
Volatilome Analysis in Prostate Cancer by Electronic Nose: A Pilot Monocentric Study

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Electronic Nose and Measurement Chamber
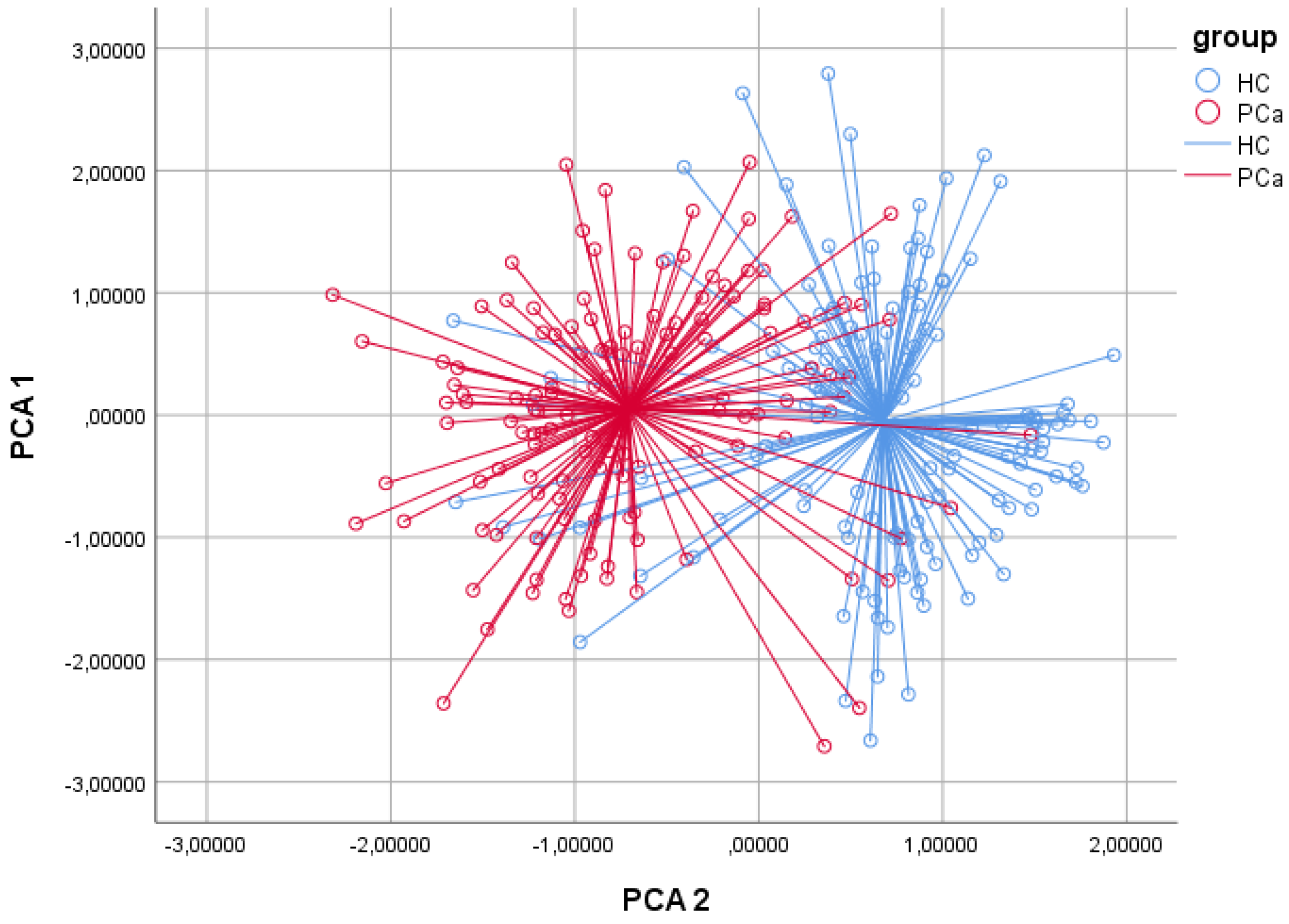
2.3. Data Analysis
3. Results
4. Discussion
5. Clinical Translation
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| VOCs | Volatile organic compounds |
| PCa: | Prostate cancer |
| PCA | Principal component analysis |
| CDA | canonical discriminant analysis |
| CVA | Cross Validated Accuracy |
| ROC | Receiver operator curve |
| VPP | Positive prognostic value |
| VPN | Negative prognostic value |
| PSA | Prostate-specific antigen |
| eNOSE | Electronic nose |
| G/LC-MS | Gas/Liquid Chromatography-Mass Spectrometry |
| HC | Healthy control group |
| UTIs | Urinary tract infections |
| cfDNA | Cell-free DNA |
| ctDNA | Circulating tumor DNA |
References
- Ferlay, J.; Soerjomataram, I.; Ervik, M. GLOBOCAN 2012 v1.0: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Church, J.; Williams, H. Another sniffer dog for the clinic? Lancet 2001, 15, 358–930. [Google Scholar] [CrossRef]
- Gordon, R.T.; Schatz, C.B.; Myers, L.J.; Kosty, M.; Gonczy, C.; Kroener, J.; Tran, M.; Kurtzhals, P.; Heath, S.; Koziol, J.A.; et al. The Use of Canines in the Detection of Human Cancers. J. Altern. Complement. Med. 2008, 14, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Gardner, J.; Bartlett, P.N. A brief history of electronic noses. Sens. Actuators B Chem. 1994, 18, 210–211. [Google Scholar] [CrossRef]
- Capelli, L.; Taverna, G.; Bellini, A.; Eusebio, L.; Buffi, N.; Lazzeri, M.; Guazzoni, G.; Bozzini, G.; Seveso, M.; Mandressi, A.; et al. Application and Uses of Electronic Noses for Clinical Diagnosis on Urine Samples: A Review. Sensors 2016, 16, 1708. [Google Scholar] [CrossRef] [Green Version]
- Bonah, E.; Huang, X.; Aheto, J.H.; Osae, R. Application of electronic nose as a non-invasive technique for odor fingerprinting and detection of bacterial foodborne pathogens: A review. J. Food Sci. Technol. 2020, 57, 1977–1990. [Google Scholar] [CrossRef]
- Gębicki, J.; Dymerski, T.; Namieśnik, J. Monitoring of odour nuisance from landfill using electronic nose. Chem. Eng. Trans. 2014, 40, 85–90. [Google Scholar]
- Brudzewski, K.; Osowski, S.; Pawłowski, W. Metal oxide sensor arrays for detection of explosives at sub-parts-per million concentration levels by the differential electronic nose. Sens. Actuators B Chem. 2011, 161, 528–533. [Google Scholar] [CrossRef]
- Deshmukh, S.; Bandyopadhyay, R.; Bhattacharyya, N.; Pandey, R.; Jana, A. Application of electronic nose for industrial odors and gaseous emissions measurement and monitoring—An overview. Talanta 2015, 144, 329–340. [Google Scholar] [CrossRef]
- Dang, L.; Tian, F.; Zhang, L.; Kadri, C.; Yin, X.; Peng, X.; Liu, S. A novel classifier ensemble for recognition of multiple indoor air contaminants by an electronic nose. Sens. Actuators B Chem. 2014, 207, 67–74. [Google Scholar] [CrossRef]
- Rosi, P.E.; Miscoria, S.A.; Bernik, D.L.; Negri, R.M. Customized design of electronic noses placed on top of air-lift bioreactors for in situ monitoring the off-gas patterns. Bioprocess Biosyst. Eng. 2012, 35, 835–842. [Google Scholar] [CrossRef]
- Dragonieri, S.; Annema, J.T.; Schot, R.; van der Schee, M.P.; Spanevello, A.; Carratú, P.; Resta, O.; Rabe, K.F.; Sterk, P.J. An electronic nose in the discrimination of patients with lung cancer and COPD. Lung Cancer 2009, 64, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Lewis, N.S. Comparisons between Mammalian and Artificial Olfaction Based on Arrays of Carbon Black−Polymer Composite Vapor Detectors. Acc. Chem. Res. 2004, 37, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Broadhurst, D.I.; Kjell, D.B. Statistical strategies for avoiding false discoveries in metabolomics and related experiments. Metabolomics 2006, 2, 171–196. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Cancer. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 3 February 2022).
- Blumen, H.; Fitch, K.; Polkus, V. Comparison of Treatment Costs for Breast Cancer, by Tumor Stage and Type of Service. Am. Health Drug Benefits 2016, 9, 23–32. [Google Scholar]
- Cipriano, L.E.; Romanus, D.; Earle, C.C.; Neville, B.A.; Halpern, E.F.; Gazelle, G.S.; McMahon, P.M. Lung cancer treatment costs, including patient responsibility, by disease stage and treatment modality, 1992 to 2003. Value Health 2011, 14, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Kwapisz, D. The first liquid biopsy test approved. Is it a new era of mutation testing for non-small cell lung cancer? Ann. Transl. Med. 2017, 5, 46. [Google Scholar] [CrossRef] [Green Version]
- Crowley, E.; Di Nicolantonio, F.; Loupakis, F.; Bardelli, A. Liquid biopsy: Monitoring cancer-genetics in the blood. Nat. Rev. Clin. Oncol. 2013, 10, 472–484. [Google Scholar] [CrossRef]
- Yoshioka, Y.; Kosaka, N.; Konishi, Y.; Ohta, H.; Okamoto, H.; Sonoda, H.; Nonaka, R.; Yamamoto, H.; Ishii, H.; Mori, M.; et al. Ultra-sensitive liquid biopsy of circulating extracellular vesicles using exoscreen. Nat. Commun. 2014, 5, 3591. [Google Scholar] [CrossRef]
- Pantel, K.; Alix-Panabières, C. Real-time liquid biopsy in cancer patients: Fact or fiction? Cancer Res. 2013, 73, 6384–6388. [Google Scholar] [CrossRef] [Green Version]
- Labib, M.; Mohamadi, R.M.; Poudineh, M.; Ahmed, S.U.; Ivanov, I.; Huang, C.-L.; Moosavi, M.; Sargent, E.H.; Kelley, S.O. Single-cell mrna cytometry via sequence-specific nanoparticle clustering and trapping. Nat. Chem. 2018, 10, 489–495. [Google Scholar] [CrossRef]
- Stroun, M.; Lyautey, J.; Lederrey, C.; Olson-Sand, A.; Anker, P. About the possible origin and mechanism of circulating DNA: Apoptosis and active DNA release. Clin. Chim. Acta 2001, 313, 139–142. [Google Scholar] [CrossRef]
- Siena, S.; Sartore-Bianchi, A.; Garcia-Carbonero, R.; Karthaus, M.; Smith, D.; Tabernero, J.; Van Cutsem, E.; Guan, X.; Boedigheimer, M.; Ang, A.; et al. Dynamic molecular analysis and clinical correlates of tumor evolution within a phase ii trial of panitumumab-based therapy in metastatic colorectal cancer. Ann. Oncol. 2017, 29, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Thierry, A.R.; Mouliere, F.; Gongora, C.; Ollier, J.; Robert, B.; Ychou, M.; Del Rio, M.; Molina, F. Origin and quantification of circulating DNA in mice with human colorectal cancer xenografts. Nucleic Acids Res. 2010, 38, 6159–6175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early-and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra24. [Google Scholar] [CrossRef] [Green Version]
- Bajaj, A.; Miranda, O.R.; Kim, I.-B.; Phillips, R.L.; Jerry, D.J.; Bunz, U.H.; Rotello, V.M. Detection and differentiation of normal, cancerous, and metastatic cells using nanoparticlepolymer sensor arrays. Proc. Natl. Acad. Sci. USA 2009, 106, 10912–10916. [Google Scholar] [CrossRef] [Green Version]
- Lorenzo, N.; Wan, T.; Harper, R.J.; Hsu, Y.-L.; Chow, M.; Rose, S.; Furton, K.G. Laboratory and field experiments used to identify Canis lupus var. familiaris active odor signature chemicals from drugs, explosives, and humans. Anal. Bioanal. Chem. 2003, 376, 1212–1224. [Google Scholar] [CrossRef]
- Williams, H.; Pembroke, A. Sniffer dogs in the melanoma clinic? Lancet 1989, 1, 734. [Google Scholar] [CrossRef]
- Cornu, J.N.; Cancel-Tassin, G.; Ondet, V.; Girardet, C.; Cussenot, O. Olfactory detection of prostate cancer by dogs sniffing urine: A step forward in early diagnosis. Eur. Urol. 2011, 59, 197–201. [Google Scholar] [CrossRef]
- Taverna, G.; Tidu, L.; Grizzi, F. Sniffing out prostate cancer: A new clinical opportunity. Central Eur. J. Urol. 2015, 68, 308–310. [Google Scholar] [CrossRef] [Green Version]
- Willis, C.M.; Church, S.M.; Guest, C.M.; Cook, W.A.; McCarthy, N.; Bransbury, A.J.; Church, M.R.T.; Church, J.C.T. Olfactory detection of human bladder cancer by dogs: Proof of principle study. BMJ 2004, 329, 712. [Google Scholar] [CrossRef] [Green Version]
- Wojnowski, W.; Dymerski, T.; Gębicki, J.; Namieśnik, J. Electronic Noses in Medical Diagnostics. Curr. Med. Chem. 2019, 26, 197–215. [Google Scholar] [CrossRef] [PubMed]
- Bernabei, M.; Pennazza, G.; Santonico, M.; Corsi, C.; Roscioni, C.; Paolesse, R.; Di Natale, C.; D’Amico, A. A preliminary study on the possibility to diagnose urinary tract cancers by an electronic nose. Sens. Actuators B Chem. 2008, 131, 1–4. [Google Scholar] [CrossRef]
- Capelli, L.; Bax, C.; Grizzi, F.; Taverna, G. Optimization of training and measurement protocol for eNose analysis of urine headspace aimed at prostate cancer diagnosis. Sci. Rep. 2021, 11, 20898. [Google Scholar] [CrossRef] [PubMed]
- Roine, A.; Veskimäe, E.; Tuokko, A.; Kumpulainen, P.; Koskimäki, J.; Keinänen, T.A.; Häkkinen, M.R.; Vepsäläinen, J.; Paavonen, T.; Lekkala, J.; et al. Detection of Prostate Cancer by an Electronic Nose: A Proof of Principle Study. J. Urol. 2014, 192, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Thorn, R.M.S.; Greenman, J. Microbial volatile compounds in health and disease conditions. J. Breath Res. 2012, 6, 024001. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, L.P.; Lebastchi, A.H.; Horuz, R.; Rastinehad, A.R.; Siddiqui, M.M.; Grummet, J.; Kastner, C.; Ahmed, H.U.; Pinto, P.A.; Turkbey, B. Role of multiparametric prostate MRI in the management of prostate cancer. World J. Urol. 2020, 39, 651–659. [Google Scholar] [CrossRef]
- Moradi, A.; Srinivasan, S.; Clements, J.; Batra, J. Beyond the biomarker role: Prostate-specific antigen (PSA) in the prostate cancer microenvironment. Cancer Metastasis Rev. 2019, 38, 333–346. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | PCa Group | HC Group | p-Value |
|---|---|---|---|
| N | 133 | 139 | |
| Age (years), mean ± SD (range) | 67.37 ± 6.10 (46–82) | 65.97 ± 12.99 (42–90) | 0.259 |
| Psa (ng/mL), mean ± SD (range) | 12.65 ± 37.05 (0.5–425) | 3.34 ± 4.64 (0.5–425) | 0.004 |
| Smokers, N (%) | 27 (20.3%) | 22 (15.8%) | 0.339 |
| Comorbidities, N (%) | |||
| - Arterial hypertension | 69 (51.8%) | 60 (43.1%) | 0.15 |
| - History of AMI | 4 (3%) | 2 (1.4%) | 0.38 |
| - COPD | 4 (3%) | 4 (2.8%) | 0.94 |
| - Dyslipidemia | 23 (17.2%) | 27 (19.4%) | 0.65 |
| Prostate Cancer Histopathological Results (TNM and Gleason Score) | |||
|---|---|---|---|
| TNM Stage | n (%) | Gleason Score | n (%) |
| T2a | 8 (6) | 3 + 3 | 30 (22.6) |
| T2b | 4 (3) | 3 + 4 | 52 (39.1) |
| T2c | 71 (53.4) | 4 + 3 | 25 (18.8) |
| T3a | 38 (28.6) | 4 + 4 | 21 (15.8) |
| T3b | 12 (9) | 4 + 5 | 3 (2.2) |
| 5 + 4 | 2 (1.5) | ||
| Total | 133 (100) | 133 (100) | |
| Expected Group Membership | ||||
|---|---|---|---|---|
| Group | HC | PCa | Total | |
| Count | HC | 123 | 16 | 139 |
| PCa | 23 | 110 | 133 | |
| % | HC | 88.5 | 11.5 | 100 |
| PCa | 17.3 | 82.7 | 100 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filianoti, A.; Costantini, M.; Bove, A.M.; Anceschi, U.; Brassetti, A.; Ferriero, M.; Mastroianni, R.; Misuraca, L.; Tuderti, G.; Ciliberto, G.; et al. Volatilome Analysis in Prostate Cancer by Electronic Nose: A Pilot Monocentric Study. Cancers 2022, 14, 2927. https://doi.org/10.3390/cancers14122927
Filianoti A, Costantini M, Bove AM, Anceschi U, Brassetti A, Ferriero M, Mastroianni R, Misuraca L, Tuderti G, Ciliberto G, et al. Volatilome Analysis in Prostate Cancer by Electronic Nose: A Pilot Monocentric Study. Cancers. 2022; 14(12):2927. https://doi.org/10.3390/cancers14122927
Chicago/Turabian StyleFilianoti, Alessio, Manuela Costantini, Alfredo Maria Bove, Umberto Anceschi, Aldo Brassetti, Mariaconsiglia Ferriero, Riccardo Mastroianni, Leonardo Misuraca, Gabriele Tuderti, Gennaro Ciliberto, and et al. 2022. "Volatilome Analysis in Prostate Cancer by Electronic Nose: A Pilot Monocentric Study" Cancers 14, no. 12: 2927. https://doi.org/10.3390/cancers14122927
APA StyleFilianoti, A., Costantini, M., Bove, A. M., Anceschi, U., Brassetti, A., Ferriero, M., Mastroianni, R., Misuraca, L., Tuderti, G., Ciliberto, G., & Simone, G. (2022). Volatilome Analysis in Prostate Cancer by Electronic Nose: A Pilot Monocentric Study. Cancers, 14(12), 2927. https://doi.org/10.3390/cancers14122927