
Meta-Analysis of Isolated Hepatic Perfusion and Percutaneous Hepatic Perfusion as a Treatment for Uveal Melanoma Liver Metastases



Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
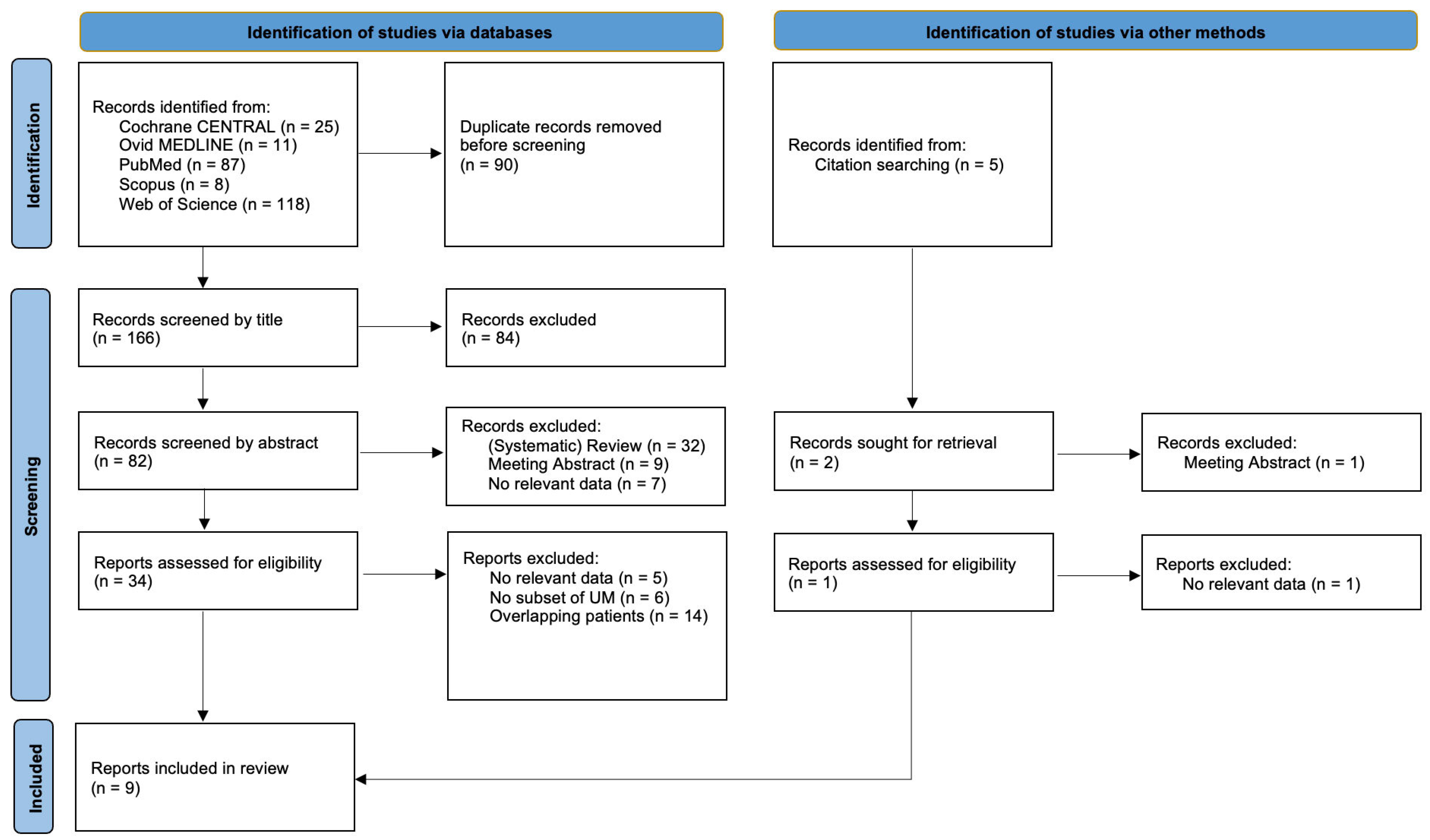
2.1. Database Search Methodology
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Study and Patient Characteristics
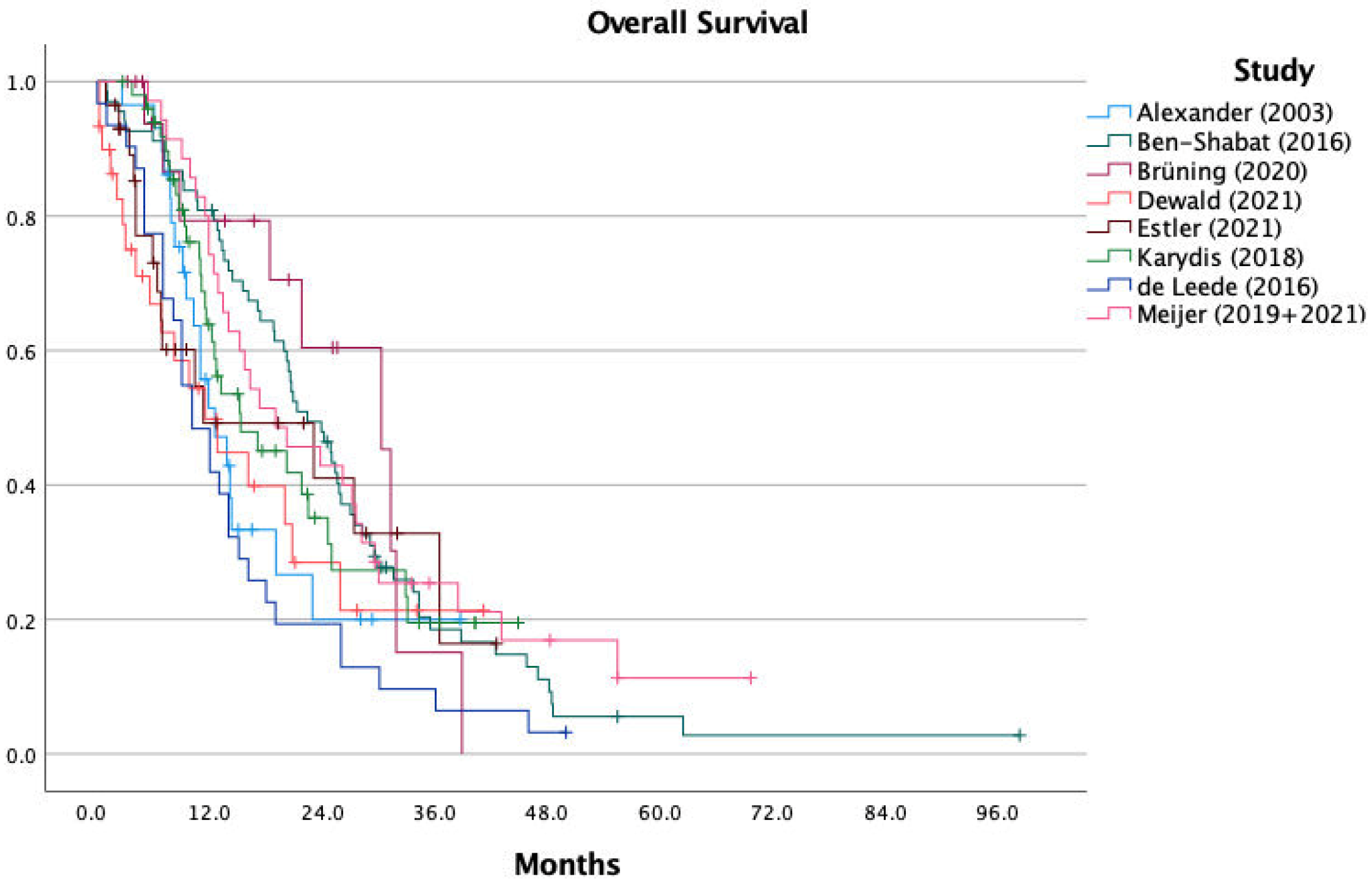
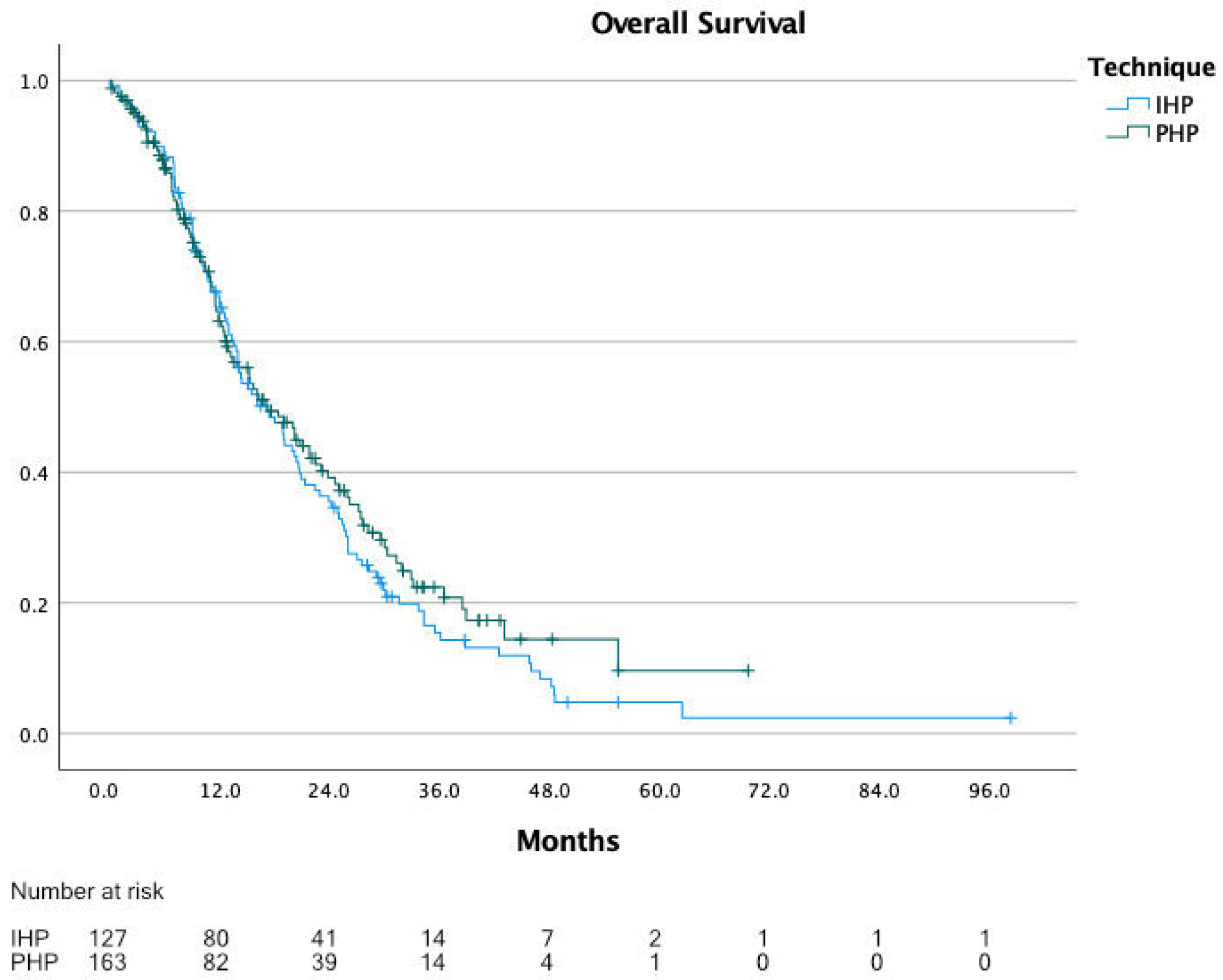
3.2. Overall Survival
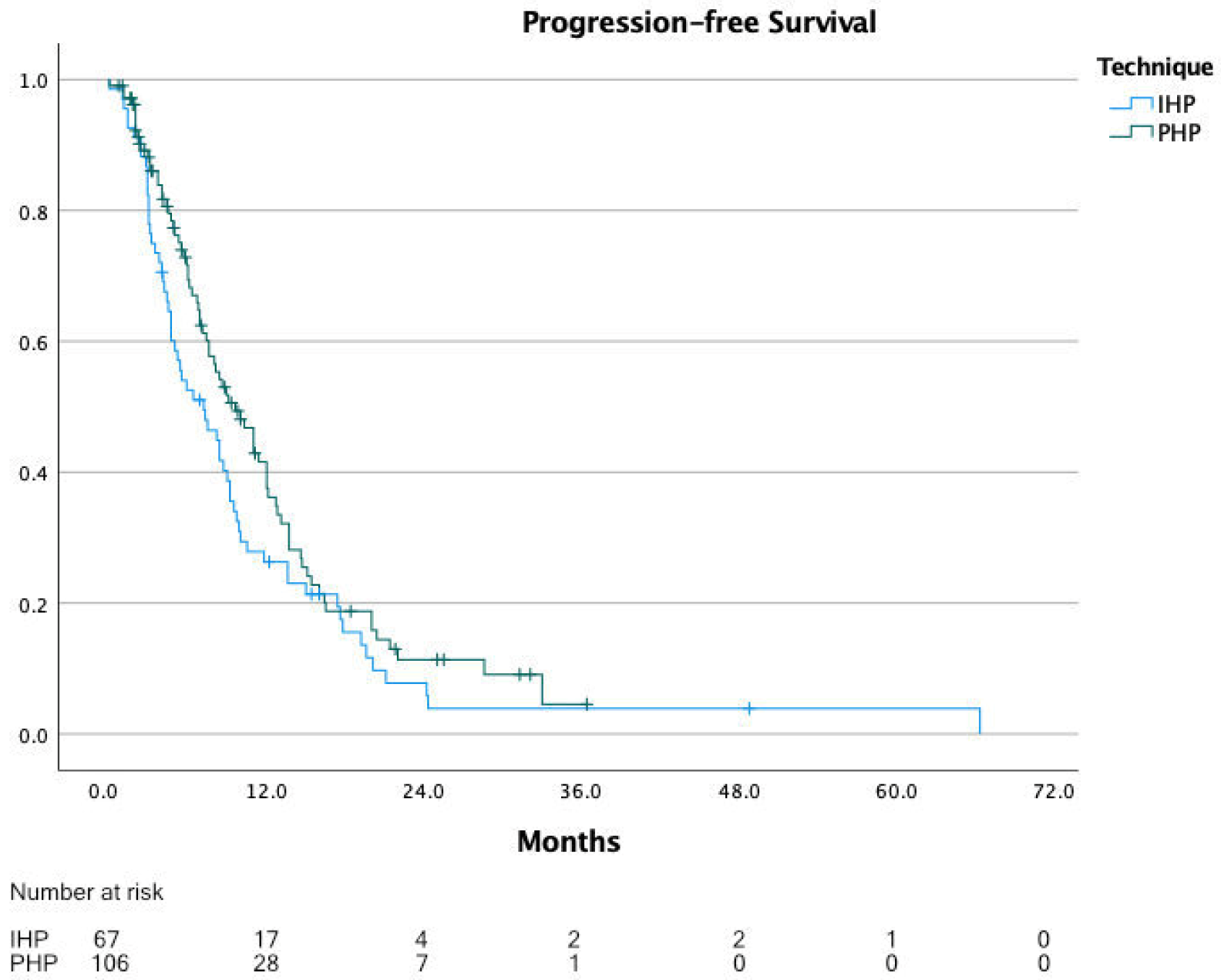
3.3. Progression-Free Survival
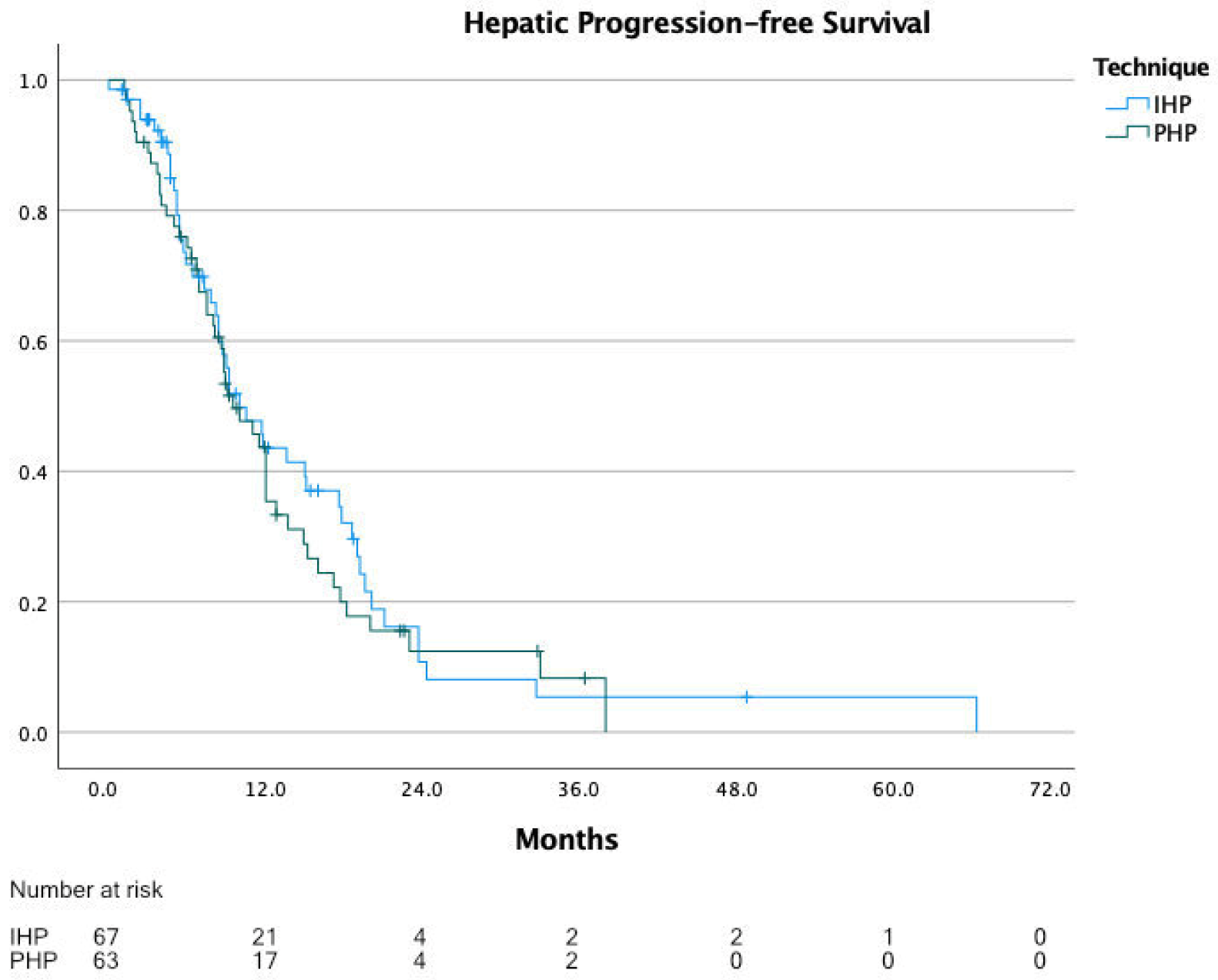
3.4. Hepatic Progression-Free Survival
3.5. Complications and Mortality
3.6. Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jovanovic, P.; Mihajlovic, M.; Djordjevic-Jocic, J.; Vlajkovic, S.; Cekic, S.; Stefanovic, V. Ocular melanoma: An overview of the current status. Int. J. Clin. Exp. Pathol. 2013, 6, 1230–1244. [Google Scholar]
- Amaro, A.; Gangemi, R.; Piaggio, F.; Angelini, G.; Barisione, G.; Ferrini, S.; Pfeffer, U. The biology of uveal melanoma. Cancer Metastasis Rev. 2017, 36, 109–140. [Google Scholar] [CrossRef] [PubMed]
- Vidwans, S.J.; Flaherty, K.T.; Fisher, D.E.; Tenenbaum, J.M.; Travers, M.D.; Shrager, J. A melanoma molecular disease model. PLoS ONE 2011, 6, e18257. [Google Scholar] [CrossRef] [Green Version]
- Jager, M.J.; Shields, C.L.; Cebulla, C.M.; Abdel-Rahman, M.H.; Grossniklaus, H.E.; Stern, M.H.; Carvajal, R.D.; Belfort, R.N.; Jia, R.; Shields, J.A.; et al. Uveal melanoma. Nat. Rev. Dis. Primers 2020, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Shoushtari, A.N.; Carvajal, R.D. Treatment of Uveal Melanoma. Cancer Treat. Res. 2016, 167, 281–293. [Google Scholar] [CrossRef]
- Bronkhorst, I.H.; Jager, M.J. Inflammation in uveal melanoma. Eye 2013, 27, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Isager, P.; Engholm, G.; Overgaard, J.; Storm, H. Uveal and conjunctival malignant melanoma in Denmark 1943–1997: Observed and relative survival of patients followed through 2002. Ophthalmic Epidemiol. 2006, 13, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Kujala, E.; Makitie, T.; Kivela, T. Very long-term prognosis of patients with malignant uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4651–4659. [Google Scholar] [CrossRef] [Green Version]
- Diener-West, M.; Reynolds, S.M.; Agugliaro, D.J.; Caldwell, R.; Cumming, K.; Earle, J.D.; Hawkins, B.S.; Hayman, J.A.; Jaiyesimi, I.; Jampol, L.M.; et al. Development of metastatic disease after enrollment in the COMS trials for treatment of choroidal melanoma: Collaborative Ocular Melanoma Study Group Report No. 26. Arch. Ophthalmol. 2005, 123, 1639–1643. [Google Scholar] [CrossRef] [PubMed]
- Carvajal, R.D.; Schwartz, G.K.; Tezel, T.; Marr, B.; Francis, J.H.; Nathan, P.D. Metastatic disease from uveal melanoma: Treatment options and future prospects. Br. J. Ophthalmol. 2017, 101, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Spagnolo, F.; Caltabiano, G.; Queirolo, P. Uveal melanoma. Cancer Treat. Rev. 2012, 38, 549–553. [Google Scholar] [CrossRef]
- Singh, A.D.; Turell, M.E.; Topham, A.K. Uveal melanoma: Trends in incidence, treatment, and survival. Ophthalmology 2011, 118, 1881–1885. [Google Scholar] [CrossRef]
- Agarwala, S.S.; Eggermont, A.M.; O’Day, S.; Zager, J.S. Metastatic melanoma to the liver: A contemporary and comprehensive review of surgical, systemic, and regional therapeutic options. Cancer 2014, 120, 781–789. [Google Scholar] [CrossRef]
- Khoja, L.; Atenafu, E.G.; Suciu, S.; Leyvraz, S.; Sato, T.; Marshall, E.; Keilholz, U.; Zimmer, L.; Patel, S.P.; Piperno-Neumann, S.; et al. Meta-analysis in metastatic uveal melanoma to determine progression free and overall survival benchmarks: An international rare cancers initiative (IRCI) ocular melanoma study. Ann. Oncol. 2019, 30, 1370–1380. [Google Scholar] [CrossRef]
- Rantala, E.S.; Hernberg, M.; Kivela, T.T. Overall survival after treatment for metastatic uveal melanoma: A systematic review and meta-analysis. Melanoma Res. 2019, 29, 561–568. [Google Scholar] [CrossRef]
- Rodriguez-Vidal, C.; Fernandez-Diaz, D.; Fernandez-Marta, B.; Lago-Baameiro, N.; Pardo, M.; Silva, P.; Paniagua, L.; Blanco-Teijeiro, M.J.; Pineiro, A.; Bande, M. Treatment of Metastatic Uveal Melanoma: Systematic Review. Cancers 2020, 12, 2557. [Google Scholar] [CrossRef]
- Rowcroft, A.; Loveday, B.P.T.; Thomson, B.N.J.; Banting, S.; Knowles, B. Systematic review of liver directed therapy for uveal melanoma hepatic metastases. HPB 2020, 22, 497–505. [Google Scholar] [CrossRef]
- Ausman, R.K. Development of a technic for isolated perfusion of the liver. N. Y. State J. Med. 1961, 61, 3993–3997. [Google Scholar] [PubMed]
- Ben-Shabat, I.; Hansson, C.; Sternby Eilard, M.; Cahlin, C.; Rizell, M.; Lindner, P.; Mattsson, J.; Olofsson Bagge, R. Isolated hepatic perfusion as a treatment for liver metastases of uveal melanoma. J. Vis. Exp. 2015, 52490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravikumar, T.S.; Pizzorno, G.; Bodden, W.; Marsh, J.; Strair, R.; Pollack, J.; Hendler, R.; Hanna, J.; D’Andrea, E. Percutaneous hepatic vein isolation and high-dose hepatic arterial infusion chemotherapy for unresectable liver tumors. J. Clin. Oncol. 1994, 12, 2723–2736. [Google Scholar] [CrossRef] [PubMed]
- De Leede, E.M.; Burgmans, M.C.; Martini, C.H.; Tijl, F.G.; van Erkel, A.R.; Vuyk, J.; Kapiteijn, E.; Verhoef, C.; van de Velde, C.J.; Vahrmeijer, A.L. Percutaneous Hepatic Perfusion (PHP) with Melphalan as a Treatment for Unresectable Metastases Confined to the Liver. J. Vis. Exp. 2016. [Google Scholar] [CrossRef]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021, 156, 787–788. [Google Scholar] [CrossRef]
- PROSPERO. International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/PROSPERO/ (accessed on 21 June 2021).
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Rohatgi, A. WebPlotDigitizer (Version 4.4). 2020. Available online: https://automeris.io/WebPlotDigitizer (accessed on 11 May 2021).
- Drevon, D.; Fursa, S.R.; Malcolm, A.L. Intercoder Reliability and Validity of WebPlotDigitizer in Extracting Graphed Data. Behav. Modif. 2017, 41, 323–339. [Google Scholar] [CrossRef] [PubMed]
- Moeyaert, M.; Maggin, D.; Verkuilen, J. Reliability, Validity, and Usability of Data Extraction Programs for Single-Case Research Designs. Behav. Modif. 2016, 40, 874–900. [Google Scholar] [CrossRef]
- Earle, C.C.; Pham, B.; Wells, G.A. An assessment of methods to combine published survival curves. Med. Decis. Mak. 2000, 20, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Pingpank, J.F.; Libutti, S.K.; Chang, R.; Wood, B.J.; Neeman, Z.; Kam, A.W.; Figg, W.D.; Zhai, S.; Beresneva, T.; Seidel, G.D.; et al. Phase I study of hepatic arterial melphalan infusion and hepatic venous hemofiltration using percutaneously placed catheters in patients with unresectable hepatic malignancies. J. Clin. Oncol. 2005, 23, 3465–3474. [Google Scholar] [CrossRef] [Green Version]
- Heusner, T.A.; Antoch, G.; Wittkowski-Sterczewski, A.; Ladd, S.C.; Forsting, M.; Verhagen, R.; Scheulen, M. Transarterial hepatic chemoperfusion of uveal melanoma metastases: Survival and response to treatment. Fortschr Röntgenstr 2011, 183, 1151–1160. [Google Scholar] [CrossRef]
- Buzzacco, D.M.; Abdel-Rahman, M.H.; Park, S.; Davidorf, F.; Olencki, T.; Cebulla, C.M. Long-term survivors with metastatic uveal melanoma. Open Ophthalmol. J. 2012, 6, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Ludwig, J.; Haubold, J.; Heusner, T.A.; Bauer, S.; Siveke, J.T.; Richly, H.; Wetter, A.; Umutlu, L.; Theysohn, J.M. Lactate Dehydrogenase Prior to Transarterial Hepatic Chemoperfusion Predicts Survival and Time to Progression in Patients with Uveal Melanoma Liver Metastases. Fortschr Röntgenstr 2021, 193, 683–691. [Google Scholar] [CrossRef]
- Teal, L.; Yorio, J. Fulminant Hepatic Failure after Chemosaturation with Percutaneous Hepatic Perfusion and Nivolumab in a Patient with Metastatic Uveal Melanoma. Case Rep. Oncol. Med. 2021, 2021, 8870334. [Google Scholar] [CrossRef] [PubMed]
- Libutti, S.K.; Barlett, D.L.; Fraker, D.L.; Alexander, H.R. Technique and results of hyperthermic isolated hepatic perfusion with tumor necrosis factor and melphalan for the treatment of unresectable hepatic malignancies. J. Am. Coll. Surg. 2000, 191, 519–530. [Google Scholar] [CrossRef]
- Rizell, M.; Mattson, J.; Cahlin, C.; Hafstrom, L.; Lindner, P.; Olausson, M. Isolated hepatic perfusion for liver metastases of malignant melanoma. Melanoma Res. 2008, 18, 120–126. [Google Scholar] [CrossRef]
- Magge, D.; Choudry, H.A.; Zeh, H.J., 3rd; Cunningham, D.E.; Steel, J.; Holtzman, M.P.; Jones, H.L.; Pingpank, J.F.; Bartlett, D.L.; Zureikat, A.H. Outcome analysis of a decade-long experience of isolated hepatic perfusion for unresectable liver metastases at a single institution. Ann. Surg. 2014, 259, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Vogl, T.J.; Zangos, S.; Scholtz, J.E.; Schmitt, F.; Paetzold, S.; Trojan, J.; Orsi, F.; Lotz, G.; Ferrucci, P. Chemosaturation with percutaneous hepatic perfusions of melphalan for hepatic metastases: Experience from two European centers. Fortschr Röntgenstr 2014, 186, 937–944. [Google Scholar] [CrossRef] [Green Version]
- Hughes, M.S.; Zager, J.; Faries, M.; Alexander, H.R.; Royal, R.E.; Wood, B.; Choi, J.; McCluskey, K.; Whitman, E.; Agarwala, S.; et al. Results of a Randomized Controlled Multicenter Phase III Trial of Percutaneous Hepatic Perfusion Compared with Best Available Care for Patients with Melanoma Liver Metastases. Ann. Surg. Oncol. 2016, 23, 1309–1319. [Google Scholar] [CrossRef]
- Abbott, A.M.; Doepker, M.P.; Kim, Y.; Perez, M.C.; Gandle, C.; Thomas, K.L.; Choi, J.; Shridhar, R.; Zager, J.S. Hepatic Progression-free and Overall Survival After Regional Therapy to the Liver for Metastatic Melanoma. Am. J. Clin. Oncol. 2018, 41, 747–753. [Google Scholar] [CrossRef]
- Dewald, C.L.A.; Becker, L.S.; Maschke, S.K.; Meine, T.C.; Alten, T.A.; Kirstein, M.M.; Vogel, A.; Wacker, F.K.; Meyer, B.C.; Hinrichs, J.B. Percutaneous isolated hepatic perfusion (chemosaturation) with melphalan following right hemihepatectomy in patients with cholangiocarcinoma and metastatic uveal melanoma: Peri- and post-interventional adverse events and therapy response compared to a matched group without prior liver surgery. Clin. Exp. Metastasis 2020, 37, 683–692. [Google Scholar] [CrossRef]
- Noter, S.L.; Rothbarth, J.; Pijl, M.E.; Keunen, J.E.; Hartgrink, H.H.; Tijl, F.G.; Kuppen, P.J.; van de Velde, C.J.; Tollenaar, R.A. Isolated hepatic perfusion with high-dose melphalan for the treatment of uveal melanoma metastases confined to the liver. Melanoma Res. 2004, 14, 67–72. [Google Scholar] [CrossRef]
- Van Iersel, L.B.; Hoekman, E.J.; Gelderblom, H.; Vahrmeijer, A.L.; van Persijn van Meerten, E.L.; Tijl, F.G.; Hartgrink, H.H.; Kuppen, P.J.; Nortier, J.W.; Tollenaar, R.A.; et al. Isolated hepatic perfusion with 200 mg melphalan for advanced noncolorectal liver metastases. Ann. Surg. Oncol. 2008, 15, 1891–1898. [Google Scholar] [CrossRef] [Green Version]
- Van Iersel, L.B.; de Leede, E.M.; Vahrmeijer, A.L.; Tijl, F.G.; den Hartigh, J.; Kuppen, P.J.; Hartgrink, H.H.; Gelderblom, H.; Nortier, J.W.; Tollenaar, R.A.; et al. Isolated hepatic perfusion with oxaliplatin combined with 100 mg melphalan in patients with metastases confined to the liver: A phase I study. Eur. J. Surg. Oncol. 2014, 40, 1557–1563. [Google Scholar] [CrossRef]
- Van Etten, B.; Brunstein, F.; van, I.M.G.; Marinelli, A.W.; Verhoef, C.; van der Sijp, J.R.; Guetens, G.; de Boeck, G.; de Bruijn, E.A.; de Wilt, J.H.; et al. Isolated hypoxic hepatic perfusion with orthograde or retrograde flow in patients with irresectable liver metastases using percutaneous balloon catheter techniques: A phase I and II study. Ann. Surg. Oncol. 2004, 11, 598–605. [Google Scholar] [CrossRef]
- Verhoef, C.; de Wilt, J.H.; Brunstein, F.; Marinelli, A.W.; van Etten, B.; Vermaas, M.; Guetens, G.; de Boeck, G.; de Bruijn, E.A.; Eggermont, A.M. Isolated hypoxic hepatic perfusion with retrograde outflow in patients with irresectable liver metastases; a new simplified technique in isolated hepatic perfusion. Ann. Surg. Oncol. 2008, 15, 1367–1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Etten, B.; de Wilt, J.H.; Brunstein, F.; Eggermont, A.M.; Verhoef, C. Isolated hypoxic hepatic perfusion with melphalan in patients with irresectable ocular melanoma metastases. Eur. J. Surg. Oncol. 2009, 35, 539–545. [Google Scholar] [CrossRef]
- Kirstein, M.M.; Marquardt, S.; Jedicke, N.; Marhenke, S.; Koppert, W.; Manns, M.P.; Wacker, F.; Vogel, A. Safety and efficacy of chemosaturation in patients with primary and secondary liver tumors. J. Cancer Res. Clin. Oncol. 2017, 143, 2113–2121. [Google Scholar] [CrossRef] [PubMed]
- Vogl, T.J.; Koch, S.A.; Lotz, G.; Gebauer, B.; Willinek, W.; Engelke, C.; Bruning, R.; Zeile, M.; Wacker, F.; Vogel, A.; et al. Percutaneous Isolated Hepatic Perfusion as a Treatment for Isolated Hepatic Metastases of Uveal Melanoma: Patient Outcome and Safety in a Multi-centre Study. Cardiovasc. Interv. Radiol. 2017, 40, 864–872. [Google Scholar] [CrossRef]
- Schonfeld, L.; Hinrichs, J.B.; Marquardt, S.; Voigtlander, T.; Dewald, C.; Koppert, W.; Manns, M.P.; Wacker, F.; Vogel, A.; Kirstein, M.M. Chemosaturation with percutaneous hepatic perfusion is effective in patients with ocular melanoma and cholangiocarcinoma. J. Cancer Res. Clin. Oncol. 2020, 146, 3003–3012. [Google Scholar] [CrossRef] [PubMed]
- Artzner, C.; Mossakowski, O.; Hefferman, G.; Grosse, U.; Hoffmann, R.; Forschner, A.; Eigentler, T.; Syha, R.; Grozinger, G. Chemosaturation with percutaneous hepatic perfusion of melphalan for liver-dominant metastatic uveal melanoma: A single center experience. Cancer Imaging 2019, 19, 31. [Google Scholar] [CrossRef] [Green Version]
- Olofsson, R.; Cahlin, C.; All-Ericsson, C.; Hashimi, F.; Mattsson, J.; Rizell, M.; Lindner, P. Isolated hepatic perfusion for ocular melanoma metastasis: Registry data suggests a survival benefit. Ann. Surg. Oncol. 2014, 21, 466–472. [Google Scholar] [CrossRef] [Green Version]
- Forster, M.R.; Rashid, O.M.; Perez, M.C.; Choi, J.; Chaudhry, T.; Zager, J.S. Chemosaturation with percutaneous hepatic perfusion for unresectable metastatic melanoma or sarcoma to the liver: A single institution experience. J. Surg. Oncol. 2014, 109, 434–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, H.R.; Libutti, S.K.; Bartlett, D.L.; Puhlmann, M.; Fraker, D.L.; Bachenheimer, L.C. A phase I-II study of isolated hepatic perfusion using melphalan with or without tumor necrosis factor for patients with ocular melanoma metastatic to liver. Clin. Cancer Res. 2000, 6, 3062–3070. [Google Scholar] [PubMed]
- Varghese, S.; Xu, H.; Bartlett, D.; Hughes, M.; Pingpank, J.F.; Beresnev, T.; Alexander, H.R., Jr. Isolated hepatic perfusion with high-dose melphalan results in immediate alterations in tumor gene expression in patients with metastatic ocular melanoma. Ann. Surg. Oncol. 2010, 17, 1870–1877. [Google Scholar] [CrossRef] [PubMed]
- Alexander, H.R., Jr.; Libutti, S.K.; Pingpank, J.F.; Steinberg, S.M.; Bartlett, D.L.; Helsabeck, C.; Beresneva, T. Hyperthermic isolated hepatic perfusion using melphalan for patients with ocular melanoma metastatic to liver. Clin. Cancer Res. 2003, 9, 6343–6349. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shabat, I.; Belgrano, V.; Ny, L.; Nilsson, J.; Lindner, P.; Olofsson Bagge, R. Long-Term Follow-Up Evaluation of 68 Patients with Uveal Melanoma Liver Metastases Treated with Isolated Hepatic Perfusion. Ann. Surg. Oncol. 2016, 23, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Bruning, R.; Tiede, M.; Schneider, M.; Wohlmuth, P.; Weilert, H.; Oldhafer, K.; Stang, A. Unresectable Hepatic Metastasis of Uveal Melanoma: Hepatic Chemosaturation with High-Dose Melphalan-Long-Term Overall Survival Negatively Correlates with Tumor Burden. Radiol. Res. Pract. 2020, 2020, 5672048. [Google Scholar] [CrossRef]
- Dewald, C.L.A.; Hinrichs, J.B.; Becker, L.S.; Maschke, S.; Meine, T.C.; Saborowski, A.; Schonfeld, L.J.; Vogel, A.; Kirstein, M.M.; Wacker, F.K. Chemosaturation with Percutaneous Hepatic Perfusion: Outcome and Safety in Patients with Metastasized Uveal Melanoma. Fortschr Röntgenstr 2021, 193, 928–936. [Google Scholar] [CrossRef]
- Estler, A.; Artzner, C.; Bitzer, M.; Nikolaou, K.; Hoffmann, R.; Hepp, T.; Hagen, F.; Eigentler, T.; Forschner, A.; Grozinger, G. Efficacy and tolerability of chemosaturation in patients with hepatic metastases from uveal melanoma. Acta Radiol. 2021, 2841851211019808. [Google Scholar] [CrossRef]
- Karydis, I.; Gangi, A.; Wheater, M.J.; Choi, J.; Wilson, I.; Thomas, K.; Pearce, N.; Takhar, A.; Gupta, S.; Hardman, D.; et al. Percutaneous hepatic perfusion with melphalan in uveal melanoma: A safe and effective treatment modality in an orphan disease. J. Surg. Oncol. 2018, 117, 1170–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Leede, E.M.; Burgmans, M.C.; Kapiteijn, E.; Luyten, G.P.; Jager, M.J.; Tijl, F.G.; Hartgrink, H.H.; Grunhagen, D.J.; Rothbarth, J.; van de Velde, C.J.; et al. Isolated (hypoxic) hepatic perfusion with high-dose chemotherapy in patients with unresectable liver metastases of uveal melanoma: Results from two experienced centres. Melanoma Res. 2016, 26, 588–594. [Google Scholar] [CrossRef]
- Meijer, T.S.; Burgmans, M.C.; Fiocco, M.; de Geus-Oei, L.F.; Kapiteijn, E.; de Leede, E.M.; Martini, C.H.; van der Meer, R.W.; Tijl, F.G.J.; Vahrmeijer, A.L. Safety of Percutaneous Hepatic Perfusion with Melphalan in Patients with Unresectable Liver Metastases from Ocular Melanoma Using the Delcath Systems’ Second-Generation Hemofiltration System: A Prospective Non-randomized Phase II Trial. Cardiovasc. Interv. Radiol. 2019, 42, 841–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijer, T.S.; Burgmans, M.C.; de Leede, E.M.; de Geus-Oei, L.F.; Boekestijn, B.; Handgraaf, H.J.M.; Hilling, D.E.; Lutjeboer, J.; Vuijk, J.; Martini, C.H.; et al. Percutaneous Hepatic Perfusion with Melphalan in Patients with Unresectable Ocular Melanoma Metastases Confined to the Liver: A Prospective Phase II Study. Ann. Surg. Oncol. 2021, 28, 1130–1141. [Google Scholar] [CrossRef] [PubMed]
- Quadri, H.S.; Payabyab, E.C.; Chen, D.J.; Figg, W.; Hughes, M.S. Percutaneous hepatic perfusion with melphalan for unresectable liver metastasis. Hepatoma Res. 2016, 2, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Heppt, M.V.; Amaral, T.; Kahler, K.C.; Heinzerling, L.; Hassel, J.C.; Meissner, M.; Kreuzberg, N.; Loquai, C.; Reinhardt, L.; Utikal, J.; et al. Combined immune checkpoint blockade for metastatic uveal melanoma: A retrospective, multi-center study. J. Immunother. Cancer 2019, 7, 299. [Google Scholar] [CrossRef] [PubMed]
- Heppt, M.V.; Heinzerling, L.; Kahler, K.C.; Forschner, A.; Kirchberger, M.C.; Loquai, C.; Meissner, M.; Meier, F.; Terheyden, P.; Schell, B.; et al. Prognostic factors and outcomes in metastatic uveal melanoma treated with programmed cell death-1 or combined PD-1/cytotoxic T-lymphocyte antigen-4 inhibition. Eur. J. Cancer 2017, 82, 56–65. [Google Scholar] [CrossRef]
- Algazi, A.P.; Tsai, K.K.; Shoushtari, A.N.; Munhoz, R.R.; Eroglu, Z.; Piulats, J.M.; Ott, P.A.; Johnson, D.B.; Hwang, J.; Daud, A.I.; et al. Clinical outcomes in metastatic uveal melanoma treated with PD-1 and PD-L1 antibodies. Cancer 2016, 122, 3344–3353. [Google Scholar] [CrossRef]
- Zimmer, L.; Vaubel, J.; Mohr, P.; Hauschild, A.; Utikal, J.; Simon, J.; Garbe, C.; Herbst, R.; Enk, A.; Kampgen, E.; et al. Phase II DeCOG-study of ipilimumab in pretreated and treatment-naive patients with metastatic uveal melanoma. PLoS ONE 2015, 10, e0118564. [Google Scholar] [CrossRef]
- Mignard, C.; Deschamps Huvier, A.; Gillibert, A.; Duval Modeste, A.B.; Dutriaux, C.; Khammari, A.; Avril, M.F.; Kramkimel, N.; Mortier, L.; Marcant, P.; et al. Efficacy of Immunotherapy in Patients with Metastatic Mucosal or Uveal Melanoma. J. Oncol. 2018, 2018, 1908065. [Google Scholar] [CrossRef] [Green Version]
- Ny, L.; Jespersen, H.; Karlsson, J.; Alsen, S.; Filges, S.; All-Eriksson, C.; Andersson, B.; Carneiro, A.; Helgadottir, H.; Levin, M.; et al. The PEMDAC phase 2 study of pembrolizumab and entinostat in patients with metastatic uveal melanoma. Nat. Commun. 2021, 12, 5155. [Google Scholar] [CrossRef]
- Piperno-Neumann, S.; Hassel, J.C.; Rutkowski, P.; Baurain, J.; Butler, M.O.; Schlaak, M.; Sullivan, R.J.; Ochsenreither, S.; Dummer, R.; Kirkwood, J.M.; et al. Phase 3 randomized trial comparing tebentafusp with investigator’s choice in first line metastatic uveal melanoma. In Proceedings of the Proceedings of the 112th Annual Meeting of the American Association for Cancer Research, Philadelphia, PA, USA, 10–15 April 2021; 17–21 May 2021. [Google Scholar]
- Olofsson, R.; Ny, L.; Eilard, M.S.; Rizell, M.; 2021Cahlin, C.; Stierner, U.; Lonn, U.; Hansson, J.; Ljuslinder, I.; Lundgren, L.; et al. Isolated hepatic perfusion as a treatment for uveal melanoma liver metastases (the SCANDIUM trial): Study protocol for a randomized controlled trial. Trials 2014, 15, 317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCT02678572, Percutaneous Hepatic Perfusion vs. Best Alternative Care in Patients with Hepatic-dominant Ocular Melanoma. 2016. Available online: https://clinicaltrials.gov/show/NCT02678572 (accessed on 10 June 2021).
- Zager, J.S.; Orloff, M.; Ferrucci, P.F.; Glazer, E.S.; Ejaz, A.; Richtig, E.; Ochsenreither, S.; Lowe, M.C.; Reddy, S.A.; Beasley, G.; et al. Percutaneous hepatic perfusion (PHP) with melphalan for patients with ocular melanoma liver metastases: Preliminary results of FOCUS (PHP-OCM-301/301A) phase III trial. J. Clin. Oncol. 2021, 39, 9510. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Author | Year of Publication | Study Design | No. of Centers (Country) | Number of Patients | Technique | Years of Inclusion |
|---|---|---|---|---|---|---|
| Alexander [57] | 2003 | Phase I + II | 1 (USA) | 29 | IHP | 1997–2002 |
| Ben-Shabat [58] | 2016 | Retrospective | 1 (SWE) | 68 | IHP | 1989–2013 |
| Brüning [59] | 2020 | Retrospective | 1 (DEU) | 19 | PHP | 2014–2019 |
| Dewald [60] | 2021 | Retrospective | 1 (DEU) | 30 | PHP | 2014–2019 |
| Estler [61] | 2021 | Retrospective | 1 (DEU) | 29 | PHP | 2015–2020 |
| Karydis [62] | 2018 | Retrospective | 2 (GBR and USA) | 51 | PHP | 2008–2016 |
| de Leede [63] | 2016 | Retrospective | 2 (NLD) | 31 | IHP | 1999–2009 |
| Meijer [64,65] | 2019 + 2021 | Phase II | 1 (NLD) | 35 | PHP | 2014–2017 |
| Study | Age (Years) (Range) | Female: Male (No. of Patients) | Tumor Load (No. of Patients) | Extra-Hepatic Disease (No. of Patients, %) | |
|---|---|---|---|---|---|
| Alexander [57] | 49 (26–73) | 15:14 | <25% 25–50% >50% | 20 8 1 | Not Included |
| Ben-Shabat [58] | 61 (18–77) | 40:28 | 1–4 met 5–10 met 11–100 met >100 met | 11 24 13 4 | Not Included |
| Brüning [59] | 58 (range not specified) | 8:11 | Not specified | Included Number of patients not specified | |
| Dewald [60] | 57 (52–66) | 21:9 | ≤30% >30% | 21 8 | 5 (16.7%) |
| Estler [61] | 69.7 (30–81) | 18:11 | <25% >25% | 22 7 | 12 (41.4%) |
| Karydis [62] | 57.9 (27.9–77.1) | 28:23 | 1–3 met 4–10 met >10 met |
12 23 16 | 8 (15.7%) |
| de Leede [63] | 57 (27–68) | 19:12 | <50% | 31 | Not Included |
| Meijer [64,65] | 59 (42–71) | 19:16 | 1–5 met 6–9 met ≥10 met | 9 8 18 | Not Included |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bethlehem, M.S.; Katsarelias, D.; Olofsson Bagge, R. Meta-Analysis of Isolated Hepatic Perfusion and Percutaneous Hepatic Perfusion as a Treatment for Uveal Melanoma Liver Metastases. Cancers 2021, 13, 4726. https://doi.org/10.3390/cancers13184726
Bethlehem MS, Katsarelias D, Olofsson Bagge R. Meta-Analysis of Isolated Hepatic Perfusion and Percutaneous Hepatic Perfusion as a Treatment for Uveal Melanoma Liver Metastases. Cancers. 2021; 13(18):4726. https://doi.org/10.3390/cancers13184726
Chicago/Turabian StyleBethlehem, Martijn S., Dimitrios Katsarelias, and Roger Olofsson Bagge. 2021. "Meta-Analysis of Isolated Hepatic Perfusion and Percutaneous Hepatic Perfusion as a Treatment for Uveal Melanoma Liver Metastases" Cancers 13, no. 18: 4726. https://doi.org/10.3390/cancers13184726