef] [Green Version]
- Nahata, L.; Dattilo, T.M.; Olsavsky, A.L.; Lipak, K.G.; Whiteside, S.; Yeager, N.D.; Audino, A.; Klosky, J.L.; Rausch, J.; Saraf, A.; et al. Impact of a novel family-centered values clarification tool on adolescent sperm banking attempts at the time of a new cancer diagnosis. J. Assist. Reprod. Genet. 2021. [Google Scholar] [CrossRef]
- Ehrbar, V.; Germeyer, A.; Nawroth, F.; Dangel, A.; Findeklee, S.; Urech, C.; Rochlitz, C.; Stiller, R.; Tschudin, S. Long-term effectiveness of an online decision aid for female cancer patients regarding fertility preservation: Knowledge, attitude, and decisional regret. Acta. Obstet. Gynecol. Scand. 2021. [Google Scholar] [CrossRef]
- Rubin, D.C. On the retention function for autobiographical memory. J. Verbal Learning Verbal Behav. 1982, 21, 21–38. [Google Scholar] [CrossRef] [Green Version]
- Mohamedali, H.Z.; Breunis, H.; Panju, A.; Alibhai, S.M.H. Information needs, decisional regret and satisfaction of older and younger adults with acute myeloid leukemia. J. Geriatr. Oncol. 2010, 1, 66–72. [Google Scholar] [CrossRef]
- Resnicow, K.; Abrahamse, P.; Tocco, R.S.; Hawley, S.; Griggs, J.; Janz, N.; Fagerlin, A.; Wilson, A.; Ward, K.C.; Gabram, S.G.A.; et al. Development and psychometric properties of a brief measure of subjective decision quality for breast cancer treatment. BMC Med. Inform. Decis. Mak. 2014, 14, 110. [Google Scholar] [CrossRef] [Green Version]
- IBM SPSS Statistics for Windows. 2017. Version 25.0. Available online: https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-25 (accessed on 6 June 2021).
- Glaser, B.G. The Constant Comparative Method of Qualitative Analysis. Social Problems 2014, 12, 436–445. [Google Scholar] [CrossRef]
- Guetterman, T.C.; Fetters, M.D.; Creswell, J.W. Integrating Quantitative and Qualitative Results in Health Science Mixed Methods Research Through Joint Displays. Ann. Fam. Med. 2015, 13, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Peate, M.; Meiser, B.; Cheah, B.C.; Saunders, C.; Butow, P.; Thewes, B.; Hart, R.; Phillips, K.A.; Hickey, M.; Friedlander, M. Making hard choices easier: A prospective, multicentre study to assess the efficacy of a fertility-related decision aid in young women with early-stage breast cancer. Br. J. Cancer. 2012, 106, 1053–1061. [Google Scholar] [CrossRef] [Green Version]
- Ehrbar, V.; Urech, C.; Rochlitz, C.; Zanetti Dällenbach, R.; Moffat, R.; Stiller, R.; Germeyer, A.; Nawroth, F.; Dangel, A.; Findeklee, S.; et al. Randomized controlled trial on the effect of an online decision aid for young female cancer patients regarding fertility preservation. Hum. Reprod. 2019, 34, 1726–1734. [Google Scholar] [CrossRef]
- Wyns, C.; Collienne, C.; Shenfield, F.; Robert, A.; Laurent, P.; Roegiers, L.; Brichard, B. Fertility preservation in the male pediatric population: Factors influencing the decision of parents and children. Hum. Reprod. 2015, 30, 2022–2030. [Google Scholar] [CrossRef] [Green Version]
- Lim, J.-W.; Shon, E.-J. Decisional Conflict: Relationships Between and Among Family Context Variables in Cancer Survivors. Oncol. Nurs. Forum. 2016, 43, 480. [Google Scholar] [CrossRef]
- Nahata, L.; Morgan, T.L.; Lipak, K.G.; Clark, O.E.; Yeager, N.D.; O’Brien, S.H.; Whiteside, S.; Audino, A.; Quinn, G.P.; Gerhardt, C.A. Perceptions of participating in family-centered fertility research among adolescent and young adult males newly diagnosed with cancer: A qualitative study. Pediatric. Blood Cancer 2019, 66, e27966. [Google Scholar] [CrossRef]
- Morgan, T.L.; Clark, O.E.; Whiteside, S.; Audino, A.; Yeager, N.D.; Klosky, J.L.; O’Brien, S.H.; Quinn, G.P.; Gerhardt, C.A.; Nahata, L. Recruiting families and children newly diagnosed with cancer for behavioral research: Important considerations and successful strategies. Psychooncology 2019, 28, 928–930. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Lee, S. Regret appraisals, Coping Styles of Regret and Subjective Well-Being in Middle Aged Women. Psychology 2015. [Google Scholar] [CrossRef]
- Ano, G.G.; Vasconcelles, E.B. Religious coping and psychological adjustment to stress: A meta-analysis. J. Clin. Psychol. 2005, 61, 461–480. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, S.P.; Macêdo, D.S.; Sales, P.M.; Figueiredo, S.M.; Daher, E.F.; Araújo, S.M.; Pargament, K.I.; Hyphantis, T.N.; Carvalho, A.F. The relationship between religious coping, psychological distress and quality of life in hemodialysis patients. J. Psychosom. Res. 2012, 72, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.L.; Chien, C.H.; Hsieh, C.Y.; Huang, X.Y.; Wang, H.H.; Lin, K.J.; Chiang, Y.J. Effective Decision-Making and Decisional Regret in Living Kidney Donors of Taiwan. Transpl. Proc. 2018, 50, 3059–3064. [Google Scholar] [CrossRef]

{kind=link}
| Sample Characteristics | Adolescents | Mothers | Fathers | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Race | ||||||
| White | 27 | 77% | 30 | 88% | 19 | 86% |
| Black | 2 | 5% | 3 | 9% | - | -- |
| Native Hawaiian/Pacific Islander | 4 | 11% | 1 | 3% | 1 | 5% |
| Other | 2 | 6% | - | -- | 2 | 9% |
| Ethnicity | ||||||
| Non-Hispanic/Latino | 30 | 86% | 34 | 100% | 20 | 91% |
| Hispanic/Latino | 1 | 3% | - | -- | 1 | 5% |
| Relationship Status | ||||||
| Single/Separated/Divorced | 23 | 66% | 7 | 21% | 5 | 23% |
| Married/Engaged/In a Serious Relationship | 8 | 23% | 27 | 79% | 17 | 77% |
| Religion | ||||||
| Christian | 19 | 54% | 28 | 82% | 13 | 59% |
| Catholic | 3 | 9% | - | -- | 1 | 5% |
| Jewish | 1 | 3% | 1 | 3% | 1 | 5% |
| Muslim | - | -- | 1 | 3% | - | -- |
| Agnostic | 1 | 3% | 1 | 3% | 3 | 14% |
| None | 5 | 14% | 2 | 6% | 3 | 14% |
| Other | 2 | 6% | 1 | 3% | 1 | 5% |
| Income | ||||||
| Less than USD 25,000 | 3 | 9% | 1 | 5% | ||
| USD 25,000–USD 49,999 | 7 | 21% | 2 | 9% | ||
| USD 50,000–USD 74,999 | 6 | 18% | 4 | 18% | ||
| USD 75,000–USD 99,999 | 8 | 24% | 5 | 23% | ||
| USD 100,000–USD 149,999 | 4 | 12% | 4 | 18% | ||
| USD 150,000 or more | 4 | 12% | 6 | 27% | ||
| Unsure | 2 | 6% | ||||
| Level of Education | ||||||
| Some High School | 2 | 6% | ||||
| High School Diploma or GED | 6 | 18% | 2 | 9% | ||
| Some College, No Degree | 6 | 18% | 9 | 41% | ||
| Associate Degree | 5 | 15% | 2 | 9% | ||
| Bachelor’s Degree | 11 | 32% | 4 | 18% | ||
| Graduate or Professional Degree | 3 | 9% | 4 | 18% | ||
| Other | 1 | 3% | 1 | 5% | ||
| Diagnosis Type | ||||||
| Brain or Spinal Cord Tumor | 4 | 11% | ||||
| Leukemia | 8 | 23% | ||||
| Lymphoma | 12 | 34% | ||||
| Solid Tumors | 10 | 29% | ||||
| Other | 1 | 3% | ||||
| Risk for Infertility | ||||||
| Minimally Increased Risk | 13 | 37% | ||||
| High Level of Increased Risk | 22 | 63% | ||||
| Comparison of Decision Quality Scores between Attempter and Non-Attempter Families a | Attempters | Non-Attempters | Composite Score | ||||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | t-Test | p | d | |
| Patient BSDQ Score | 5.76 | 0.97 | 5.68 | 1.03 | 5.79 | 0.98 | −0.23 | 0.821 | 0.08 |
| Mother BSDQ Score | 6.13 | 0.72 | 5.68 | 1.02 | 5.98 | 0.94 | −1.18 | 0.255 | 0.45 |
| Father BSDQ Score | 6.44 | 0.61 | 6.17 | 0.61 | 6.37 | 0.61 | −1.02 | 0.322 | 0.44 |
| Variable | n | M | SD | t-Test | df | p |
|---|---|---|---|---|---|---|
| Adolescents vs. Mothers | −1.61 | 31 | 0.119 | |||
| Adolescents | 32 | 5.79 | 0.98 | |||
| Mothers | 32 | 5.97 | 0.94 | |||
| Adolescents vs. Fathers | −2.26 | 19 | 0.036 * | |||
| Adolescents | 20 | 5.93 | 0.90 | |||
| Fathers | 20 | 6.37 | 0.61 | |||
| Mothers vs. Fathers | −1.31 | 17 | 0.209 | |||
| Mothers | 18 | 6.18 | 0.95 | |||
| Fathers | 18 | 6.44 | 0.52 |
| Domains | Qualitative Investigation | Frequency (%) | Quantitative Investigation * | Mixed Methods Interpretation |
|---|---|---|---|---|
| Non-attempter group | Quantitively, short-term decisional satisfaction was high regardless of banking decision. However, qualitative findings suggest experiences of families who did not bank may be more nuanced, as participants in this group reported a potential for future regret as well as a sense of acceptance with their decision. | |||
| Potential for regret | “My biggest fear is that he would regret it later.” (Mother of a 12-year-old, acute myeloid leukemia) “I mean obviously if we get 15 years down the road or whatever and he and his future wife are having trouble conceiving a child, there probably is gonna be a time where we’re gonna look at each other and go, did we do the right thing?” (Father of a 13-year-old, acute myeloid leukemia) “I feel like it could have been a good thing but just at that time it wasn’t…something we really could have done…(how I feel in the future) dependss if I’m fertile or not...” (14-year-old, osteosarcoma) | Overall: 50% Adolescents: 36% Mothers: 45%, Fathers: 44% | BSDQ Means: Adolescents: M = 5.68 Mothers: M = 5.68 Fathers: M = 6.17 | |
| Acceptance | “I’m sure when I see him active and healthy and himself you know that would help me a lot that I didn’t delay (treatment)…if we delayed it, he would probably not be here.” (Mother of a 13-year-old, germ cell carcinoma) “I agree with him…if it’s God’s will, I guess…He can always, I guess adopt.” (Father of a 20-year-old, acute lymphoid leukemia) “Probably wish I had done it if I can’t have kids but what are you gonna do? It’s over with.” (16-year-old, acute lymphoblastic leukemia) | Overall: 60% Adolescents: 50% Mothers: 64%, Fathers: 67% | ||
| Satisfaction | “Completely comfortable with the decision. Completely good with it…whatever his decision was, that’s his choice.” (Mother of a 12-year-old, Ewing’s sarcoma) “He would kind of like to help somebody who needs help, somebody who might need adopted, like his friend, and some other people he’s known.” (Father of a 12-year-old, acute myeloid leukemia) “I think I’m very satisfied with it. I think it was the right decision for me. Maybe others would choose something else but for me it was the best decision for me.” (17-year-old, chronic myelocytic leukemia) | Overall: 40% Adolescents: 40% Mothers: 36%, Fathers: 44% | ||
| Attempter group | ||||
| Satisfaction | “It was 100% good…I was happy that he (banked) and I am very happy the topic came up.” (Mother of an 18-year-old, CNS tumor) “If he’s like alright and he finds the girl…and they start their life together then…it all works out and it would be like again no brainer good” (Father of a 16-year-old, rhabdomyosarcoma) “I think my family might appreciate it when I’m older if I actually am not able to have kids and I think that they might be thankful that I did it because then I’ll actually be able to have my own biological child.” (17-year-old, nodular sclerosing Hodgkin’s disease) | Overall: 93% Adolescents: 96% Mothers: 91%, Fathers: 92% | BSDQ Means: Adolescent: M = 5.76 Mothers: M = 6.13 Fathers: M = 6.44 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theroux, C.I.; Hill, K.N.; Olsavsky, A.L.; Klosky, J.L.; Yeager, N.D.; Audino, A.; O’Brien, S.H.; Quinn, G.P.; Gerhardt, C.A.; Nahata, L. Satisfaction with Fertility Preservation Decisions among Adolescent Males with Cancer: A Mixed Methods Study. Cancers 2021, 13, 3559. https://doi.org/10.3390/cancers13143559
Theroux CI, Hill KN, Olsavsky AL, Klosky JL, Yeager ND, Audino A, O’Brien SH, Quinn GP, Gerhardt CA, Nahata L. Satisfaction with Fertility Preservation Decisions among Adolescent Males with Cancer: A Mixed Methods Study. Cancers. 2021; 13(14):3559. https://doi.org/10.3390/cancers13143559
Chicago/Turabian StyleTheroux, Charleen I., Kylie N. Hill, Anna L. Olsavsky, James L. Klosky, Nicholas D. Yeager, Anthony Audino, Sarah H. O’Brien, Gwendolyn P. Quinn, Cynthia A. Gerhardt, and Leena Nahata. 2021. "Satisfaction with Fertility Preservation Decisions among Adolescent Males with Cancer: A Mixed Methods Study" Cancers 13, no. 14: 3559. https://doi.org/10.3390/cancers13143559