
Updated Principles of Surgical Management of Pancreatic Neuroendocrine Tumours (pNETs): What Every Surgeon Needs to Know

1
Department of General, Visceral, and Endocrine Surgery, Pitié-Salpêtrière Hospital, AP-HP, Bat. Husson Mourier, 47-83 Boulevard de l’Hôpital, 75013 Paris, France
2
Department of Hepato-Biliary and Pancreatic Surgery and Liver Transplantation, AP-HP, Bat. Husson Mourier, 47-83 Boulevard de l’Hôpital, 75013 Paris, France
3
Paris-Sorbonne University, 21 rue de l’Ecole de Médecine, 75006 Paris, France
*
Author to whom correspondence should be addressed.
Cancers 2021, 13(23), 5969; https://doi.org/10.3390/cancers13235969
Submission received: 31 October 2021
/
Revised: 25 November 2021
/
Accepted: 25 November 2021
/
Published: 27 November 2021
(This article belongs to the Collection Neuroendocrine Tumors: Treatment and Management)
{kind=link}
Simple Summary
In this narrative review, we update the surgical management of pancreatic neuroendocrine tumours (pNETs) and highlight key elements in view of the recent literature. These tumours are rare and suffer from a lack of data and randomized controlled trials. The pNETs management is difficult due to their heterogeneity and the risks associated with pancreatic surgery. Innovative managements such as “watch and wait” strategies, parenchymal sparing surgery and minimally invasive approach are emerging. The correct use of all these therapeutic options requires a good selection of patients but also a constant update of knowledge.
Abstract
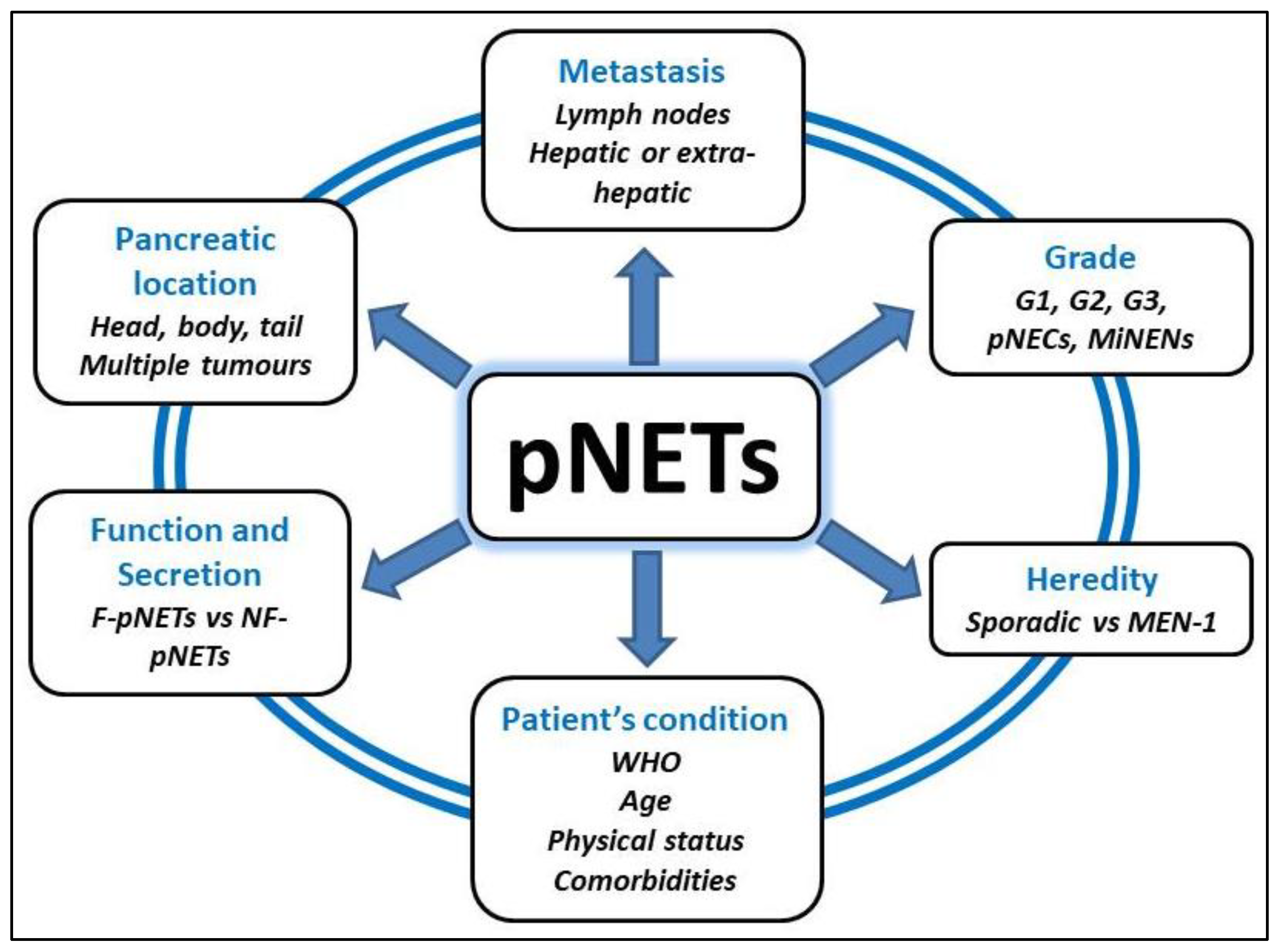
Pancreatic neuroendocrine tumours (pNETs) represent 1 to 2% of all pancreatic neoplasm with an increasing incidence. They have a varied clinical, biological and radiological presentation, depending on whether they are sporadic or genetic in origin, whether they are functional or non-functional, and whether there is a single or multiple lesions. These pNETs are often diagnosed at an advanced stage with locoregional lymph nodes invasion or distant metastases. In most cases, the gold standard curative treatment is surgical resection of the pancreatic tumour, but the postoperative complications and functional consequences are not negligible. Thus, these patients should be managed in specialised high-volume centres with multidisciplinary discussion involving surgeons, oncologists, radiologists and pathologists. Innovative managements such as “watch and wait” strategies, parenchymal sparing surgery and minimally invasive approach are emerging. The correct use of all these therapeutic options requires a good selection of patients but also a constant update of knowledge. The aim of this work is to update the surgical management of pNETs and to highlight key elements in view of the recent literature.