
A Scoping Review on Gaps in the Diagnostic Criteria for Proliferative Verrucous Leukoplakia: A Conceptual Proposal and Diagnostic Evidence-Based Criteria




Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection Process
2.5. Data Extraction
2.6. Critical Analysis and Evidence Synthesis
3. Results
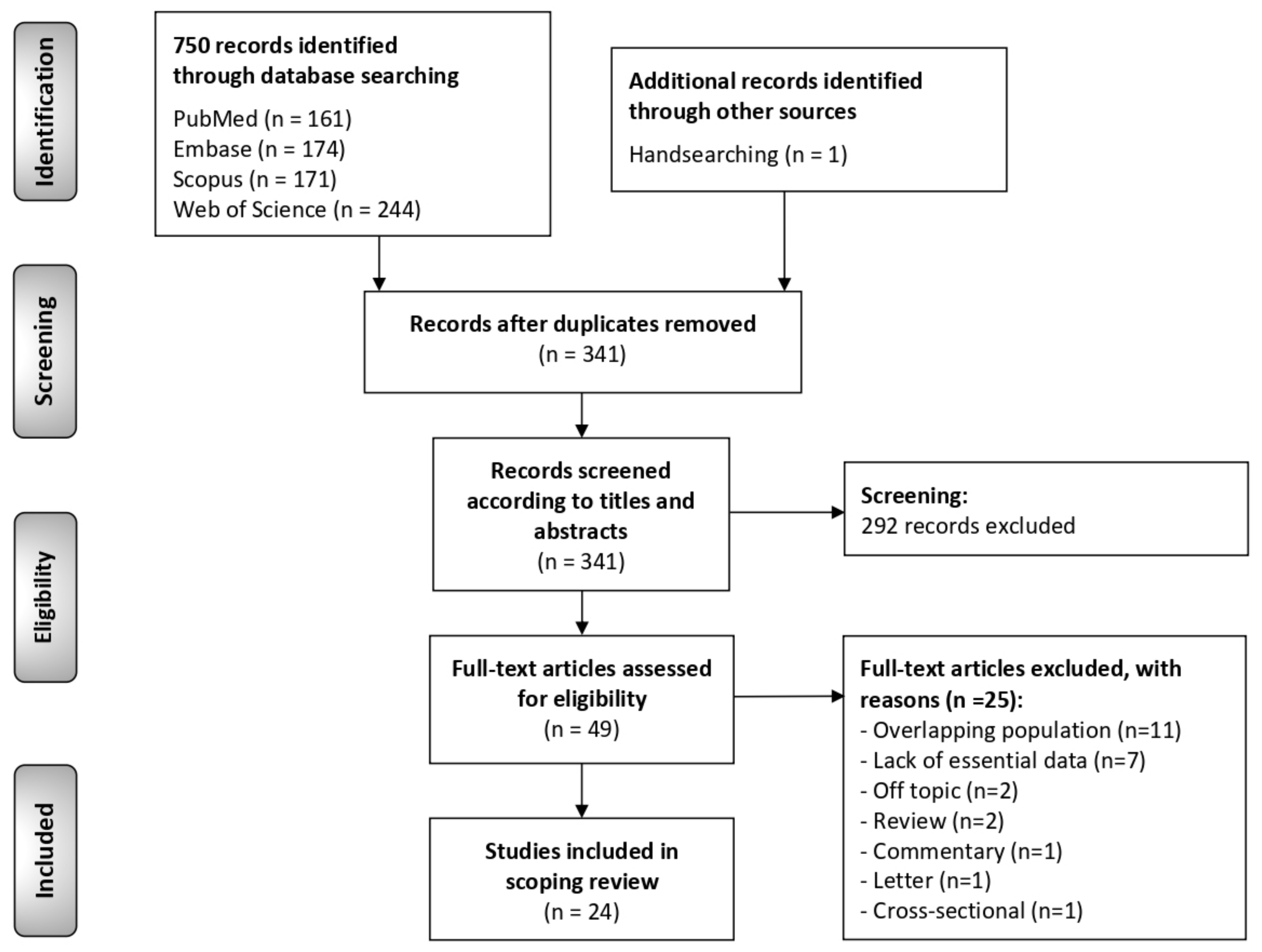
3.1. Results of the Literature Search
3.2. Study Characteristics
3.3. Critical Analysis and Evidence Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; González-Moles, M.Á.; Kerr, A.R.; Lodi, G.; Mello, F.W.; Monteiro, L.; Ogden, G.R.; et al. Oral potentially malignant disorders: A consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. 2020, in press. [Google Scholar] [CrossRef]
- Cabay, R.J.; Morton, T.H.; Epstein, J.B. Proliferative verrucous leukoplakia and its progression to oral carcinoma: A review of the literature. J. Oral Pathol. Med. 2007, 36, 255–261. [Google Scholar] [CrossRef]
- Iocca, O.; Sollecito, T.P.; Alawi, F.; Weinstein, G.S.; Newman, J.G.; De Virgilio, A.; Di Maio, P.; Spriano, G.; Pardiñas López, S.; Shanti, R.M. Potentially malignant disorders of the oral cavity and oral dysplasia: A systematic review and meta-analysis of malignant transformation rate by subtype. Head Neck 2019, 42, 539–555. [Google Scholar] [CrossRef] [PubMed]
- Bagan, J.; Murillo-Cortes, J.; Poveda-Roda, R.; Leopoldo-Rodado, M.; Bagan, L. Second primary tumors in proliferative verrucous leukoplakia: A series of 33 cases. Clin. Oral Investig. 2020, 24, 1963–1969. [Google Scholar] [CrossRef]
- Ramos-García, P.; González-Moles, M.Á.; Mello, F.W.; Bagan, J.V.; Warnakulasuriya, S. Malignant transformation of oral proliferative verrucous leukoplakia: A systematic review and meta-analysis. Oral Dis. 2021, in press. [Google Scholar] [CrossRef]
- Mehrotra, D.; Goel, M.; Kumar, S.; Pandey, R.; Ram, H. Oral verrucous lesions: Controversies in diagnosis and management. J. Oral Biol. Craniofacial Res. 2012, 2, 163–169. [Google Scholar] [CrossRef] [Green Version]
- Zakrzewska, J.M.; Lopes, V.; Speight, P.; Hopper, C. Proliferative verrucous leukoplakia: A report of ten cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 82, 396–401. [Google Scholar] [PubMed]
- Thennavan, A.; Byatnal, A.; Solomon, M.; Radhakrishnan, R. The role of Ki-67, p16, CD34, Bcl-2, cyclooxygenase-2 in the pathogenesis of proliferative verrucous leukoplakia. Indian J. Cancer 2015, 52, 498–502. [Google Scholar]
- Kahn, M.A.; Dockter, M.E.; Hermann-Petrin, J.M. Proliferative verrucous leukoplakia. Four cases with flow cytometric analysis. Oral Surg. Oral Med. Oral Pathol. 1994, 78, 469–475. [Google Scholar] [CrossRef]
- Hansen, L.S.; Olson, J.A.; Silverman, S. Proliferative verrucous leukoplakia. A long-term study of thirty patients. Oral Surg. Oral Med. Oral Pathol. 1985, 60, 285–298. [Google Scholar] [CrossRef]
- Cerero-Lapiedra, R.; Baladé-Martínez, D.; Moreno-López, L.-A.; Esparza-Gómez, G.; Bagán, J.V. Proliferative verrucous leukoplakia: A proposal for diagnostic criteria. Med. Oral Patol. Oral Cir. Bucal 2010, 15, e839–e845. [Google Scholar] [CrossRef] [Green Version]
- Carrard, V.C.; Brouns, E.R.E.A.; van der Waal, I. Proliferative verrucous leukoplakia; a critical appraisal of the diagnostic criteria. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e411–e413. [Google Scholar] [CrossRef]
- Villa, A.; Menon, R.; Kerr, A.; De Abreu Alves, F.; Guollo, A.; Ojeda, D.; Woo, S. Proliferative leukoplakia: Proposed new clinical diagnostic criteria. Oral Dis. 2018, 24, 749–760. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Sucharew, H.; Macaluso, M. Progress Notes: Methods for Research Evidence Synthesis: The Scoping Review Approach. J. Hosp. Med. 2019, 14, 416–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Chichester, UK, 2008; ISBN 9780470712184. [Google Scholar]
- Ghazali, N.; Bakri, M.M.; Zain, R.B. Aggressive, multifocal oral verrucous leukoplakia: Proliferative verrucous leukoplakia or not? J. Oral Pathol. Med. 2003, 32, 383–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campisi, G.; Giovannelli, L.; Ammatuna, P.; Capra, G.; Colella, G.; Di Liberto, C.; Gandolfo, S.; Pentenero, M.; Carrozzo, M.; Serpico, R.; et al. Proliferative verrucous vs. conventional leukoplakia: No significantly increased risk of HPV infection. Oral Oncol. 2004, 40, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Morton, T.H.; Cabay, R.J.; Epstein, J.B. Proliferative verrucous leukoplakia and its progression to oral carcinoma: Report of three cases. J. Oral Pathol. Med. 2007, 36, 315–318. [Google Scholar] [CrossRef]
- Klanrit, P.; Sperandio, M.; Brown, A.L.; Shirlaw, P.J.; Challacombe, S.J.; Morgan, P.R.; Odell, E.W. DNA ploidy in proliferative verrucous leukoplakia. Oral Oncol. 2007, 43, 310–316. [Google Scholar] [CrossRef]
- Ottavioli, A.; Campana, F.; Catherine, J.-H.; Massereau, E.; Del Grande, J.; Ordioni, U. Proliferative verrucous leukoplakia: Three cases and literature review. Ann. Dermatol. Venereol. 2016, 143, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Flores, I.L.; Santos-Silva, A.R.; Della Coletta, R.; Leme, A.F.P.; Lopes, M.A. Low expression of angiotensinogen and dipeptidyl peptidase 1 in saliva of patients with proliferative verrucous leukoplakia. World J. Clin. Cases 2016, 4, 356. [Google Scholar] [CrossRef]
- Borgna, S.C.; Clarke, P.T.; Schache, A.G.; Lowe, D.; Ho, M.W.; McCarthy, C.E.; Adair, S.; Field, E.A.; Field, J.K.; Holt, D.; et al. Management of proliferative verrucous leukoplakia: Justification for a conservative approach. Head Neck 2017, 39, 1997–2003. [Google Scholar] [CrossRef]
- Thomson, P.J.; Goodson, M.L.; Smith, D.R. Potentially malignant disorders revisited-The lichenoid lesion/proliferative verrucous leukoplakia conundrum. J. Oral Pathol. Med. 2018, 47, 557–565. [Google Scholar] [CrossRef]
- Akrish, S.; Ben-Izhak, O.; Sabo, E.; Rachmiel, A. Oral squamous cell carcinoma associated with proliferative verrucous leukoplakia compared with conventional squamous cell carcinoma—A clinical, histologic and immunohistochemical study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 318–325. [Google Scholar] [CrossRef]
- García-Chías, B.; Casado-De La Cruz, L.; Esparza-Gómez, G.-C.; Cerero-Lapiedra, R. Diagnostic criteria in proliferative verrucous leukoplakia: Evaluation. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e335–e339. [Google Scholar] [CrossRef] [PubMed]
- Owosho, A.; Bilodeau, E.A.; Summersgill, K.F. Seven Cases of Proliferative Verrucous Leukoplakia: The Need for a High Clinical Suspicion Among Dental Practitioners. J. Mich. Dent. Assoc. 2015, 97, 48–51, 95. [Google Scholar] [PubMed]
- Garcia-Pola, M.-J.; Llorente-Pendás, S.; González-Garcia, M.; García-Martín, J.-M. The development of proliferative verrucous leukoplakia in oral lichen planus. A preliminary study. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e328–e334. [Google Scholar] [CrossRef] [PubMed]
- Li, C.-C.; Almazrooa, S.; Carvo, I.; Salcines, A.; Woo, S.-B. Architectural Alterations in Oral Epithelial Dysplasia are Similar in Unifocal and Proliferative Leukoplakia. Head Neck Pathol. 2021, 15, 443–460. [Google Scholar] [CrossRef] [PubMed]
- McParland, H.; Warnakulasuriya, S. Lichenoid morphology could be an early feature of oral proliferative verrucous leukoplakia. J. Oral Pathol. Med. 2021, 50, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Upadhyaya, J.D.; Fitzpatrick, S.G.; Islam, M.N.; Bhattacharyya, I.; Cohen, D.M. A Retrospective 20-Year Analysis of Proliferative Verrucous Leukoplakia and Its Progression to Malignancy and Association with High-risk Human Papillomavirus. Head Neck Pathol. 2018, 12, 500–510. [Google Scholar] [CrossRef]
- Koh, J.; Kurago, Z.B. Expanded Expression of Toll-Like Receptor 2 in Proliferative Verrucous Leukoplakia. Head Neck Pathol. 2019, 13, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Favia, G.; Capodiferro, S.; Limongelli, L.; Tempesta, A.; Maiorano, E. Malignant transformation of oral proliferative verrucous leukoplakia: A series of 48 patients with suggestions for management. Int. J. Oral Maxillofac. Surg. 2021, 50, 14–20. [Google Scholar] [CrossRef]
- Proaño-Haro, A.; Bagan, L.; Bagan, J.V. Recurrences following treatment of proliferative verrucous leukoplakia: A systematic review and meta-analysis. J. Oral Pathol. Med. 2021, in press. [Google Scholar] [CrossRef]
- Thompson, L.D.R.; Fitzpatrick, S.G.; Müller, S.; Eisenberg, E.; Upadhyaya, J.D.; Lingen, M.W.; Vigneswaran, N.; Woo, S.-B.; Bhattacharyya, I.; Bilodeau, E.A.; et al. Proliferative Verrucous Leukoplakia: An Expert Consensus Guideline for Standardized Assessment and Reporting. Head Neck Pathol. 2021, 15, 572–587. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| CRITERIA/Conceptual Proposal | Definitions or Proposal for PVL Diagnostic Criteria |
|---|---|
| Hansen et al. 1985 [10] | “…specific form of leukoplakia. It began as a simple hyperkeratosis but tended to extend and become multifocal over varying periods of time. The lesions were slow-growing, persistent, irreversible, and frequently developed erythematous components. Some areas later became exophytic and wart-like and transformed into lesions that were clinically and microscopically identical to verrucous carcinoma and squamous cell carcinoma. In addition, they were resistant to every kind of therapy.” |
| Cerero-Lapiedra et al. 2010 [11] | Major Criteria (MC):
|
| Carrard et al. 2013 [12] |
|
| Villa et al. 2018 [13] |
|
| Proposal by Gonzalez-Moles et al. 2021 [5] derived from the evidence obtained in this scoping review | PVL is an oral potentially malignant disorder that presents in the form of multifocal white plaques, which have expanded throughout its evolution, persistent and resistant to treatment, which is diagnosed in people in the second half of life, although it probably begins in earlier stages, and which has a very high risk of developing into oral cancer. |
| Question 1 | Is the clinical course of the disease (persistent or recurrent, periodicity of recurrences) determining in the PVL diagnosis? |
| Question 2 | To what extent is the age of the lesion decisive for the diagnosis? Do the studies provide information on the age of the lesions? (follow-up time and/or months of evolution) |
| Question 3 | What should be the clinical appearance of the lesions to make a diagnosis of proliferative verrucous leukoplakia? Were the clinical descriptions made by the authors of the lesions included in their incorporated cohorts? |
| Question 4 | Is it necessary for the affection of gingiva and/or palate to make the diagnosis of proliferative verrucous leukoplakia? Were the anatomical affectations per patient reported from the included cohorts? |
| Question 5 | Is it necessary to demonstrate malignant transformation to make the diagnosis of proliferative verrucous leukoplakia? Were the malignant transformation proportions reported in the included cohorts? |
| Question 6 | Is resistance to treatment necessary to make the diagnosis of proliferative verrucous leukoplakia? |
| Question 7 | To what extent is sex required to make the diagnosis of proliferative verrucous leukoplakia? Was the number of females and males reported in the included cohorts? |
| Question 8 | To what extent is age required to make the diagnosis of proliferative verrucous leukoplakia? Was the age of patients reported in the included cohorts? |
| Question 9 | To what extent is tobacco use or its absence necessary to make the diagnosis of proliferative verrucous leukoplakia? Was number of smokers and non-smokers reported in the included cohorts? |
| Question 10 | Is the histological study necessary for the diagnosis of proliferative verrucous leukoplakia? What should be the histological substrate required to make the diagnosis of proliferative verrucous leukoplakia? Were the histological descriptions reported by the authors of the lesions analyzed incorporated in their cohorts? |
| Author (Year) | Country | Diagnostic Criteria | Study Design (Recruitment Period) | Sample (n); Sex; Age Distribution (y) Mean ± SD (Range) | Anatomical Sites per Patients (n, Analysis Units = Patients, Not Lesions) | Malignant Transformation (n, %) | Malignant Transformation (High: >40%; Intermediate: 20–40%; Low: <20%) | Smoking | Clinical Diagnosis | Histological Diagnosis | Follow Up (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| McParland and Warnakulasuriya (2020) [34] | UK | Hansen et al. (1985) [10] | Retrospective cohort (2000–2016) | Sample size = 51 M = 25 (49.1%) F = 26 (50.9%) Mean age: 52.3 ± 8.65 | NR | MT = 11 (21.57%) No MT = 40 | Intermediate | Yes = 10 Former = 12 Never = 29 (56.86%) | NR | ED = 12 | ≤48 |
| Li et al. (2021) [33] | USA | Own | Retrospective cohort (NR) | Sample size = 4 M = 2 (50%) F = 2 (50%) Mean age: 58 ± 21.74 | Gingiva = 3 Bm = 4 Tongue = 4 Palate = 2 FOM = 1 Lip = 1 Other = 1 | MT = 3 (75%) (SCC = 3 patients, 7 tumors) No MT = 4 | High | NR | NR | HK = 4 Papillomatosis = 2 Corrugated = 2 | Mean = 114 |
| Favia et al. (2021) [37] | Italy | Hansen et al. (1985) [10] | Retrospective cohort (1989–2008) | Sample size = 75 Sex = NR Age = NR | NR | MT = 48 (64%) (VC = 33 patients, 57 tumors; SCC = 15 patients; 73 tumors) No MT = 27 | High | Yes = 11 No = 64 (84.33%) | NR | NR | Mean = 62.45 Range = 18–240 |
| Bagan et al. (2020) [4] | Spain | Villa et al. (2018) [13] | Retrospective cohort (1996–2018) | Sample size = 81 M = 29 (35.8%) F = 52 (64.2%) Mean age: 62.6 ± 12.3 | NR | MT = 33 (40.74%) (SCC = 33 patients, 105 tumors) No MT = 48 | High | NR | NR | NR | Mean = 65.61 ± 77.45 Range: 12–256.8 |
| Koh and Kurago (2019) [36] | USA | Own | Retrospective cohort (NR) | Sample size = 10 M = 5 (50%) F = 5 (50%) Mean age: 60.7 ± 11.94 | Gingiva = 6 Bm = 6 Tongue = 4 Palate = 2 FOM = 2 Lip = 1 Other = 0 | MT = 5 (50%) (VC = 2, SCC = 2, SCC+VC = 1; 6 tumors) No MT = 5 | High | Yes = 6 No = 2 (20%) Missing = 2 | NR | VH = 10 ED = 8 | Mean = 39.6 Range: 12–84 |
| Upadhyaya et al. (2018) [35] | USA | Hansen et al. (1985) [10] | Retrospective cohort (1994–2016) | Sample size = 20 M = 6 (30%) F = 14 (70%) Mean age: 62.7 (range: 34–87) | NR | MT = 9 (45%) (VC = 6, PSCC = 1, SCC = 2) No MT = 11 | High | Yes = 12 (60%) No = 5 (25%) NA = 3 | NR | Grade 2 = 12 Grade 4 = 3 Grade 5 = 1 | Mean = 91.8 |
| Villa et al. (2018) [13] | USA and Brazil | Villa et al. (2018) [13] | Retrospective cohort (1996–2016) | Sample size = 42 M = 7 (16.7%) F = 35 (83.3%) Mean age: 67.23 ± 11.95 | NR | MT = 30 (71.43%) (SCC = 25, VC = 5) No MT = 12 | High | Yes = 5 Former = 12 Never = 24 (57.14%) | NR | HK = 22 ED = 17 VH = 5 | Mean = 47.06 ± 47.33 |
| Thomson et al. (2018) [28] | UK | NR | Retrospective cohort (1996–2014) | Sample size = 80 M = 41 (51.25%) F = 39 (48.75%) Mean age: 62.3 (range: 25–94) | Gingiva = 11 Bm = 15 Tongue = 19 Palate = 5 FOM = 16 Lip = 11 Other = 3 | MT = 2 (2.5%) No MT = 78 | Low | NR | White plaque = 80 Progressive = NR Multifocal = NR Slow growth = NR Erithematous = 2 Verrucous-like = NR Fissured = NR Ulcerated = NR | ED = 68 | Mean = 87.6 |
| Borgna et al. (2017) [27] | UK | Hansen et al. (1985) [10] | Retrospective cohort (1990–2015) | Sample size = 48 M = 24 (50%) F = 24 (50%) Mean age: 70 ± 13 | NR | MT = 23 (47.92%) (VC = 10, SCC = 9, papillary SCC = 4) No MT = 25 | High | Yes = 33 No = 15 (31.25%) | NR | Grade 2 = 2 Grade 3 = 14 Grade 4 = 14 Grade 5 = 9 Grade 6 = 5 Grade 8 = 1 Grade 9 = 3 | Mean = 51.6 ± 44.4 |
| Flores et al. (2016) [26] | Brazil. | Own | Retrospective cohort (NA) | Sample size = 15 M = 0 (0%) F = 15 (100%) Mean age: 68.13 ± 9.82 | Gingiva = 9 Bm = 15 Tongue = 11 Palate = 5 FOM = 7 Lip = 3 Other = 1 | MT = 4 (26.67%) (VC = 1, SCC = 5;6 tumors) No MT = 11 | Intermediate | Yes = 0 (0%) No = 15 (100%) | NR | HK = 4 ED = 13 Acanthosis = 3 Atrophy = 1 | Mean = 65.6 ± 63.15 |
| García-Pola et al. (2016) [32] | Spain | Own | Prospective cohort (1984–2015) | Sample size = 14 M = 3 (21.4%) F = 11 (78.6%) Mean age: 56.4 (range: 35–69) | NR | MT = 4 (28.57%) (VC = 1, SCC = 3;12 tumors, 2 VCs, 10 SCCs) No MT = 10 | Intermediate | Former = 3 No = 11 (78.57%) | NR | HK = 14 Papillomatosis = 10 VH = 9 ED = 1 | Mean = 174 |
| Ottavioli et al. (2016) [25] | France | Carrard et al. (2013) [12] | Retrospective cohort (NA) | Sample size = 3 M = 0 (0%) F = 3 (100%) Mean age: 80.7 ± 4.9 | NR | MT = 2 (66.67%) (VC = 1, SCC = 1) No MT = 1 | High | Yes = 0 (0%) No = 3 (100%) | NR | HK = 3 Papillomatosis = 3 Acanthosis = 1 | Mean = 24 ± 12 |
| Akrish et al. (2015) [29] | Israel | Own | Retrospective cohort (1990–2012) | Sample size = 11 M = 6 (55.5%) F = 5 (45.5%) Mean age: 64 | NR | MT = 11 patients (38 SCCs) No MT = NR | NA | Yes = 1 No = 10 (90.91%) | NR | NR | >70 |
| Thennavan et al. (2015) [8] | India | Own | Retrospective cohort (NR) | Sample size = 7 M = 1 (14.3%) F = 6 (85.7%) Mean age: 63.7 (range: 54–76) | Gingiva = 6 Bm = 7 Tongue = 2 Palate = 1 FOM = 0 Lip = 1 Other = 1 | MT = 1 (14.29%) (SCC = 1; 1 tumor) No MT = 6 | Low | Yes = 3 No = 4 (57.14%) | White plaque = 7 Progressive = 7 Multifocal = 7 Slow growth = NR Erithematous = 1 Verrucous-like = 2 Fissured = NR Ulcerated = 1 | VH = 7 ED = 6 | 14 |
| Owosho et al. (2015) [31] | USA | Cerero-Lapiedra et al. (2010) [11] | Retrospective cohort (2007–2013) | Sample size = 7 M = 4 (57.1%) F = 3 (42.9%): Mean age = 63.7 (range: 47–82) | Gingiva = 6 Bm = 6 Tongue = 2 Palate = 0 FOM = 0 Lip = 0 Other = 0 | MT: 2 (28.57%) (1 VC, 1 SCC; 4 tumors, 1 VC, 2 SCCs, 1 hybrid VC/SCC) No MT: 5 | Intermediate | Yes = 0 No = 7 (100%) | White plaque = 7 Progressive = NR Multifocal = 5 Slow growth = NR Erithematous = 2 Verrucous-like = 2 Fissured = NR Ulcerated = NR | HK = 6 Lymphocytic infiltrate = 2 VH = 2 ED = 7 | Mean = 56.4 |
| García-Chías et al. (2014) [30] | Spain | Cerero-Lapiedra et al. (2010) [11] | Retrospective cohort (1984–2011) | Sample size = 40 M = 15 (37.5%) F = 25 (62.5%) Mean age: 62.3 | NR | MT = 7 (17.5%) (3 VC, 4 OSCC) No MT = 33 | Low | Yes = 12 No = 28 (70%) | White plaque = 40 Progressive = 26 Multifocal = 38 Slow growth = NR Erithematous = 9 Verrucous-like = 14 Fissured = NR Ulcerated = NR | HK = 40 ED = 20 | Mean = 44 |
| Mehrotra et al. (2012) [6] | India | NR | Retrospective cohort (2007–2009) | Sample size = 3 M = 3 (100%) F = 0 (0%) Age: 40.3 ± 7.6 | NR | MT = 0 (0%) No MT = 3 | Low | NR | NR | NR | ≤48 |
| Morton et al. (2007) [23] | USA | NR | Retrospective cohort (NR) | Sample size = 3 M = 1 (33.33%) F = 2 (66.67%) Age: 80 ± 8.19 | Gingiva = 2 Bm = 1 Tongue = 0 Palate = 1 FOM = 0 Lip = 1 Other = 1 | MT = 3 (100%) (VC = 1, SCC = 2) No MT = 0 | High | Yes = 1 No = 2 (66.67%) | White plaque = 3 Progressive = NR Multifocal = 1 Slow growth = NR Erithematous = 1 Verrucous-like = 1 Fissured = NR Ulcerated = NR | HK = 2 Lymphocytic infiltrate = 1 VH = 2 | NR |
| Klanrit et al. (2007) [24] | UK | Own | Retrospective cohort (1990–1999) | Sample size = 6 M = 1 (16.67%) F = 5 (83.33%) Age: 65.83 ± 10.11 | Gingiva = 6 Bm = 2 Tongue = 2 Palate = 3 FOM = 0 Lip = 1 Other = 0 | MT = 6 patients (13 tumors VC = 2, cuniculatum = 3, SCC = 8) No MT = NR | NA | Yes = 1 Former = 1 No = 3 (50%) Missing = 1 | NR | HK = 6 EP = 6 VH = 1 | Mean = 116 |
| Campisi et al. (2004) [22] | Italy | Own | Retrospective cohort (NR) | Sample size = 58 M = 22 (37.93%) F = 36 (62.07%) Age: 66.5 ± 12.92 | NR | MT = 25 (43.10%) (VC = 3, SCC = 22) No MT = 33 | High | Yes = 8 Former = 9 No = 41 (70.69%) | NR | NR | NR |
| Ghazali et al. (2003) [21] | Malaysia | Hansen et al. (1985) [10] | Retrospective cohort (NR) | Sample size = 9 M = 2 (22.22%) F = 7 (77.78%) Mean age: 61.67 ± 15.16 | Gingiva = 6 Bm = 5 Tongue = 3 Palate = 1 FOM = 1 Lip = 1 Other = 0 | MT = 7 (77.78%) (VC = 1, SCC = 3, VC+SCC = 3; 13 tumors, 5 VCs, 8SCCs) No MT = 2 | High | Yes = 4 No = 5 (55.56%) | NR | VH = 3 ED = 7 | Mean = 56.4 |
| Zakrzewska et al. (1996) [7] | UK | Hansen et al. (1985) [10] | Retrospective cohort (NA) | Sample size = 10 M = 5 (50%) F = 5 (50%) Mean age (63.5, range: 42–81) | NR | MT = 10 (100%) No MT = 0 | High | Yes = 7 No = 3 (30%) | NR | Grade 2 = 2 Grade 3 = 3 Grade 4 = 1 Grade 5 = 4 | Mean = 79.2 |
| Kahn et al. (1994) [9] | USA | NR | Retrospective cohort (1988–1990) | Sample (n = 4) M = 2 (50%) F = 2 (50%) Mean age = 68.75 (range: 51–75) | Gingiva = 3 Bm = 2 Tongue = 0 Palate = 0 FOM = 0 Lip = 0 Other = 1 | MT = 3 (75%) No MT = 1 | High | Yes = 2 No = 2 (50%) | White plaque = 4 Progressive = NR Multifocal = 3 Slow growth = NR Erithematous = 1 Verrucous-like = 3 Fissured = NR Ulcerated = 0 | VH = 3 ED = 1 | Mean = 48 Range = 24-60 |
| Hansen et al. (1985) [10] | USA | Hansen et al. (1985) [10] | Retrospective cohort (1961–1983) | Sample (n = 30) M = 6 (20%) F = 24 (80%) Mean age = 49 (range: 27–74) | NR | MT = 27 (90%) (VC = 4, papillary = 18, SCC = 5) No MT = 3 | High | Yes = 18 No = 12 (40%) | NR | Grade 3 = 1 Grade 4 = 2 Grade 5 = 1 Grade 6 = 3 Grade 7 = 6 Grade 8 = 12 Grade 9 = 2 Grade 10 = 3 | Mean = 73.2 |
| Research Questions | Hansen et al. [10] | Cerero-Lapiedra et al. [11] | Carrard et al. [12] | Villa et al. [13] | |
|---|---|---|---|---|---|
| Q1 | - Is the clinical course of the disease (persistent or recurrent, periodicity of recurrences) determining in the PVL diagnosis? | Yes | No | No | No |
| Q2 | - To what extent is the age of the lesion decisive for the PVL diagnosis? | No | Yes | Yes | No |
| Q3 | - What should be the clinical appearance of the lesions to make a diagnosis of PVL? | Yes | Yes | Yes | Yes |
| Clinical descriptions of the PVL lesions made by the authors: White plaque | Yes | Yes | Yes | Yes | |
| Multifocality | Yes | Yes | Yes | Yes | |
| Progressive/expansive nature | Yes | Yes | Yes | Yes | |
| Verrucous-like | No | No | Yes | No | |
| Erythematous areas | Yes | No | No | Yes | |
| Ulcerated areas | No | No | No | Yes | |
| Fissured appearance | No | No | No | Yes | |
| Smooth appearance | No | Yes | No | No | |
| Q4 | - Is it necessary the affectation of gingiva and/or palate to make the diagnosis of PVL? | No | Yes | Yes | No |
| Intraoral sites affected by PVL lesions: Buccal Mucosa | No | No | No | No | |
| Gingiva | No | Yes | Yes | No | |
| Tongue | No | No | No | No | |
| Palate | No | Yes | Yes | No | |
| Q5 | - Is it necessary to demonstrate malignant transformation to make the diagnosis of PVL? | Yes | Yes | Yes | Yes |
| - Malignant transformation reported | Yes | Yes | Yes | Yes | |
| Q6 | - Is resistance to treatment necessary to make the diagnosis of PVL? | Yes | No | Yes | No |
| Q7 | - To what extent is sex required to make the diagnosis of PVL? | No | Yes | No | No |
| Description per sex: Females | No | Yes | No | No | |
| Q8 | - To what extent is age required to make the diagnosis of PVL? | No | No | No | No |
| Description of age reported | No | No | No | No | |
| Q9 | - To what extent is tobacco use or its absence necessary to make the diagnosis of PVL? | No | Yes | No | No |
| Description for smoking habit: Non-smokers | No | Yes | No | No | |
| Q10 | - Is the histological study necessary for the diagnosis of PVL? | Yes | Yes | Yes | Yes |
| Description of alterations in histology of PVL: Hyperkeratosis | Yes | Yes | No | Yes | |
| Atrophy | No | No | No | Yes | |
| Acanthosis | No | No | No | Yes | |
| Lymphocytic infiltrate in the lamina propria | No | No | No | Yes | |
| Verrucous hyperplasia | Yes | Yes | No | Yes | |
| Epithelial dysplasia | Yes | No | No | Yes | |
| Verrucous carcinoma | Yes | Yes | No | No | |
| Papillary carcinoma | Yes | No | No | No | |
| Squamous cell carcinoma | Yes | Yes | No | Yes | |
| Research Questions | PVL Diagnostic Criteria Proposed Including Each Research Question * | Primary-Level Studies Included in This Scoping Review | |||
|---|---|---|---|---|---|
| Studies (n, %) Considering the Research Question among Their PVL Diagnostic Criteria | Patients (n) with Available Data ** | Positive Cases (%) ** | |||
| Q1 | - Is the clinical course of the disease (persistent or recurrent, periodicity of recurrences) determining in the PVL diagnosis? | Hansen et al. (1985) [10] | 6/24 (25%) (all persistent) | NR | NR |
| Q2 | - To what extent is the age of the lesion decisive for the PVL diagnosis? | Cerero-Lapiedra et al. (2010) [11] Carrard et al. (2013) [12] | 5/24 (20.83%) | NR | NR |
| Q3 | - What should be the clinical appearance of the lesions to make a diagnosis of PVL? | All | NA | NA | NA |
| Clinical descriptions of the PVL lesions made by the authors: White plaque | All | 6/24 (25%) | 141 | 141 (100%) | |
| Multifocality | All | 6/24 (25%) | 81 | 74 (91.36%) | |
| Progressive/expansive nature | All | 3/24 (12.5%) | 51 | 36 (70.59%) | |
| Verrucous-like | Carrard et al. (2013) [12] | 5/24 (20.83%) | 61 | 22 (36.07%) | |
| Erythematous areas | Hansen et al. (1985) [10] Villa et al. (2018) [13] | 6/24 (25%) | 141 | 16 (11.35%) | |
| Ulcerated areas | Villa et al. (2018) [13] | 2/24 (8.33%) | 11 | 1 (9.09%) | |
| Fissured appearance | Villa et al. (2018) [13] | 0/24 (0%) | 0 | 0 (0%) | |
| Smooth appearance | Cerero-Lapiedra et al. (2010) [11] | 0/24 (0%) | 0 | 0 (0%) | |
| Q4 | - Is it necessary the affectation of gingiva and/or palate to make the diagnosis of PVL? | Cerero-Lapiedra et al. (2010) [11] Carrard et al. (2013) [12] | 1/24 (4.17%) | NA | NA |
| Intraoral sites affected by PVL lesions: Buccal Mucosa | None | 10/24 (41.67%) | 145 | 63 (43.45%) | |
| Gingiva | Cerero-Lapiedra et al. (2010) [11] Carrard et al. (2013) [12] | 10/24 (41.67%) | 145 | 58 (40%) | |
| Tongue | None | 10/24 (41.67%) | 145 | 47 (32.41%) | |
| Palate | Cerero-Lapiedra et al. (2010) [11] Carrard et al. (2013) [12] | 10/24 (41.67%) | 145 | 29 (13.79%) | |
| Q5 | - Is it necessary to demonstrate malignant transformation to make the diagnosis of PVL? | All | 0/24 (0%) *** | NA | NA |
| - Malignant transformation reported | All | 24/24 (100%) | 631 | 266 (43.74%) | |
| Q6 | - Is resistance to treatment necessary to make the diagnosis of PVL? | Hansen et al. (1985) [10] Carrard et al. (2013) [12] | 2/24 (8.33%) | 54 | 24 (44.44%) |
| Q7 | - To what extent is sex required to make the diagnosis of PVL? | Cerero-Lapiedra et al. (2010) [11] | 2/24 (8.33%) | NA | NA |
| Description per sex: Females | Cerero-Lapiedra et al. (2010) [11] | 23/24 (95.83%) | 556 | 363 (62.23%) | |
| Q8 | - To what extent is age required to make the diagnosis of PVL? | None | 0/24 (0%) | NA | NA |
| Description of age reported | None | 23/24 (95.83%) | 556 **** | Mean of means = 63.06y | |
| Q9 | - To what extent is tobacco use or its absence necessary to make the diagnosis of PVL? | Cerero-Lapiedra et al. (2010) [11] | 2/24 (8.33%) | NA | NA |
| Description for smoking habit:Non-smokers | Cerero-Lapiedra et al. (2010) [11] | 20/24 (83.33%) | 463 | 285 (61.56%) | |
| Q10 | - Is the histological study necessary for the diagnosis of PVL? | All | 16/24 (66.67%) | NA | NA |
| Description of alterations in histology of PVL: Hyperkeratosis | Hansen et al. (1985) [10] Cerero-Lapiedra et al. (2010) [11] Villa et al. (2018) [13] | 10/24 (41.67%) | 143 | 101 (70.63%) | |
| Atrophy | Villa et al. (2018) [13] | 1/24 (4.17%) | 15 | 1 (6.67%) | |
| Acanthosis | Villa et al. (2018) [13] | 2/24 (8.33%) | 18 | 6 (33.33%) | |
| Lymphocytic infiltrate in the chorion | Villa et al. (2018) [13] | 2/24 (8.33%) | 10 | 3 (30%) | |
| Verrucous hyperplasia | Hansen et al. (1985) [10] Cerero-Lapiedra et al. (2010) [11] Villa et al. (2018) [13] | 7/24 (29.17%) | 87 | 38 (43.68%) | |
| Epithelial dysplasia | Hansen et al. (1985) [10] Villa et al. (2018) [13] | 10/24 (41.67%) | 274 | 159 (58.03%) | |
| Verrucous carcinoma | Hansen et al. (1985) [10] Cerero-Lapiedra et al. (2010) [11] | 16/24 (66.67%) | 384 | 81 (21.09%) | |
| Papillary carcinoma | Hansen et al. (1985) [10] | 3/24 (12.5%) | 98 | 21 (21.43%) | |
| Squamous cell carcinoma | Hansen et al. (1985) [10] Cerero-Lapiedra et al. (2010) [11] Villa et al. (2018) [13] | 18/24 (75%) | 472 | 139 (29.45%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Moles, M.Á.; Ramos-García, P.; Warnakulasuriya, S. A Scoping Review on Gaps in the Diagnostic Criteria for Proliferative Verrucous Leukoplakia: A Conceptual Proposal and Diagnostic Evidence-Based Criteria. Cancers 2021, 13, 3669. https://doi.org/10.3390/cancers13153669
González-Moles MÁ, Ramos-García P, Warnakulasuriya S. A Scoping Review on Gaps in the Diagnostic Criteria for Proliferative Verrucous Leukoplakia: A Conceptual Proposal and Diagnostic Evidence-Based Criteria. Cancers. 2021; 13(15):3669. https://doi.org/10.3390/cancers13153669
Chicago/Turabian StyleGonzález-Moles, Miguel Ángel, Pablo Ramos-García, and Saman Warnakulasuriya. 2021. "A Scoping Review on Gaps in the Diagnostic Criteria for Proliferative Verrucous Leukoplakia: A Conceptual Proposal and Diagnostic Evidence-Based Criteria" Cancers 13, no. 15: 3669. https://doi.org/10.3390/cancers13153669
APA StyleGonzález-Moles, M. Á., Ramos-García, P., & Warnakulasuriya, S. (2021). A Scoping Review on Gaps in the Diagnostic Criteria for Proliferative Verrucous Leukoplakia: A Conceptual Proposal and Diagnostic Evidence-Based Criteria. Cancers, 13(15), 3669. https://doi.org/10.3390/cancers13153669