
Predominance of BRCA2 Mutation and Estrogen Receptor Positivity in Unselected Breast Cancer with BRCA1 or BRCA2 Mutation

 , ,
, ,  , ,
, ,  , and
, and 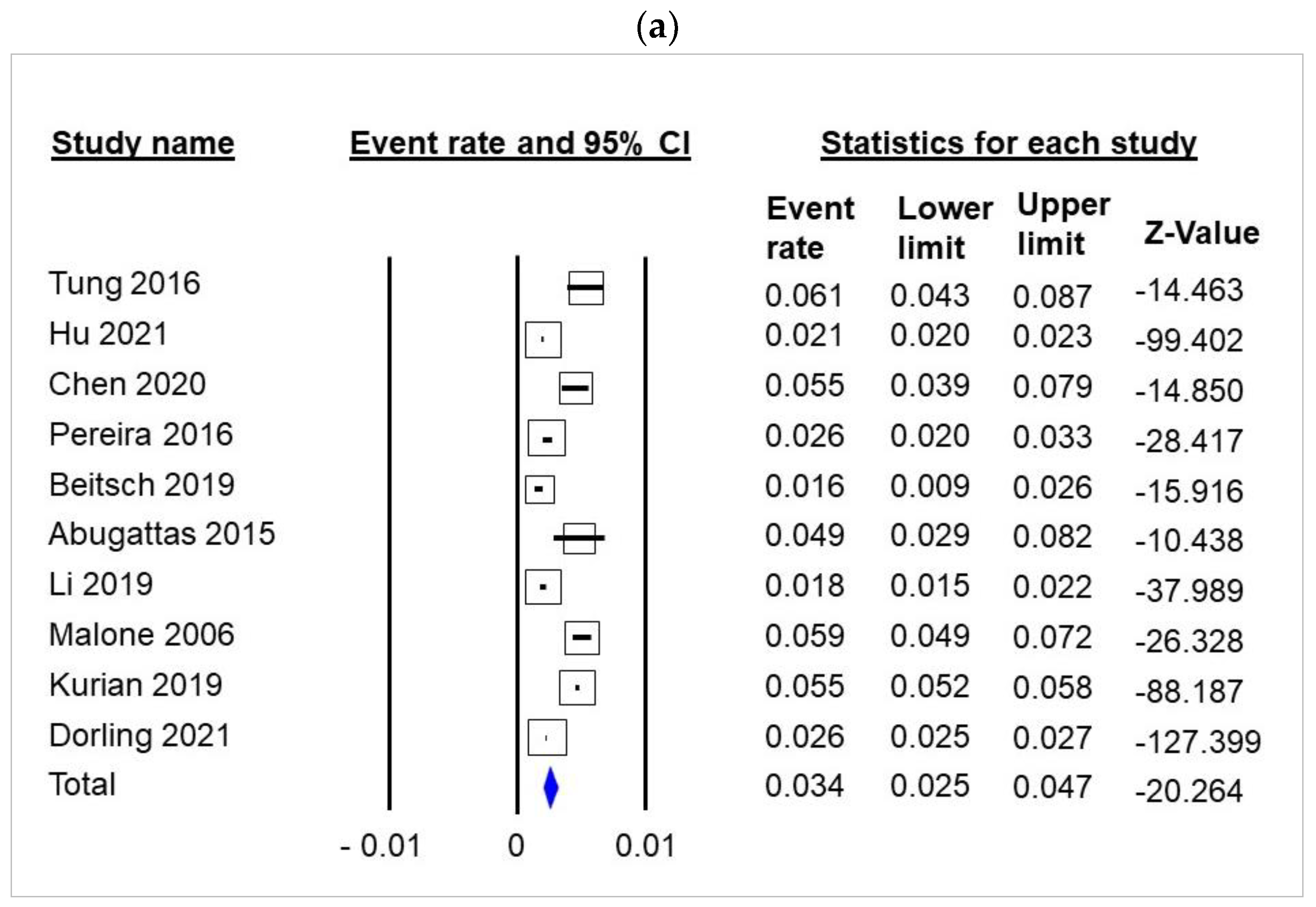{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Literature Search Strategy
2.2. Meta-Analyses
3. Results
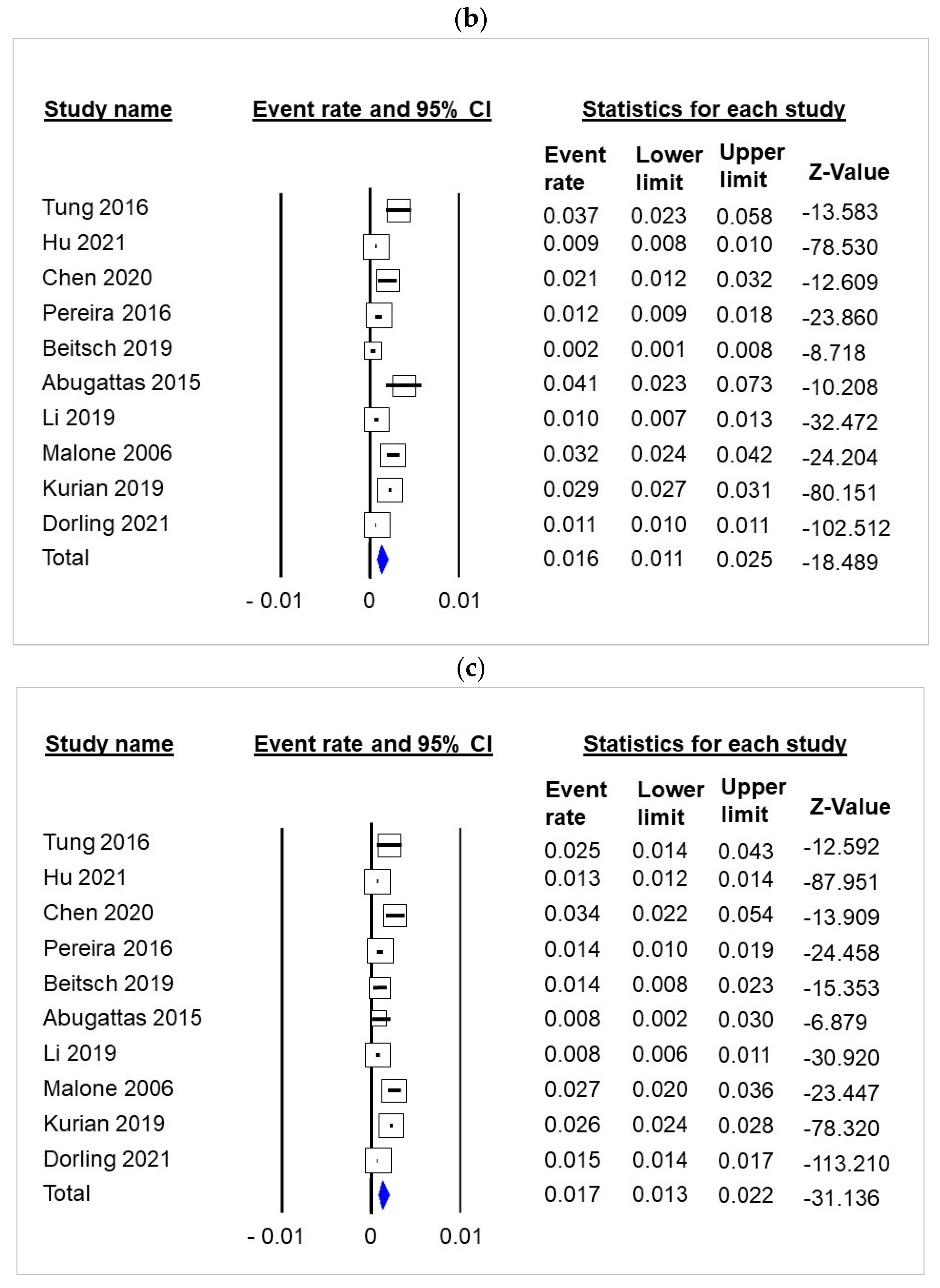
3.1. Carriage of gBRCA in Unselected Breast Cancer Patients
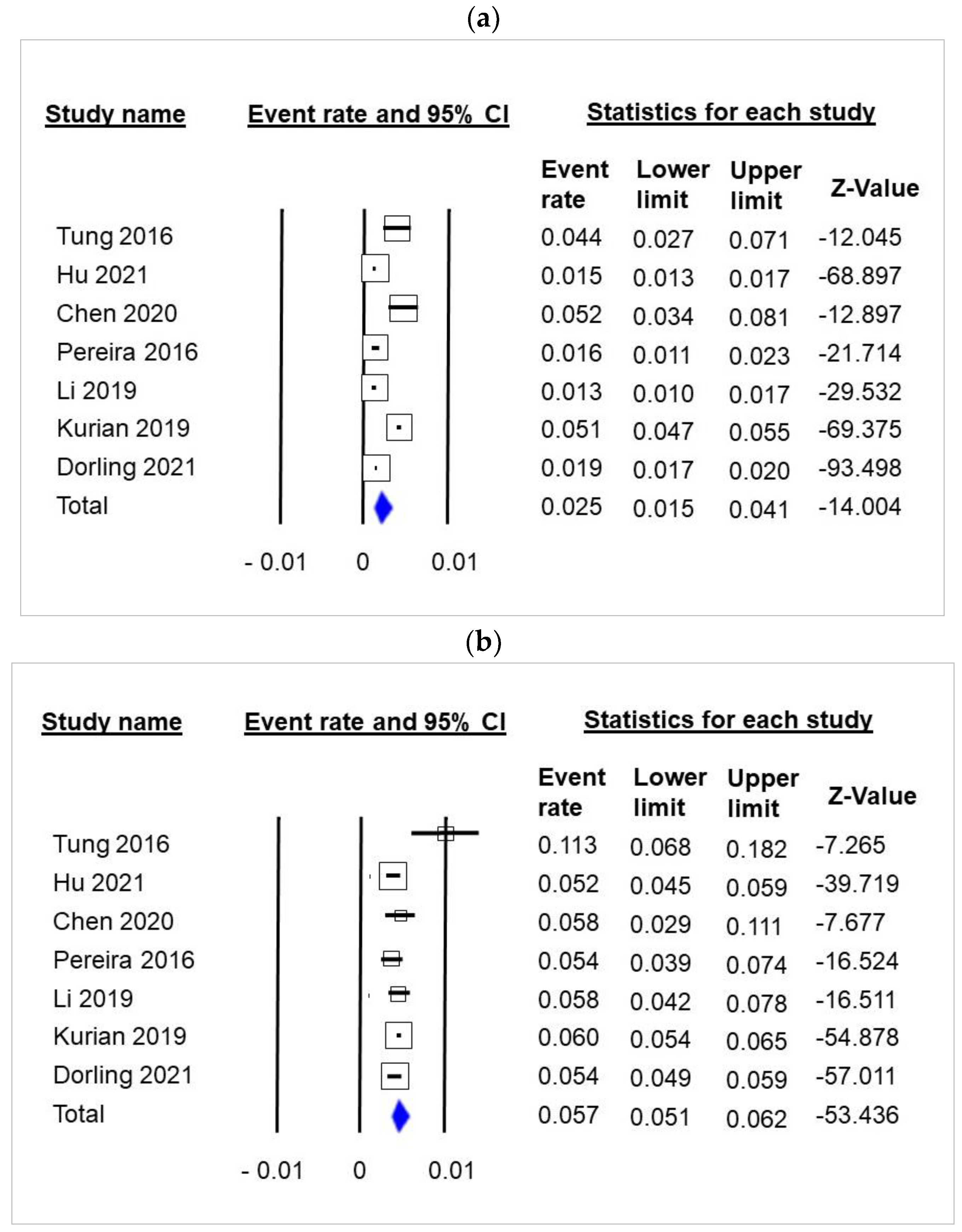
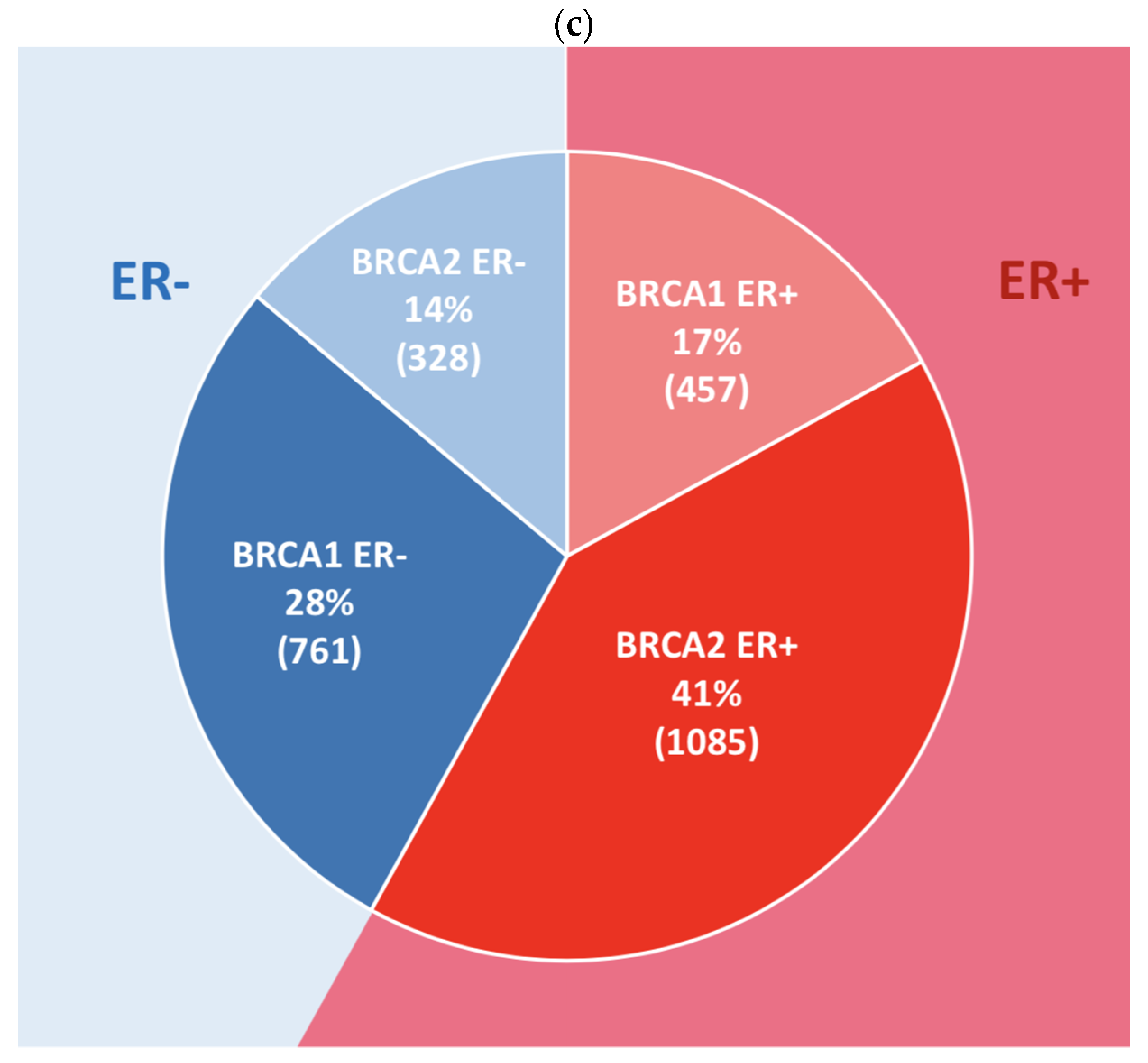
3.2. Frequency of ER+ Tumors among Unselected Breast Cancer Patients with gBRCA Mutation
3.3. Frequency of gBRCA Carriers among Unaffected Individuals
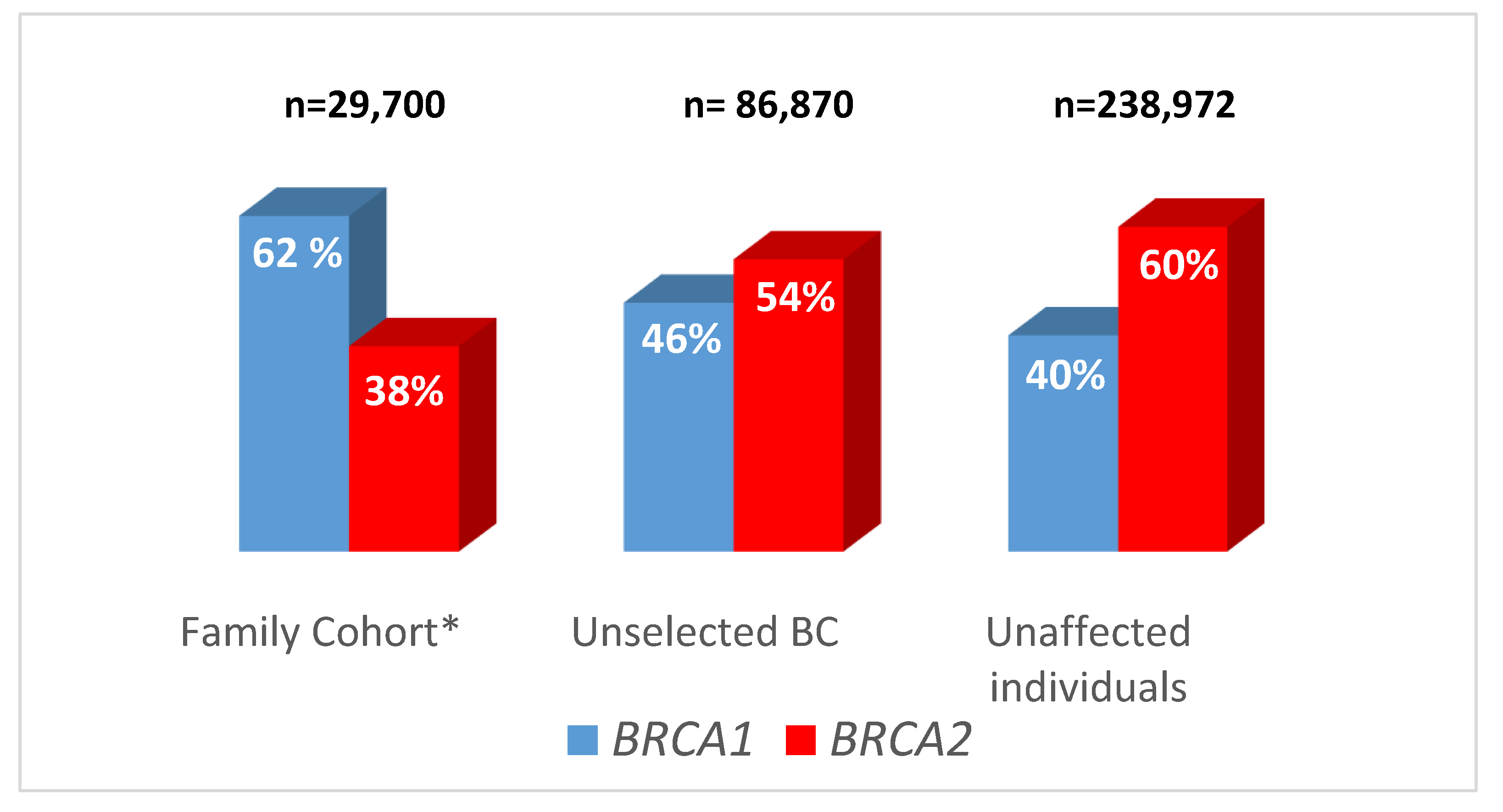
3.4. Comparison of gBRCA1 and gBRCA2 Contribution in Family Cohorts, Unselected Breast Cancer Patients and Unaffected Individuals
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Norquist, B.M.; Harrell, M.I.; Brady, M.F.; Walsh, T.; Lee, M.K.; Gulsuner, S.; Bernards, S.S.; Casadei, S.; Yi, Q.; Burger, R.A.; et al. Inherited Mutations in Women with Ovarian Carcinoma. JAMA Oncol. 2016, 2, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Tung, N.; Lin, N.U.; Kidd, J.; Allen, B.A.; Singh, N.; Wenstrup, R.J.; Hartman, A.-R.; Winer, E.P.; Garber, J.E. Frequency of Germline Mutations in 25 Cancer Susceptibility Genes in a Sequential Series of Patients with Breast Cancer. J. Clin. Oncol. 2016, 34, 1460–1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurian, A.W.; Hare, E.E.; Mills, M.A.; Kingham, K.E.; McPherson, L.; Whittemore, A.S.; McGuire, V.; Ladabaum, U.; Kobayashi, Y.; Lincoln, S.E.; et al. Clinical Evaluation of a Multiple-Gene Sequencing Panel for Hereditary Cancer Risk Assessment. J. Clin. Oncol. 2014, 32, 2001–2009. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.; Hart, S.N.; Gnanaolivu, R.; Huang, H.; Lee, K.Y.; Na, J.; Gao, C.; Lilyquist, J.; Yadav, S.; Boddicker, N.J.; et al. A Population-Based Study of Genes Previously Implicated in Breast Cancer. N. Engl. J. Med. 2021, 384, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Breast Cancer Association Consortium; Dorling, L.; Carvalho, S.; Allen, J.; González-Neira, A.; Luccarini, C.; Wahlström, C.; Pooley, K.A.; Parsons, M.T.; Fortuno, C.; et al. Breast Cancer Risk Genes—Association Analysis in More than 113,000 Women. N. Engl. J. Med. 2021, 384, 428–439. [Google Scholar] [PubMed]
- Drohan, B.; Roche, C.A.; Cusack, J.C., Jr.; Hughes, K.S. Hereditary Breast and Ovarian Cancer and Other Hereditary Syndromes: Using Technology to Identify Carriers. Ann. Surg. Oncol. 2012, 19, 1732–1737. [Google Scholar] [CrossRef] [PubMed]
- Childers, C.P.; Childers, K.K.; Maggard-Gibbons, M.; Macinko, J. National Estimates of Genetic Testing in Women With a History of Breast or Ovarian Cancer. J. Clin. Oncol. 2017, 35, 3800–3806. [Google Scholar] [CrossRef] [PubMed]
- Levy-Lahad, E.; Lahad, A.; King, M.-C. Precision Medicine Meets Public Health: Population Screening for BRCA1 and BRCA2. J. Natl. Cancer Inst. 2015, 107, 420. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Axilbund, J.E.; O’Leary, E.; Michalski, S.T.; Evans, R.; Lincoln, S.E.; Esplin, E.D.; Nussbaum, R.L. Underdiagnosis of Hereditary Breast and Ovarian Cancer in Medicare Patients: Genetic Testing Criteria Miss the Mark. Ann. Surg. Oncol. 2018, 25, 2925–2931. [Google Scholar] [CrossRef]
- Tutt, A.N.J.; Garber, J.E.; Kaufman, B.; Viale, G.; Fumagalli, D.; Rastogi, P.; Gelber, R.D.; de Azambuja, E.; Fielding, A.; Balmaña, J.; et al. Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer. N. Engl. J. Med. 2021, 384, 2394–2405. [Google Scholar] [CrossRef]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.-H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Diéras, V.; Han, H.S.; Kaufman, B.; Wildiers, H.; Friedlander, M.; Ayoub, J.-P.; Puhalla, S.L.; Bondarenko, I.; Campone, M.; Jakobsen, E.H.; et al. Veliparib with Carboplatin and Paclitaxel in BRCA-Mutated Advanced Breast Cancer (BROCADE3): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Oncol. 2020, 21, 1269–1282. [Google Scholar] [CrossRef]
- Tutt, A.N.J.; Garber, J.; Gelber, R.D.; Phillips, K.-A.; Eisen, A.; Johannsson, O.T.; Rastogi, P.; Cui, K.Y.; Im, S.-A.; Yerushalmi, R.; et al. VP1-2022: Pre-Specified Event Driven Analysis of Overall Survival (OS) in the OlympiA Phase III Trial of Adjuvant Olaparib (OL) in Germline BRCA1/2 Mutation (gBRCAm) Associated Breast Cancer. Ann. Oncol. 2022, 33, 566–568. [Google Scholar] [CrossRef]
- Mavaddat, N.; Barrowdale, D.; Andrulis, I.L.; Domchek, S.M.; Eccles, D.; Nevanlinna, H.; Ramus, S.J.; Spurdle, A.; Robson, M.; Sherman, M.; et al. Pathology of Breast and Ovarian Cancers among BRCA1 and BRCA2 Mutation Carriers: Results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol. Biomark. Prev. 2012, 21, 134–147. [Google Scholar] [CrossRef] [Green Version]
- Rebbeck, T.R.; Friebel, T.M.; Friedman, E.; Hamann, U.; Huo, D.; Kwong, A.; Olah, E.; Olopade, O.I.; Solano, A.R.; Teo, S.-H.; et al. Mutational Spectrum in a Worldwide Study of 29,700 Families with BRCA1 or BRCA2 Mutations. Hum. Mutat. 2018, 39, 593–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collet, L.; Péron, J.; Penault-Llorca, F.; Pujol, P.; Lopez, J.; Freyer, G.; You, B. PARP Inhibitors: A Major Therapeutic Option in Endocrine-Receptor Positive Breast Cancers. Cancers 2022, 14, 599. [Google Scholar] [CrossRef]
- Chen, B.; Zhang, G.; Li, X.; Ren, C.; Wang, Y.; Li, K.; Mok, H.; Cao, L.; Wen, L.; Jia, M.; et al. Comparison of BRCA versus Non-BRCA Germline Mutations and Associated Somatic Mutation Profiles in Patients with Unselected Breast Cancer. Aging 2020, 12, 3140–3155. [Google Scholar] [CrossRef]
- Pereira, B.; Chin, S.-F.; Rueda, O.M.; Vollan, H.-K.M.; Provenzano, E.; Bardwell, H.A.; Pugh, M.; Jones, L.; Russell, R.; Sammut, S.-J.; et al. The Somatic Mutation Profiles of 2,433 Breast Cancers Refines Their Genomic and Transcriptomic Landscapes. Nat. Commun. 2016, 7, 11479. [Google Scholar] [CrossRef] [Green Version]
- Beitsch, P.D.; Whitworth, P.W.; Hughes, K.; Patel, R.; Rosen, B.; Compagnoni, G.; Baron, P.; Simmons, R.; Smith, L.A.; Grady, I.; et al. Underdiagnosis of Hereditary Breast Cancer: Are Genetic Testing Guidelines a Tool or an Obstacle? J. Clin. Oncol. 2019, 37, 453–460. [Google Scholar] [CrossRef]
- Abugattas, J.; Llacuachaqui, M.; Allende, Y.S.; Velásquez, A.A.; Velarde, R.; Cotrina, J.; Garcés, M.; León, M.; Calderón, G.; de la Cruz, M.; et al. Prevalence of BRCA1 and BRCA2 Mutations in Unselected Breast Cancer Patients from Peru. Clin. Genet. 2015, 88, 371–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landrum, M.J.; Lee, J.M.; Benson, M.; Brown, G.R.; Chao, C.; Chitipiralla, S.; Gu, B.; Hart, J.; Hoffman, D.; Jang, W.; et al. ClinVar: Improving Access to Variant Interpretations and Supporting Evidence. Nucleic Acids Res. 2018, 46, D1062–D1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malone, K.E.; Daling, J.R.; Doody, D.R.; Hsu, L.; Bernstein, L.; Coates, R.J.; Marchbanks, P.A.; Simon, M.S.; McDonald, J.A.; Norman, S.A.; et al. Prevalence and Predictors of BRCA1 and BRCA2 Mutations in a Population-Based Study of Breast Cancer in White and Black American Women Ages 35 to 64 Years. Cancer Res. 2006, 66, 8297–8308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurian, A.W.; Ward, K.C.; Howlader, N.; Deapen, D.; Hamilton, A.S.; Mariotto, A.; Miller, D.; Penberthy, L.S.; Katz, S.J. Genetic Testing and Results in a Population-Based Cohort of Breast Cancer Patients and Ovarian Cancer Patients. J. Clin. Oncol. 2019, 37, 1305–1315. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Wen, W.X.; Eklund, M.; Kvist, A.; Eriksson, M.; Christensen, H.N.; Torstensson, A.; Bajalica-Lagercrantz, S.; Dunning, A.M.; Decker, B.; et al. Prevalence of BRCA1 and BRCA2 Pathogenic Variants in a Large, Unselected Breast Cancer Cohort. Int. J. Cancer 2019, 144, 1195–1204. [Google Scholar] [CrossRef] [Green Version]
- Manickam, K.; Buchanan, A.H.; Schwartz, M.L.B.; Hallquist, M.L.G.; Williams, J.L.; Rahm, A.K.; Rocha, H.; Savatt, J.M.; Evans, A.E.; Butry, L.M.; et al. Exome Sequencing-Based Screening for BRCA1/2 Expected Pathogenic Variants Among Adult Biobank Participants. JAMA Netw. Open 2018, 1, e182140. [Google Scholar] [CrossRef] [Green Version]
- Abul-Husn, N.S.; Soper, E.R.; Odgis, J.A.; Cullina, S.; Bobo, D.; Moscati, A.; Rodriguez, J.E.; CBIPM Genomics Team; Regeneron Genetics Center; Loos, R.J.F.; et al. Exome Sequencing Reveals a High Prevalence of BRCA1 and BRCA2 Founder Variants in a Diverse Population-Based Biobank. Genome Med. 2019, 12, 2. [Google Scholar] [CrossRef]
- Karczewski, K.J.; Francioli, L.C.; Tiao, G.; Cummings, B.B.; Alföldi, J.; Wang, Q.; Collins, R.L.; Laricchia, K.M.; Ganna, A.; Birnbaum, D.P.; et al. The Mutational Constraint Spectrum Quantified from Variation in 141,456 Humans. Nature 2020, 581, 434–443. [Google Scholar] [CrossRef]
- Di Cosimo, S.; Porcu, L.; Cardoso, F. CDK 4/6 Inhibitors Mired in Uncertainty in HR Positive and HER2 Negative Early Breast Cancer. Breast 2021, 55, 75–78. [Google Scholar] [CrossRef]
- McLaurin, K.; Dalvi, T.; Collins, J.M.; Nordstrom, B.L.; McCutcheon, S.; Bennett, J.C.; Murphy, B.R.; Singhal, P.K.; Briceno, J.M. A Real-World Evidence Study of CDK4/6 Inhibitor Treatment Patterns and Outcomes in Metastatic Breast Cancer by gBRCA Mutation Status. J. Clin. Oncol. 2019, 37, 1563. [Google Scholar] [CrossRef]
- Collins, J.M.; Nordstrom, B.L.; McLaurin, K.K.; Dalvi, T.B.; McCutcheon, S.C.; Bennett, J.C.; Murphy, B.R.; Singhal, P.K.; McCrea, C.; Shinde, R.; et al. A Real-World Evidence Study of CDK4/6 Inhibitor Treatment Patterns and Outcomes in Metastatic Breast Cancer by Germline BRCA Mutation Status. Oncol. Ther. 2021, 9, 575–589. [Google Scholar] [CrossRef]
- Frenel, J.-S.; Dalenc, F.; Pistilli, B.; de La Motte Rouge, T.; Levy, C.; Mouret-Reynier, M.-A.; Hardy-Bessard, A.-C.; Bonichon-Lamichhane, N.; Greilsamer, C.; Delecroix, V.; et al. 304P ESR1 Mutations and Outcomes in BRCA1/2 or PALB2 Germline Mutation Carriers Receiving First Line Aromatase Inhibitor + Palbociclib (AI+P) for Metastatic Breast Cancer (MBC) in the PADA-1 Trial. Ann. Oncol. 2020, 31, S364. [Google Scholar] [CrossRef]
- Pujol, P.; Barberis, M.; Beer, P.; Friedman, E.; Piulats, J.M.; Capoluongo, E.D.; Garcia Foncillas, J.; Ray-Coquard, I.; Penault-Llorca, F.; Foulkes, W.D.; et al. Clinical Practice Guidelines for BRCA1 and BRCA2 Genetic Testing. Eur. J. Cancer 2021, 146, 30–47. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef] [PubMed]
- Tung, N.M.; Zakalik, D.; Somerfield, M.R. Hereditary Breast Cancer Guideline Expert Panel Adjuvant PARP Inhibitors in Patients With High-Risk Early-Stage HER2-Negative Breast Cancer and Germline Mutations: ASCO Hereditary Breast Cancer Guideline Rapid Recommendation Update. J. Clin. Oncol. 2021, 39, 2959–2961. [Google Scholar] [CrossRef] [PubMed]
- Gennari, A.; André, F.; Barrios, C.H.; Cortés, J.; de Azambuja, E.; DeMichele, A.; Dent, R.; Fenlon, D.; Gligorov, J.; Hurvitz, S.A.; et al. ESMO Clinical Practice Guideline for the Diagnosis, Staging and Treatment of Patients with Metastatic Breast Cancer. Ann. Oncol. 2021, 32, 1475–1495. [Google Scholar] [CrossRef]
- NCCN Guidelines for Breast Cancer, V.6.2021 & V.7. 2021. Interim on 08/12/21. Available online: https://www1.nccn.org/guidelines/guidelines-process/transparency-process-and-recommandations/GetFileFromFileManager?fileManagerId=12652 (accessed on 1 March 2022).
- Tung, N.; Miron, A.; Schnitt, S.J.; Gautam, S.; Fetten, K.; Kaplan, J.; Yassin, Y.; Buraimoh, A.; Kim, J.Y.; Szász, A.M.; et al. Prevalence and predictors of loss of wild type BRCA1 in estrogen receptor positive and negative BRCA1-associated breast cancers. Breast Cancer Res. 2010, 12, R95. [Google Scholar] [CrossRef] [Green Version]
- Martins, F.C.; De, S.; Almendro, V.; Gönen, M.; Park, S.Y.; Blum, J.L.; Herlihy, W.; Ethington, G.; Schnitt, S.J.; Tung, N.; et al. Evolutionary pathways in BRCA1-associated breast tumors. Cancer Discov. 2012, 2, 503–511. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, K.N.; Wubbenhorst, B.; Wenz, B.M.; De Sloover, D.; Pluta, J.; Emery, L.; Barrett, A.; Kraya, A.A.; Anastopoulos, I.N.; Yu, S.; et al. BRCA locus-specific loss of heterozygosity in germline BRCA1 and BRCA2 carriers. Nat. Commun. 2017, 8, 319. [Google Scholar] [CrossRef]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.-A.; Mooij, T.M.; Roos-Blom, M.-J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pujol, P.; Yauy, K.; Coffy, A.; Duforet-Frebourg, N.; Gabteni, S.; Daurès, J.-P.; Penault Llorca, F.; Thomas, F.; Hughes, K.; Turnbull, C.; et al. Predominance of BRCA2 Mutation and Estrogen Receptor Positivity in Unselected Breast Cancer with BRCA1 or BRCA2 Mutation. Cancers 2022, 14, 3266. https://doi.org/10.3390/cancers14133266
Pujol P, Yauy K, Coffy A, Duforet-Frebourg N, Gabteni S, Daurès J-P, Penault Llorca F, Thomas F, Hughes K, Turnbull C, et al. Predominance of BRCA2 Mutation and Estrogen Receptor Positivity in Unselected Breast Cancer with BRCA1 or BRCA2 Mutation. Cancers. 2022; 14(13):3266. https://doi.org/10.3390/cancers14133266
Chicago/Turabian StylePujol, Pascal, Kevin Yauy, Amandine Coffy, Nicolas Duforet-Frebourg, Sana Gabteni, Jean-Pierre Daurès, Frédérique Penault Llorca, Frédéric Thomas, Kevin Hughes, Clare Turnbull, and et al. 2022. "Predominance of BRCA2 Mutation and Estrogen Receptor Positivity in Unselected Breast Cancer with BRCA1 or BRCA2 Mutation" Cancers 14, no. 13: 3266. https://doi.org/10.3390/cancers14133266
APA StylePujol, P., Yauy, K., Coffy, A., Duforet-Frebourg, N., Gabteni, S., Daurès, J.-P., Penault Llorca, F., Thomas, F., Hughes, K., Turnbull, C., Galibert, V., Rideau, C., Corsini, C., Collet, L., You, B., Geneviève, D., & Philippe, N. (2022). Predominance of BRCA2 Mutation and Estrogen Receptor Positivity in Unselected Breast Cancer with BRCA1 or BRCA2 Mutation. Cancers, 14(13), 3266. https://doi.org/10.3390/cancers14133266