
Integrative Analysis of Intrahepatic Cholangiocarcinoma Subtypes for Improved Patient Stratification: Clinical, Pathological, and Radiological Considerations

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Clinical Features of iCCA Subtypes
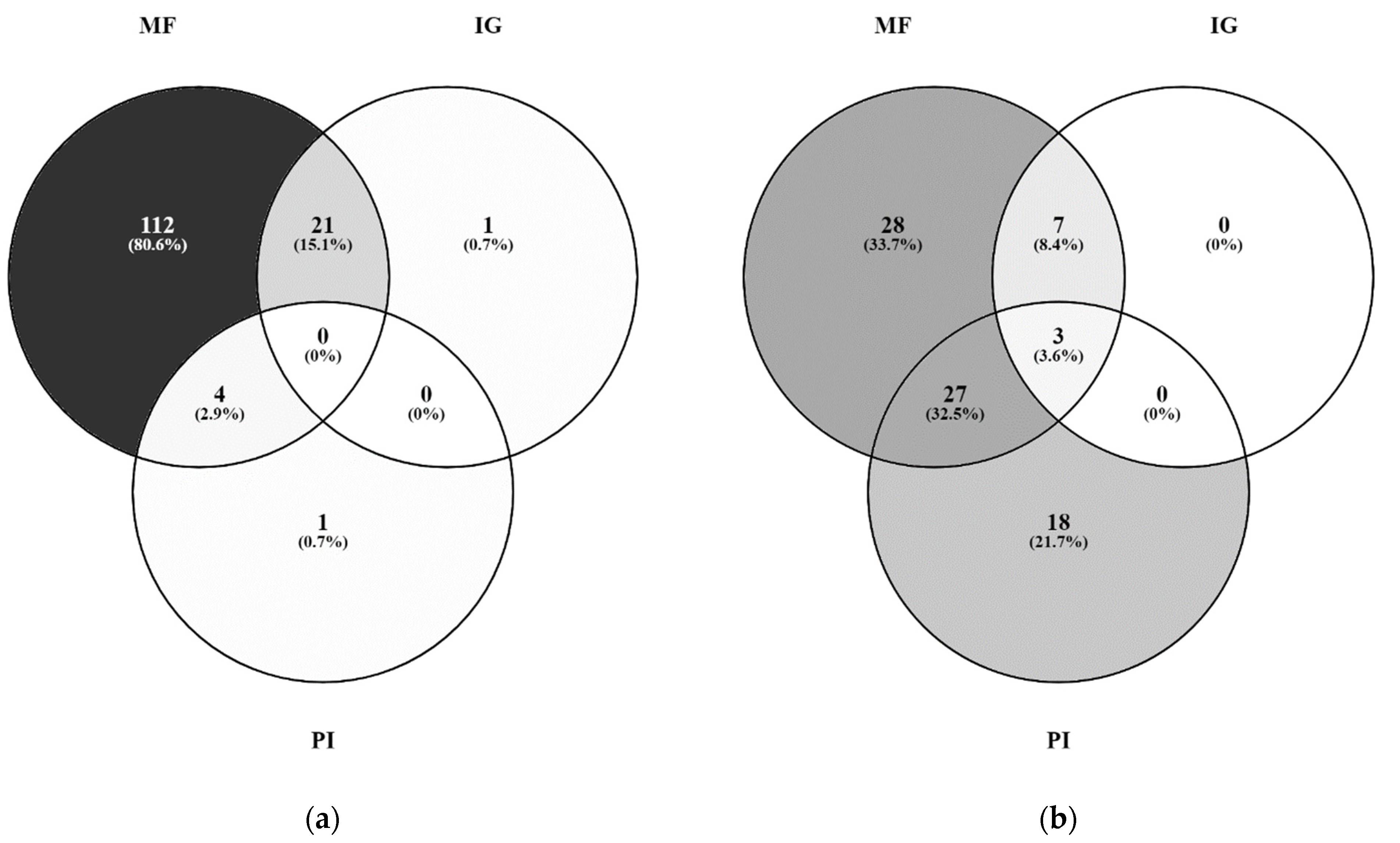
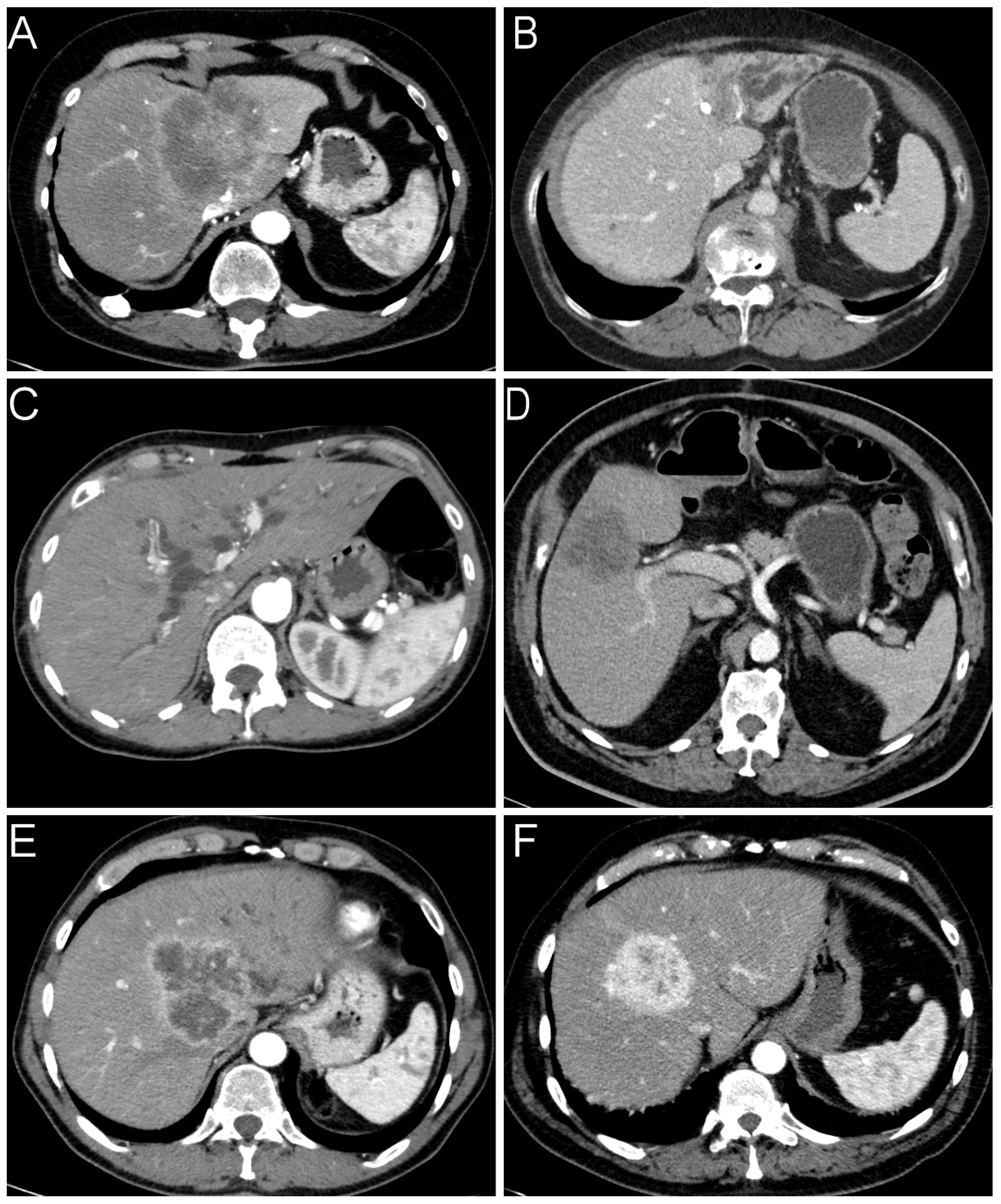
2.2. Radiological Findings
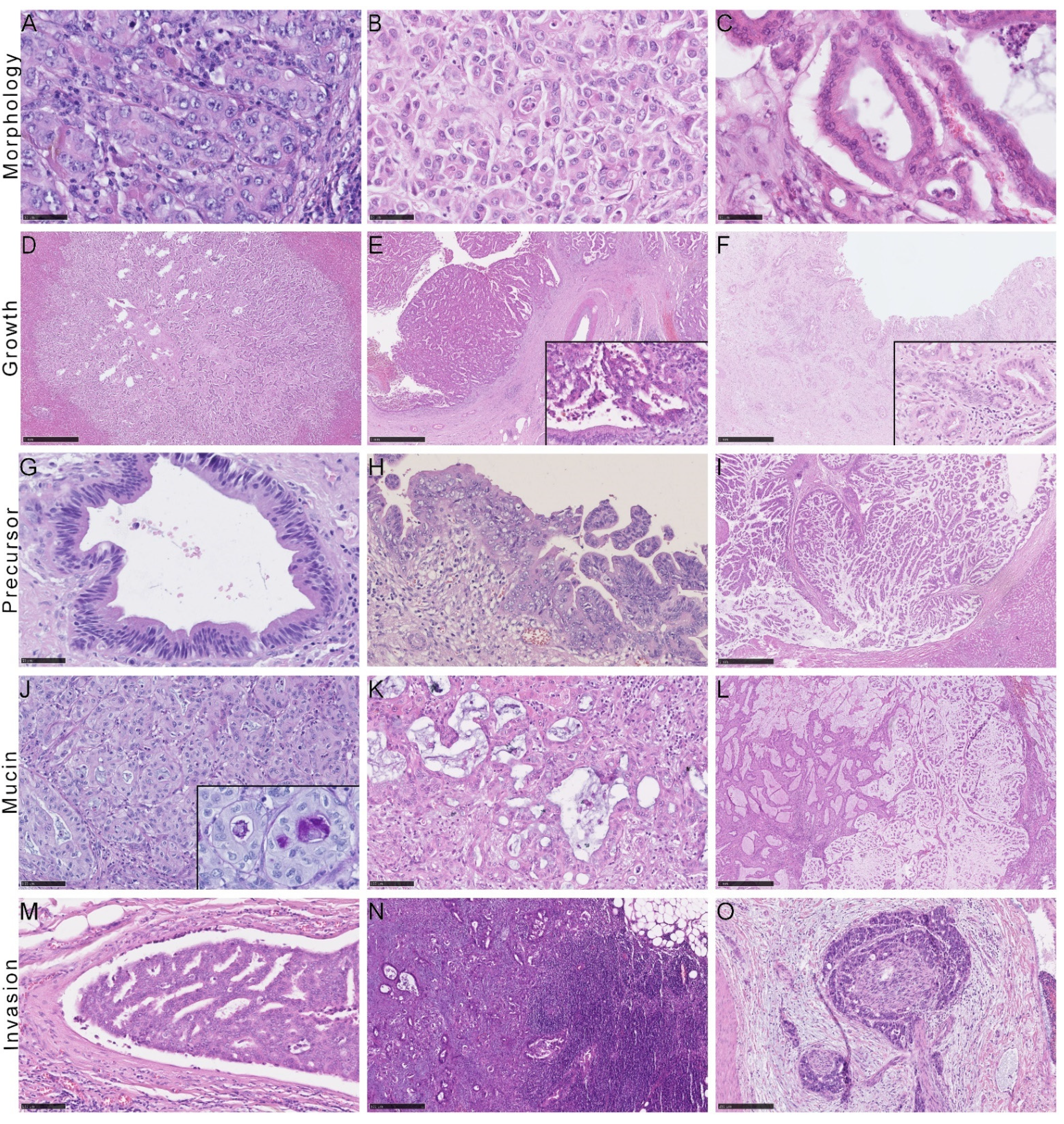
2.3. Histological and Immunohistochemical Features of iCCA Subtypes
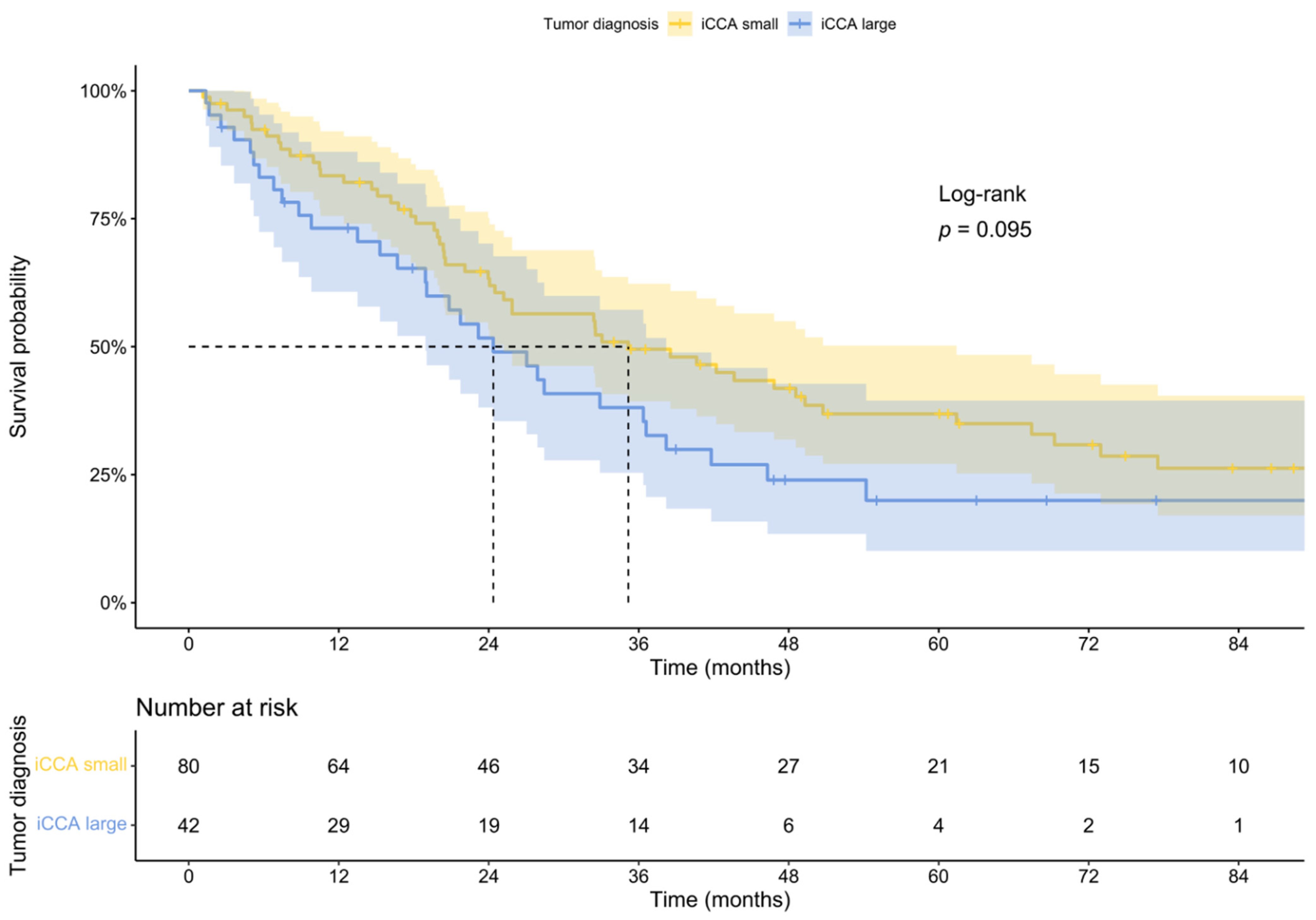
2.4. Patient Survival
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Patient Cohort
5.2. Radiologic Workup
5.3. Histology and Immunohistology
5.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Bertuccio, P.; Malvezzi, M.; Carioli, G.; Hashim, D.; Boffetta, P.; El-Serag, H.B.; La Vecchia, C.; Negri, E. Global trends in mortality from intrahepatic and extrahepatic cholangiocarcinoma. J. Hepatol. 2019, 71, 104–114. [Google Scholar] [CrossRef]
- Rizvi, S.; Khan, S.A.; Hallemeier, C.L.; Kelley, R.K.; Gores, G.J. Cholangiocarcinoma—Evolving concepts and therapeutic strategies. Nat. Rev. Clin. Oncol. 2018, 15, 95–111. [Google Scholar] [CrossRef] [Green Version]
- Xing, H.; Tan, B.; Yang, C.; Zhang, M. Incidence Trend and Competing Risk Analysis of Patients with Intrahepatic Cholangiocarcinoma: A Population-Based Study. Front. Med. 2022, 9, 846276. [Google Scholar] [CrossRef]
- Lamarca, A.; Palmer, D.H.; Wasan, H.S.; Ross, P.J.; Ma, Y.T.; Arora, A.; Falk, S.; Gillmore, R.; Wadsley, J.; Patel, K. ABC-06|A randomised phase III, multi-centre, open-label study of active symptom control (ASC) alone or ASC with oxaliplatin/5-FU chemotherapy (ASC + mFOLFOX) for patients (pts) with locally advanced/metastatic biliary tract cancers (ABC) previously-treated with cisplatin/gemcitabine (CisGem) chemotherapy. J. Clin. Oncol. 2019, 37. [Google Scholar]
- Massironi, S.; Pilla, L.; Elvevi, A.; Longarini, R.; Rossi, R.E.; Bidoli, P.; Invernizzi, P. New and Emerging Systemic Therapeutic Options for Advanced Cholangiocarcinoma. Cells 2020, 9, 688. [Google Scholar] [CrossRef] [Green Version]
- Lanzoni, G.; Cardinale, V.; Carpino, G. The hepatic, biliary, and pancreatic network of stem/progenitor cell niches in humans: A new reference frame for disease and regeneration. Hepatology 2016, 64, 277–286. [Google Scholar] [CrossRef] [Green Version]
- Classification of Tumours Editorial Board. Digestive System Tumours; International Agency for Research on Cancer: Lyon, France, 2019. [Google Scholar]
- Akita, M.; Fujikura, K.; Ajiki, T.; Fukumoto, T.; Otani, K.; Azuma, T.; Itoh, T.; Ku, Y.; Zen, Y. Dichotomy in intrahepatic cholangiocarcinomas based on histologic similarities to hilar cholangiocarcinomas. Mod. Pathol. 2017, 30, 986–997. [Google Scholar] [CrossRef] [Green Version]
- Saha, S.K.; Parachoniak, C.A.; Ghanta, K.S.; Fitamant, J.; Ross, K.N.; Najem, M.S.; Gurumurthy, S.; Akbay, E.A.; Sia, D.; Cornella, H.; et al. Mutant IDH inhibits HNF-4α to block hepatocyte differentiation and promote biliary cancer. Nature 2014, 513, 110–114. [Google Scholar] [CrossRef] [Green Version]
- Kendall, T.; Verheij, J.; Gaudio, E.; Evert, M.; Guido, M.; Goeppert, B.; Carpino, G. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. 2019, 39 (Suppl. S1), 7–18. [Google Scholar] [CrossRef] [Green Version]
- Komuta, M. Histological Heterogeneity of Primary Liver Cancers: Clinical Relevance, Diagnostic Pitfalls and the Pathologist’s Role. Cancers 2021, 13, 2871. [Google Scholar] [CrossRef]
- ASA Physical Status Classification System. Available online: https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system (accessed on 2 May 2022).
- Liau, J.Y.; Tsai, J.H.; Yuan, R.H.; Chang, C.N.; Lee, H.J.; Jeng, Y.M. Morphological subclassification of intrahepatic cholangiocarcinoma: Etiological, clinicopathological, and molecular features. Mod. Pathol. 2014, 27, 1163–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ichikawa, S.; Isoda, H.; Shimizu, T.; Tamada, D.; Taura, K.; Togashi, K.; Onishi, H.; Motosugi, U. Distinguishing intrahepatic mass-forming biliary carcinomas from hepatocellular carcinoma by computed tomography and magnetic resonance imaging using the Bayesian method: A bi-center study. Eur. Radiol. 2020, 30, 5992–6002. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.Y.; Yeom, S.K.; Shin, H.; Choi, S.H.; Rhee, H.; Park, J.H.; Cho, E.S.; Park, S.; Lee, S.S.; Park, M.S. Clinical Staging of Mass-Forming Intrahepatic Cholangiocarcinoma: Computed Tomography Versus Magnetic Resonance Imaging. Hepatol. Commun. 2021, 5, 2009–2018. [Google Scholar] [CrossRef]
- Park, H.J.; Park, B.; Park, S.Y.; Choi, S.H.; Rhee, H.; Park, J.H.; Cho, E.-S.; Yeom, S.-K.; Park, S.; Park, M.-S.; et al. Preoperative prediction of postsurgical outcomes in mass-forming intrahepatic cholangiocarcinoma based on clinical, radiologic, and radiomics features. Eur. Radiol. 2021, 31, 8638–8648. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, X.; Xu, C.; Zhou, G.; Liu, X.; Gao, S.; Xu, P. Mass-forming intrahepatic cholangiocarcinoma: Can diffusion-weighted imaging predict microvascular invasion? J. Magn. Reson. Imaging 2019, 50, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Seo, N.; Kim, D.Y.; Choi, J.Y. Cross-Sectional Imaging of Intrahepatic Cholangiocarcinoma: Development, Growth, Spread, and Prognosis. AJR Am. J. Roentgenol. 2017, 209, W64–W75. [Google Scholar] [CrossRef] [PubMed]
- Akita, M.; Sofue, K.; Fujikura, K.; Otani, K.; Itoh, T.; Ajiki, T.; Fukumoto, T.; Zen, Y. Histological and molecular characterization of intrahepatic bile duct cancers suggests an expanded definition of perihilar cholangiocarcinoma. HPB 2019, 21, 226–234. [Google Scholar] [CrossRef]
- Ariizumi, S.; Kotera, Y.; Takahashi, Y.; Katagiri, S.; Chen, I.P.; Ota, T.; Yamamoto, M. Mass-forming intrahepatic cholangiocarcinoma with marked enhancement on arterial-phase computed tomography reflects favorable surgical outcomes. J. Surg. Oncol. 2011, 104, 130–139. [Google Scholar] [CrossRef]
- Kim, S.J.; Lee, J.M.; Han, J.K.; Kim, K.H.; Lee, J.Y.; Choi, B.I. Peripheral mass-forming cholangiocarcinoma in cirrhotic liver. AJR Am. J. Roentgenol. 2007, 189, 1428–1434. [Google Scholar] [CrossRef]
- Chen, L.D.; Xu, H.X.; Xie, X.Y.; Lu, M.D.; Xu, Z.F.; Liu, G.J.; Liang, J.Y.; Lin, M.X. Enhancement patterns of intrahepatic cholangiocarcinoma: Comparison between contrast-enhanced ultrasound and contrast-enhanced CT. Br. J. Radiol. 2008, 81, 881–889. [Google Scholar] [CrossRef]
- Fujita, N.; Asayama, Y.; Nishie, A.; Ishigami, K.; Ushijima, Y.; Takayama, Y.; Okamoto, D.; Moirta, K.; Shirabe, K.; Aishima, S.; et al. Mass-forming intrahepatic cholangiocarcinoma: Enhancement patterns in the arterial phase of dynamic hepatic CT—Correlation with clinicopathological findings. Eur. Radiol. 2017, 27, 498–506. [Google Scholar] [CrossRef]
- Takahashi, Y.; Dungubat, E.; Kusano, H.; Ganbat, D.; Tomita, Y.; Odgerel, S.; Fukusato, T. Application of Immunohistochemistry in the Pathological Diagnosis of Liver Tumors. Int. J. Mol. Sci. 2021, 22, 5780. [Google Scholar] [CrossRef] [PubMed]
- Krenzien, F.; Nevermann, N.; Krombholz, A.; Benzing, C.; Haber, P.; Fehrenbach, U.; Lurje, G.; Pelzer, U.; Pratschke, J.; Schmelzle, M.; et al. Treatment of Intrahepatic Cholangiocarcinoma-A Multidisciplinary Approach. Cancers 2022, 14, 362. [Google Scholar] [CrossRef] [PubMed]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef]
- Nakanuma, Y.; Kakuda, Y. Pathologic classification of cholangiocarcinoma: New concepts. Best Pract. Res. Clin. Gastroenterol. 2015, 29, 277–293. [Google Scholar] [CrossRef] [PubMed]
- Nakanuma, Y.; Sudo, Y. Biliary tumors with pancreatic counterparts. Semin. Diagn. Pathol. 2017, 34, 167–175. [Google Scholar] [CrossRef]
- Aishima, S.; Oda, Y. Pathogenesis and classification of intrahepatic cholangiocarcinoma: Different characters of perihilar large duct type versus peripheral small duct type. J. Hepatobiliary Pancreat. Sci. 2015, 22, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Aishima, S.; Kuroda, Y.; Nishihara, Y.; Iguchi, T.; Taguchi, K.; Taketomi, A.; Maehara, Y.; Tsuneyoshi, M. Proposal of progression model for intrahepatic cholangiocarcinoma: Clinicopathologic differences between hilar type and peripheral type. Am. J. Surg. Pathol. 2007, 31, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Komuta, M.; Govaere, O.; Vandecaveye, V.; Akiba, J.; Van Steenbergen, W.; Verslype, C.; Laleman, W.; Pirenne, J.; Aerts, R.; Yano, H.; et al. Histological diversity in cholangiocellular carcinoma reflects the different cholangiocyte phenotypes. Hepatology 2012, 55, 1876–1888. [Google Scholar] [CrossRef]
- Akita, M.; Sawada, R.; Komatsu, M.; Suleman, N.; Itoh, T.; Ajiki, T.; Heaton, N.; Fukumoto, T.; Zen, Y. An immunostaining panel of C-reactive protein, N-cadherin, and S100 calcium binding protein P is useful for intrahepatic cholangiocarcinoma subtyping. Hum. Pathol. 2021, 109, 45–52. [Google Scholar] [CrossRef]
- Chi, Z.; Bhalla, A.; Saeed, O.; Cheng, L.; Curless, K.; Wang, H.L.; Patil, D.T.; Lin, J. Mucinous intrahepatic cholangiocarcinoma: A distinct variant. Hum. Pathol. 2018, 78, 131–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loy, T.S.; Sharp, S.C.; Andershock, C.J.; Craig, S.B. Distribution of CA 19-9 in adenocarcinomas and transitional cell carcinomas. An immunohistochemical study of 527 cases. Am. J. Clin. Pathol. 1993, 99, 726–728. [Google Scholar] [CrossRef]
- Brunt, E.; Aishima, S.; Clavien, P.A.; Fowler, K.; Goodman, Z.; Gores, G.; Gouw, A.; Kagen, A.; Klimstra, D.; Komuta, M.; et al. cHCC-CCA: Consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentation. Hepatology 2018, 68, 113–126. [Google Scholar] [CrossRef] [Green Version]
- Tillich, M.; Mischinger, H.J.; Preisegger, K.H.; Rabl, H.; Szolar, D.H. Multiphasic helical CT in diagnosis and staging of hilar cholangiocarcinoma. AJR Am. J. Roentgenol. 1998, 171, 651–658. [Google Scholar] [CrossRef]
- Clavien, P.-A.; Petrowsky, H.; DeOliveira, M.L.; Graf, R. Strategies for Safer Liver Surgery and Partial Liver Transplantation. N. Engl. J. Med. 2007, 356, 1545–1559. [Google Scholar] [CrossRef] [PubMed]
- Gerber, T.S.; Bartsch, F.; Wagner, D.C.; Schindeldecker, M.; Heuft, L.K.; Roth, W.; Lang, H.; Straub, B.K. Clinicopathological Significance of Syndecan-1 in Cholangiocarcinoma: A Study Based on Immunohistochemistry and Public Sequencing Data. J. Clin. Med. 2021, 10, 2745. [Google Scholar] [CrossRef] [PubMed]
- Wittekind, C. TNM: Klassifikation Maligner Tumoren; Wiley: Hoboken, NJ, USA, 2017. [Google Scholar]
- Stefani, L.C.; Gamermann, P.W.; Backof, A.; Guollo, F.; Borges, R.M.J.; Martin, A.; Caumo, W.; Felix, E.A. Perioperative mortality related to anesthesia within 48 h and up to 30 days following surgery: A retrospective cohort study of 11,562 anesthetic procedures. J. Clin. Anesth. 2018, 49, 79–86. [Google Scholar] [CrossRef]
- Cramér, H. Mathematical Methods of Statistics; Princeton University Press: Princeton, NJ, USA, 1999. [Google Scholar]
- R Core Team, R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2008; Available online: https://www.r-project.org/ (accessed on 22 May 2022).
- FIRTH, D. Bias reduction of maximum likelihood estimates. Biometrika 1993, 80, 27–38. [Google Scholar] [CrossRef]
- Wessa, P. Bias Reduced Logistic Regression (v 1.0.6) in Free Statistics Software (v 1.2.1). Available online: http://www.wessa.net/rwasp_logisticregression.wasp/ (accessed on 2 May 2022).
- Oliveros, J.C. Venny. An Interactive Tool for Comparing Lists with Venn’s Diagrams. Available online: https://bioinfogp.cnb.csic.es/tools/venny/index.html (accessed on 2 May 2022).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Small Duct iCCAs n = 148 | Large Duct iCCAs n = 84 | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|---|
| p-Value | Effect Size | p-Value | OR | 95% CI | ||||
| Clinical | Age [sd (range)] | 65.64 (32–84) | 62.37 (34–83) | |||||
| Male/Female [%] | 52/48 | 56/44 | ||||||
| ASA I/II/III/IV [%] | 1/46/51/2 | 1/43/52/4 | ||||||
| BMI [mean ± sd] | 26.86 ± 4.42 | 26.58 ± 5.03 | ||||||
| Jaundice at diagnosis [%] | 8 | 27 | 0.005 | 0.260 | 0.136 | 3.70 | 0.64–21.5 | |
| Cardial/ pulmonal/ | 22/11/5 | 24/5/3 | ||||||
| renal comorbidities [%] | ||||||||
| Diabetes mellitus [%] | 24 | 15 | 0.16 | 0.583 | 1.37 | 0.44–4.31 | ||
| Alcohol abuse [%] | 4 | 7 | 0.573 | 0.749 | 0.67 | 0.06–8.02 | ||
| Nicotine abuse [%] | 30 | 15 | 0.068 | 0.299 | 0.53 | 0.15–1.81 | ||
| PSC [%] | 0 | 3 | 0.021 | 0.152 | 0.202 | 12.18 | 0.24–610.39 | |
| Viral Hepatitis [%] | 1 | 4 | 0.945 | 0.491 | 2.76 | 0.14–52.94 | ||
| Surgical | Neoadjuvant treatment [%] | 9 | 11 | |||||
| RFA/TACE/ | 8/8/0/84 | 0/12/0/88 | ||||||
| SIRT/ Chemotherapy [%] | ||||||||
| Initially irresectable [%] | 19 | 7 | 0.018 | 0.166 | 0.325 | 4.59 | 0.21–101.85 | |
| Major liver resection [%] | 54 | 76 | 0.002 | 0.222 | 0.416 | 1.56 | 0.52–4.64 | |
| Resection of hilar bifurcation [%] | 10 | 33 | <0.001 | 0.279 | 0.316 | 1.98 | 0.51–7.73 | |
| Lymphadenectomy [%] | 71 | 78 | 0.3032 | 0.416 | 0.63 | 0.20–1.96 | ||
| Major complication [%] | 34 | 32 | 0.735 | 0.543 | 0.71 | 0.23–2.21 | ||
| Recurrence [%] | 51 | 60 | ||||||
| Months to recurrence [mean ± sd] | 15.66 ± 23.51 | 11.24 ± 11.05 | ||||||
| Tumor Characteristics | Small Duct iCCAs n = 122 | Large Duct iCCAs n = 69 | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|---|
| p-Value | Effect Size | p-Value | OR | 95% CI | ||||
| Radiology | CT/ MRT [%] | 79/21 | 72/28 | |||||
| Tumor size [mean ± sd] | 7.79 ± 3.73 | 6.23 ± 2.30 | ||||||
| Ductal growing pattern [%] | 2 | 33 | <0.001 | 0.446 | <0.001 | 16.17 | 3.07–85.06 | |
| Obstruction bile ducts [%] | 25 | 48 | 0.001 | 0.237 | ||||
| Vascular invasion [%] | 20 | 25 | 0.586 | 0.997 | 1.00 | 0.34–2.98 | ||
| Portal vein | 0.229 | 0.939 | 1.02 | 0.56–1.87 | ||||
| invasion [%] | 17 | 18 | ||||||
| entrapment [%] | 20 | 29 | ||||||
| Hepatic artery | 0.713 | 0.156 | 0.62 | 0.32–1.21 | ||||
| invasion [%] | 3 | 1 | ||||||
| entrapment [%] | 16 | 12 | ||||||
| Distant metastasis [%] | 7 | 6 | 0.677 | 0.710 | 0.75 | 0.16–3.58 | ||
| Distance portal bifurcation [mean ± sd] | 2.98 ± 2.37 | 1.56 ± 2.20 | ||||||
| ≥0.5 cm [%] | 58 | 41 | 0.039 | 0.151 | 0.240 | 0.66 | 0.23–1.86 | |
| Distance serosa [mean ± sd] | 0.38 ± 0.82 | 0.43 ± 0.88 | ||||||
| ≥0.5 cm [%] | 16 | 20 | 0.192 | 0.812 | 0.86 | 0.25–2.98 | ||
| Tumor density [mean ± sd] | 0.97 ± 0.34 | 0.91 ± 0.39 | ||||||
| Contrast agent behavior | ||||||||
| hypovascular [%] | 44 | 65 | 0.006 | 0.204 | ||||
| rim-enhanced [%] | 28 | 18 | 0.154 | |||||
| hypervascular [%] | 28 | 17 | 0.074 | |||||
| Multifocal [%] | 31 | 28 | 0.600 | 0.622 | 1.25 | 0.51–3.07 | ||
| Invasion visceral peritoneum [%] | 20 | 28 | 0.211 | 0.622 | 1.34 | 0.41–4.32 | ||
| Invasion extrahepatic structures [%] | 8 | 13 | .282 | 0.786 | 1.23 | 0.27–5.60 | ||
| Radiological diagnosis | ||||||||
| HCC/iCCA/ primary liver tumor/ | 1/63/6/1/10 | 1/68/19/0/12 | ||||||
| metastasis/not classified [%] | ||||||||
| Tumor Characteristics | Small Duct iCCAs n = 148 | Large Duct iCCAs n = 84 | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|---|
| p-Value | Effect Size | p-Value | OR | 95% CI | ||||
| Pathology | Tumor size [mean ± sd] | 7.66 ± 4.03 | 6.31 ± 3.01 | |||||
| BilIn/IPNB [%] | 0/0 | 64/ 11 | <0.001 | 0.731 | <0.001 | 91.69 | 5.71–1472.03 | |
| BilIn low/high-grade [%] | 25/ 75 | |||||||
| Mass-forming [%] | 99 | 78 | <0.001 | 0.342 | ||||
| Intraductal-growing [%] | 15 | 12 | 0.156 | |||||
| Periductal-infiltrating [%] | 3 | 57 | <0.001 | 0.605 | ||||
| Multifocal [%] | 32 | 19 | 0.028 | 0.144 | 0.251 | 0.47 | 0.13–1.74 | |
| Mucin [%] | 88/10/2/0 | 18/56/24/2 | <0.001 | 0.696 | <0.001 | 13.70 | 4.31–43.55 | |
| Necrosis [%] | 36/27/29/8 | 25/32/37/6 | 0.131 | 0.599 | 1.22 | 0.57–2.58 | ||
| Desmoplasia [%] | 36/55/9 | 14/67/19 | <0.001 | 0.282 | 0.011 | 4.41 | 1.37–14.23 | |
| Liver steatosis [mean ± sd] | 10.00 ± 15.39 | 12.98 ± 21.14 | ||||||
| Liver fibrosis [%] | 49/34/11/1/4 | 47/35/13/1/4 | ||||||
| UICC I/II/III/IV [%] | 36/30/28/6 | 32/12/46/10 | ||||||
| pT1/pT2/pT3/pT4 [%] | 46/42/7/6 | 43/31/14/12 | ||||||
| pNX [%] | 18 | 20 | ||||||
| pN0/pN1 [%] | 58/24 | 39/41 | 0.010 | 0.199 | 0.152 | 2.62 | 0.68–10.03 | |
| G1/G2/G3/G4 [%] | 1/73/25/1 | 1/68/31/0 | ||||||
| L1 [%] | 13 | 28 | 0.006 | 0.189 | 0.092 | 3.78 | 0.78–18.35 | |
| Lymph node metastases [mean (range)] | 2.32 (1–7) | 3.09 (1–16) | ||||||
| V1-2 [%] | 22 | 23 | 0.068 | 0.877 | 1.12 | 0.27–4.59 | ||
| Pn1 [%] | 16 | 40 | <0.001 | 0.293 | 0.666 | 1.36 | 0.33–5.63 | |
| R0/R1-2 [%] | 81/15 | 73/26 | 0.002 | 0.253 | 0.786 | 1.23 | 0.27–5.52 | |
| Margin distance [mean ± sd] | 0.47 ± 0.60 | 0.48 ± 0.60 | ||||||
| IHC | CK7 [%] | 1/8/91 | 1/4/95 | 0.369 | 0.149 | 2.94 | 0.66–13.10 | |
| CK20 [%] | 77/22/1 | 50/41/9 | <0.001 | 0.218 | 0.020 | 2.30 | 1.12–4.72 | |
| Ca19-9 [%] | 12/53/35 | 4/46/50 | 0.027 | 0.177 | 0.186 | 1.54 | 0.80–2.95 | |
| EMA [%] | 4/39/56 | 0/25/75 | 0.008 | 0.204 | 0.055 | 2.13 | 0.97–4.69 | |
| S100 [%] | 72/26/2 | 76/24/0 | 0.498 | 0.792 | 1.23 | 0.25–5.96 | ||
| CD56 [%] | 39/45/16 | 61/33/6 | 0.003 | 0.226 | 0.008 | 0.45 | 0.25–0.82 | |
| N-cadherin [%] | 13/31/56 | 27/33/30 | 0.004 | 0.262 | 0.124 | 0.67 | 0.40–1.13 | |
| CRP [%] | 7/16/77 | 24/26/50 | <0.001 | 0.290 | 0.101 | 0.63 | 0.36–1.11 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerber, T.S.; Müller, L.; Bartsch, F.; Gröger, L.-K.; Schindeldecker, M.; Ridder, D.A.; Goeppert, B.; Möhler, M.; Dueber, C.; Lang, H.; et al. Integrative Analysis of Intrahepatic Cholangiocarcinoma Subtypes for Improved Patient Stratification: Clinical, Pathological, and Radiological Considerations. Cancers 2022, 14, 3156. https://doi.org/10.3390/cancers14133156
Gerber TS, Müller L, Bartsch F, Gröger L-K, Schindeldecker M, Ridder DA, Goeppert B, Möhler M, Dueber C, Lang H, et al. Integrative Analysis of Intrahepatic Cholangiocarcinoma Subtypes for Improved Patient Stratification: Clinical, Pathological, and Radiological Considerations. Cancers. 2022; 14(13):3156. https://doi.org/10.3390/cancers14133156
Chicago/Turabian StyleGerber, Tiemo S., Lukas Müller, Fabian Bartsch, Lisa-Katharina Gröger, Mario Schindeldecker, Dirk A. Ridder, Benjamin Goeppert, Markus Möhler, Christoph Dueber, Hauke Lang, and et al. 2022. "Integrative Analysis of Intrahepatic Cholangiocarcinoma Subtypes for Improved Patient Stratification: Clinical, Pathological, and Radiological Considerations" Cancers 14, no. 13: 3156. https://doi.org/10.3390/cancers14133156