
Risk-Adapted, Individualized Treatment Strategies of Myelodysplastic Syndromes (MDS) and Chronic Myelomonocytic Leukemia (CMML)



Abstract
:Simple Summary
Abstract
1. Introduction
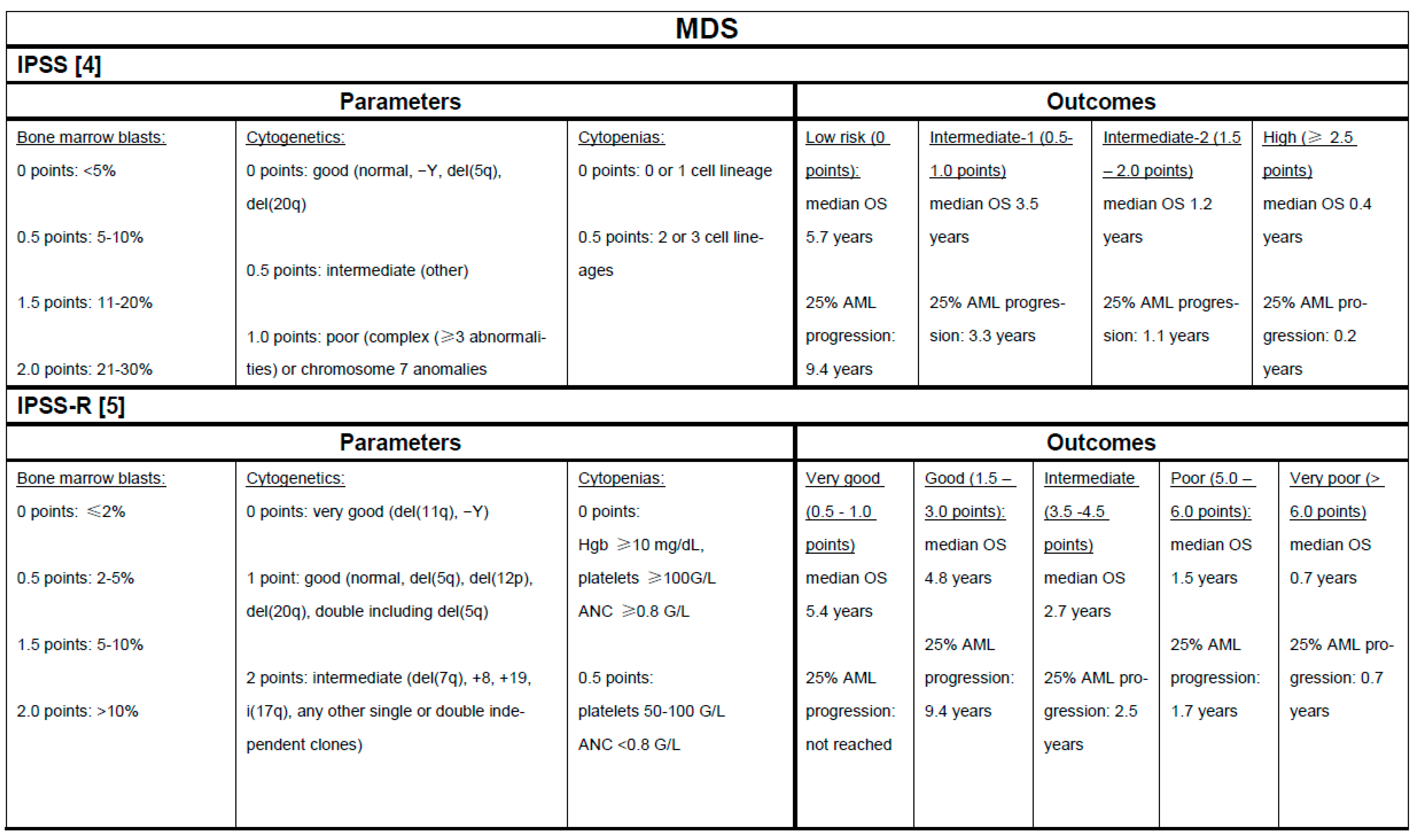
2. Risk Stratification in MDS and CMML as the Basis for Treatment Selection
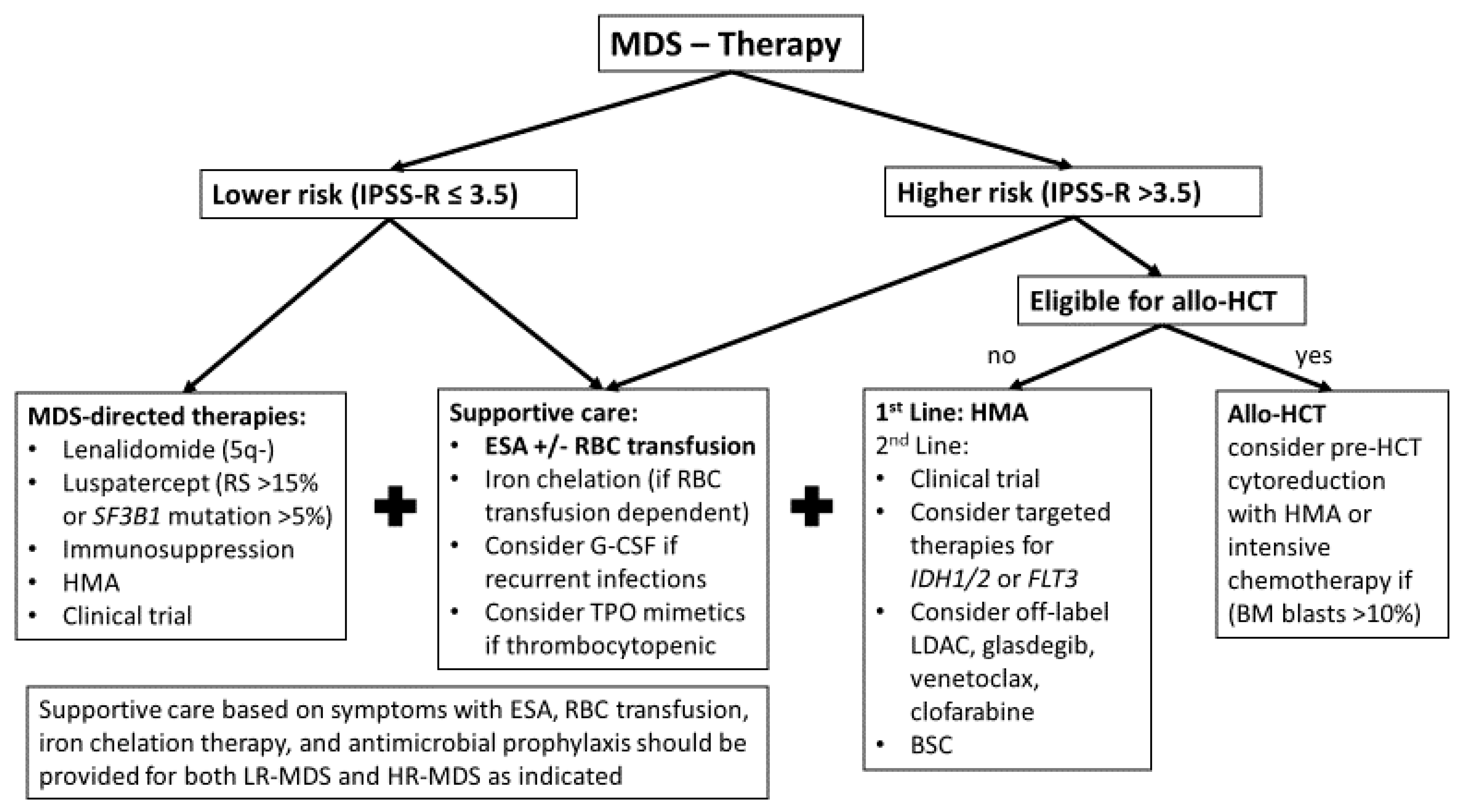
3. Treatment Algorithm for MDS
3.1. Lower-Risk MDS
3.2. Higher-Risk MDS
4. Treatment Algorithm for CMML
5. Future Directions
6. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Platzbecker, U. Treatment of MDS. Blood 2019, 133, 1096–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, P.L.; Stone, R.M.; Al-Kali, A.; Barta, S.K.; Bejar, R.; Bennett, J.M.; Carraway, H.; De Castro, C.M.; Deeg, H.J.; DeZern, A.E.; et al. Myelodysplastic Syndromes, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 60–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bewersdorf, J.P.; Zeidan, A.M. Prognostic Models in Myelodysplastic Syndromes. In Diagnosis and Management of Myelodysplastic Syndromes: A Clinical Guide; Nazha, A., Ed.; Springer International Publishing: Cham, Switzerland, 2020; pp. 109–127. [Google Scholar] [CrossRef]
- Greenberg, P.; Cox, C.; LeBeau, M.M.; Fenaux, P.; Morel, P.; Sanz, G.; Sanz, M.; Vallespi, T.; Hamblin, T.; Oscier, D.; et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood 1997, 89, 2079–2088. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.L.; Tuechler, H.; Schanz, J.; Sanz, G.; Garcia-Manero, G.; Solé, F.; Bennett, J.M.; Bowen, D.; Fenaux, P.; Dreyfus, F.; et al. Revised international prognostic scoring system for myelodysplastic syndromes. Blood 2012, 120, 2454–2465. [Google Scholar] [CrossRef] [PubMed]
- Bernard, E.; Nannya, Y.; Hasserjian, R.P.; Devlin, S.M.; Tuechler, H.; Medina-Martinez, J.S.; Yoshizato, T.; Shiozawa, Y.; Saiki, R.; Malcovati, L.; et al. Implications of TP53 allelic state for genome stability, clinical presentation and outcomes in myelodysplastic syndromes. Nat. Med. 2020. [Google Scholar] [CrossRef]
- Fenaux, P.; Platzbecker, U.; Mufti, G.J.; Garcia-Manero, G.; Buckstein, R.; Santini, V.; Diez-Campelo, M.; Finelli, C.; Cazzola, M.; Ilhan, O.; et al. Luspatercept in Patients with Lower-Risk Myelodysplastic Syndromes. N. Engl. J. Med. 2020, 382, 140–151. [Google Scholar] [CrossRef]
- Bejar, R.; Papaemmanuil, E.; Haferlach, T.; Garcia-Manero, G.; Maciejewski, J.P.; Sekeres, M.A.; Walter, M.J.; Graubert, T.A.; Cazzola, M.; Malcovati, L.; et al. Somatic Mutations in MDS Patients Are Associated with Clinical Features and Predict Prognosis Independent of the IPSS-R: Analysis of Combined Datasets from the International Working Group for Prognosis in MDS-Molecular Committee. Blood 2015, 126, 907. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Patnaik, M.M.; Tefferi, A. Chronic Myelomonocytic leukemia: 2020 update on diagnosis, risk stratification and management. Am. J. Hematol. 2020, 95, 97–115. [Google Scholar] [CrossRef] [Green Version]
- Valent, P.; Orazi, A.; Savona, M.R.; Patnaik, M.M.; Onida, F.; van de Loosdrecht, A.A.; Haase, D.; Haferlach, T.; Elena, C.; Pleyer, L.; et al. Proposed diagnostic criteria for classical chronic myelomonocytic leukemia (CMML), CMML variants and pre-CMML conditions. Haematologica 2019, 104, 1935–1949. [Google Scholar] [CrossRef]
- Bewersdorf, J.P.; Carraway, H.; Prebet, T. Emerging treatment options for patients with high-risk myelodysplastic syndrome. Ther. Adv. Hematol. 2020, 11, 2040620720955006. [Google Scholar] [CrossRef]
- Bewersdorf, J.P.; Zeidan, A.M. Following in the footsteps of acute myeloid leukemia: Are we witnessing the start of a therapeutic revolution for higher-risk myelodysplastic syndromes? Leuk. Lymphoma 2020, 1–18. [Google Scholar] [CrossRef]
- Cazzola, M. Myelodysplastic Syndromes. N. Engl. J. Med. 2020, 383, 1358–1374. [Google Scholar] [CrossRef]
- Nazha, A.; Komrokji, R.S.; Garcia-Manero, G.; Barnard, J.; Roboz, G.J.; Steensma, D.P.; DeZern, A.E.; Zell, K.; Zimmerman, C.; Ali, N.A.; et al. The efficacy of current prognostic models in predicting outcome of patients with myelodysplastic syndromes at the time of hypomethylating agent failure. Haematologica 2016, 101, e224–e227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Manero, G.; Shan, J.; Faderl, S.; Cortes, J.; Ravandi, F.; Borthakur, G.; Wierda, W.G.; Pierce, S.; Estey, E.; Liu, J.; et al. A prognostic score for patients with lower risk myelodysplastic syndrome. Leukemia 2008, 22, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Quintás-Cardama, A.; Daver, N.; Kim, H.; Dinardo, C.; Jabbour, E.; Kadia, T.; Borthakur, G.; Pierce, S.; Shan, J.; Cardenas-Turanzas, M.; et al. A prognostic model of therapy-related myelodysplastic syndrome for predicting survival and transformation to acute myeloid leukemia. Clin. Lymphoma Myeloma Leuk. 2014, 14, 401–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haferlach, T.; Nagata, Y.; Grossmann, V.; Okuno, Y.; Bacher, U.; Nagae, G.; Schnittger, S.; Sanada, M.; Kon, A.; Alpermann, T.; et al. Landscape of genetic lesions in 944 patients with myelodysplastic syndromes. Leukemia 2014, 28, 241–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazha, A.; Narkhede, M.; Radivoyevitch, T.; Seastone, D.J.; Patel, B.J.; Gerds, A.T.; Mukherjee, S.; Kalaycio, M.; Advani, A.; Przychodzen, B.; et al. Incorporation of molecular data into the Revised International Prognostic Scoring System in treated patients with myelodysplastic syndromes. Leukemia 2016, 30, 2214–2220. [Google Scholar] [CrossRef]
- Haase, D.; Stevenson, K.E.; Neuberg, D.; Maciejewski, J.P.; Nazha, A.; Sekeres, M.A.; Ebert, B.L.; Garcia-Manero, G.; Haferlach, C.; Haferlach, T.; et al. TP53 mutation status divides myelodysplastic syndromes with complex karyotypes into distinct prognostic subgroups. Leukemia 2019, 33, 1747–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malcovati, L.; Stevenson, K.; Papaemmanuil, E.; Neuberg, D.; Bejar, R.; Boultwood, J.; Bowen, D.T.; Campbell, P.J.; Ebert, B.L.; Fenaux, P.; et al. SF3B1-mutant MDS as a distinct disease subtype: A proposal from the International Working Group for the Prognosis of MDS. Blood 2020, 136, 157–170. [Google Scholar] [CrossRef]
- Bejar, R.; Lord, A.; Stevenson, K.; Bar-Natan, M.; Perez-Ladaga, A.; Zaneveld, J.; Wang, H.; Caughey, B.; Stojanov, P.; Getz, G.; et al. TET2 mutations predict response to hypomethylating agents in myelodysplastic syndrome patients. Blood 2014, 124, 2705–2712. [Google Scholar] [CrossRef]
- Hunter, A.M.; Komrokji, R.S.; Yun, S.; Al Ali, N.; Chan, O.; Song, J.; Hussaini, M.; Talati, C.; Sweet, K.L.; Lancet, J.E.; et al. Baseline and serial molecular profiling predicts outcomes with hypomethylating agents in myelodysplastic syndromes. Blood Adv. 2021, 5, 1017–1028. [Google Scholar] [CrossRef] [PubMed]
- Onida, F.; Kantarjian, H.M.; Smith, T.L.; Ball, G.; Keating, M.J.; Estey, E.H.; Glassman, A.B.; Albitar, M.; Kwari, M.I.; Beran, M. Prognostic factors and scoring systems in chronic myelomonocytic leukemia: A retrospective analysis of 213 patients. Blood 2002, 99, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Such, E.; Germing, U.; Malcovati, L.; Cervera, J.; Kuendgen, A.; Della Porta, M.G.; Nomdedeu, B.; Arenillas, L.; Luño, E.; Xicoy, B.; et al. Development and validation of a prognostic scoring system for patients with chronic myelomonocytic leukemia. Blood 2013, 121, 3005–3015. [Google Scholar] [CrossRef]
- Elena, C.; Gallì, A.; Such, E.; Meggendorfer, M.; Germing, U.; Rizzo, E.; Cervera, J.; Molteni, E.; Fasan, A.; Schuler, E.; et al. Integrating clinical features and genetic lesions in the risk assessment of patients with chronic myelomonocytic leukemia. Blood 2016, 128, 1408–1417. [Google Scholar] [CrossRef]
- Palomo, L.; Garcia, O.; Arnan, M.; Xicoy, B.; Fuster, F.; Cabezón, M.; Coll, R.; Ademà, V.; Grau, J.; Jiménez, M.J.; et al. Targeted deep sequencing improves outcome stratification in chronic myelomonocytic leukemia with low risk cytogenetic features. Oncotarget 2016, 7, 57021–57035. [Google Scholar] [CrossRef] [PubMed]
- Palomo, L.; Meggendorfer, M.; Hutter, S.; Twardziok, S.; Ademà, V.; Fuhrmann, I.; Fuster-Tormo, F.; Xicoy, B.; Zamora, L.; Acha, P.; et al. Molecular landscape and clonal architecture of adult myelodysplastic/myeloproliferative neoplasms. Blood 2020, 136, 1851–1862. [Google Scholar] [CrossRef] [PubMed]
- Malcovati, L.; Germing, U.; Kuendgen, A.; Della Porta, M.G.; Pascutto, C.; Invernizzi, R.; Giagounidis, A.; Hildebrandt, B.; Bernasconi, P.; Knipp, S.; et al. Time-dependent prognostic scoring system for predicting survival and leukemic evolution in myelodysplastic syndromes. J. Clin. Oncol. 2007, 25, 3503–3510. [Google Scholar] [CrossRef] [PubMed]
- Della Porta, M.G.; Galli, A.; Bacigalupo, A.; Zibellini, S.; Bernardi, M.; Rizzo, E.; Allione, B.; van Lint, M.T.; Pioltelli, P.; Marenco, P.; et al. Clinical Effects of Driver Somatic Mutations on the Outcomes of Patients with Myelodysplastic Syndromes Treated with Allogeneic Hematopoietic Stem-Cell Transplantation. J. Clin. Oncol. 2016, 34, 3627–3637. [Google Scholar] [CrossRef] [PubMed]
- Malcovati, L.; Hellström-Lindberg, E.; Bowen, D.; Adès, L.; Cermak, J.; Del Cañizo, C.; Della Porta, M.G.; Fenaux, P.; Gattermann, N.; Germing, U.; et al. Diagnosis and treatment of primary myelodysplastic syndromes in adults: Recommendations from the European LeukemiaNet. Blood 2013, 122, 2943–2964. [Google Scholar] [CrossRef] [Green Version]
- Pfeilstöcker, M.; Tuechler, H.; Sanz, G.; Schanz, J.; Garcia-Manero, G.; Solé, F.; Bennett, J.M.; Bowen, D.; Fenaux, P.; Dreyfus, F.; et al. Time-dependent changes in mortality and transformation risk in MDS. Blood 2016, 128, 902–910. [Google Scholar] [CrossRef] [Green Version]
- Fenaux, P.; Platzbecker, U.; Ades, L. How we manage adults with myelodysplastic syndrome. Br. J. Haematol. 2020, 189, 1016–1027. [Google Scholar] [CrossRef]
- Santini, V. How I treat MDS after hypomethylating agent failure. Blood 2019, 133, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Lewis, R.; Bewersdorf, J.P.; Zeidan, A.M. Clinical Management of Anemia in Patients with Myelodysplastic Syndromes: An Update on Emerging Therapeutic Options. Cancer Manag. Res. 2021, 13, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Grabar, S.; Kelaidi, C.; Beyne-Rauzy, O.; Picard, F.; Bardet, V.; Coiteux, V.; Leroux, G.; Lepelley, P.; Daniel, M.T.; et al. Predictive factors of response and survival in myelodysplastic syndrome treated with erythropoietin and G-CSF: The GFM experience. Blood 2008, 111, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Santini, V.; Schemenau, J.; Levis, A.; Balleari, E.; Sapena, R.; Adès, L.; Guerci, A.; Beyne-Rauzy, O.; Gourin, M.-P.; Cheze, S.; et al. Can the revised IPSS predict response to erythropoietic-stimulating agents in patients with classical IPSS low or intermediate-1 MDS? Blood 2013, 122, 2286–2288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Fenaux, P.; Greenberg, P.; Mehta, B.; Callaghan, F.; Kim, C.; Tomita, D.; Xu, H. Efficacy and safety of darbepoetin alpha in patients with myelodysplastic syndromes: A systematic review and meta-analysis. Br. J. Haematol. 2016, 174, 730–747. [Google Scholar] [CrossRef]
- Hellström-Lindberg, E.; Gulbrandsen, N.; Lindberg, G.; Ahlgren, T.; Dahl, I.M.S.; Dybedal, I.; Grimfors, G.; Hesse-Sundin, E.; Hjorth, M.; Kanter-Lewensohn, L.; et al. A validated decision model for treating the anaemia of myelodysplastic syndromes with erythropoietin + granulocyte colony-stimulating factor: Significant effects on quality of life. Br. J. Haematol. 2003, 120, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Fenaux, P.; Santini, V.; Spiriti, M.A.A.; Giagounidis, A.; Schlag, R.; Radinoff, A.; Gercheva-Kyuchukova, L.; Anagnostopoulos, A.; Oliva, E.N.; Symeonidis, A.; et al. A phase 3 randomized, placebo-controlled study assessing the efficacy and safety of epoetin-α in anemic patients with low-risk MDS. Leukemia 2018, 32, 2648–2658. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, P.L.; Sun, Z.; Miller, K.B.; Bennett, J.M.; Tallman, M.S.; Dewald, G.; Paietta, E.; van der Jagt, R.; Houston, J.; Thomas, M.L.; et al. Treatment of myelodysplastic syndrome patients with erythropoietin with or without granulocyte colony-stimulating factor: Results of a prospective randomized phase 3 trial by the Eastern Cooperative Oncology Group (E1996). Blood 2009, 114, 2393–2400. [Google Scholar] [CrossRef] [Green Version]
- Angelucci, E.; Li, J.; Greenberg, P.; Wu, D.; Hou, M.; Montano Figueroa, E.H.; Rodriguez, M.G.; Dong, X.; Ghosh, J.; Izquierdo, M.; et al. Iron Chelation in Transfusion-Dependent Patients with Low- to Intermediate-1-Risk Myelodysplastic Syndromes: A Randomized Trial. Ann. Intern. Med. 2020, 172, 513–522. [Google Scholar] [CrossRef]
- List, A.; Dewald, G.; Bennett, J.; Giagounidis, A.; Raza, A.; Feldman, E.; Powell, B.; Greenberg, P.; Thomas, D.; Stone, R.; et al. Lenalidomide in the myelodysplastic syndrome with chromosome 5q deletion. N. Engl. J. Med. 2006, 355, 1456–1465. [Google Scholar] [CrossRef] [Green Version]
- Fenaux, P.; Giagounidis, A.; Selleslag, D.; Beyne-Rauzy, O.; Mufti, G.; Mittelman, M.; Muus, P.; Te Boekhorst, P.; Sanz, G.; Del Canizo, C.; et al. A randomized phase 3 study of lenalidomide versus placebo in RBC transfusion-dependent patients with Low-/Intermediate-1-risk myelodysplastic syndromes with del5q. Blood 2011, 118, 3765–3776. [Google Scholar] [CrossRef]
- Santini, V.; Almeida, A.; Giagounidis, A.; Gropper, S.; Jonasova, A.; Vey, N.; Mufti, G.J.; Buckstein, R.; Mittelman, M.; Platzbecker, U.; et al. Randomized Phase III Study of Lenalidomide Versus Placebo in RBC Transfusion-Dependent Patients with Lower-Risk Non-del(5q) Myelodysplastic Syndromes and Ineligible for or Refractory to Erythropoiesis-Stimulating Agents. J. Clin. Oncol. 2016, 34, 2988–2996. [Google Scholar] [CrossRef]
- Toma, A.; Kosmider, O.; Chevret, S.; Delaunay, J.; Stamatoullas, A.; Rose, C.; Beyne-Rauzy, O.; Banos, A.; Guerci-Bresler, A.; Wickenhauser, S.; et al. Lenalidomide with or without erythropoietin in transfusion-dependent erythropoiesis-stimulating agent-refractory lower-risk MDS without 5q deletion. Leukemia 2016, 30, 897–905. [Google Scholar] [CrossRef]
- Mossner, M.; Jann, J.C.; Nowak, D.; Platzbecker, U.; Giagounidis, A.; Gotze, K.; Letsch, A.; Haase, D.; Shirneshan, K.; Braulke, F.; et al. Prevalence, clonal dynamics and clinical impact of TP53 mutations in patients with myelodysplastic syndrome with isolated deletion (5q) treated with lenalidomide: Results from a prospective multicenter study of the german MDS study group (GMDS). Leukemia 2016, 30, 1956–1959. [Google Scholar] [CrossRef]
- Oliva, E.N.; Lauseker, M.; Aloe Spiriti, M.A.; Poloni, A.; Cortelezzi, A.; Palumbo, G.A.; Balleari, E.; Sanpaolo, G.; Volpe, A.; Ricco, A.; et al. Early lenalidomide treatment for low and intermediate-1 International Prognostic Scoring System risk myelodysplastic syndromes with del(5q) before transfusion dependence. Cancer Med. 2015, 4, 1789–1797. [Google Scholar] [CrossRef] [PubMed]
- Bewersdorf, J.P.; Zeidan, A.M. Transforming growth factor (TGF)-beta pathway as a therapeutic target in lower risk myelodysplastic syndromes. Leukemia 2019, 33, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Dorn, D.C.; Erdjument-Bromage, H.; Tempst, P.; Moore, M.A.; Massague, J. Hematopoiesis controlled by distinct TIF1gamma and Smad4 branches of the TGFbeta pathway. Cell 2006, 125, 929–941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suragani, R.N.; Cadena, S.M.; Cawley, S.M.; Sako, D.; Mitchell, D.; Li, R.; Davies, M.V.; Alexander, M.J.; Devine, M.; Loveday, K.S.; et al. Transforming growth factor-β superfamily ligand trap ACE-536 corrects anemia by promoting late-stage erythropoiesis. Nat. Med. 2014, 20, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Platzbecker, U.; Germing, U.; Gotze, K.S.; Kiewe, P.; Mayer, K.; Chromik, J.; Radsak, M.; Wolff, T.; Zhang, X.; Laadem, A.; et al. Luspatercept for the treatment of anaemia in patients with lower-risk myelodysplastic syndromes (PACE-MDS): A multicentre, open-label phase 2 dose-finding study with long-term extension study. Lancet Oncol. 2017, 18, 1338–1347. [Google Scholar] [CrossRef]
- Platzbecker, U.; Dunshee, D.; Komrokji, R.S.; Mufti, G.J.; Garcia-Manero, G.; Buckstein, R.; Santini, V.; Díez-Campelo, M.; Sekeres, M.A.; See, W.L.; et al. Luspatercept Significantly Reduces Red Blood Cell (RBC) Transfusion Burden, Regardless of Gene Mutation Frequency, Spectrum, and Prognostic Significance, Among Patients (Pts) with LR-MDS Enrolled in the MEDALIST Trial. Blood 2019, 134. [Google Scholar] [CrossRef]
- Garcia-Manero, G.; Mufti, G.J.; Fenaux, P.; Buckstein, R.; Santini, V.; Díez-Campelo, M.; Finelli, C.; Cazzola, M.; Ilhan, O.; Sekeres, M.A.; et al. Hematologic Improvement-Neutrophil and -Platelet in the MEDALIST Trial: Multilineage Data from a Phase 3, Randomized, Double-Blind, Placebo-Controlled Study of Luspatercept to Treat Anemia in Patients with Very Low-, Low-, or Intermediate-Risk Myelodysplastic Syndromes (MDS) with Ring Sideroblasts (RS) Who Require Red Blood Cell (RBC) Transfusions. Blood 2019, 134, 4243. [Google Scholar] [CrossRef]
- Oliva, E.N.; Platzbecker, U.; Garcia-Manero, G.; Mufti, G.J.; Santini, V.; Sekeres, M.A.; Komrokji, R.S.; Shetty, J.K.; Tang, D.; Guo, S.; et al. Health-Related Quality of Life Outcomes in Patients with Myelodysplastic Syndromes with Ring Sideroblasts Treated with Luspatercept in the Medalist Study. Blood 2020, 136, 10–12. [Google Scholar] [CrossRef]
- Komrokji, R.S.; Platzbecker, U.; Fenaux, P.; Garcia-Manero, G.; Mufti, G.J.; Santini, V.; Diez-Campelo, M.; Finelli, C.; Jurcic, J.G.; Greenberg, P.L.; et al. Efficacy and Safety of Luspatercept Treatment in Patients with Myelodysplastic Syndrome/Myeloproliferative Neoplasm with Ring Sideroblasts and Thrombocytosis (MDS/MPN-RS-T): A Retrospective Analysis from the Medalist Study. Blood 2020, 136, 13–15. [Google Scholar] [CrossRef]
- Della Porta, M.; Platzbecker, U.; Santini, V.; Garcia-Manero, G.; Komrokji, R.S.; Ito, R.; Fenaux, P. The Commands Trial: A Phase 3 Study of the Efficacy and Safety of Luspatercept Versus Epoetin Alfa for the Treatment of Anemia Due to IPSS-R Very Low-, Low-, or Intermediate-Risk MDS in Erythropoiesis Stimulating Agent-Naive Patients Who Require RBC Transfusions. Blood 2020, 136, 1–2. [Google Scholar] [CrossRef]
- Passweg, J.R.; Giagounidis, A.A.; Simcock, M.; Aul, C.; Dobbelstein, C.; Stadler, M.; Ossenkoppele, G.; Hofmann, W.K.; Schilling, K.; Tichelli, A.; et al. Immunosuppressive therapy for patients with myelodysplastic syndrome: A prospective randomized multicenter phase III trial comparing antithymocyte globulin plus cyclosporine with best supportive care—SAKK 33/99. J. Clin. Oncol. 2011, 29, 303–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stahl, M.; DeVeaux, M.; de Witte, T.; Neukirchen, J.; Sekeres, M.A.; Brunner, A.M.; Roboz, G.J.; Steensma, D.P.; Bhatt, V.R.; Platzbecker, U.; et al. The use of immunosuppressive therapy in MDS: Clinical outcomes and their predictors in a large international patient cohort. Blood Adv. 2018, 2, 1765–1772. [Google Scholar] [CrossRef] [Green Version]
- Stahl, M.; Bewersdorf, J.P.; Giri, S.; Wang, R.; Zeidan, A.M. Use of immunosuppressive therapy for management of myelodysplastic syndromes: A systematic review and meta-analysis. Haematologica 2020, 105, 102–111. [Google Scholar] [CrossRef] [Green Version]
- Sloand, E.M.; Wu, C.O.; Greenberg, P.; Young, N.; Barrett, J. Factors affecting response and survival in patients with myelodysplasia treated with immunosuppressive therapy. J. Clin. Oncol. 2008, 26, 2505–2511. [Google Scholar] [CrossRef]
- Bewersdorf, J.P.; Zeidan, A.M. Evolving therapies for lower-risk myelodysplastic syndromes. Ann. Hematol. 2020. [Google Scholar] [CrossRef]
- Girmenia, C.; Candoni, A.; Delia, M.; Latagliata, R.; Molteni, A.; Oliva, E.N.; Palumbo, G.A.; Poloni, A.; Salutari, P.; Santini, V.; et al. Infection control in patients with myelodysplastic syndromes who are candidates for active treatment: Expert panel consensus-based recommendations. Blood Rev. 2019, 34, 16–25. [Google Scholar] [CrossRef]
- Kantarjian, H.; Fenaux, P.; Sekeres, M.A.; Becker, P.S.; Boruchov, A.; Bowen, D.; Hellstrom-Lindberg, E.; Larson, R.A.; Lyons, R.M.; Muus, P.; et al. Safety and efficacy of romiplostim in patients with lower-risk myelodysplastic syndrome and thrombocytopenia. J. Clin. Oncol. 2010, 28, 437–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekeres, M.A.; Kantarjian, H.; Fenaux, P.; Becker, P.; Boruchov, A.; Guerci-Bresler, A.; Hu, K.; Franklin, J.; Wang, Y.M.; Berger, D. Subcutaneous or intravenous administration of romiplostim in thrombocytopenic patients with lower risk myelodysplastic syndromes. Cancer 2011, 117, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Oliva, E.N.; Alati, C.; Santini, V.; Poloni, A.; Molteni, A.; Niscola, P.; Salvi, F.; Sanpaolo, G.; Balleari, E.; Germing, U.; et al. Eltrombopag versus placebo for low-risk myelodysplastic syndromes with thrombocytopenia (EQoL-MDS): Phase 1 results of a single-blind, randomised, controlled, phase 2 superiority trial. Lancet Haematol 2017, 4, e127–e136. [Google Scholar] [CrossRef]
- Mittelman, M.; Platzbecker, U.; Afanasyev, B.; Grosicki, S.; Wong, R.S.M.; Anagnostopoulos, A.; Brenner, B.; Denzlinger, C.; Rossi, G.; Nagler, A.; et al. Eltrombopag for advanced myelodysplastic syndromes or acute myeloid leukaemia and severe thrombocytopenia (ASPIRE): A randomised, placebo-controlled, phase 2 trial. Lancet Haematol 2018, 5, e34–e43. [Google Scholar] [CrossRef]
- Dickinson, M.; Cherif, H.; Fenaux, P.; Mittelman, M.; Verma, A.; Portella, M.S.O.; Burgess, P.; Ramos, P.M.; Choi, J.; Platzbecker, U.; et al. Azacitidine with or without eltrombopag for first-line treatment of intermediate- or high-risk MDS with thrombocytopenia. Blood 2018, 132, 2629–2638. [Google Scholar] [CrossRef] [PubMed]
- Thepot, S.; Ben Abdelali, R.; Chevret, S.; Renneville, A.; Beyne-Rauzy, O.; Prebet, T.; Park, S.; Stamatoullas, A.; Guerci-Bresler, A.; Cheze, S.; et al. A randomized phase II trial of azacitidine +/- epoetin-beta in lower-risk myelodysplastic syndromes resistant to erythropoietic stimulating agents. Haematologica 2016, 101, 918–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jabbour, E.; Short, N.J.; Montalban-Bravo, G.; Huang, X.; Bueso-Ramos, C.; Qiao, W.; Yang, H.; Zhao, C.; Kadia, T.; Borthakur, G.; et al. Randomized phase 2 study of low-dose decitabine vs low-dose azacitidine in lower-risk MDS and MDS/MPN. Blood 2017, 130, 1514–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, E.S.; Lyons, R.M.; Larson, R.A.; Gandhi, S.; Liu, D.; Matei, C.; Scott, B.; Hu, K.; Yang, A.S. A randomized, double-blind, placebo-controlled phase 2 study evaluating the efficacy and safety of romiplostim treatment of patients with low or intermediate-1 risk myelodysplastic syndrome receiving lenalidomide. J. Hematol. Oncol. 2012, 5, 71. [Google Scholar] [CrossRef] [Green Version]
- Fenaux, P.; Muus, P.; Kantarjian, H.; Lyons, R.M.; Larson, R.A.; Sekeres, M.A.; Becker, P.S.; Orejudos, A.; Franklin, J. Romiplostim monotherapy in thrombocytopenic patients with myelodysplastic syndromes: Long-term safety and efficacy. Br. J. Haematol. 2017, 178, 906–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantarjian, H.M.; Fenaux, P.; Sekeres, M.A.; Szer, J.; Platzbecker, U.; Kuendgen, A.; Gaidano, G.; Wiktor-Jedrzejczak, W.; Carpenter, N.; Mehta, B.; et al. Long-term follow-up for up to 5 years on the risk of leukaemic progression in thrombocytopenic patients with lower-risk myelodysplastic syndromes treated with romiplostim or placebo in a randomised double-blind trial. Lancet Haematol 2018, 5, e117–e126. [Google Scholar] [CrossRef]
- de Witte, T.; Bowen, D.; Robin, M.; Malcovati, L.; Niederwieser, D.; Yakoub-Agha, I.; Mufti, G.J.; Fenaux, P.; Sanz, G.; Martino, R.; et al. Allogeneic hematopoietic stem cell transplantation for MDS and CMML: Recommendations from an international expert panel. Blood 2017, 129, 1753–1762. [Google Scholar] [CrossRef] [PubMed]
- Schetelig, J.; de Wreede, L.C.; van Gelder, M.; Koster, L.; Finke, J.; Niederwieser, D.; Beelen, D.; Mufti, G.J.; Platzbecker, U.; Ganser, A.; et al. Late treatment-related mortality versus competing causes of death after allogeneic transplantation for myelodysplastic syndromes and secondary acute myeloid leukemia. Leukemia 2019, 33, 686–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidenreich, S.; Ziagkos, D.; de Wreede, L.C.; van Biezen, A.; Finke, J.; Platzbecker, U.; Niederwieser, D.; Einsele, H.; Bethge, W.; Schleuning, M.; et al. Allogeneic Stem Cell Transplantation for Patients Age >/= 70 Years with Myelodysplastic Syndrome: A Retrospective Study of the MDS Subcommittee of the Chronic Malignancies Working Party of the EBMT. Biol. Blood Marrow Transplant. 2017, 23, 44–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damaj, G.; Duhamel, A.; Robin, M.; Beguin, Y.; Michallet, M.; Mohty, M.; Vigouroux, S.; Bories, P.; Garnier, A.; Cheikh, J.E.; et al. Impact of Azacitidine before Allogeneic Stem-Cell Transplantation for Myelodysplastic Syndromes: A Study by the Société Française de Greffe de Moelle et de Thérapie-Cellulaire and the Groupe-Francophone des Myélodysplasies. J. Clin. Oncol. 2012, 30, 4533–4540. [Google Scholar] [CrossRef] [PubMed]
- Prébet, T.; Gore, S.D.; Esterni, B.; Gardin, C.; Itzykson, R.; Thepot, S.; Dreyfus, F.; Rauzy, O.B.; Recher, C.; Adès, L.; et al. Outcome of high-risk myelodysplastic syndrome after azacitidine treatment failure. J. Clin. Oncol. 2011, 29, 3322–3327. [Google Scholar] [CrossRef]
- Lindsley, R.C.; Saber, W.; Mar, B.G.; Redd, R.; Wang, T.; Haagenson, M.D.; Grauman, P.V.; Hu, Z.H.; Spellman, S.R.; Lee, S.J.; et al. Prognostic Mutations in Myelodysplastic Syndrome after Stem-Cell Transplantation. N. Engl. J. Med. 2017, 376, 536–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshizato, T.; Nannya, Y.; Atsuta, Y.; Shiozawa, Y.; Iijima-Yamashita, Y.; Yoshida, K.; Shiraishi, Y.; Suzuki, H.; Nagata, Y.; Sato, Y.; et al. Genetic abnormalities in myelodysplasia and secondary acute myeloid leukemia: Impact on outcome of stem cell transplantation. Blood 2017, 129, 2347–2358. [Google Scholar] [CrossRef]
- Fenaux, P.; Mufti, G.J.; Hellstrom-Lindberg, E.; Santini, V.; Finelli, C.; Giagounidis, A.; Schoch, R.; Gattermann, N.; Sanz, G.; List, A.; et al. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: A randomised, open-label, phase III study. Lancet Oncol. 2009, 10, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Sekeres, M.A.; Othus, M.; List, A.F.; Odenike, O.; Stone, R.M.; Gore, S.D.; Litzow, M.R.; Buckstein, R.; Fang, M.; Roulston, D.; et al. Randomized Phase II Study of Azacitidine Alone or in Combination with Lenalidomide or with Vorinostat in Higher-Risk Myelodysplastic Syndromes and Chronic Myelomonocytic Leukemia: North American Intergroup Study SWOG S1117. J. Clin. Oncol. 2017, 35, 2745–2753. [Google Scholar] [CrossRef]
- Bernal, T.; Martinez-Camblor, P.; Sanchez-Garcia, J.; de Paz, R.; Luno, E.; Nomdedeu, B.; Ardanaz, M.T.; Pedro, C.; Amigo, M.L.; Xicoy, B.; et al. Effectiveness of azacitidine in unselected high-risk myelodysplastic syndromes: Results from the Spanish registry. Leukemia 2015, 29, 1875–1881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeidan, A.M.; Hu, X.; Zhu, W.; Stahl, M.; Wang, R.; Huntington, S.F.; Giri, S.; Bewersdorf, J.P.; Podoltsev, N.A.; Gore, S.D.; et al. Association of provider experience and clinical outcomes in patients with myelodysplastic syndromes receiving hypomethylating agents. Leuk. Lymphoma 2020, 61, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Itzykson, R.; Kosmider, O.; Cluzeau, T.; Mansat-De Mas, V.; Dreyfus, F.; Beyne-Rauzy, O.; Quesnel, B.; Vey, N.; Gelsi-Boyer, V.; Raynaud, S.; et al. Impact of TET2 mutations on response rate to azacitidine in myelodysplastic syndromes and low blast count acute myeloid leukemias. Leukemia 2011, 25, 1147–1152. [Google Scholar] [CrossRef] [Green Version]
- Itzykson, R.; Thépot, S.; Quesnel, B.; Dreyfus, F.; Beyne-Rauzy, O.; Turlure, P.; Vey, N.; Recher, C.; Dartigeas, C.; Legros, L.; et al. Prognostic factors for response and overall survival in 282 patients with higher-risk myelodysplastic syndromes treated with azacitidine. Blood 2011, 117, 403–411. [Google Scholar] [CrossRef] [Green Version]
- Kantarjian, H.; Issa, J.P.; Rosenfeld, C.S.; Bennett, J.M.; Albitar, M.; DiPersio, J.; Klimek, V.; Slack, J.; de Castro, C.; Ravandi, F.; et al. Decitabine improves patient outcomes in myelodysplastic syndromes: Results of a phase III randomized study. Cancer 2006, 106, 1794–1803. [Google Scholar] [CrossRef] [PubMed]
- Lubbert, M.; Suciu, S.; Baila, L.; Ruter, B.H.; Platzbecker, U.; Giagounidis, A.; Selleslag, D.; Labar, B.; Germing, U.; Salih, H.R.; et al. Low-dose decitabine versus best supportive care in elderly patients with intermediate- or high-risk myelodysplastic syndrome (MDS) ineligible for intensive chemotherapy: Final results of the randomized phase III study of the European Organisation for Research and Treatment of Cancer Leukemia Group and the German MDS Study Group. J. Clin. Oncol. 2011, 29, 1987–1996. [Google Scholar] [CrossRef] [PubMed]
- Silverman, L.R.; Fenaux, P.; Mufti, G.J.; Santini, V.; Hellstrom-Lindberg, E.; Gattermann, N.; Sanz, G.; List, A.F.; Gore, S.D.; Seymour, J.F. Continued azacitidine therapy beyond time of first response improves quality of response in patients with higher-risk myelodysplastic syndromes. Cancer 2011, 117, 2697–2702. [Google Scholar] [CrossRef] [Green Version]
- Voso, M.T.; Breccia, M.; Lunghi, M.; Poloni, A.; Niscola, P.; Finelli, C.; Bari, A.; Musto, P.; Zambello, R.; Fianchi, L.; et al. Rapid loss of response after withdrawal of treatment with azacitidine: A case series in patients with higher-risk myelodysplastic syndromes or chronic myelomonocytic leukemia. Eur. J. Haematol. 2013, 90, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Manero, G.; Roboz, G.; Walsh, K.; Kantarjian, H.; Ritchie, E.; Kropf, P.; O’Connell, C.; Tibes, R.; Lunin, S.; Rosenblat, T.; et al. Guadecitabine (SGI-110) in patients with intermediate or high-risk myelodysplastic syndromes: Phase 2 results from a multicentre, open-label, randomised, phase 1/2 trial. Lancet Haematol. 2019, 6, e317–e327. [Google Scholar] [CrossRef]
- Buckland, M. Astex and Otsuka Announce Results of Phase 3 ASTRAL-2 and ASTRAL-3 Studies of Guadecitabine (SGI-110) in Patients with Previously Treated Acute Myeloid Leukemia (AML) and Myelodysplastic Syndromes or Chronic Myelomonocytic Leukemia (MDS/CMML). Available online: https://www.businesswire.com/news/home/20201014005914/en/Astex-and-Otsuka-Announce-Results-of-Phase-3-ASTRAL-2-and-ASTRAL-3-Studies-of-Guadecitabine-SGI-110-in-Patients-with-Previously-Treated-Acute-Myeloid-Leukemia-AML-and-Myelodysplastic-Syndromes-or-Chronic-Myelomonocytic-Leukemia-MDSCMML (accessed on 12 December 2020).
- Garcia-Manero, G.; Griffiths, E.A.; Steensma, D.P.; Roboz, G.J.; Wells, R.; McCloskey, J.; Odenike, O.; DeZern, A.E.; Yee, K.; Busque, L.; et al. Oral cedazuridine/decitabine for MDS and CMML: A phase 2 pharmacokinetic/pharmacodynamic randomized crossover study. Blood 2020, 136, 674–683. [Google Scholar] [CrossRef]
- Wei, A.H.; Döhner, H.; Pocock, C.; Montesinos, P.; Afanasyev, B.; Dombret, H.; Ravandi, F.; Sayar, H.; Jang, J.-H.; Porkka, K.; et al. Oral Azacitidine Maintenance Therapy for Acute Myeloid Leukemia in First Remission. N. Engl. J. Med. 2020, 383, 2526–2537. [Google Scholar] [CrossRef]
- Savona, M.R.; Kolibaba, K.; Conkling, P.; Kingsley, E.C.; Becerra, C.; Morris, J.C.; Rifkin, R.M.; Laille, E.; Kellerman, A.; Ukrainskyj, S.M.; et al. Extended dosing with CC-486 (oral azacitidine) in patients with myeloid malignancies. Am. J. Hematol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Manero, G.; Gore, S.D.; Kambhampati, S.; Scott, B.; Tefferi, A.; Cogle, C.R.; Edenfield, W.J.; Hetzer, J.; Kumar, K.; Laille, E.; et al. Efficacy and safety of extended dosing schedules of CC-486 (oral azacitidine) in patients with lower-risk myelodysplastic syndromes. Leukemia 2016, 30, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Manero, G.; Scott, B.L.; Cogle, C.R.; Boyd, T.E.; Kambhampati, S.; Hetzer, J.; Dong, Q.; Kumar, K.; Ukrainskyj, S.M.; Beach, C.L.; et al. CC-486 (oral azacitidine) in patients with myelodysplastic syndromes with pretreatment thrombocytopenia. Leuk. Res. 2018, 72, 79–85. [Google Scholar] [CrossRef]
- Prebet, T.; Sun, Z.; Figueroa, M.E.; Ketterling, R.; Melnick, A.; Greenberg, P.L.; Herman, J.; Juckett, M.; Smith, M.R.; Malick, L.; et al. Prolonged administration of azacitidine with or without entinostat for myelodysplastic syndrome and acute myeloid leukemia with myelodysplasia-related changes: Results of the US Leukemia Intergroup trial E1905. J. Clin. Oncol. 2014, 32, 1242–1248. [Google Scholar] [CrossRef] [Green Version]
- DiNardo, C.D.; Jonas, B.A.; Pullarkat, V.; Thirman, M.J.; Garcia, J.S.; Wei, A.H.; Konopleva, M.; Döhner, H.; Letai, A.; Fenaux, P.; et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N. Engl. J. Med. 2020, 383, 617–629. [Google Scholar] [CrossRef]
- Wei, A.H.; Montesinos, P.; Ivanov, V.; DiNardo, C.D.; Novak, J.; Laribi, K.; Kim, I.; Stevens, D.; Fiedler, W.; Pagoni, M.; et al. Venetoclax plus LDAC for patients with untreated AML ineligible for intensive chemotherapy: Phase 3 randomized placebo-controlled trial. Blood 2020. [Google Scholar] [CrossRef]
- Garcia, J.S.; Wei, A.H.; Borate, U.; Fong, C.Y.; Baer, M.R.; Nolte, F.; Jurcic, J.G.; Jacoby, M.A.; Hong, W.-J.; Platzbecker, U.; et al. Safety, Efficacy, and Patient-Reported Outcomes of Venetoclax in Combination with Azacitidine for the Treatment of Patients with Higher-Risk Myelodysplastic Syndrome: A Phase 1b Study. Blood 2020, 136, 55–57. [Google Scholar] [CrossRef]
- Zeidan, A.M.; Pollyea, D.A.; Garcia, J.S.; Brunner, A.; Roncolato, F.; Borate, U.; Odenike, O.; Bajel, A.R.; Watson, A.M.; Götze, K.; et al. A Phase 1b Study Evaluating the Safety and Efficacy of Venetoclax in Combination with Azacitidine for the Treatment of Relapsed/Refractory Myelodysplastic Syndrome. Blood 2019, 134. [Google Scholar] [CrossRef]
- Zeidan, A.M.; Cavenagh, J.; Voso, M.T.; Taussig, D.; Tormo, M.; Boss, I.; Copeland, W.B.; Gray, V.E.; Previtali, A.; O’Connor, T.; et al. Efficacy and Safety of Azacitidine (AZA) in Combination with the Anti-PD-L1 Durvalumab (durva) for the Front-Line Treatment of Older Patients (pts) with Acute Myeloid Leukemia (AML) Who Are Unfit for Intensive Chemotherapy (IC) and Pts with Higher-Risk Myelodysplastic Syndromes (HR-MDS): Results from a Large, International, Randomized Phase 2 Study. Blood 2019, 134, 829. [Google Scholar] [CrossRef]
- Sallman, D.A. Tolerability and efficacy of the first-in-class anti-CD47 antibody magrolimab combined with azacitidine in MDS and AML patients: Phase Ib results. J. Clin. Oncol. 2020, 38, 7507. [Google Scholar] [CrossRef]
- Brunner, A.M.; Esteve, J.; Porkka, K.; Knapper, S.; Vey, N.; Scholl, S.; Garcia-Manero, G.; Wermke, M.; Janssen, J.; Traer, E.; et al. Efficacy and Safety of Sabatolimab (MBG453) in Combination with Hypomethylating Agents (HMAs) in Patients with Acute Myeloid Leukemia (AML) and High-Risk Myelodysplastic Syndrome (HR-MDS): Updated Results from a Phase 1b Study. Blood 2020, 136, 1–2. [Google Scholar] [CrossRef]
- Zeidan, A.M.; Knaus, H.A.; Robinson, T.M.; Towlerton, A.M.H.; Warren, E.H.; Zeidner, J.F.; Blackford, A.L.; Duffield, A.S.; Rizzieri, D.; Frattini, M.G.; et al. A Multi-center Phase I Trial of Ipilimumab in Patients with Myelodysplastic Syndromes following Hypomethylating Agent Failure. Clin. Cancer Res. 2018, 24, 3519–3527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekeres, M.A.; Watts, J.M.; Radinoff, A.; Sangerman, M.A.; Cerrano, M.; Lopez, P.F.; Zeidner, J.F.; Diez-Campelo, M.; Graux, C.; Liesveld, J.L.; et al. Efficacy and Safety of Pevonedistat Plus Azacitidine vs Azacitidine Alone in Higher-Risk Myelodysplastic Syndromes (MDS) from Study P-2001. Blood 2020, 136. Available online: https://ash.confex.com/ash/2020/webprogram/Paper135840.html (accessed on 12 December 2020).
- Ball, B.; Komrokji, R.S.; Ades, L.; Sekeres, M.A.; DeZern, A.E.; Pleyer, L.; Vey, N.; Almeida, A.; Germing, U.; Cluzeau, T.; et al. Evaluation of induction chemotherapies after hypomethylating agent failure in myelodysplastic syndromes and acute myeloid leukemia. Blood Adv. 2018, 2, 2063–2071. [Google Scholar] [CrossRef]
- Welch, J.S.; Petti, A.A.; Miller, C.A.; Fronick, C.C.; O’Laughlin, M.; Fulton, R.S.; Wilson, R.K.; Baty, J.D.; Duncavage, E.J.; Tandon, B.; et al. TP53 and Decitabine in Acute Myeloid Leukemia and Myelodysplastic Syndromes. N. Engl. J. Med. 2016, 375, 2023–2036. [Google Scholar] [CrossRef]
- Kantarjian, H.; Beran, M.; Cortes, J.; O’Brien, S.; Giles, F.; Pierce, S.; Shan, J.; Plunkett, W.; Keating, M.; Estey, E. Long-term follow-up results of the combination of topotecan and cytarabine and other intensive chemotherapy regimens in myelodysplastic syndrome. Cancer 2006, 106, 1099–1109. [Google Scholar] [CrossRef]
- Lancet, J.E.; Uy, G.L.; Cortes, J.E.; Newell, L.F.; Lin, T.L.; Ritchie, E.K.; Stuart, R.K.; Strickland, S.A.; Hogge, D.; Solomon, S.R.; et al. CPX-351 (cytarabine and daunorubicin) Liposome for Injection Versus Conventional Cytarabine Plus Daunorubicin in Older Patients with Newly Diagnosed Secondary Acute Myeloid Leukemia. J. Clin. Oncol. 2018, 36, 2684–2692. [Google Scholar] [CrossRef]
- Silverman, L.R.; McKenzie, D.R.; Peterson, B.L.; Holland, J.F.; Backstrom, J.T.; Beach, C.L.; Larson, R.A. Further analysis of trials with azacitidine in patients with myelodysplastic syndrome: Studies 8421, 8921, and 9221 by the Cancer and Leukemia Group B. J. Clin. Oncol. 2006, 24, 3895–3903. [Google Scholar] [CrossRef] [Green Version]
- Santini, V.; Allione, B.; Zini, G.; Gioia, D.; Lunghi, M.; Poloni, A.; Cilloni, D.; Sanna, A.; Masiera, E.; Ceccarelli, M.; et al. A phase II, multicentre trial of decitabine in higher-risk chronic myelomonocytic leukemia. Leukemia 2018, 32, 413–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfonso, A.; Montalban-Bravo, G.; Takahashi, K.; Jabbour, E.J.; Kadia, T.; Ravandi, F.; Cortes, J.; Estrov, Z.; Borthakur, G.; Pemmaraju, N.; et al. Natural history of chronic myelomonocytic leukemia treated with hypomethylating agents. Am. J. Hematol. 2017, 92, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Pleyer, L.; Leisch, M.; Kourakli, A.; Padron, E.; Maciejewski, J.P.; Xicoy Cirici, B.; Kaivers, J.; Ungerstedt, J.; Heibl, S.; Patiou, P.; et al. Outcomes of patients with chronic myelomonocytic leukaemia treated with non-curative therapies: A retrospective cohort study. Lancet Haematol 2021, 8, e135–e148. [Google Scholar] [CrossRef]
- Zeidan, A.M.; Hu, X.; Long, J.B.; Wang, R.; Ma, X.; Podoltsev, N.A.; Huntington, S.F.; Gore, S.D.; Davidoff, A.J. Hypomethylating agent therapy use and survival in older patients with chronic myelomonocytic leukemia in the United States: A large population-based study. Cancer 2017, 123, 3754–3762. [Google Scholar] [CrossRef]
- Wijermans, P.W.; Rüter, B.; Baer, M.R.; Slack, J.L.; Saba, H.I.; Lübbert, M. Efficacy of decitabine in the treatment of patients with chronic myelomonocytic leukemia (CMML). Leuk. Res. 2008, 32, 587–591. [Google Scholar] [CrossRef]
- Braun, T.; Itzykson, R.; Renneville, A.; de Renzis, B.; Dreyfus, F.; Laribi, K.; Bouabdallah, K.; Vey, N.; Toma, A.; Recher, C.; et al. Molecular predictors of response to decitabine in advanced chronic myelomonocytic leukemia: A phase 2 trial. Blood 2011, 118, 3824–3831. [Google Scholar] [CrossRef] [Green Version]
- Duchmann, M.; Yalniz, F.F.; Sanna, A.; Sallman, D.; Coombs, C.C.; Renneville, A.; Kosmider, O.; Braun, T.; Platzbecker, U.; Willems, L.; et al. Prognostic Role of Gene Mutations in Chronic Myelomonocytic Leukemia Patients Treated with Hypomethylating Agents. EBioMedicine 2018, 31, 174–181. [Google Scholar] [CrossRef] [Green Version]
- Coston, T.; Pophali, P.; Vallapureddy, R.; Lasho, T.L.; Finke, C.M.; Ketterling, R.P.; Carr, R.; Binder, M.; Mangaonkar, A.A.; Gangat, N.; et al. Suboptimal response rates to hypomethylating agent therapy in chronic myelomonocytic leukemia; a single institutional study of 121 patients. Am. J. Hematol. 2019, 94, 767–779. [Google Scholar] [CrossRef]
- Liu, H.D.; Ahn, K.W.; Hu, Z.H.; Hamadani, M.; Nishihori, T.; Wirk, B.; Beitinjaneh, A.; Rizzieri, D.; Grunwald, M.R.; Sabloff, M.; et al. Allogeneic Hematopoietic Cell Transplantation for Adult Chronic Myelomonocytic Leukemia. Biol. Blood Marrow Transplant. 2017, 23, 767–775. [Google Scholar] [CrossRef] [Green Version]
- Gagelmann, N.; Bogdanov, R.; Stölzel, F.; Rautenberg, C.; Panagiota, V.; Becker, H.; Radujkovic, A.; Luft, T.; Christopeit, M.; Finke, J.; et al. Long-Term Survival Benefit after Allogeneic Hematopoietic Cell Transplantation for Chronic Myelomonocytic Leukemia. Transplant. Cell. Ther. 2021, 27, 95–e1. [Google Scholar] [CrossRef]
- Pophali, P.; Matin, A.; Mangaonkar, A.A.; Carr, R.; Binder, M.; Al-Kali, A.; Begna, K.H.; Reichard, K.K.; Alkhateeb, H.; Shah, M.V.; et al. Prognostic impact and timing considerations for allogeneic hematopoietic stem cell transplantation in chronic myelomonocytic leukemia. Blood Cancer J. 2020, 10, 121. [Google Scholar] [CrossRef]
- Platzbecker, U.; Fenaux, P.; Steensma, D.P.; Van Eygen, K.; Raza, A.; Germing, U.; Font, P.; Diez-Campelo, M.; Thepot, S.; Vellenga, E.; et al. Imerge: A Phase 3 Study to Evaluate Imetelstat in Transfusion-Dependent Subjects with IPSS Low or Intermediate-1 Risk Myelodysplastic Syndromes (MDS) That Is Relapsed/Refractory to Erythropoiesis-Stimulating Agent (ESA) Treatment. Blood 2020, 136, 17. [Google Scholar] [CrossRef]
- Chen, N.; Hao, C.; Liu, B.C.; Lin, H.; Wang, C.; Xing, C.; Liang, X.; Jiang, G.; Liu, Z.; Li, X.; et al. Roxadustat Treatment for Anemia in Patients Undergoing Long-Term Dialysis. N. Engl. J. Med. 2019, 381, 1011–1022. [Google Scholar] [CrossRef]
- Henry, D.H.; Glaspy, J.; Harrup, R.A.; Mittelman, M.; Zhou, A.; Carraway, H.E.; Bradley, C.; Saha, G.; Bartels, P.; Leong, R.; et al. Oral Roxadustat Demonstrates Efficacy in Anemia Secondary to Lower-Risk Myelodysplastic Syndrome Irrespective of Ring Sideroblasts and Baseline Erythropoietin Levels. Blood 2020, 136, 29–30. [Google Scholar] [CrossRef]
- Sallman, D.A.; DeZern, A.E.; Garcia-Manero, G.; Steensma, D.P.; Roboz, G.J.; Sekeres, M.A.; Cluzeau, T.; Sweet, K.L.; McLemore, A.; McGraw, K.L.; et al. Eprenetapopt (APR-246) and Azacitidine in TP53-Mutant Myelodysplastic Syndromes. J. Clin. Oncol. 2021, JCO2002341. [Google Scholar] [CrossRef]
- Cluzeau, T.; Sebert, M.; Rahmé, R.; Cuzzubbo, S.; Lehmann-Che, J.; Madelaine, I.; Peterlin, P.; Bève, B.; Attalah, H.; Chermat, F.; et al. Eprenetapopt Plus Azacitidine in TP53-Mutated Myelodysplastic Syndromes and Acute Myeloid Leukemia: A Phase II Study by the Groupe Francophone des Myélodysplasies (GFM). J. Clin. Oncol. 2021, 20, JCO2002342. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, A.M.; Esteve, J.; Giagounidis, A.; Kim, H.-J.; Miyazaki, Y.; Platzbecker, U.; Schuh, A.C.; Sekeres, M.A.; Westermann, J.; Xiao, Z.; et al. The STIMULUS Program: Clinical Trials Evaluating Sabatolimab (MBG453) Combination Therapy in Patients (Pts) with Higher-Risk Myelodysplastic Syndromes (HR-MDS) or Acute Myeloid Leukemia (AML). Blood 2020, 136, 45–46. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Watts, J.M.; Stein, E.M.; de Botton, S.; Fathi, A.T.; Prince, G.T.; Stein, A.S.; Foran, J.M.; Stone, R.M.; Patel, P.A.; et al. Ivosidenib (AG-120) Induced Durable Remissions and Transfusion Independence in Patients with IDH1-Mutant Relapsed or Refractory Myelodysplastic Syndrome: Results from a Phase 1 Dose Escalation and Expansion Study. Blood 2018, 132, 1812. [Google Scholar] [CrossRef]
- Patnaik, M.M.; Sallman, D.A.; Sekeres, M.A.; Luger, S.; Bejar, R.; Hobbs, G.S.; DeZern, A.E.; Bolognese, J.; Traynor, M.; Mishra, V.; et al. Preliminary Results from an Open-Label, Phase 2 Study of Tipifarnib in Chronic Myelomonocytic Leukemia (CMML). Blood 2017, 130, 2963. [Google Scholar] [CrossRef]
- Patnaik, M.M.; Ali, H.; Gupta, V.; Schiller, G.J.; Lee, S.; Yacoub, A.; Talpaz, M.; Sardone, M.; Wysowskyj, H.; Shemesh, S.; et al. Results from Ongoing Phase 1/2 Clinical Trial of Tagraxofusp (SL-401) in Patients with Relapsed/Refractory Chronic Myelomonocytic Leukemia (CMML). Blood 2018, 132, 1821. [Google Scholar] [CrossRef]
- Patnaik, M.M.; Sallman, D.A.; Mangaonkar, A.A.; Heuer, R.; Hirvela, J.; Zblewski, D.; Al-Kali, A.; Binder, M.; Balasis, M.E.; Newman, H.; et al. Phase 1 study of lenzilumab, a recombinant anti–human GM-CSF antibody, for chronic myelomonocytic leukemia. Blood 2020, 136, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Greenberg, P.L.; Bennett, J.M.; Lowenberg, B.; Wijermans, P.W.; Nimer, S.D.; Pinto, A.; Beran, M.; de Witte, T.M.; Stone, R.M.; et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood 2006, 108, 419–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platzbecker, U.; Fenaux, P.; Adès, L.; Giagounidis, A.; Santini, V.; van de Loosdrecht, A.A.; Bowen, D.; de Witte, T.; Garcia-Manero, G.; Hellström-Lindberg, E.; et al. Proposals for revised IWG 2018 hematological response criteria in patients with MDS included in clinical trials. Blood 2019, 133, 1020–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komrokji, R.S.; Al Ali, N.H.; Sallman, D.; Padron, E.; DeZern, A.E.; Barnard, J.; Roboz, G.J.; Garcia-Manero, G.; List, A.; Steensma, D.P.; et al. Validation of International Working Group response criteria in higher-risk myelodysplastic syndromes: A report on behalf of the MDS Clinical Research Consortium. Cancer Med. 2021, 10, 447–453. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | Phase | NCT | Patient Characteristics | Intervention |
|---|---|---|---|---|
| Hypomethylating Agents | ||||
| Decitabine | III | NCT02214407 (GFM-DAC-CMML) | CMML | DEC + hydroxyurea vs. hydroxyurea alone |
| Azacitidine | II | NCT01522976 | HR-MDS or CMML | AZA +/− lenalidomide or vorinostat |
| I/II | NCT00392353 | HR-MDS, CMML or AML | AZA + vorinostat | |
| Guadecitabine | I/II | NCT02935361 | R/R MDS or CMML | Guadecitabine + atezolizumab |
| III | NCT02907359 (ASTRAL-3 trial) | HMA-refractory MDS or CMML | Guadecitabine vs. treatment choice (low-dose cytarabine, BSC, 7 + 3) | |
| CC-486 | II | NCT02281084 | HMA-refractory MDS | CC-486 + durvalumab vs. CC-486 alone |
| III | NCT01566695 | Transfusion-dependent LR-MDS | CC-486 vs. placebo | |
| III | NCT04173533 (AMADEUS trial) | AML and MDS post-HSCT maintenance therapy | CC-486 vs. placebo | |
| ASTX030 | II/III | NCT04256317 | MDS, CMML, MDS/MPN, or AML who are candidates for AZA monotherapy | Phase 2: randomized open-label crossover study oral ASTX030 vs. subcutaneous AZA Phase 3: randomized open-label crossover study of final oral ASTX030 tablet vs. subcutaneous AZA |
| ASTX727 | III | NCT03306264 | HR-MDS, CMLL, or AML | ASTX727 vs. IV DEC |
| I/II | NCT04061421 | MDS/MPN overlap except JMML | ASTX727 + INCB053914, itacitinib, or INCB059872 | |
| I/II | NCT03502668 | RBC-TD LR-MDS | Low-dose vs. standard-dose ASTX727 | |
| II | NCT04655755 | Newly diagnosed HR-MDS or CMML | ASTX727 + venetoclax | |
| II | NCT04093570 | Any prior enrollment in ASTX727 trials | ASTX727 | |
| Molecularly Targeted Agents | ||||
| APR-246 (p53-refolding agent) | III | NCT03745716 | TP53-mutant MDS | APR-246 + AZA vs. AZA alone |
| II | NCT03931291 | TP53-mutant MDS or AML following allo-HCT | APR-246 | |
| I/II | NCT03072043 | TP53-mutant MDS, CMML or AML | APR-246 + AZA | |
| I/II | NCT03588078 | TP53-mutant MDS, CMML or AML | APR-246 + AZA | |
| Quizartinib (FLT3 inhibitor) | I/II | NCT01892371 | R/R AML, MDS, CMML | Quizartinib + AZA |
| I/II | NCT04493138 | Untreated or HMA-refractory MDS, MDS/MPN with FLT3 or CBL mutations | Quizartinib + AZA | |
| II | NCT04047641 | Untreated or R/R AML or HR-MDS with FLT3 mutations | Cladribine + idarubicin + cytarabine + quizartinib | |
| Gilteritinib (FLT3 inhibitor) | III | NCT04027309 (HOVON 156 AML) | Untreated AML or HR-MDS with FLT3 mutations | Gilteritinib + induction chemotherapy vs. midostaurin + induction chemotherapy |
| Ivosidenib (IDH1 inhibitor) | II | NCT03503409 | IDH1 Mutated, HMA-refractory MDS | Ivosidenib |
| II | NCT03471260 | IDH1 Mutated MDS, MPN, AML | Ivosidenib + venetoclax +/− AZA | |
| III | NCT03839771 (HOVON150AML) | IDH1 Mutated newly diagnosed and R/R-AML and HR-MDS | Ivosidenib or placebo in combination with induction and consolidation therapy | |
| Enasidenib (IDH2 inhibitor) | II | NCT03744390 | IDH2 Mutated MDS | Enasidenib |
| II | NCT03383575 | IDH2 Mutated, HMA-naïve and HMA-refractory MDS | Enasidenib + AZA or enasidenib alone in HMA-refractory patients | |
| III | NCT03839771 (HOVON150AML) | IDH2 Mutated newly diagnosed and R/R-AML and HR-MDS | Ivosidenib or placebo in combination with induction and consolidation therapy | |
| II | NCT01915498 | IDH2 Mutated R/R-AML and HR-MDS | Enasidenib | |
| FT-2102 (IDH1 inhibitor) | II | NCT02719574 | IDH1 Mutated R/R-AML and HR-MDS | FT-2102 alone or in combination with AZA or cytarabine |
| Immune Checkpoint Inhibitors/Cellular Immunotherapy/Monoclonal Antibodies | ||||
| MBG453 (anti-TIM3) | II | NCT03946670 | HMA-naïve, HR-MDS | MBG453 + HMA vs. placebo + HMA |
| III | NCT04266301 (STIMULUS-MDS2) | HMA-naïve, HR-MDS | MBG453 + AZA vs. placebo + AZA | |
| Nivolumab (anti-PD1) | I/II | NCT02530463 | Untreated or HMA-refractory MDS | Nivolumab +/− ipilimumab +/− AZA |
| II/III | NCT03092674 | Untreated AML or HR-MDS | AZA +/− nivolumab or midostaurin vs. DEC/cytarabine | |
| Durvalumab (anti-PD-L1) | II | NCT02775903 | Untreated HR-MDS or AML ≥65 years old and not eligible for allo-HCT | Durvalumab + AZA vs. AZA alone |
| Pembrolizumab (anti- PD1) | II | NCT03094637 | Untreated or HMA-refractory MDS | Pembrolizumab + AZA |
| Ipilimumab (anti-CTLA4) | Ib/II | NCT02890329 | R/R-AML and MDS | Ipilimumab + DEC |
| Magrolimab (anti-CD47) | III | NCT04313881 (ENHANCE) | Untreated HR-MDS | Magrolimab + AZA vs. placebo + AZA |
| ALX148 (anti-CD47) | I/II | NCT04417517 (ASPEN-02) | HR-MDS | ALX148 + AZA |
| TJ011133 (anti-CD47) | II | NCT04202003 | R/R-AML or MDS | TJ011133 |
| Cusatuzumab (anti-CD27/70) | II | NCT04264806 | HR-MDS and CMML | Cusatuzumab + AZA vs. AZA alone |
| II | NCT03030612 | Newly-diagnosed AML or HR-MDS ineligible for chemotherapy | Cusatuzumab + AZA | |
| BLEX 404 (immune stimulant) | II | NCT02944955 | Intermediate-1, Intermediate-2 or High-Risk MDS and CMML | BLEX404 + AZA |
| Talacotuzumab (JNJ-56022473; anti-CD123) or Daratumumab (anti-CD38) | II | NCT03011034 | RBC-TD LR-MDS | Talacotuzumab (JNJ-56022473) or Daratumumab |
| Daratumumab (anti-CD38) | II | NCT03067571 | R/R-AML or HR-MDS | Daratumumab |
| ADCT-301 (anti-CD25 antibody drug conjugate) | II | NCT04639024 | R/R-AML, MDS, or MDS/MPN | ADCT-301 |
| ASP7517 (tumor vaccine) | II | NCT04079296 | R/R-AML or MDS | ASP7517 |
| Canakinumab (anti-IL-1β) | II | NCT04239157 | ESA or HMA-refractory LR-MDS or CMML | Canakinumab |
| SAR440234 (CD3-CD123 T-cell engaging bispecific monoclonal antibody) | II | NCT03594955 | R/R AML, ALL or HR-MDS | SAR440234 |
| Conventional Cytotoxic Chemotherapy | ||||
| CPX-351 (liposomal cytarabine + daunorubicin) | I/II | NCT04109690 | HMA-refractory MDS | CPX-351 |
| II | NCT03957876 | HMA-refractory MDS | CPX-351 | |
| I/II | NCT04273802 | Untreated or HMA-refractory MDS | CPX-351 | |
| I/II | NCT04128748 | Frontline and R/R AML and MDS | CPX-351 + quizartinib | |
| II | NCT04668885 | R/R AML and MDS | CPX-351 | |
| II | NCT04493164 | Frontline and R/R AML and MDS with IDH1 mutation | CPX-351 + ivosidenib | |
| II | NCT03672539 | R/R AML or HR-MDS | CPX-351 + gemtuzumab ozogamicin | |
| BST-236 (cytarabine prodrug) | II | NCT04749355 | R/R-AML or HMA-failure, HR-MDS; MDS/MPN overlap excluded | BST-236 |
| Small Molecule Inhibitors and Miscellaneous Agents | ||||
| Pevonedistat (NEDD8 inhibitor) | II | NCT03238248 | HMA-refractory MDS or MDS/MPN | Pevonedistat + AZA |
| III | NCT03268954 (PANTHER) | Newly-diagnosed HR-MDS, CMML or AML <30% blasts | Pevonedistat + AZA vs. AZA alone | |
| II | NCT03238248 | HMA-refractory MDS or MDS/MPN | Pevonedistat + AZA | |
| Venetoclax (BCL2 inhibitor) | II | NCT04146038 | R/R-AML or MDS | Salsalate + DEC/AZA + venetoclax |
| I/II | NCT03661307 | Frontline and R/R, AML and MDS | DEC + venetoclax + quizartinib | |
| I/II | NCT04140487 | R/R, FLT3-mutated AML and MDS | Venetoclax + AZA + gilteritinib | |
| II | NCT04487106 | R/R, RAS pathway-mutated AML and MDS | Venetoclax + AZA + trametinib | |
| I/II | NCT03218683 | R/R AML or MDS | AZD5991 +/− venetoclax | |
| II | NCT03404193 | R/R AML and MDS | Venetoclax + DEC | |
| I/II | NCT04550442 | HMA-refractory MDS and CMML | Venetoclax + AZA | |
| I/II | NCT04160052 | Frontline and R/R HR-MDS | Venetoclax + AZA | |
| II | NCT02115295 | Frontline or R/R AML or HR-MDS | Cladribine + idarubicin + cytarabine + venetoclax | |
| III | NCT04401748 (VERONA trial) | Newly diagnosed HR-MDS | Venetoclax + AZA vs. AZA + placebo | |
| III | NCT04628026 | Newly diagnosed AML or HR-MDS | Venetoclax + induction chemotherapy vs. placebo + induction chemotherapy | |
| BGB-11417 (BCL2 inhibitor) | II | NCT04771130 | Newly-diagnosed AML, MDS, or MDS/MPN overlap | BGB-11417 + AZA |
| Rigosertib (PLK1 inhibitor) | III | NCT02562443 (INSPIRE trial) | HMA-refractory HR-MDS | Rigosertib vs. treatment choice |
| II | NCT01904682 | RBC-TD LR-MDS | rigosertib | |
| II | NCT01926587 | HR-MDS, CMML, or AML <30% blasts | Rigosertib + AZA | |
| Roxadustat (HIF1α inhibitor) | III | NCT03263091 | Very Low, Low or Intermediate IPSS-R With <5% Blasts) MDS with low-transfusion burden | Roxadustat vs. placebo |
| Imetelstat (telomerase inhibitor) | II/III | NCT02598661 (IMerge trial) | LR-MDS, ESA-refractory | Imetelstat vs. placebo |
| Recombinant TPO | II/III | NCT04324060 | LR-MDS with thrombocytopenia | Danazol +/− recombinant human TPO |
| Eltrombopag (TPO mimetic) | II | NCT00961064 | LR-MDS with thrombocytopenia | Eltrombopag |
| II | NCT02912208 | LR-MDS with thrombocytopenia | Eltrombopag vs. placebo | |
| II | NCT01286038 | HMA-refractory MDS, MDS/MPN overlap, AML <30% blasts with thrombocytopenia | Eltrombopag | |
| II | NCT01772420 | LR-MDS with symptomatic anemia | Eltrombopag + lenalidomide | |
| Glasdegib (hedgehog pathway inhibitor) | II | NCT01842646 | MDS, CMML, or AML with <30% bone marrow blasts with HMA failure | Glasdegib |
| II | NCT02367456 (BRIGHT 1012) | Untreated MDS, CMML, or AML ineligible for intensive chemotherapy | Glasdegib + AZA | |
| Luspatercept (TGFβ pathway inhibitor) | III | NCT03682536 | RBC-TD, ESA-naïve LR-MDS | Luspatercept vs. Epoetin alfa |
| III | NCT02631070 (MEDALIST) | RBC-TD, ESA-resistant LR-MDS with ≥15% ring sideroblast or ≥5% SF3B1 mutation | Luspatercept vs. placebo | |
| I/II | NCT04539236 | RBC-TD, ESA-resistant LR-MDS | Luspatercept + lenalidomide | |
| IIIb | NCT04064060 | MDS, myelofibrosis, beta-thalassemia previously enrolled in luspatercept clinical trials | Luspatercept | |
| KER-050 (TGFβ pathway inhibitor) | II | NCT04419649 | RBC-TD LR-MDS | KER-050 |
| SY-1425 (selective retinoic acid receptor α agonist) | II | NCT02807558 | R/R-AML or HR-MDS; frontline AML ineligible for intensive chemotherapy | SY-1425 (tamibarotene) + AZA + daratumumab |
| Alvocidib (CDK9 inhibitor) | Ib/II | NCT03593915 | Untreated HR-MDS | Alvocidib + DEC or AZA |
| Selinexor (selective inhibitor of nuclear export) | II | NCT02228525 | HMA-refractory MDS | Selinexor |
| ATG 016 (selective inhibitor of nuclear export) | II | NCT04691141 | HMA-refractory HR-MDS | ATG 016 |
| I/II | NCT02649790 | HMA-refractory, HR-MDS | KPT-8602 | |
| Bemcentinib (AXL kinase inhibitor) | II | NCT03824080 | HMA-refractory MDS and AML | Bemcentinib |
| ONO-7475 (AXL inhibitor) | II | NCT03176277 | R/R AML or MDS | ONO-7475 +/− venetoclax |
| LB-100 (protein phosphatase 2A inhibitor) | II | NCT03886662 | HMA-refractory LR-MDS | LB-100 |
| TEW-7197 (Vactosertib; ALK5 inhibitor) | II | NCT03074006 | LR-MDS | TEW-7197 |
| INCB000928 (ALK2 inhibitor) | II | NCT04582539 | ESA-refractory MDS | INCB000928 |
| TP-0184 (ALK2 or ACRV1 kinase inhibitor) | II | NCT04623996 | ESA-refractory LR-MDS | TP-0184 |
| Omacetaxine (protein translation inhibitor) | II | NCT03564873 | Newly diagnosed, HR-MDS or CMML-2 | Omacetaxine + AZA |
| CG200745 PPA (HDAC inhibitor) | II | NCT02737462 | HMA-refractory MDS | CG200745 PPA |
| CPI-613 (PDH/α-KGDH inhibitor) | II | NCT03929211 | HMA-refractory HR-MDS | CPI-613 + hydroxychloroquine |
| Ascorbic acid | II | NCT03397173 | Newly diagnosed AML, MDS, or MDS/MPN overlap with TET2 mutations | Ascorbic acid + AZA |
| CFI-400945 (PLK4 inhibitor) | II | NCT04730258 | R/R or untreated AML, MDS, or CMML | CFI-40095 +/− AZA or DEC |
| ONC201 (dopamine D2 receptor antagonist) | II | NCT02392572 | R/R-AML or HR-MDS | ONC201 + LDAC |
| Olaparib (PARP inhibitor) | II | NCT03953898 | R/R-AML or HR-MDS with IDH mutations | Olaparib |
| Veliparib (PARP inhibitor) | II | NCT03289910 | Newly-diagnosed or R/R-AML, CMML or MPN | Carboplatin + Topotecan +/− veliparib |
| Sirolimus (mTOR inhibitor) | II | NCT01869114 | R/R-AML or HR-MDS | Sirolimus + AZA |
| IGF-MTX (methotrexate conjugate) | I/II | NCT03175978 | R/R-AML or HR-MDS/CMML | IGF-methotrexate conjugate |
| OTS167 (MELK inhibitor) | I/II | NCT02795520 | R/R AML, MDS, ALL, CML, MPN | OTS167 |
| Ruxolitinib (JAK inhibitor) | II | NCT01787487 | MDS/MPN overlap | Ruxolitinib + AZA |
| Seclidemstat (LSD1 inhibitor) | II | NCT04734990 | HMA-refractory, HR-MDS or CMML | Seclidemstat + AZA |
| CB-839 (glutaminase inhibitor) | II | NCT03047993 | HR-MDS | CB-839 + AZA |
| Tipifarnib (farnesyl transferase inhibitor) | II | NCT02807272 | CMML, MDS/MPN overlap or AML | Tipifarnib |
| EP0042 | II | NCT04581512 | R/R-AML, MDS, or CMML | EP0042 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bewersdorf, J.P.; Zeidan, A.M. Risk-Adapted, Individualized Treatment Strategies of Myelodysplastic Syndromes (MDS) and Chronic Myelomonocytic Leukemia (CMML). Cancers 2021, 13, 1610. https://doi.org/10.3390/cancers13071610
Bewersdorf JP, Zeidan AM. Risk-Adapted, Individualized Treatment Strategies of Myelodysplastic Syndromes (MDS) and Chronic Myelomonocytic Leukemia (CMML). Cancers. 2021; 13(7):1610. https://doi.org/10.3390/cancers13071610
Chicago/Turabian StyleBewersdorf, Jan Philipp, and Amer M. Zeidan. 2021. "Risk-Adapted, Individualized Treatment Strategies of Myelodysplastic Syndromes (MDS) and Chronic Myelomonocytic Leukemia (CMML)" Cancers 13, no. 7: 1610. https://doi.org/10.3390/cancers13071610
APA StyleBewersdorf, J. P., & Zeidan, A. M. (2021). Risk-Adapted, Individualized Treatment Strategies of Myelodysplastic Syndromes (MDS) and Chronic Myelomonocytic Leukemia (CMML). Cancers, 13(7), 1610. https://doi.org/10.3390/cancers13071610