
Glioblastoma Stem-like Cell Detection Using Perfusion and Diffusion MRI

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Ethics Statement
2.2. Patient Population
2.3. MR Imaging Data Acquisition
- T1CE. 3D T1-weighted after 15 mL injection of Gadolinium contrast (TR/TE = 8/4 ms, FA = 8°, matrix = 165 × 241, 240 slices, 1 × 1 × 1 mm3 resolution).
- FLAIR (TI/TR/TE = 2400/8000/335 ms, FA = 90°, matrix = 200 × 256, 256 slices, resolution = 1 × 1 × 1 mm3)
- T2w. Turbo-spin echo T2-weighted (TR/TE = 4130/80 ms, FA = 90°, matrix = 512 × 512, 43 slices, resolution = 0.5 × 0.5 × 3 mm3).
2.4. MR Imaging Data Processing
2.5. Surgical Planning and Definition of Targets
2.6. Stem Cell Culture and Analysis
2.7. Statistics
3. Results
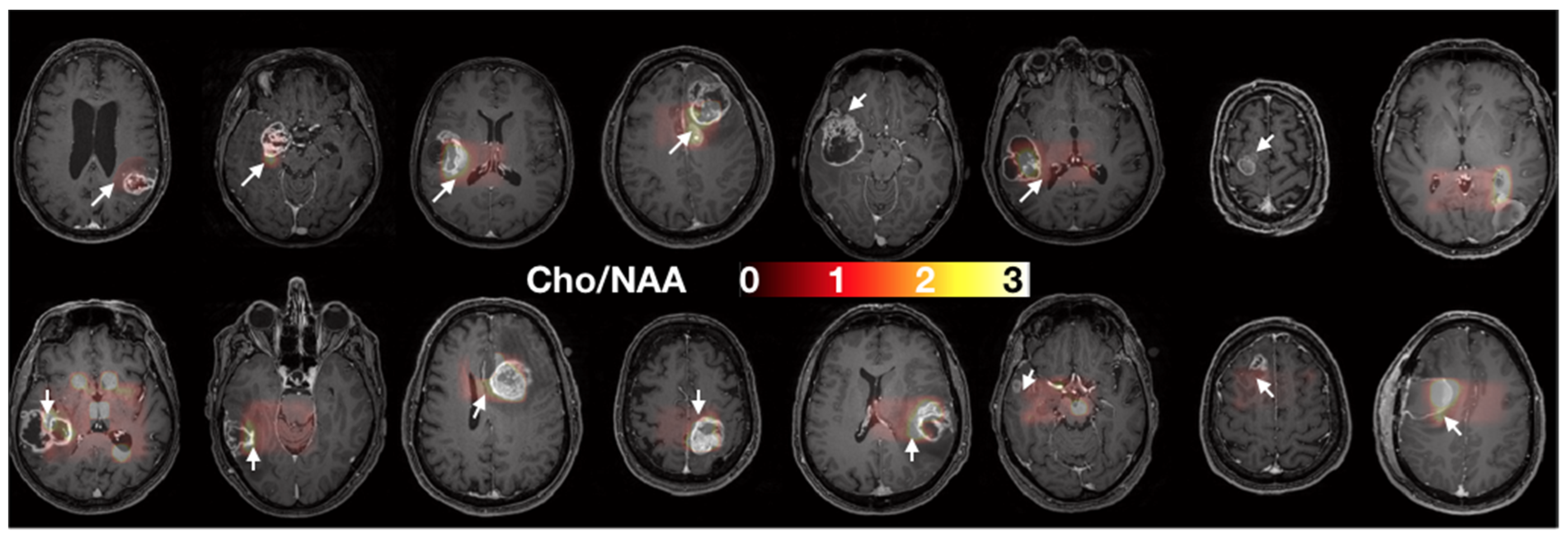
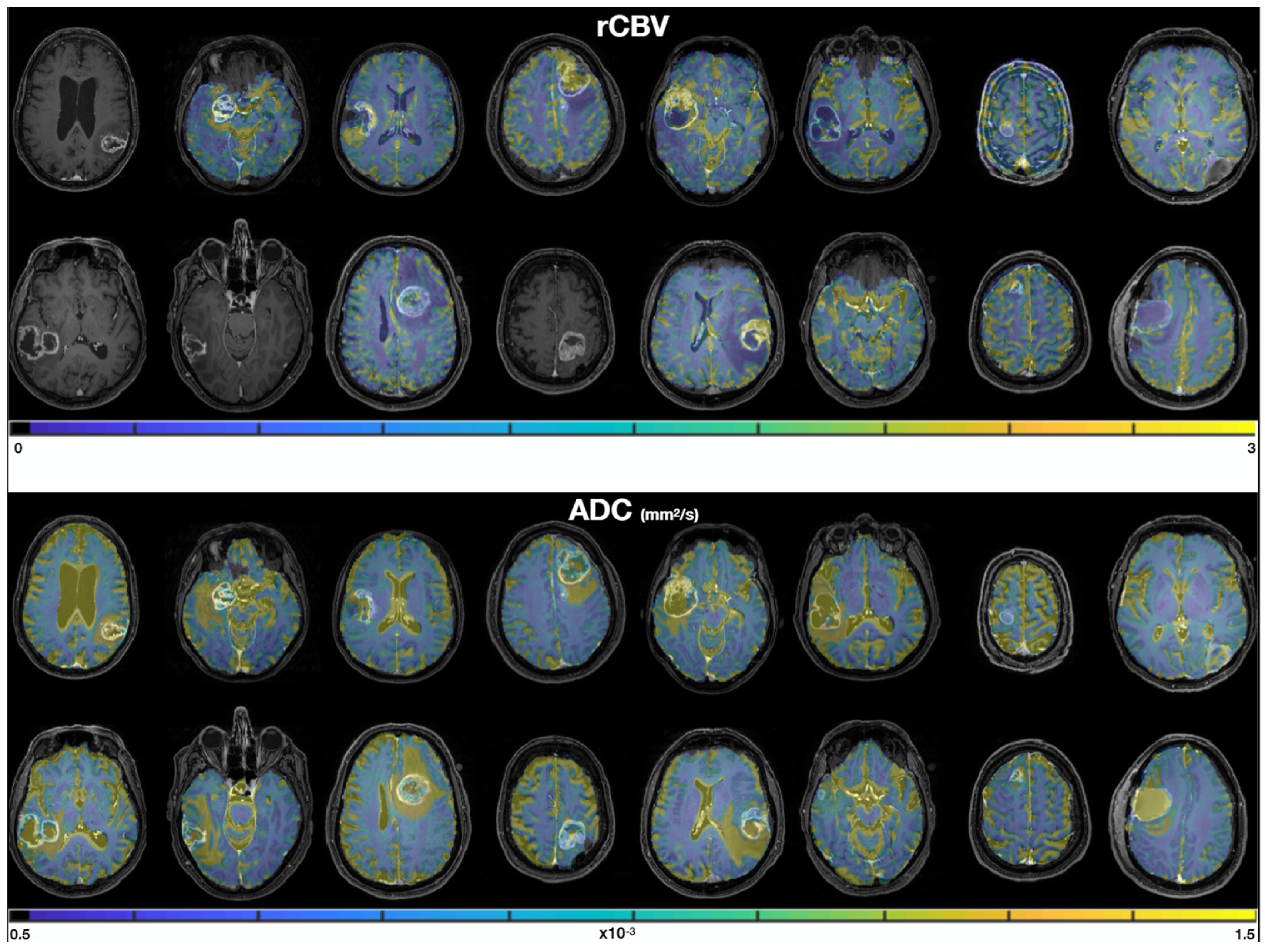
3.1. Multiparametric MRI Maps
3.2. Cell Culture
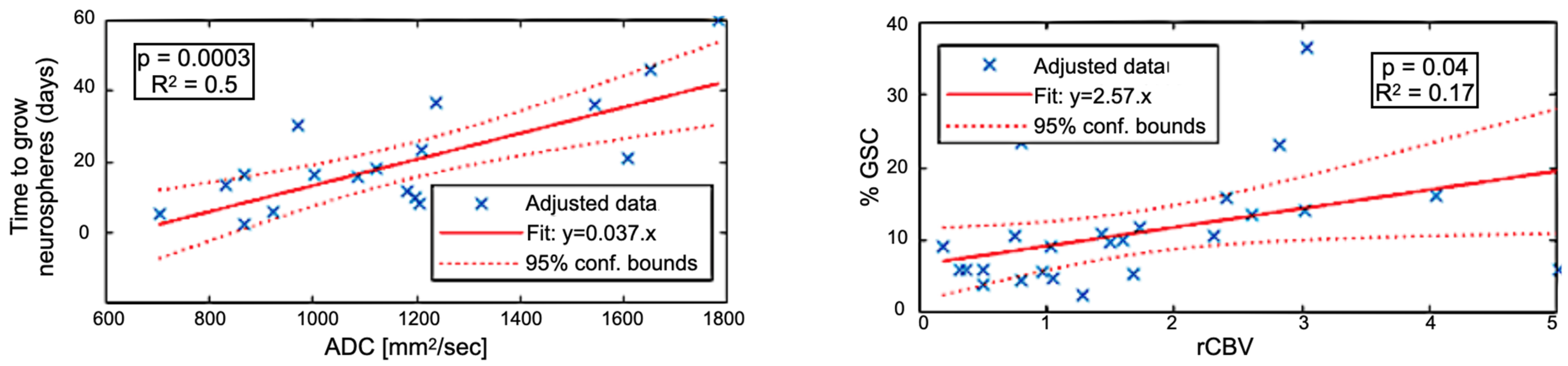
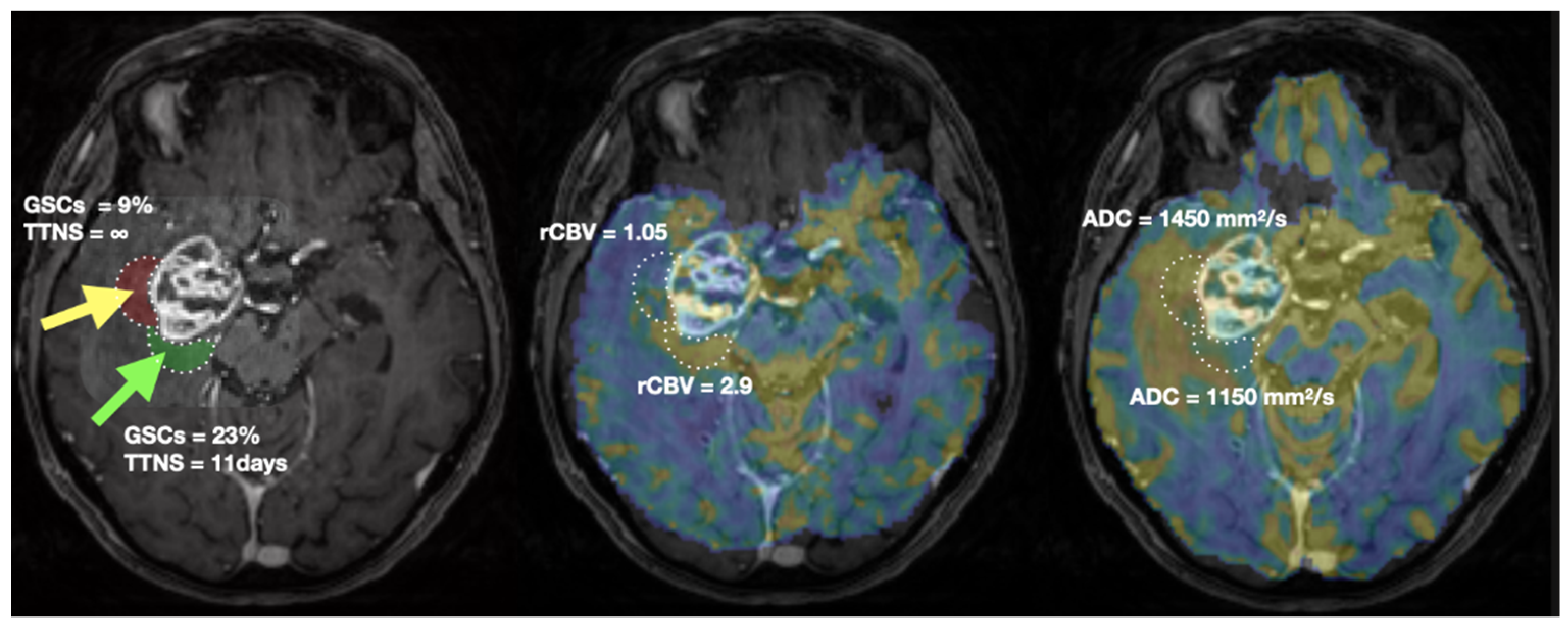
3.3. Correlations between MRI and Biology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Minniti, G.; Amelio, D.; Amichetti, M.; Salvati, M.; Muni, R.; Bozzao, A.; Lanzetta, G.; Scarpino, S.; Arcella, A.; Enrici, R.M. Patterns of Failure and Comparison of Different Target Volume Delineations in Patients with Glioblastoma Treated with Conformal Radiotherapy plus Concomitant and Adjuvant Temozolomide. Radiother. Oncol. 2010, 97, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Milano, M.T.; Okunieff, P.; Donatello, R.S.; Mohile, N.A.; Sul, J.; Walter, K.A.; Korones, D.N. Patterns and Timing of Recurrence after Temozolomide-Based Chemoradiation for Glioblastoma. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1147–1155. [Google Scholar] [CrossRef] [PubMed]
- Park, D.M.; Sathornsumetee, S.; Rich, J.N. Medical Oncology: Treatment and Management of Malignant Gliomas. Nat. Rev. Clin. Oncol. 2010, 7, 75–77. [Google Scholar] [CrossRef]
- Lathia, J.D.; Mack, S.C.; Mulkearns-Hubert, E.E.; Valentim, C.L.L.; Rich, J.N. Cancer Stem Cells in Glioblastoma. Genes Dev. 2015, 29, 1203–1217. [Google Scholar] [CrossRef] [Green Version]
- Cheng, L.; Bao, S.; Rich, J.N. Potential Therapeutic Implications of Cancer Stem Cells in Glioblastoma. Biochem. Pharmacol. 2010, 80, 654–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garnier, D.; Renoult, O.; Alves-Guerra, M.-C.; Paris, F.; Pecqueur, C. Glioblastoma Stem-Like Cells, Metabolic Strategy to Kill a Challenging Target. Front. Oncol. 2019, 9, 118. [Google Scholar] [CrossRef]
- Dahan, P.; Martinez Gala, J.; Delmas, C.; Monferran, S.; Malric, L.; Zentkowski, D.; Lubrano, V.; Toulas, C.; Cohen-Jonathan Moyal, E.; Lemarie, A. Ionizing Radiations Sustain Glioblastoma Cell Dedifferentiation to a Stem-like Phenotype through Survivin: Possible Involvement in Radioresistance. Cell Death Dis. 2014, 5, e1543. [Google Scholar] [CrossRef] [Green Version]
- Deshors, P.; Toulas, C.; Arnauduc, F.; Malric, L.; Siegfried, A.; Nicaise, Y.; Lemarié, A.; Larrieu, D.; Tosolini, M.; Cohen-Jonathan Moyal, E.; et al. Ionizing Radiation Induces Endothelial Transdifferentiation of Glioblastoma Stem-like Cells through the Tie2 Signaling Pathway. Cell Death Dis. 2019, 10, 816. [Google Scholar] [CrossRef]
- Sabatier, J.; Gilard, V.; Malet-Martino, M.; Ranjeva, J.P.; Terral, C.; Breil, S.; Delisle, M.B.; Manelfe, C.; Tremoulet, M.; Berry, I. Characterization of Choline Compounds with in Vitro 1H Magnetic Resonance Spectroscopy for the Discrimination of Primary Brain Tumors. Investig. Radiol. 1999, 34, 230–235. [Google Scholar] [CrossRef]
- Stefano, N.D.; Matthews, P.M.; Arnold, D.L. Reversible Decreases in N-Acetylaspartate after Acute Brain Injury. Magn. Reson. Med. 1995, 34, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.B. N-Acetyl Aspartate: A Marker for Neuronal Loss or Mitochondrial Dysfunction. Dev. Neurosci. 1998, 20, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Stadlbauer, A.; Moser, E.; Gruber, S.; Buslei, R.; Nimsky, C.; Fahlbusch, R.; Ganslandt, O. Improved Delineation of Brain Tumors: An Automated Method for Segmentation Based on Pathologic Changes of 1H-MRSI Metabolites in Gliomas. Neuroimage 2004, 23, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Crawford, F.W.; Khayal, I.S.; McGue, C.; Saraswathy, S.; Pirzkall, A.; Cha, S.; Lamborn, K.R.; Chang, S.M.; Berger, M.S.; Nelson, S.J. Relationship of Pre-Surgery Metabolic and Physiological MR Imaging Parameters to Survival for Patients with Untreated GBM. J. Neurooncol. 2009, 91, 337–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laprie, A.; Catalaa, I.; Cassol, E.; McKnight, T.R.; Berchery, D.; Marre, D.; Bachaud, J.-M.; Berry, I.; Moyal, E.C.-J. Proton Magnetic Resonance Spectroscopic Imaging in Newly Diagnosed Glioblastoma: Predictive Value for the Site of Postradiotherapy Relapse in a Prospective Longitudinal Study. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Barker, P.B. MR Spectroscopy and Spectroscopic Imaging of the Brain. Methods Mol. Biol. 2011, 711, 203–226. [Google Scholar]
- Le Bihan, D.; Breton, E.; Lallemand, D.; Grenier, P.; Cabanis, E.; Laval-Jeantet, M. MR Imaging of Intravoxel Incoherent Motions: Application to Diffusion and Perfusion in Neurologic Disorders. Radiology 1986, 161, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Arvinda, H.R.; Kesavadas, C.; Sarma, P.S.; Thomas, B.; Radhakrishnan, V.V.; Gupta, A.K.; Kapilamoorthy, T.R.; Nair, S. Glioma Grading: Sensitivity, Specificity, Positive and Negative Predictive Values of Diffusion and Perfusion Imaging. J. Neurooncol. 2009, 94, 87–96. [Google Scholar] [CrossRef]
- Duc, N.M. The Role of Diffusion Tensor Imaging Metrics in the Discrimination between Cerebellar Medulloblastoma and Brainstem Glioma. Pediatr. Blood Cancer 2020, 67, e28468. [Google Scholar] [CrossRef]
- Nakamura, H.; Murakami, R.; Hirai, T.; Kitajima, M.; Yamashita, Y. Can MRI-Derived Factors Predict the Survival in Glioblastoma Patients Treated with Postoperative Chemoradiation Therapy? Acta Radiol. 2013, 54, 214–220. [Google Scholar] [CrossRef]
- Saraswathy, S.; Crawford, F.W.; Lamborn, K.R.; Pirzkall, A.; Chang, S.; Cha, S.; Nelson, S.J. Evaluation of MR Markers That Predict Survival in Patients with Newly Diagnosed GBM prior to Adjuvant Therapy. J. Neurooncol. 2009, 91, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Salama, G.R.; Heier, L.A.; Patel, P.; Ramakrishna, R.; Magge, R.; Tsiouris, A.J. Diffusion Weighted/Tensor Imaging, Functional MRI and Perfusion Weighted Imaging in Glioblastoma-Foundations and Future. Front. Neurol. 2017, 8, 660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, M.; Yang, S.; Wang, H.; Babb, J.S.; Johnson, G.; Cha, S.; Knopp, E.A.; Zagzag, D. Glioma Grading: Sensitivity, Specificity, and Predictive Values of Perfusion MR Imaging and Proton MR Spectroscopic Imaging Compared with Conventional MR Imaging. Am. J. Neuroradiol. 2003, 24, 1989–1998. [Google Scholar] [PubMed]
- McKinney, A.M. Differentiation of Recurrent Glioblastoma Multiforme from Radiation Necrosis after External Beam Radiation Therapy with Dynamic Susceptibility-Weighted Contrast-Enhanced Perfusion MR Imaging. Yearb. Neurol. Neurosurg. 2010, 2010, 159–160. [Google Scholar] [CrossRef]
- Cha, J.; Kim, S.T.; Kim, H.-J.; Kim, B.-J.; Kim, Y.K.; Lee, J.Y.; Jeon, P.; Kim, K.H.; Kong, D.-S.; Nam, D.-H. Differentiation of Tumor Progression from Pseudoprogression in Patients with Posttreatment Glioblastoma Using Multiparametric Histogram Analysis. Am. J. Neuroradiol. 2014, 35, 1309–1317. [Google Scholar] [CrossRef] [Green Version]
- Boonzaier, N.R.; Larkin, T.J.; Matys, T.; van der Hoorn, A.; Yan, J.-L.; Price, S.J. Multiparametric MR Imaging of Diffusion and Perfusion in Contrast-Enhancing and Nonenhancing Components in Patients with Glioblastoma. Radiology 2017, 284, 180–190. [Google Scholar] [CrossRef]
- Laks, D.R.; Masterman-Smith, M.; Visnyei, K.; Angenieux, B.; Orozco, N.M.; Foran, I.; Yong, W.H.; Vinters, H.V.; Liau, L.M.; Lazareff, J.A.; et al. Neurosphere Formation Is an Independent Predictor of Clinical Outcome in Malignant Glioma. Stem Cells 2009, 27, 980–987. [Google Scholar] [CrossRef] [Green Version]
- Cusulin, C.; Chesnelong, C.; Bose, P.; Bilenky, M.; Kopciuk, K.; Chan, J.A.; Cairncross, J.G.; Jones, S.J.; Marra, M.A.; Luchman, H.A.; et al. Precursor States of Brain Tumor Initiating Cell Lines Are Predictive of Survival in Xenografts and Associated with Glioblastoma Subtypes. Stem Cell Rep. 2015, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; Degroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated Response Assessment Criteria for High-Grade Gliomas: Response Assessment in Neuro-Oncology Working Group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef]
- Tensaouti, F.; Lotterie, J.A.; Clarisse, P. Sysiphe-Neuroimaging Software Toolbox; Springer: Berlin, Germany, 2008. [Google Scholar]
- Gumprecht, H.K.; Widenka, D.C.; Lumenta, C.B. BrainLab VectorVision Neuronavigation System: Technology and Clinical Experiences in 131 Cases. Neurosurgery 1999, 44, 97–104; discussion 104–105. [Google Scholar] [CrossRef]
- Dick, A.S.; Bernal, B.; Tremblay, P. The Language Connectome: New Pathways, New Concepts. Neuroscientist 2014, 20, 453–467. [Google Scholar] [CrossRef] [PubMed]
- Bello, L.; Castellano, A.; Fava, E.; Casaceli, G.; Riva, M.; Scotti, G.; Gaini, S.M.; Falini, A. Intraoperative Use of Diffusion Tensor Imaging Fiber Tractography and Subcortical Mapping for Resection of Gliomas: Technical Considerations. Neurosurg. Focus 2010, 28, E6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sener, R.N. Diffusion MRI: Apparent Diffusion Coefficient (ADC) Values in the Normal Brain and a Classification of Brain Disorders Based on ADC Values. Comput. Med. Imaging Graph. 2001, 25, 299–326. [Google Scholar] [CrossRef]
- Paldino, M.J.; Barboriak, D.; Desjardins, A.; Friedman, H.S.; Vredenburgh, J.J. Repeatability of Quantitative Parameters Derived from Diffusion Tensor Imaging in Patients with Glioblastoma Multiforme. J. Magn. Reson. Imaging 2009, 29, 1199–1205. [Google Scholar] [CrossRef]
- Kondo, M.; Uchiyama, Y. Apparent Diffusion Coefficient Histogram Analysis for Prediction of Prognosis in Glioblastoma. J. Neuroradiol. 2018, 45, 236–241. [Google Scholar] [CrossRef]
- Cho, N.; Wang, C.; Raymond, C.; Kaprealian, T.; Ji, M.; Salamon, N.; Pope, W.B.; Nghiemphu, P.L.; Lai, A.; Cloughesy, T.F.; et al. Diffusion MRI Changes in the Anterior Subventricular Zone Following Chemoradiation in Glioblastoma with Posterior Ventricular Involvement. J. Neurooncol. 2020, 147, 643–652. [Google Scholar] [CrossRef]
- Arain, F.M.; Shaikh, A.; Waqas, M.; Tariq, M.U.; Raghib, M.F.; Haider, G.; Shamim, M.S.; Mubarak, F.; Hassan, S.H.; Enam, S.A.; et al. Molecular and Radiological Characterization of Glioblastoma Multiforme Using Magnetic Resonance Imaging. J. Neurosurg. Sci. 2021, 65, 47–53. [Google Scholar] [CrossRef]
- Valentini, M.C.; Mellai, M.; Annovazzi, L.; Melcarne, A.; Denysenko, T.; Cassoni, P.; Casalone, C.; Maurella, C.; Grifoni, S.; Fania, P.; et al. Comparison among Conventional and Advanced MRI, 18F-FDG PET/CT, Phenotype and Genotype in Glioblastoma. Oncotarget 2017, 8, 91636–91653. [Google Scholar] [CrossRef] [Green Version]
- Badaut, J.; Ashwal, S.; Adami, A.; Tone, B.; Recker, R.; Spagnoli, D.; Ternon, B.; Obenaus, A. Brain Water Mobility Decreases after Astrocytic Aquaporin-4 Inhibition Using RNA Interference. J. Cereb. Blood Flow Metab. 2011, 31, 819–831. [Google Scholar] [CrossRef] [Green Version]
- Lan, Y.-L.; Wang, X.; Lou, J.-C.; Ma, X.-C.; Zhang, B. The Potential Roles of Aquaporin 4 in Malignant Gliomas. Oncotarget 2017, 8, 32345–32355. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, J.S.; Hirschi, K.K. Diverse Roles of the Vasculature within the Neural Stem Cell Niche. Regen. Med. 2009, 4, 879–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, L.; Huang, Z.; Zhou, W.; Wu, Q.; Donnola, S.; Liu, J.K.; Fang, X.; Sloan, A.E.; Mao, Y.; Lathia, J.D.; et al. Glioblastoma Stem Cells Generate Vascular Pericytes to Support Vessel Function and Tumor Growth. Cell 2013, 153, 139–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, A.; Shiras, A. Cancer Stem Cell-Vascular Endothelial Cell Interactions in Glioblastoma. Biochem. Biophys. Res. Commun. 2016, 473, 688–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheray, M.; Bégaud, G.; Deluche, E.; Nivet, A.; Battu, S.; Lalloué, F.; Verdier, M.; Bessette, B. Cancer Stem-Like Cells in Glioblastoma. In Glioblastoma; Vleeschouwer, S.D., Ed.; Codon Publications: Brisbane, Australia, 2017; ISBN 9780994438126. [Google Scholar]
- Heddleston, J.M.; Li, Z.; McLendon, R.E.; Hjelmeland, A.B.; Rich, J.N. The Hypoxic Microenvironment Maintains Glioblastoma Stem Cells and Promotes Reprogramming towards a Cancer Stem Cell Phenotype. Cell Cycle 2009, 8, 3274–3284. [Google Scholar] [CrossRef] [Green Version]
- Jain, R.; Poisson, L.M.; Gutman, D.; Scarpace, L.; Hwang, S.N.; Holder, C.A.; Wintermark, M.; Rao, A.; Colen, R.R.; Kirby, J.; et al. Outcome Prediction in Patients with Glioblastoma by Using Imaging, Clinical, and Genomic Biomarkers: Focus on the Nonenhancing Component of the Tumor. Radiology 2014, 272, 484–493. [Google Scholar] [CrossRef]
- Mampre, D.; Ehresman, J.; Pinilla-Monsalve, G.; Osorio, M.A.G.; Olivi, A.; Quinones-Hinojosa, A.; Chaichana, K.L. Extending the Resection beyond the Contrast-Enhancement for Glioblastoma: Feasibility, Efficacy, and Outcomes. Br. J. Neurosurg. 2018, 32, 528–535. [Google Scholar] [CrossRef]
- Yan, J.-L.; van der Hoorn, A.; Larkin, T.J.; Boonzaier, N.R.; Matys, T.; Price, S.J. Extent of Resection of Peritumoral Diffusion Tensor Imaging-Detected Abnormality as a Predictor of Survival in Adult Glioblastoma Patients. J. Neurosurg. 2017, 126, 234–241. [Google Scholar] [CrossRef]
- Certo, F.; Altieri, R.; Maione, M.; Schonauer, C.; Sortino, G.; Fiumanò, G.; Tirrò, E.; Massimino, M.; Broggi, G.; Vigneri, P.; et al. FLAIRectomy in Supramarginal Resection of Glioblastoma Correlates With Clinical Outcome and Survival Analysis: A Prospective, Single Institution, Case Series. Oper. Neurosurg. 2021, 20, 151–163. [Google Scholar] [CrossRef]
- Gill, B.J.; Pisapia, D.J.; Malone, H.R.; Goldstein, H.; Lei, L.; Sonabend, A.; Yun, J.; Samanamud, J.; Sims, J.S.; Banu, M.; et al. MRI-Localized Biopsies Reveal Subtype-Specific Differences in Molecular and Cellular Composition at the Margins of Glioblastoma. Proc. Natl. Acad. Sci. USA 2014, 111, 12550–12555. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.M.; Suki, D.; Hess, K.; Sawaya, R. The Influence of Maximum Safe Resection of Glioblastoma on Survival in 1229 Patients: Can We Do Better than Gross-Total Resection? J. Neurosurg. 2016, 124, 977–988. [Google Scholar] [CrossRef] [Green Version]
- Schoenegger, K.; Oberndorfer, S.; Wuschitz, B.; Struhal, W.; Hainfellner, J.; Prayer, D.; Heinzl, H.; Lahrmann, H.; Marosi, C.; Grisold, W. Peritumoral Edema on MRI at Initial Diagnosis: An Independent Prognostic Factor for Glioblastoma? Eur. J. Neurol. 2009, 16, 874–878. [Google Scholar] [CrossRef] [PubMed]
- Niyazi, M.; Brada, M.; Chalmers, A.J.; Combs, S.E.; Erridge, S.C.; Fiorentino, A.; Grosu, A.L.; Lagerwaard, F.J.; Minniti, G.; Mirimanoff, R.-O.; et al. ESTRO-ACROP Guideline “Target Delineation of Glioblastomas”. Radiother. Oncol. 2016, 118, 35–42. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age | FLAIR Volume (cm3) | Contrast-Enhanced Volume (cm3) |
|---|---|---|---|---|
| sub-001 | M | 76 | 60 | 23 |
| sub-002 | F | 76 | 37 | 9 |
| sub-003 | M | 66 | 92 | 8 |
| sub-006 | F | 73 | 66 | 14 |
| sub-007 | M | 59 | 151 | 36 |
| sub-008 | F | 57 | 37 | 22 |
| sub-009 | F | 72 | 39 | 19 |
| sub-010 | M | 52 | 114 | 23 |
| sub-012 | M | 62 | 166 | 15 |
| sub-013 | F | 60 | 92 | 32 |
| sub-014 | M | 72 | 26 | 1 |
| sub-015 | M | 73 | 79 | 17 |
| sub-017 | M | 49 | 22 | 2 |
| sub-019 | M | 78 | 14 | 3 |
| sub-020 | M | 37 | 90 | 10 |
| sub-021 | M | 56 | 31 | 11 |
| MEDIAN | 64 | 63 | 15 | |
| MIN | 376 | 14 | 1 | |
| MAX | 787 | 166 | 36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duval, T.; Lotterie, J.-A.; Lemarie, A.; Delmas, C.; Tensaouti, F.; Moyal, E.C.-J.; Lubrano, V. Glioblastoma Stem-like Cell Detection Using Perfusion and Diffusion MRI. Cancers 2022, 14, 2803. https://doi.org/10.3390/cancers14112803
Duval T, Lotterie J-A, Lemarie A, Delmas C, Tensaouti F, Moyal EC-J, Lubrano V. Glioblastoma Stem-like Cell Detection Using Perfusion and Diffusion MRI. Cancers. 2022; 14(11):2803. https://doi.org/10.3390/cancers14112803
Chicago/Turabian StyleDuval, Tanguy, Jean-Albert Lotterie, Anthony Lemarie, Caroline Delmas, Fatima Tensaouti, Elizabeth Cohen-Jonathan Moyal, and Vincent Lubrano. 2022. "Glioblastoma Stem-like Cell Detection Using Perfusion and Diffusion MRI" Cancers 14, no. 11: 2803. https://doi.org/10.3390/cancers14112803
APA StyleDuval, T., Lotterie, J.-A., Lemarie, A., Delmas, C., Tensaouti, F., Moyal, E. C.-J., & Lubrano, V. (2022). Glioblastoma Stem-like Cell Detection Using Perfusion and Diffusion MRI. Cancers, 14(11), 2803. https://doi.org/10.3390/cancers14112803