
Antitumoral Effects of Tricyclic Antidepressants: Beyond Neuropathic Pain Treatment

 , ,
, ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. The Role of Nerves in Cancer
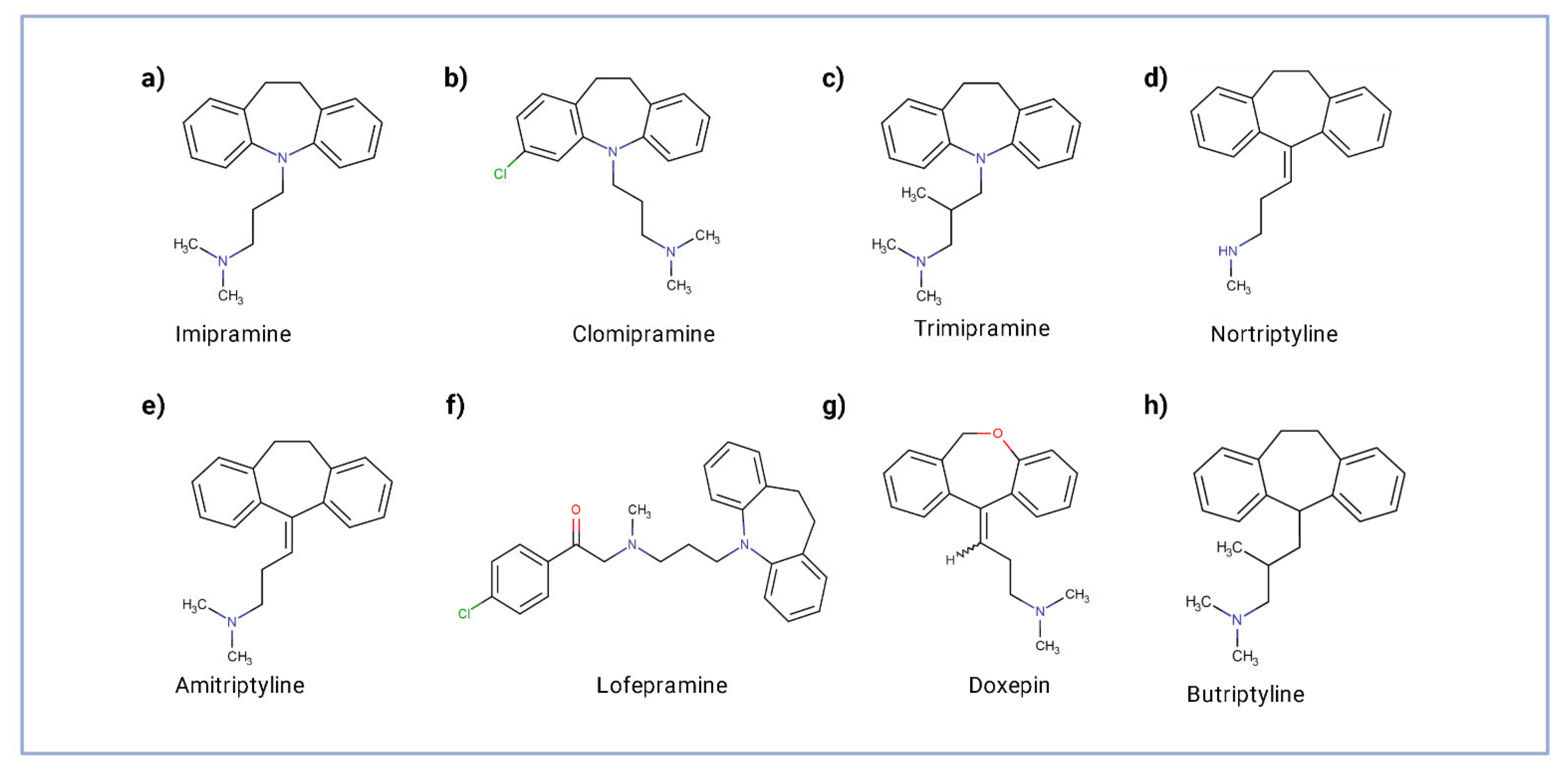
1.2. TCA Mechanisms of Action
2. Safety and Central Effects of Antidepressant in Oncology Patients
2.1. Cancer Risk and Safety of TCAs
2.2. Central Effects of TCA against Neuropathic Pain
3. In Vitro and Preclinical Evidence of Antitumoral Properties of Tricyclic Antidepressants

{kind=link}
{kind=link}
| Tumor | Compound | Targets of TCA | Effects | Reference |
|---|---|---|---|---|
| Glioblastoma | Imipramine | Extrinsic/intrinsic pathways and suppression of ERK/NF-κB signaling. | Induction of apoptosis. | [55] |
| Inhibition of yes-associated protein (YAP), independent of Hippo pathway. | Suppression of tumor proliferation. Reduced orthotopic tumor progression and prolonged survival of tumor-bearing mice. | [56] | ||
| PI3K/Akt/mTOR signaling. | Autophagic cell death. | [57] | ||
| Amitriptyline Imipramine | p65 NF-κB expression. | Partially reversion of mitochondrial abnormalities. | [58] | |
| Silencing of the glioma stem cells’ profile. | Partially reversion of the malignant phenotype. | [59] | ||
| Imipramine blue followed by liposomal doxorubicin | Profilin-1, scinderin, α-actin, calgranulin, and RhoGDP dissociation inhibitor α. | Reduction in actin fiber Formation. | [60] | |
| Imipramine + ticlopidine | Imipramine activates adenylate cyclase and induces cAMP-mediated autophagy. | By elevating cAMP levels via distinct mechanisms, combined therapy increased autophagic flux. | [61] | |
| Clomipramine, norclomipramine, amitriptyline, and doxepin | Potent inhibitors of cellular respiration. Inhibition of complex III of the mitochondrial respiratory chain. | Increasing cell death. | [62] | |
| Clomipramine + imatinib | Inhibits complex-III of the respiratory chain, resulting in increased ROS, cytochrome C release and caspase-activated apoptosis. | Inhibition of cell growth and enhanced cell death. Synergistic apoptosis. There was also a synergistic effect in autophagy by the combination. | [63] | |
| Sonic Hedgehog Medulloblastoma | Imipramine blue in liposomal nanoparticle (liposome–IB) | NADPH oxidase (NOX) family. | Dose-dependent decrease in SHH MB cell viability and migration. Inhibition of tumor growth. Reduced tumor volume. Complete tumor response. Improved survival. | [64] |
| Neuroblastoma | Imipramine | Potentiates ER-stress-induced death of SH-SY5Y cells. | Concentration-dependent reduction of the relative viability. | [65] |
| Clomipramine + vinorelbine | Capable of potentiating vinorelbine cytotoxicity. Leads to ROS production through inhibition of complex III of the respiratory chain, resulting in increased ROS, mitochondria damage, cytochrome C release, and caspase- activated apoptosis of tumorigenic cell lines. | Increased the percentage of apoptotic cells. | [66] | |
| Breast cancer | Imipramine blue + nanoparticle-based delivery approach | Inhibition of FoxM1. | Blockage of the ability of repair DNA strand breaks by homologous recombination (HR). | [67] |
| Amitriptyline | Unknown. | Reduced viability. | [68] | |
| Clomipramine | Inhibition of distinct ubiquitin E3 ligases. Specifically blocks ITCH auto-ubiquitylation, as well as p73 ubiquitylation. | Reduces cancer cell growth and synergizes with gemcitabine or mitomycin in killing cancer cells by blocking autophagy. | [69] | |
| Imipramine | Able to cause changes in the structural organization of the phosphatidylserine bilayer and that these changes correlate with their MDR-reversing activity and potency to inhibit PKC. | Inhibition of either the cell growth or protein kinase C (PKC) in MCF7 and P338 doxorubicin resistant cells. | [70] | |
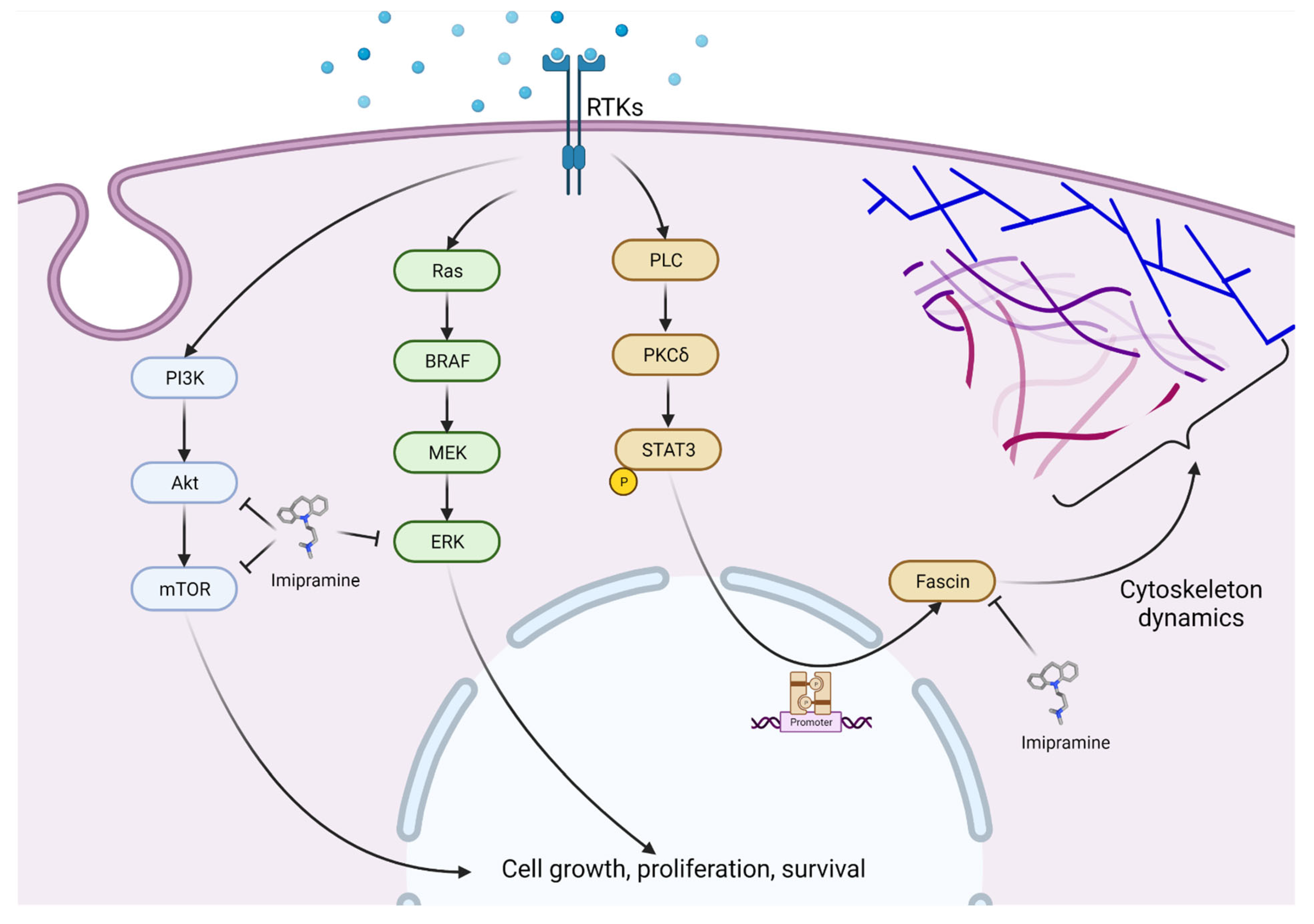
| Colorectal cancer | Imipramine | Fascin1 inhibition. | Dose-dependent anti-invasive and antimetastatic activities. | [71] |
| Head and neck squamous cell carcinoma | Imipramine blue | Inhibition of Twist1-mediated let-7i downregulation and Rac1 activation and the EMT signaling. | Represses mesenchymal-mode migration in two-and-a-half-dimensional/3D culture system | [72] |
| Lung Cancer | Imipramine | EGFR/PKC-δ/NF-κB pathway suppression in non-small-cell lung cancer. | Induced apoptosis of NSCLC cells via both intrinsic and extrinsic apoptosis signaling. DNA damage increased. Invasion and migration of NSCLC cells suppressed by imipramine. | [73] |
| Amitriptyline | Increases death receptor (DR) 4 and 5 expression, a requirement for TRAIL-induced cell death. | Blockage of autophagy by inhibiting the fusion of autophagosomes with lysosomes. | [74] | |
| Desmethylclomipramine | Inhibits in vitro the E3 ubiquitin ligase Itch. | Inhibits lung cancer stem cells’ growth, decreases their stemness potential, and increases the cytotoxic effect of conventional chemotherapeutic drugs. | [75] | |
| Acute myeloid leukemia | Imipramine blue + pimozide | Induces calcium release from the ER/lysosomes and can inhibit tyrosine phosphorylation of STAT5. | Important calcium channel blocker activity converging with IB on mitochondrial oxidative metabolism. | [76] |
| Lymphoma | Imipramine blue | Inhibition of NADPH oxidase NOX4 in Burkitt lymphoma. | Potent growth inhibition. | [77] |
| Clomipramine | SERT-binding (SERT/SLC6A4) | Promoted growth arrest of chronic lymphocytic leukemia (CLL), Small lymphocytic lymphoma (SLL), mantle cell lymphoma (MCL), follicular lymphoma (FL), and diffuse large B cell lymphoma (DLBCL). | [78] | |
| Imipramine dimers | Inhibition of the human serotonin transporter (hSERT). | Induction of cell death. | [79] | |
| Bladder cancer | Clomipramine | Inhibition of distinct ubiquitin E3 ligases. Specifically blocks ITCH auto-ubiquitylation, as well as p73 ubiquitylation. | Reduces cancer cell growth and synergizes with gemcitabine or mitomycin in killing cancer cells by blocking autophagy. | [69] |
| Prostate cancer | Imipramine | Suppression of AKT and NF-κB-related signaling proteins and secretion of tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β), and monocyte chemoattractant protein-1 (MCP-1). | Attenuated cell viability, migration, and invasion. | [80] |
| Eag1 channel protein expression. | Inhibition of the flow thought the channel. | [81] | ||
| Clomipramine | Inhibition of distinct ubiquitin E3 ligases. Specifically blocks ITCH auto-ubiquitylation, as well as p73 ubiquitylation. | Reduces cancer cell growth and synergizes with gemcitabine or mitomycin in killing cancer cells by blocking autophagy. | [69] | |
| Inhibition of autophagy. | Effective in inhibiting autophagy and enhanced therapeutic response in ENZA-resistant cells in vitro and in vivo, using the orthotopic xenograft model combined with ENZA. | [82] | ||
| Melanoma | Amitriptyline, nortriptyline, and clomipramine | Inhibition of complex III of the mitochondria has been postulated as a mechanism of action. | All three agents showed increasing inhibition with increasing concentration in both cell lines and primary cell cultures. | [83] |
| Imipramine | Ether à go-go (hEAG) channels and Ca2+ -activated channels (KCa) of the IK/SK type. | Increasing concentrations of imipramine reduced the proliferation of IGR1 cells. | [84] | |
| Hepatocellular carcinoma | Amitriptyline | Inhibition of β-catenin and Ki-67. | Decreases β-catenin-induced liver enlargement in zebrafish. Decreases tumor burden in a mouse HCC model. Amitriptyline treatment significantly decreases tumor cell proliferation, due to a reduction in the amount of Ki-67. | [85] |
| Desipramine | Inhibition of the phosphorylation of ERK1/2, JNK, and p38. | Increases ROS generation and cell death in a dose-dependent manner. Loss of mitochondrial membrane potential. | [86] | |
| Osteosarcoma | Desipramine and Nortriptyline | Calcium homeostasis; | Causes a rapid and sustained rise of intracellular Ca2+ in a concentration-dependent manner. | [87,88] |
| Desipramine | p38 MAPK-associated activation of caspase 3. | Causes Ca2+-independent apoptosis. | [89] | |
| Multiple myeloma | Amitriptyline | Decreases histone deacetylases’ expression and inhibits their activity (HDAC3, -6, -7, and -8). Induces p53, activates caspase 3, and decreases antiapoptotic Bcl-2 and Mcl-1 in tumor tissues. | Amitriptyline induces cell apoptosis. Oral administration decreases tumor growth in two MM xenograft models derived from murine and human cells. | [90,91] |
| Nortriptyline | Most likely the target would be organic cation transport machinery. | Dose- and time-dependent toxicity on cells. Arrests cell cycle at G2/M phase. Causes mitochondrial membrane depolarization. Increases caspase-3 activity. Induction of apoptosis. | [92] |
3.1. Cancer of Central Nervous System
3.2. Breast Cancer
3.3. Colorectal Cancer
3.4. Head and Neck Cancer
3.5. Lung Cancer
3.6. Acute Myeloid Leukemia
3.7. Lymphoma
3.8. Bladder Cancer
3.9. Prostate Cancer
3.10. Melanoma
3.11. Hepatocellular Carcinoma
3.12. Osteosarcoma
3.13. Multiple Myeloma
4. Clinical Evidence of Antitumoral Properties of Antidepressants
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Magnon, C.; Hall, S.J.; Lin, J.; Xue, X.; Gerber, L.; Freedland, S.J.; Frenette, P.S. Autonomic nerve development contributes to prostate cancer progression. Science 2013, 341, 1236361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saloman, J.L.; Albers, K.M.; Li, D.; Hartman, D.J.; Crawford, H.C.; Muha, E.A.; Rhim, A.D.; Davis, B.M. Ablation of sensory neurons in a genetic model of pancreatic ductal adenocarcinoma slows initiation and progression of cancer. Proc. Natl. Acad. Sci. USA 2016, 113, 3078–3083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faulkner, S.; Jobling, P.; March, B.; Jiang, C.C.; Hondermarck, H. Tumor neurobiology and the war of nerves in cancer. Cancer Discov. 2019, 9, 702–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renz, B.W.; Takahashi, R.; Tanaka, T.; Macchini, M.; Hayakawa, Y.; Dantes, Z.; Maurer, H.C.; Chen, X.; Jiang, Z.; Westphalen, C.B.; et al. β2 Adrenergic-Neurotrophin Feedforward Loop Promotes Pancreatic Cancer. Cancer Cell 2018, 33, 75–90.e7. [Google Scholar] [CrossRef] [Green Version]
- Zhao, C.M.; Hayakawa, Y.; Kodama, Y.; Muthupalani, S.; Westphalen, C.B.; Andersen, G.T.; Flatberg, A.; Johannessen, H.; Friedman, R.A.; Renz, B.W.; et al. Denervation suppresses gastric tumorigenesis. Sci. Transl. Med. 2014, 6, 1458–1473. [Google Scholar] [CrossRef] [Green Version]
- Hillhouse, T.M.; Porter, J.H. A brief history of the development of antidepressant drugs: From monoamines to glutamate. Exp. Clin. Psychopharmacol. 2015, 23, 1–21. [Google Scholar] [CrossRef]
- Richelson, E. Antimuscarinic and other receptor-blocking properties of antidepressants. Mayo Clin. Proc. 1983, 58, 40–46. [Google Scholar]
- Lee, H.C.; Chiu, W.C.; Wang, T.N.; Liao, Y.T.; Chien, I.C.; Lee, Y.; McIntyre, R.S.; Chen, P.C.; Chen, V.C.H. Antidepressants and colorectal cancer: A population-based nested case-control study. J. Affect. Disord. 2017, 207, 353–358. [Google Scholar] [CrossRef]
- Xu, W.; Tamim, H.; Shapiro, S.; Stang, M.R.; Collet, J.P. Use of antidepressants and risk of colorectal cancer: A nested case-control study. Lancet Oncol. 2006, 7, 301–308. [Google Scholar] [CrossRef]
- Coogan, P.F.; Strom, B.L.; Rosenberg, L. Antidepressant use and colorectal cancer risk. Pharmacoepidemiol. Drug Saf. 2009, 18, 1111–1114. [Google Scholar] [CrossRef] [Green Version]
- Chung, C.M.; Kuo, T.M.; Chiang, S.L.; Wang, Z.H.; Hung, C.C.; Lane, H.Y.; Liu, C.S.; Ko, Y.C. Antidepressants in association with reducing risk of oral cancer occurrence: A nationwide population-based cohort and nested case-control studies. Oncotarget 2016, 7, 11687–11695. [Google Scholar] [CrossRef]
- Mørch, L.S.; Dehlendorff, C.; Baandrup, L.; Friis, S.; Kjær, S.K. Use of antidepressants and risk of epithelial ovarian cancer. Int. J. Cancer 2017, 141, 2197–2203. [Google Scholar] [CrossRef]
- Huo, Y.L.; Qiao, J.M.; Gao, S. Association between antidepressant medication use and epithelial ovarian cancer risk: A systematic review and meta-analysis of observational studies. Br. J. Clin. Pharmacol. 2018, 84, 649–658. [Google Scholar] [CrossRef] [Green Version]
- Chen, V.C.H.; Liao, Y.T.; Yeh, D.C.; Tseng, H.C.; Stewart, R.; Lee, C.T.C. Relationship between antidepressant prescription and breast cancer: A population based study in Taiwan. Psychooncology 2016, 25, 803–807. [Google Scholar] [CrossRef]
- Chien, C.; Li, C.I.; Heckbert, S.R.; Malone, K.E.; Boudreau, D.M.; Daling, J.R. Antidepressant use and breast cancer risk. Breast Cancer Res. Treat. 2006, 95, 131–140. [Google Scholar] [CrossRef]
- González-Pérez, A.; García Rodríguez, L.A. Breast cancer risk among users of antidepressant medications. Epidemiology 2005, 16, 101–105. [Google Scholar] [CrossRef]
- Coogan, P.F. Review of the epidemiological literature on antidepressant use and breast cancer risk. Expert Rev. Neurother. 2006, 6, 1363–1374. [Google Scholar] [CrossRef]
- Pasquini, M.; Berardelli, I.; Calabrò, F.; Roselli, V.; Hefner, S.; Biondi, M. Is amisulpride safe when prescribed to breast and prostate cancer patients? Med. Hypotheses 2013, 81, 1146–1150. [Google Scholar] [CrossRef]
- Lin, W.Y.; Chen, V.C.H.; Chiu, W.C.; Yim, S.J.; Ho, P.T.; McIntyre, R.S.; Lu, M.L.; Wu, S.I. Prostate cancer and antidepressants: A nationwide population-based nested case-control study. J. Affect. Disord. 2018, 227, 834–839. [Google Scholar] [CrossRef]
- Hsieh, Y.H.; Chiu, W.C.; Lin, C.F.; Chan, H.L.; Liang, H.Y.; Lee, Y.; McIntyre, R.S.; Chen, V.C.H. Antidepressants and gastric cancer: A nationwide population-based nested case-control study. PLoS ONE 2015, 10, e0143668. [Google Scholar] [CrossRef]
- Dalton, S.O.; Johansen, C.; Mellemkjær, L.; Sørensen, H.T.; McLaughlin, J.K.; Olsen, J.; Olsen, J.H. Antidepressant medications and risk for cancer. Epidemiology 2000, 11, 171–176. [Google Scholar] [CrossRef]
- Lowry, S.J.; Chubak, J.; Press, O.W.; McKnight, B.; Weiss, N.S. Risk of non-Hodgkin lymphoma in relation to tricyclic antidepressant use. Ann. Epidemiol. 2013, 23, 349–354. [Google Scholar] [CrossRef] [Green Version]
- Walker, A.J.; Card, T.; Bates, T.E.; Muir, K. Tricyclic antidepressants and the incidence of certain cancers: A study using the GPRD. Br. J. Cancer 2011, 104, 193–197. [Google Scholar] [CrossRef] [Green Version]
- Pottegard, A.; Rodríguez, L.A.G.; Rasmussen, L.; Damkier, P.; Friis, S.; Gaist, D. Use of tricyclic antidepressants and risk of glioma: A nationwide case-control study. Br. J. Cancer 2016, 114, 1265–1268. [Google Scholar] [CrossRef] [Green Version]
- AZIMA, H.; VISPO, R.H. Imipramine: A potent new anti-depressant compound. Am. J. Psychiatry 1958, 115, 245–246. [Google Scholar] [CrossRef]
- Dharmshaktu, P.; Tayal, V.; Kalra, B.S. Efficacy of antidepressants as analgesics: A review. J. Clin. Pharmacol. 2012, 52, 6–17. [Google Scholar] [CrossRef]
- Micó, J.A.; Ardid, D.; Berrocoso, E.; Eschalier, A. Antidepressants and pain. Trends Pharmacol. Sci. 2006, 27, 348–354. [Google Scholar] [CrossRef]
- Onghena, P.; Van Houdenhove, B. Antidepressant-induced analgesia in chronic non-malignant pain: A meta-analysis of 39 placebo-controlled studies. Pain 1992, 49, 205–219. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Magni, G.; Conlon, P.; Arsie, D. Tricyclic antidepressants in the treatment of cancer pain: A review. Pharmacopsychiatry 1987, 20, 160–164. [Google Scholar] [CrossRef]
- Egbunike, I.G.; Chaffee, B.J. Antidepressants in the Management of Chronic Pain Syndromes. Pharmacother. J. Hum. Pharmacol. Drug Ther. 1990, 10, 262–270. [Google Scholar] [CrossRef]
- Obata, H. Analgesic mechanisms of antidepressants for neuropathic pain. Int. J. Mol. Sci. 2017, 18, 2483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, S.; Bhatnagar, S.; Goyal, G.N.; Rana, S.P.S.; Upadhya, S.P. A Comparative Efficacy of Amitriptyline, Gabapentin, and Pregabalin in Neuropathic Cancer Pain: A Prospective Randomized Double-Blind Placebo-Controlled Study. Am. J. Hosp. Palliat. Med. 2012, 29, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Bhatnagar, S.; Gupta, D.; Nirwani Goyal, G.; Jain, R.; Chauhan, H. Management of neuropathic cancer pain following WHO analgesic ladder: A prospective study. Am. J. Hosp. Palliat. Med. 2009, 25, 447–451. [Google Scholar] [CrossRef]
- Ventafridda, V.; Bonezzi, C.; Caraceni, A.; De Conno, F.; Guarise, G.; Ramella, G.; Saita, L.; Silvani, V.; Tamburini, M.; Toscani, F. Antidepressants for cancer pain and other painful syndromes with deafferentation component: Comparison of Amitriptyline and Trazodone. Ital. J. Neurol. Sci. 1987, 8, 579–587. [Google Scholar] [CrossRef]
- Kautio, A.L.; Haanpää, M.; Saarto, T.; Kalso, E. Amitriptyline in the Treatment of Chemotherapy-Induced Neuropathic Symptoms. J. Pain Symptom Manag. 2008, 35, 31–39. [Google Scholar] [CrossRef]
- Arai, Y.C.P.; Matsubara, T.; Shimo, K.; Suetomi, K.; Nishihara, M.; Ushida, T.; Kobayashi, K.; Suzuki, C.; Kinoshita, A.; Kondo, M.; et al. Low-dose gabapentin as useful adjuvant to opioids for neuropathic cancer pain when combined with low-dose imipramine. J. Anesth. 2010, 24, 407–410. [Google Scholar] [CrossRef]
- Kast, R.E. Mirtazapine may be useful in treating nausea and insomnia of cancer chemotherapy. Support. Care Cancer 2001, 9, 469–470. [Google Scholar] [CrossRef]
- Theobald, D.E.; Kirsh, K.L.; Holtsclaw, E.; Donaghy, K.; Passik, S.D. An open-label, crossover trial of mirtazapine (15 and 30 mg) in cancer patients with pain and other distressing symptoms. J. Pain Symptom Manag. 2002, 23, 442–447. [Google Scholar] [CrossRef]
- Fradkin, M.; Batash, R.; Elmaleh, S.; Debi, R.; Schaffer, P.; Schaffer, M.; Asna, N. Management of Peripheral Neuropathy Induced by Chemotherapy. Curr. Med. Chem. 2019, 26, 4698–4708. [Google Scholar] [CrossRef]
- Evans, D.L.; McCartney, C.F.; Haggerty, J.J.; Nemeroff, C.B.; Golden, R.N.; Simon, J.B.; Quade, D.; Holmes, V.; Droba, M.; Mason, G.A.; et al. Treatment of depression in cancer patients is associated with better life adaptation: A pilot study. Psychosom. Med. 1988, 50, 72–76. [Google Scholar] [CrossRef]
- Holland, J.C.; Romance, S.J.; Heiligenstein, J.H.; Terner, R.G.; Wilson, M.G. A controlled trial of fluoxetine and desipramine in depressed women with advanced cancer. Psychooncology 1998, 7, 291–300. [Google Scholar] [CrossRef]
- Moslinger-Gehmayr, R.; Zaninelli, R.; Contu, A.; Oberhoff, C.; Gutschow, K.; Schindler, A.E.; Staab, H.J. Eine doppelblinde vergleichsstudie zur wirksamkeit und vertraglichkeit von paroxetin und amitriptylin bei der behandlung von brustkrebs-Patientinnen mit klinisch nachgewiesener depression. Zentralbl. Gynakol. 2000, 122, 195–202. [Google Scholar]
- Pezzella, G.; Moslinger-Gehmayr, R.; Contu, A. Treatment of depression in patients with breast cancer: A comparison between paroxetine and amitriptyline. Breast Cancer Res. Treat. 2001, 70, 1–10. [Google Scholar] [CrossRef]
- Riblet, N.; Larson, R.; Watts, B.V.; Holtzheimer, P. Reevaluating the role of antidepressants in cancer-related depression: A systematic review and meta-analysis. Gen. Hosp. Psychiatry 2014, 36, 466–473. [Google Scholar] [CrossRef]
- Raddin, R.S.; Park, E.M.; Hamer, R.M.; Nelson, K.M.; Mayer, D.K.; Rosenstein, D.L.; Bernard, S.A. A pilot study to evaluate symptom-oriented selection of antidepressants in patients with cancer. J. Palliat. Med. 2014, 17, 167–175. [Google Scholar] [CrossRef]
- Ostuzzi, G.; Matcham, F.; Dauchy, S.; Barbui, C.; Hotopf, M. Antidepressants for the treatment of depression in people with cancer. Cochrane Database Syst. Rev. 2018, 2018, CD011006. [Google Scholar] [CrossRef]
- Fallon, M.T.; Wilcock, A.; Kelly, C.A.; Paul, J.; Lewsley, L.-A.; Norrie, J.; Laird, B.J.A. Oral Ketamine vs Placebo in Patients With Cancer-Related Neuropathic Pain: A Randomized Clinical Trial. JAMA Oncol. 2018, 4, 870–872. [Google Scholar] [CrossRef] [Green Version]
- Gewandter, J.S.; Mohile, S.G.; Heckler, C.E.; Ryan, J.L.; Kirshner, J.J.; Flynn, P.J.; Hopkins, J.O.; Morrow, G.R. A phase III randomized, placebo-controlled study of topical amitriptyline and ketamine for chemotherapy-induced peripheral neuropathy (CIPN): A University of Rochester CCOP study of 462 cancer survivors. Support. Care Cancer 2014, 22, 1807–1814. [Google Scholar] [CrossRef] [Green Version]
- Barton, D.L.; Wos, E.J.; Qin, R.; Mattar, B.I.; Green, N.B.; Lanier, K.S.; Bearden, J.D.; Kugler, J.W.; Hoff, K.L.; Reddy, P.S.; et al. A double-blind, placebo-controlled trial of a topical treatment for chemotherapy-induced peripheral neuropathy: NCCTG trial N06CA. Support. Care Cancer 2011, 19, 833–841. [Google Scholar] [CrossRef] [Green Version]
- Wolf, S.L.; Barton, D.L.; Qin, R.; Wos, E.J.; Sloan, J.A.; Liu, H.; Aaronson, N.K.; Satele, D.V.; Mattar, B.I.; Green, N.B.; et al. The relationship between numbness, tingling, and shooting/burning pain in patients with chemotherapy-induced peripheral neuropathy (CIPN) as measured by the EORTC QLQ-CIPN20 instrument, N06CA. Support. Care Cancer 2012, 20, 625–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashioka, S.; Klegeris, A.; Monji, A.; Kato, T.; Sawada, M.; McGeer, P.L.; Kanba, S. Antidepressants inhibit interferon-gamma-induced microglial production of IL-6 and nitric oxide. Exp. Neurol. 2007, 206, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Zheng, L.T.; Ock, J.; Lee, M.G.; Kim, S.H.; Lee, H.W.; Lee, W.H.; Park, H.C.; Suk, K. Inhibition of glial inflammatory activation and neurotoxicity by tricyclic antidepressants. Neuropharmacology 2008, 55, 826–834. [Google Scholar] [CrossRef] [PubMed]
- Yirmiya, R.; Rimmerman, N.; Reshef, R. Depression as a Microglial Disease. Trends Neurosci. 2015, 38, 637–658. [Google Scholar] [CrossRef]
- Hsu, F.T.; Chiang, I.T.; Wang, W.S. Induction of apoptosis through extrinsic/intrinsic pathways and suppression of ERK/NF-κB signalling participate in anti-glioblastoma of imipramine. J. Cell. Mol. Med. 2020, 24, 3982–4000. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, X.; Wang, X.; Wu, D.; Qi, J.; Zhang, Y.; Wang, K.; Zhou, D.; Meng, Q.M.; Nie, E.; et al. Imipramine impedes glioma progression by inhibiting YAP as a Hippo pathway independent manner and synergizes with temozolomide. J. Cell. Mol. Med. 2021, 25, 9350–9363. [Google Scholar] [CrossRef]
- Jeon, S.H.; Kim, S.H.; Kim, Y.; Kim, Y.S.; Lim, Y.; Lee, Y.H.; Shin, S.Y. The tricyclic antidepressant imipramine induces autophagic cell death in U-87MG glioma cells. Biochem. Biophys. Res. Commun. 2011, 413, 311–317. [Google Scholar] [CrossRef]
- Bielecka-Wajdman, A.M.; Ludyga, T.; Machnik, G.; Gołyszny, M.; Obuchowicz, E. Tricyclic Antidepressants Modulate Stressed Mitochondria in Glioblastoma Multiforme Cells. Cancer Control 2018, 25, 1073274818798594. [Google Scholar] [CrossRef] [Green Version]
- Bielecka-Wajdman, A.M.; Lesiak, M.; Ludyga, T.; Sieroń, A.; Obuchowicz, E. Reversing glioma malignancy: A new look at the role of antidepressant drugs as adjuvant therapy for glioblastoma multiforme. Cancer Chemother. Pharmacol. 2017, 79, 1249–1256. [Google Scholar] [CrossRef]
- Munson, J.M.; Fried, L.; Rowson, S.A.; Bonner, M.Y.; Karumbaiah, L.; Diaz, B.; Courtneidge, S.A.; Knaus, U.G.; Brat, D.J.; Arbiser, J.L.; et al. Anti-invasive adjuvant therapy with imipramine blue enhances chemotherapeutic efficacy against glioma. Sci. Transl. Med. 2012, 4, 127ra36. [Google Scholar] [CrossRef]
- Shchors, K.; Massaras, A.; Hanahan, D. Dual Targeting of the Autophagic Regulatory Circuitry in Gliomas with Repurposed Drugs Elicits Cell-Lethal Autophagy and Therapeutic Benefit. Cancer Cell 2015, 28, 456–471. [Google Scholar] [CrossRef] [Green Version]
- Higgins, S.C.; Pelkington, G.J. The in vitro effects of tricyclic drugs and dexamethasone on cellular Respiration of malignant glioma. Anticancer Res. 2010, 30, 391–397. [Google Scholar]
- Bilir, A.; Erguven, M.; Oktem, G.; Ozdemir, A.; Uslu, A.; Aktas, E.; Bonavinda, B. Potentiation of cytotoxicity by combination of imatinib and chlorimipramine in glioma. Int. J. Oncol. 2008, 32, 829–839. [Google Scholar]
- Macdonald, T.J.; Liu, J.; Yu, B.; Malhotra, A.; Munson, J.; Park, J.C.; Wang, K.; Fei, B.; Bellamkonda, R.; Arbiser, J. Liposome-imipramine blue inhibits sonic hedgehog medulloblastoma in vivo. Cancers 2021, 13, 1220. [Google Scholar] [CrossRef]
- Brodnanova, M.; Hatokova, Z.; Evinova, A.; Cibulka, M.; Racay, P. Differential impact of imipramine on thapsigargin- and tunicamycin-induced endoplasmic reticulum stress and mitochondrial dysfunction in neuroblastoma SH-SY5Y cells. Eur. J. Pharmacol. 2021, 902, 174073. [Google Scholar] [CrossRef]
- Bilir, A.; Erguven, M.; Yazihan, N.; Aktas, E.; Oktem, G.; Sabanci, A. Enhancement of vinorelbine-induced cytotoxicity and apoptosis by clomipramine and lithium chloride in human neuroblastoma cancer cell line SH-SY5Y. J. Neurooncol. 2010, 100, 385–395. [Google Scholar] [CrossRef]
- Rajamanickam, S.; Panneerdoss, S.; Gorthi, A.; Timilsina, S.; Onyeagucha, B.; Kovalskyy, D.; Ivanov, D.; Hanes, M.A.; Vadlamudi, R.K.; Chen, Y.; et al. Inhibition of FoxM1-Mediated DNA repair by imipramine blue suppresses breast cancer growth and metastasis. Clin. Cancer Res. 2016, 22, 3524–3536. [Google Scholar] [CrossRef] [Green Version]
- Lei, B.; Xu, L.; Zhang, X.; Peng, W.; Tang, Q.; Feng, C. The proliferation effects of fluoxetine and amitriptyline on human breast cancer cells and the underlying molecular mechanisms. Environ. Toxicol. Pharmacol. 2021, 83, 103586. [Google Scholar] [CrossRef]
- Rossi, M.; Rotblat, B.; Ansell, K.; Amelio, I.; Caraglia, M.; Misso, G.; Bernassola, F.; Cavasotto, C.N.; Knight, R.A.; Ciechanover, A.; et al. High throughput screening for inhibitors of the HECT ubiquitin E3 ligase ITCH identifies antidepressant drugs as regulators of autophagy. Cell Death Dis. 2014, 5, e1203. [Google Scholar] [CrossRef] [Green Version]
- Pajeva, I.K.; Wiese, M.; Cordes, H.P.; Seydel, J.K. Membrane interactions of some catamphiphilic drugs and relation to their multidrug-resistance-reversing ability. J. Cancer Res. Clin. Oncol. 1996, 122, 27–40. [Google Scholar] [CrossRef]
- Alburquerque-González, B.; Bernabé-García, M.; Montoro-García, S.; Bernabé-García, Á.; Rodrigues, P.C.; Ruiz Sanz, J.; López-Calderón, F.F.; Luque, I.; Nicolas, F.J.; Cayuela, M.L.; et al. New role of the antidepressant imipramine as a Fascin1 inhibitor in colorectal cancer cells. Exp. Mol. Med. 2020, 52, 281–292. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.H.; Su, Y.H.; Hsu, W.H.; Wang, C.C.; Arbiser, J.L.; Yang, M.H. Imipramine blue halts head and neck cancer invasion through promoting F-box and leucine-rich repeat protein 14-mediated Twist1 degradation. Oncogene 2016, 35, 2287–2298. [Google Scholar] [CrossRef] [Green Version]
- Yueh, P.F.; Lee, Y.H.; Chiang, I.T.; Chen, W.T.; Lan, K.L.; Chen, C.H.; Hsu, F.T. Suppression of EGFR/PKC-δ/NF-κB Signaling Associated With Imipramine-Inhibited Progression of Non-Small Cell Lung Cancer. Front. Oncol. 2021, 11, 735183. [Google Scholar] [CrossRef]
- ZINNAH, K.M.A.; PARK, S.Y. Sensitizing TRAIL-resistant A549 lung cancer cells and enhancing TRAIL-induced apoptosis with the antidepressant amitriptyline. Oncol. Rep. 2021, 46, 144. [Google Scholar] [CrossRef]
- Bongiorno-Borbone, L.; Giacobbe, A.; Compagnone, M.; Eramo, A.; De Maria, R.; Peschiaroli, A.; Melino, G. Anti-tumoral effect of desmethylclomipramine in lung cancer stem cells. Oncotarget 2015, 6, 16926–16938. [Google Scholar] [CrossRef]
- Wang, Z.; Mi, T.; Bradley, H.L.; Metts, J.; Sabnis, H.; Zhu, W.; Arbiser, J.; Bunting, K.D. Pimozide and imipramine blue exploit mitochondrial vulnerabilities and reactive oxygen species to cooperatively target high risk acute myeloid leukemia. Antioxidants 2021, 10, 956. [Google Scholar] [CrossRef]
- Klingenberg, M.; Becker, J.; Eberth, S.; Kube, D.; Wilting, J. The NADPH oxidase inhibitor imipramine-blue in the treatment of burkitt lymphoma. Mol. Cancer Ther. 2014, 13, 833–841. [Google Scholar] [CrossRef] [Green Version]
- Chamba, A.; Holder, M.J.; Jarrett, R.F.; Shield, L.; Toellner, K.M.; Drayson, M.T.; Barnes, N.M.; Gordon, J. SLC6A4 expression and anti-proliferative responses to serotonin transporter ligands chlomipramine and fluoxetine in primary B-cell malignancies. Leuk. Res. 2010, 34, 1103–1106. [Google Scholar] [CrossRef]
- Bright, S.A.; Brinkø, A.; Larsen, M.T.; Sinning, S.; Williams, D.C.; Jensen, H.H. Basic N-interlinked imipramines show apoptotic activity against malignant cells including Burkitt’s lymphoma. Bioorganic Med. Chem. Lett. 2013, 23, 1220–1224. [Google Scholar] [CrossRef]
- Lim, E.Y.; Park, J.; Kim, Y.T.; Kim, M.J. Imipramine inhibits migration and invasion in metastatic castration-resistant prostate cancer PC-3 cells via AKT-mediated NF-κB signaling pathway. Molecules 2020, 25, 4619. [Google Scholar] [CrossRef]
- Söğüt, F.; Çömelekoğlu, Ü.; Dervişoğlu, H.; Eroğlu, P.; Yalin, S.; Yilmaz, N.Ş. Effect of imipramine on ether à-go-go potassium channel (Kv1.10) expression in DU145 prostate cancer cells. Andrologia 2022, 54, e14291. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.G.; Yang, J.C.; Kung, H.J.; Shi, X.B.; Tilki, D.; Lara, P.N.; Devere White, R.W.; Gao, A.C.; Evans, C.P. Targeting autophagy overcomes Enzalutamide resistance in castration-resistant prostate cancer cells and improves therapeutic response in a xenograft model. Oncogene 2014, 33, 4521–4530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, K.A.; Glaysher, S.; Hurren, J.; Knight, L.A.; McCormick, D.; Suovouri, A.; Amberger-Murphy, V.; Pilkington, G.J.; Cree, I.A. The effect of tricyclic antidepressants on cutaneous melanoma cell lines and primary cell cultures. Anticancer. Drugs 2012, 23, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Gavrilova-Ruch, O.; Schönherr, K.; Gessner, G.; Schönherr, R.; Klapperstück, T.; Wohlrab, W.; Heinemann, S.H. Effects of imipramine on ion channels and proliferation of IGR1 melanoma cells. J. Membr. Biol. 2002, 188, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Evason, K.J.; Francisco, M.T.; Juric, V.; Balakrishnan, S.; Lopez Pazmino, M.D.P.; Gordan, J.D.; Kakar, S.; Spitsbergen, J.; Goga, A.; Stainier, D.Y.R. Identification of Chemical Inhibitors of β-Catenin-Driven Liver Tumorigenesis in Zebrafish. PLoS Genet. 2015, 11, e1005305. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.K.; Kim, S.J. Desipramine induces apoptosis in hepatocellular carcinoma cells. Oncol. Rep. 2017, 38, 1029–1034. [Google Scholar] [CrossRef] [Green Version]
- Jan, C.R.; Lu, Y.C.; Tseng, L.L.; Jiann, B.P.; Chang, H.T.; Wang, J.L.; Chen, W.C.; Huang, J.K. Effect of the antidepressant desipramine on cytosolic Ca2+ movement and proliferation in human osteosarcoma cells. Pharmacology 2003, 69, 190–196. [Google Scholar] [CrossRef]
- Hsu, S.S.; Huang, C.J.; Chen, J.S.; Cheng, H.H.; Chang, H.T.; Jiann, B.P.; Lin, K.L.; Wang, J.L.; Ho, C.M.; Jan, C.R. Effect of nortriptyline on intracellular Ca2+ handling and proliferation in human osteosarcoma cells. Basic Clin. Pharmacol. Toxicol. 2004, 95, 124–130. [Google Scholar] [CrossRef]
- Lu, T.; Huang, C.C.; Lu, Y.C.; Lin, K.L.; Liu, S.I.; Wang, B.W.; Chang, P.M.; Chen, I.S.; Chen, S.S.; Tsai, J.Y.; et al. Desipramine-induced Ca2+-independent apoptosis in MG63 human osteosarcoma cells: Dependence on P38 mitogen-activated protein kinase-regulated activation of caspase 3. Clin. Exp. Pharmacol. Physiol. 2009, 36, 297–303. [Google Scholar] [CrossRef]
- Mao, X.; Hou, T.; Cao, B.; Wang, W.; Li, Z.; Chen, S.; Fei, M.; Hurren, R.; Gronda, M.; Wu, D.; et al. The tricyclic antidepressant amitriptyline inhibits D-cyclin transactivation and induces myeloma cell apoptosis by inhibiting histone deacetylases: In vitro and in silico evidence. Mol. Pharmacol. 2011, 79, 672–680. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Du, X.; Zhao, C.; Cao, B.; Zhao, Y.; Mao, X. The antidepressant amitriptyline shows potent therapeutic activity against multiple myeloma. Anticancer. Drugs 2013, 24, 792–798. [Google Scholar] [CrossRef]
- Biber, A.; Durusu, İ.Z.; Özen, C. In vitro anticancer effect of tricyclic antidepressant nortriptyline on multiple myeloma. Turkish J. Biol. 2018, 42, 414–421. [Google Scholar] [CrossRef]
- Abadi, B.; Shahsavani, Y.; Faramarzpour, M.; Rezaei, N.; Rahimi, H.R. Antidepressants with anti-tumor potential in treating glioblastoma: A narrative review. Fundam. Clin. Pharmacol. 2022, 36, 35–48. [Google Scholar] [CrossRef]
- Richelson, E. Tricyclic antidepressants block histamine H1 receptors of mouse neuroblastoma cells. Nature 1978, 274, 176–177. [Google Scholar] [CrossRef]
- Albouz, S.; Hauw, J.J.; Berwald-Netter, Y.; Boutry, J.M.; Bourdon, R.; Baumann, N. Tricyclic antidepressants induce sphingomyelinase deficiency in fibroblast and neuroblastoma cell cultures. Biomedicine 1981, 35, 218–220. [Google Scholar]
- Nakaki, T.; Roth, B.L.; Chuang, D.-M.; Costa, E. 5-Hydroxytryptamine Uptake and Imipramine Binding Sites in Neurotumor NCB-20 Cells. J. Neurochem. 1985, 45, 920–925. [Google Scholar] [CrossRef]
- Ogata, N.; Yoshii, M.; Narahashi, T. Psychotropic drug block voltage-gated ion channels in neuroblastoma cells. Brain Res. 1989, 476, 140–144. [Google Scholar] [CrossRef]
- Carignani, C.; Corsi, M. Inhibition of SK3 channels in the TE671 human medulloblastoma cell line by desipramine and imipramine. Eur. J. Pharmacol. 2002, 448, 139–142. [Google Scholar] [CrossRef]
- Slamon, D.N.; Ward, T.H.; Butler, J.; Pentreath, V.W. Assessment of DNA damage in C6 glioma cells after antidepressant treatment using an alkaline comet assay. Arch. Toxicol. 2001, 75, 243–250. [Google Scholar] [CrossRef]
- Qi, H.; Chen, H.Z.; Jin, Z.J. Caspase 3 gene expression and [Ca2+]i homeostasis underlying desipramine-induced C6 glioma cell apoptosis. Acta Pharmacol. Sin. 2002, 23, 803–807. [Google Scholar]
- Levkovitz, Y.; Gil-Ad, I.; Zeldich, E.; Dayag, M.; Weizman, A. Differential induction of apoptosis by antidepressants in glioma and neuroblastoma cell lines: Evidence for p-c-Jun, cytochrome c, and caspase-3 involvement. J. Mol. Neurosci. 2005, 27, 29–42. [Google Scholar] [CrossRef]
- Ma, J.; Qiu, Y.; Yang, L.; Peng, L.; Xia, Z.; Hou, L.N.; Fang, C.; Qi, H.; Chen, H.Z. Desipramine induces apoptosis in rat glioma cells via endoplasmic reticulum stress-dependent CHOP pathway. J. Neurooncol. 2011, 101, 41–48. [Google Scholar] [CrossRef]
- Ma, J.; Hou, L.-N.; Rong, Z.-X.; Liang, P.; Fang, C.; Li, H.-F.; Qi, H.; Chen, H.-Z. Antidepressant Desipramine Leads to C6 Glioma Cell Autophagy: Implication for the Adjuvant Therapy of Cancer. Anticancer. Agents Med. Chem. 2013, 13, 254–260. [Google Scholar] [CrossRef]
- Zhu, M.Y.; Wang, W.P.; Baldessarini, R.J.; Kim, K.S. Effects of desipramine treatment on tyrosine hydroxylase gene expression in cultured neuroblastoma cells and rat brain tissue. Mol. Brain Res. 2005, 133, 167–175. [Google Scholar] [CrossRef]
- Hisaoka, K.; Maeda, N.; Tsuchioka, M.; Takebayashi, M. Antidepressants induce acute CREB phosphorylation and CRE-mediated gene expression in glial cells: A possible contribution to GDNF production. Brain Res. 2008, 1196, 53–58. [Google Scholar] [CrossRef]
- Hisaoka-Nakashima, K.; Miyano, K.; Matsumoto, C.; Kajitani, N.; Abe, H.; Okada-Tsuchioka, M.; Yokoyama, A.; Uezono, Y.; Morioka, N.; Nakata, Y.; et al. Tricyclic antidepressant amitriptyline-induced glial cell linederived neurotrophic factor production involves pertussis toxin-sensitive Gαi/o activation in astroglial cells. J. Biol. Chem. 2015, 290, 13678–13691. [Google Scholar] [CrossRef] [Green Version]
- Koehler, A.; Karve, A.; Desai, P.; Arbiser, J.; Plas, D.R.; Qi, X.; Read, R.D.; Sasaki, A.T.; Gawali, V.S.; Toukam, D.K.; et al. Reuse of molecules for glioblastoma therapy. Pharmaceuticals 2021, 14, 99. [Google Scholar] [CrossRef]
- Lucki, A.; Klein, E.; Karry, R.; Ben-Shachar, D. Dexamethasone in the presence of desipramine enhances MAPK/ERK1/2 signaling possibly via its interference with β-arrestin. J. Neural Transm. 2014, 121, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Lieberknecht, V.; Engel, D.; Rodrigues, A.L.S.; Gabilan, N.H. Neuroprotective effects of mirtazapine and imipramine and their effect in pro- and anti-apoptotic gene expression in human neuroblastoma cells. Pharmacol. Reports 2020, 72, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Cong, Q.X.; Zhang, S.G.; Zhai, X.W.; Li, H.F.; Li, S.Q. High expression levels of fascin-1 protein in human gliomas and its clinical relevance. Open Med. 2018, 13, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Timilsina, S.; Rajamanickam, S.; Rao, A.D.; Subbarayalu, P.; Nirzhor, S.; Abdelfattah, N.; Viswanadhapalli, S.; Chen, Y.; Jatoi, I.; Brenner, A.; et al. The antidepressant imipramine inhibits breast cancer growth by targeting estrogen receptor signaling and DNA repair events. Cancer Lett. 2022, 540, 215717. [Google Scholar] [CrossRef]
- Wang, C.Q.; Tang, C.H.; Chang, H.T.; Li, X.N.; Zhao, Y.M.; Su, C.M.; Hu, G.N.; Zhang, T.; Sun, X.X.; Zeng, Y.; et al. Fascin-1 as a novel diagnostic marker of triple-negative breast cancer. Cancer Med. 2016, 5, 1983–1988. [Google Scholar] [CrossRef]
- Esnakula, A.K.; Ricks-Santi, L.; Kwagyan, J.; Kanaan, Y.M.; DeWitty, R.L.; Wilson, L.L.; Gold, B.; Frederick, W.A.I.; Naab, T.J. Strong association of fascin expression with triple negative breast cancer and basal-like phenotype in African-American women. J. Clin. Pathol. 2014, 67, 153–160. [Google Scholar] [CrossRef]
- Rodríguez-Pinilla, S.M.; Sarrió, D.; Honrado, E.; Hardisson, D.; Calero, F.; Benitez, J.; Palacios, J. Prognostic significance of basal-like phenotype and fascin expression in node-negative invasive breast carcinomas. Clin. Cancer Res. 2006, 12, 1533–1539. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Ng, A.S.; Cai, S.; Li, Q.; Yang, L.; Kerr, D. Novel therapeutic strategies: Targeting epithelial–mesenchymal transition in colorectal cancer. Lancet Oncol. 2021, 22, e358–e368. [Google Scholar] [CrossRef]
- Arimochi, H.; Morita, K. Characterization of cytotoxic actions of tricyclic antidepressants on human HT29 colon carcinoma cells. Eur. J. Pharmacol. 2006, 541, 17–23. [Google Scholar] [CrossRef]
- Kraft, R.; Kahn, A.; Medina-Franco, J.L.; Orlowski, M.L.; Baynes, C.; López-Vallejo, F.; Barnard, K.; Maggiora, G.M.; Restifo, L.L. A cell-based fascin bioassay identifies compounds with potential anti-metastasis or cognition-enhancing functions. DMM Dis. Model. Mech. 2013, 6, 217–235. [Google Scholar] [CrossRef] [Green Version]
- Montoro-García, S.; Alburquerque-González, B.; Bernabé-García, Á.; Bernabé-García, M.; Rodrigues, P.C.; den-Haan, H.; Luque, I.; Nicolás, F.J.; Pérez-Sánchez, H.; Cayuela, M.L.; et al. Novel anti-invasive properties of a Fascin1 inhibitor on colorectal cancer cells. J. Mol. Med. 2020, 98, 383–394. [Google Scholar] [CrossRef]
- Snyder, M.; Huang, X.Y.; Zhang, J.J. Signal Transducers and Activators of Transcription 3 (STAT3) directly regulates cytokine-induced fascin expression and is required for breast cancer cell migration. J. Biol. Chem. 2011, 286, 38886–38893. [Google Scholar] [CrossRef] [Green Version]
- Lii, C.K.; Chang, J.W.; Chen, J.J.; Chen, H.W.; Liu, K.L.; Yeh, S.L.; Wang, T.S.; Liu, S.H.; Tsai, C.H.; Li, C.C. Docosahexaenoic acid inhibits 12-O-tetradecanoylphorbol-13-acetate-induced fascin-1-dependent breast cancer cell migration by suppressing the PKCδ- and Wnt-1/β-catenin-mediated pathways. Oncotarget 2016, 7, 25162–25179. [Google Scholar] [CrossRef] [Green Version]
- Yao, J.; Qian, C.J.; Ye, B.; Zhao, Z.Q.; Wei, J.; Liang, Y.; Zhang, X. Signal transducer and activator of transcription 3 signaling upregulates fascin via nuclear factor-κB in gastric cancer: Implications in cell invasion and migration. Oncol. Lett. 2014, 7, 902–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, X.; Gao, S.; Sun, W.; Zhang, H.; Sun, J.; Yang, S.; Hao, J. Hypoxia-Inducible factor-1 promotes pancreatic ductal adenocarcinoma invasion and metastasis by activating transcription of the actin-Bundling protein fascin. Cancer Res. 2014, 74, 2455–2464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabolizadeh, P.; Engelmann, B.J.; Pullen, N.; Stewart, J.K.; Ryan, J.J.; Farrell, N.P. Platinum anticancer agents and antidepressants: Desipramine enhances platinum-based cytotoxicity in human colon cancer cells. J. Biol. Inorg. Chem. 2012, 17, 123–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahchan, N.S.; Dudley, J.T.; Mazur, P.K.; Flores, N.; Yang, D.; Palmerton, A.; Zmoos, A.F.; Vaka, D.; Tran, K.Q.T.; Zhou, M.; et al. A drug repositioning approach identifies tricyclic antidepressants as inhibitors of small cell lung cancer and other neuroendocrine tumors. Cancer Discov. 2013, 3, 1364–1377. [Google Scholar] [CrossRef] [Green Version]
- Lohinai, Z.; Dome, P.; Szilagyi, Z.; Ostoros, G.; Moldvay, J.; Hegedus, B.; Dome, B.; Weiss, G.J. From bench to bedside: Attempt to evaluate repositioning of drugs in the treatment of metastatic small cell lung cancer (SCLC). PLoS ONE 2016, 11, e0144797. [Google Scholar] [CrossRef] [Green Version]
- Metts, J.; Bradley, H.L.; Wang, Z.; Shah, N.P.; Kapur, R.; Arbiser, J.L.; Bunting, K.D. Imipramine blue sensitively and selectively targets FLT3-ITD positive acute myeloid leukemia cells. Sci. Rep. 2017, 7, 4447. [Google Scholar] [CrossRef]
- Huang, C.J.; Cheng, H.H.; Chou, C.T.; Kuo, C.C.; Lu, Y.C.; Tseng, L.L.; Chu, S.T.; Hsu, S.S.; Wang, J.L.; Lin, K.L.; et al. Desipramine-induced Ca2+ movement and cytotoxicity in PC3 human prostate cancer cells. Toxicol. Vitr. 2007, 21, 449–456. [Google Scholar] [CrossRef]
- Zingone, A.; Brown, D.; Bowman, E.D.; Vidal, O.M.; Sage, J.; Neal, J.; Ryan, B.M. Relationship between anti-depressant use and lung cancer survival. Cancer Treat. Res. Commun. 2017, 10, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Abdel Karim, N.F.; Hassan, R.; Siddiqi, N.I.; Eldessouki, I.; Gaber, O.; Rahouma, M.; Kamel, M.; Yellu, M.; Gulati, S.; Xie, C.; et al. Impact of tricyclic antidepressants, selective serotonin reuptake inhibitors, and other antidepressants on overall survival of patients with advanced lung cancer from 2004 to 2014: University of Cincinnati experience. J. Int. Med. Res. 2019, 47, 6016–6026. [Google Scholar] [CrossRef] [Green Version]
- Walker, A.J.; Grainge, M.; Bates, T.E.; Card, T.R. Survival of glioma and colorectal cancer patients using tricyclic antidepressants post-diagnosis. Cancer Causes Control 2012, 23, 1959–1964. [Google Scholar] [CrossRef]
- Chen, L.; Li, X.; Li, C.; Zou, C. Antidepressant use and colorectal cancer morbidity and mortality: A dose-response meta analysis. Medicine 2020, 99, e20185. [Google Scholar] [CrossRef]
- Pocobelli, G.; Yu, O.; Ziebell, R.A.; Aiello Bowles, E.J.; Fujii, M.M.; Sterrett, A.T.; Boggs, J.M.; Chen, L.; Boudreau, D.M.; Ritzwoller, D.P.; et al. Use of antidepressants after colon cancer diagnosis and risk of recurrence. Psychooncology 2019, 28, 750–758. [Google Scholar] [CrossRef]
- Chubak, J.; Bowles, E.J.A.; Yu, O.; Buist, D.S.M.; Fujii, M.; Boudreau, D.M. Breast cancer recurrence in relation to antidepressant use. Cancer Causes Control 2016, 27, 125–136. [Google Scholar] [CrossRef] [Green Version]
- Riess, J.W.; Jahchan, N.S.; Das, M.; Zach Koontz, M.; Kunz, P.L.; Wakelee, H.A.; Schatzberg, A.; Sage, J.; Neal, J.W. A Phase Iia Study Repositioning Desipramine in Small Cell Lung Cancer and Other High-Grade Neuroendocrine Tumors. Cancer Treat. Res. Commun. 2020, 23, 100174. [Google Scholar] [CrossRef]


| Clinical Trial ID Phase Status | Title | Conditions | Treatments | Primary Outcome Measures/Secondary Outcome Measures | Study Results/Publications |
|---|---|---|---|---|---|
| ISRCTN49116945 Completed | “A randomised, double-blind controlled trial of ketamine versus placebo in conjunction with best pain management in neuropathic pain in cancer patients” |
|
|
| Ketamine was equivalent to placebo for cancer-related neuropathic pain [48]. |
| |||||
| NCT00740571 Phase 3 Unknown | “Amitriptyline or Pregabalin to Treat Neuropathic Pain in Incurable Cancer” |
|
|
| No results available |
| |||||
| NCT00471445 Phase 3 Completed | “Topical Amitriptyline and Ketamine Cream in Treating Peripheral Neuropathy Caused by Chemotherapy in Cancer Patients” |
|
|
| The KA treatment showed no effect on 6-week CIPN scores [49]. |
| NCT00516503 Completed | “Baclofen–Amitriptyline Hydrochloride–Ketamine (BAK) Gel in Treating Peripheral Neuropathy Caused by Chemotherapy in Patients with Cancer” |
|
|
| Topical treatment with BAK–PLO appears to somewhat improve symptoms of CIPN. This topical gel was well tolerated, without evident systemic toxicity. Further research is needed with increased doses to better clarify the clinical role of this treatment in CIPN [50,51]. |
| |||||
| NCT00798083 Phase 3 Completed | “Neuropathic Pain Caused by Radiation Therapy” |
|
|
| No results available |
|
| Clinical Trial ID Phase Status | Title | Conditions | Treatments | Primary Outcome Measures/Secondary Outcome Measures | Study Results/Publications |
|---|---|---|---|---|---|
| NCT01719861 Phase 2 Terminated | “Phase 2a Desipramine in Small Cell Lung Cancer and Other High-Grade Neuroendocrine Tumors” |
|
|
| No clinical or radiographic benefit was observed, so this trial was terminated [134]. |
| |||||
| NCT03122444 Early Phase 1 Recruiting | “Imipramine on ER + ve and Triple Negative Breast Cancer” |
|
|
| No results available [111] |
| NCT04704453 Phase 2 Recruiting | “Study to Evaluate the Interest of Qutenza in Patients with Head and Neck Cancer in Remission and With Sequelae Neuropathic Pain” |
|
|
| No results available |
| |||||
| NCT02881125 Phase 1 Completed | “Paclitaxel and Nortriptyline Hydrochloride in Treating Patients with Relapsed Small Cell Carcinoma” |
|
|
| No results available |
| |||||
| NCT04863950 Phase 2 Not yet recruiting | “Investigator-Initiated Study of Imipramine Hydrochloride and Lomustine in Recurrent Glioblastoma” |
|
|
| No results available |
| EudraCT-2021-001328-17 Phase 2 Ongoing | “Histological and clinical effects of Imipramine in the treatment of patients with cancer over-expressing Fascin1” |
|
|
| No results available |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asensi-Cantó, A.; López-Abellán, M.D.; Castillo-Guardiola, V.; Hurtado, A.M.; Martínez-Penella, M.; Luengo-Gil, G.; Conesa-Zamora, P. Antitumoral Effects of Tricyclic Antidepressants: Beyond Neuropathic Pain Treatment. Cancers 2022, 14, 3248. https://doi.org/10.3390/cancers14133248
Asensi-Cantó A, López-Abellán MD, Castillo-Guardiola V, Hurtado AM, Martínez-Penella M, Luengo-Gil G, Conesa-Zamora P. Antitumoral Effects of Tricyclic Antidepressants: Beyond Neuropathic Pain Treatment. Cancers. 2022; 14(13):3248. https://doi.org/10.3390/cancers14133248
Chicago/Turabian StyleAsensi-Cantó, Antonio, María Dolores López-Abellán, Verónica Castillo-Guardiola, Ana María Hurtado, Mónica Martínez-Penella, Ginés Luengo-Gil, and Pablo Conesa-Zamora. 2022. "Antitumoral Effects of Tricyclic Antidepressants: Beyond Neuropathic Pain Treatment" Cancers 14, no. 13: 3248. https://doi.org/10.3390/cancers14133248
APA StyleAsensi-Cantó, A., López-Abellán, M. D., Castillo-Guardiola, V., Hurtado, A. M., Martínez-Penella, M., Luengo-Gil, G., & Conesa-Zamora, P. (2022). Antitumoral Effects of Tricyclic Antidepressants: Beyond Neuropathic Pain Treatment. Cancers, 14(13), 3248. https://doi.org/10.3390/cancers14133248