
Impact of Statin Use on Localized Prostate Cancer Outcomes after Radiation Therapy: Long-Term Follow-Up

 , ,
, ,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Variables and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Descriptive Characteristics of the Study Population
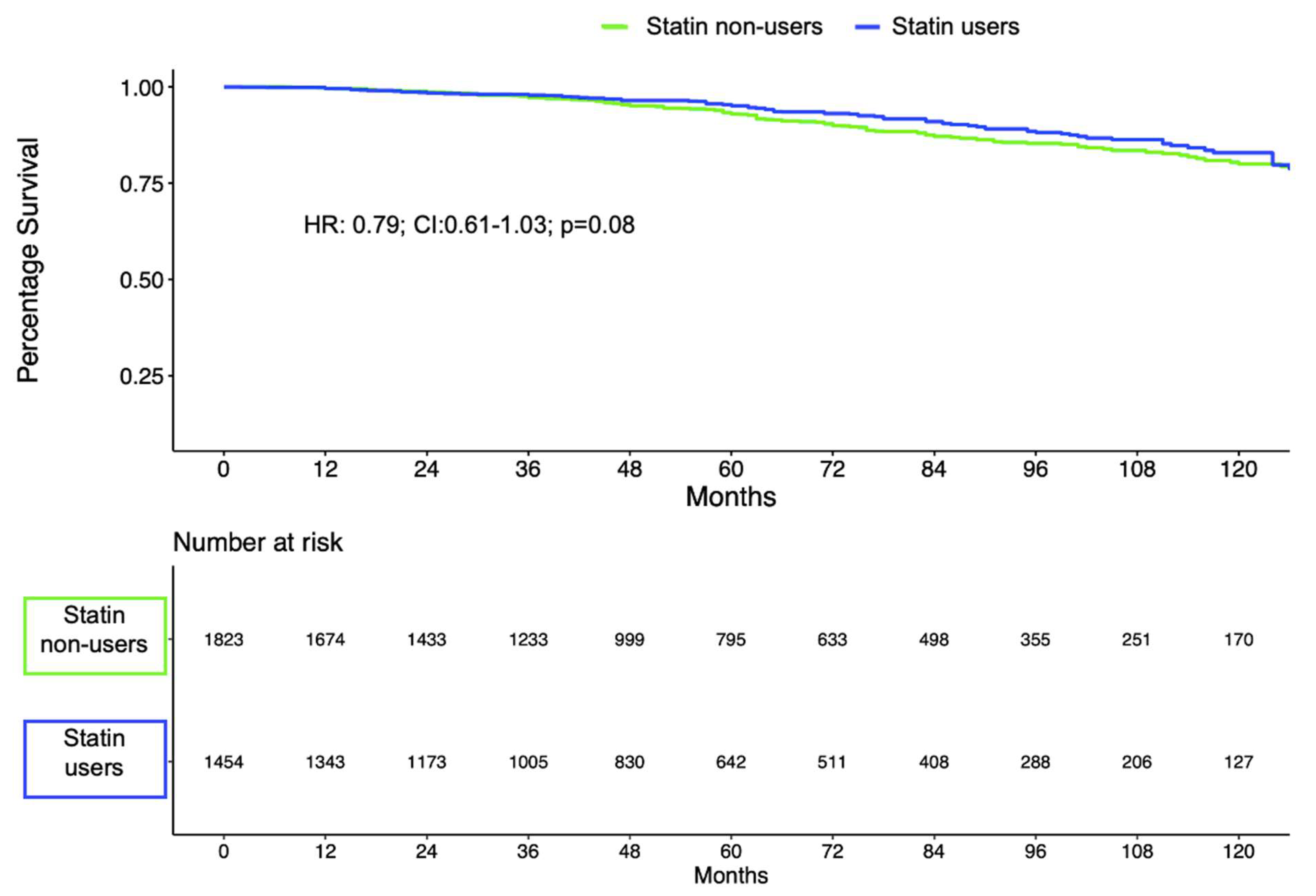
3.2. Biochemical Recurrence within the Overall Study Population According to Statin Use
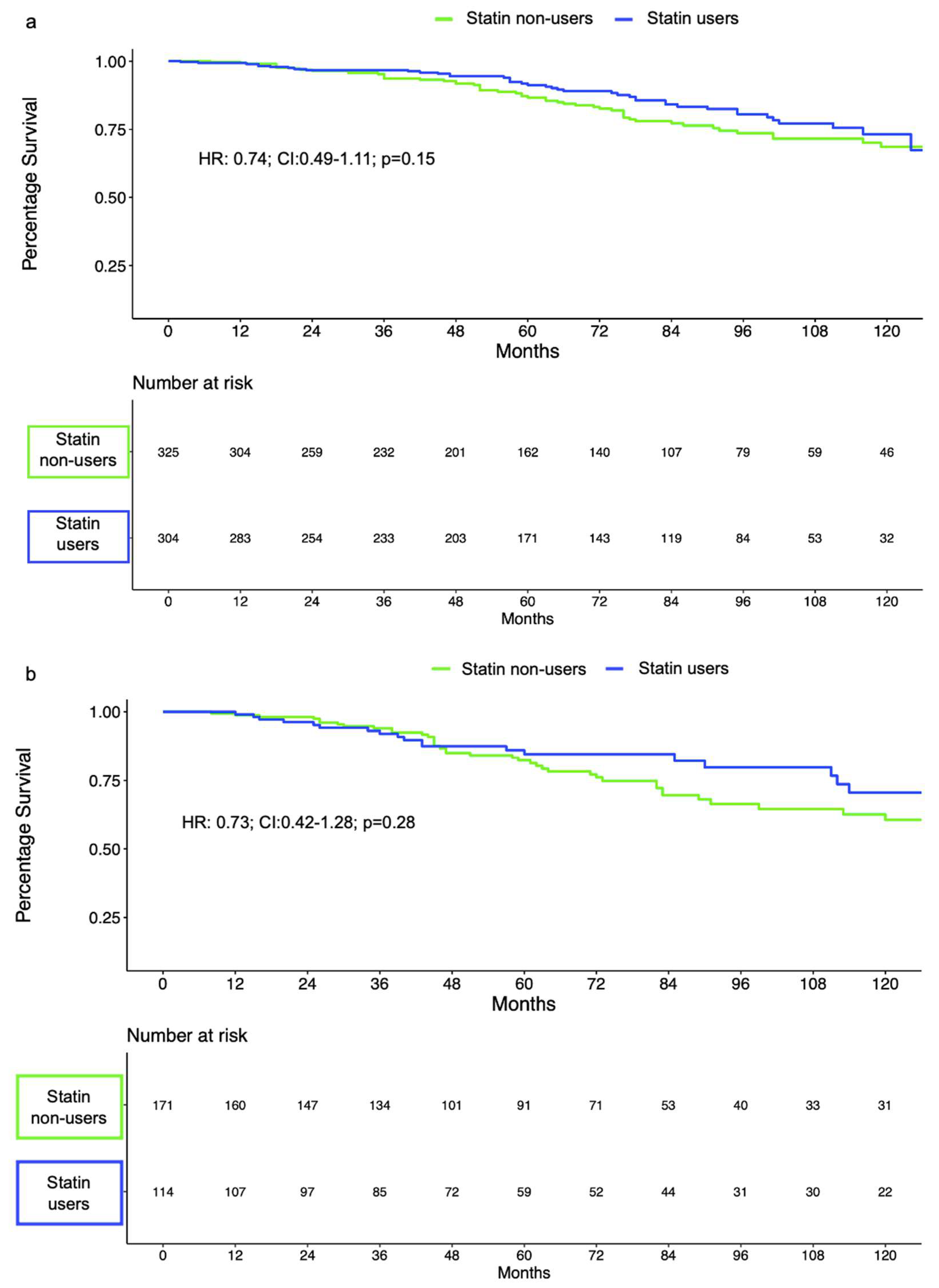
3.3. Biochemical Recurrence within EBRT-Treated Patients According to Statin Use
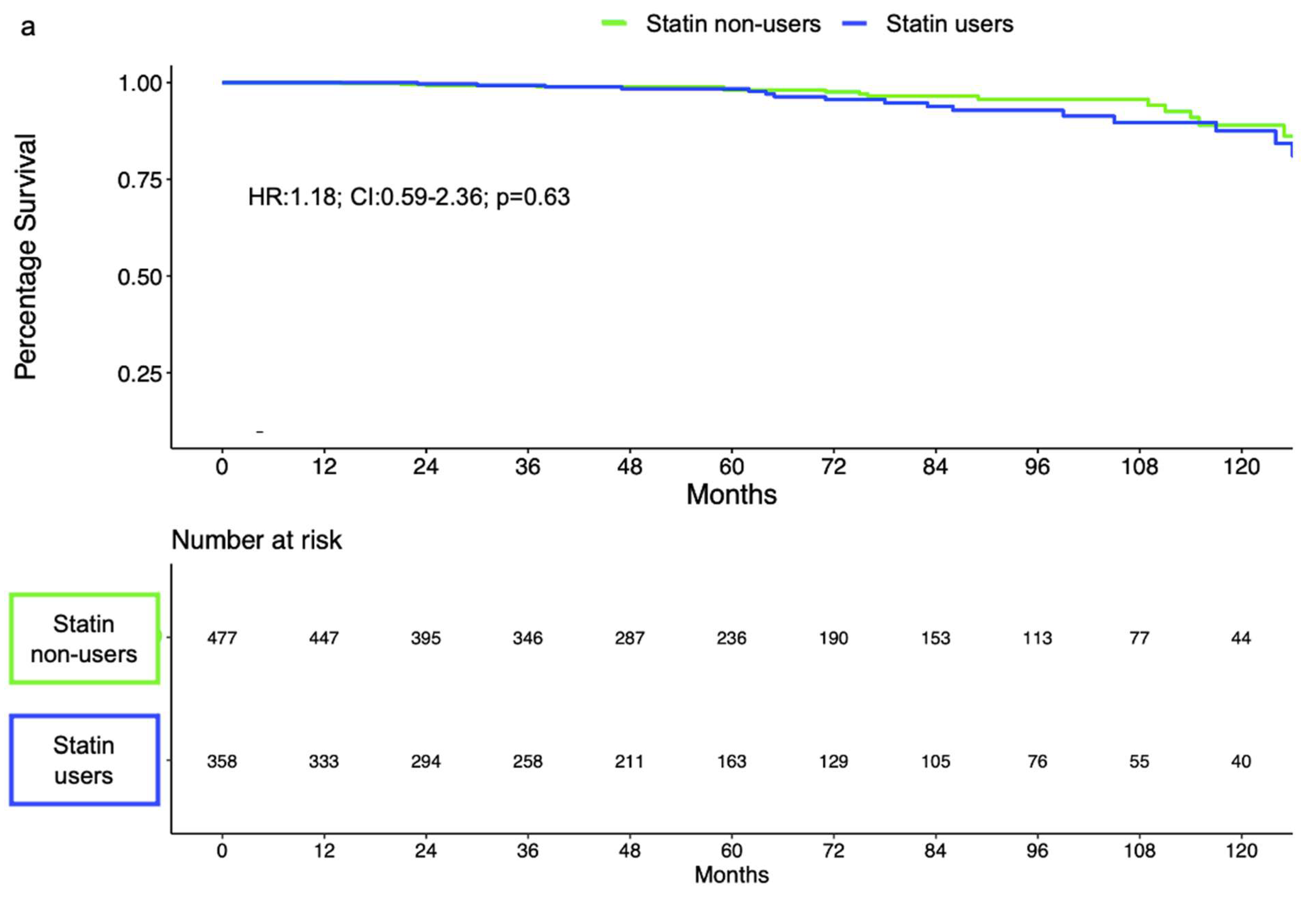
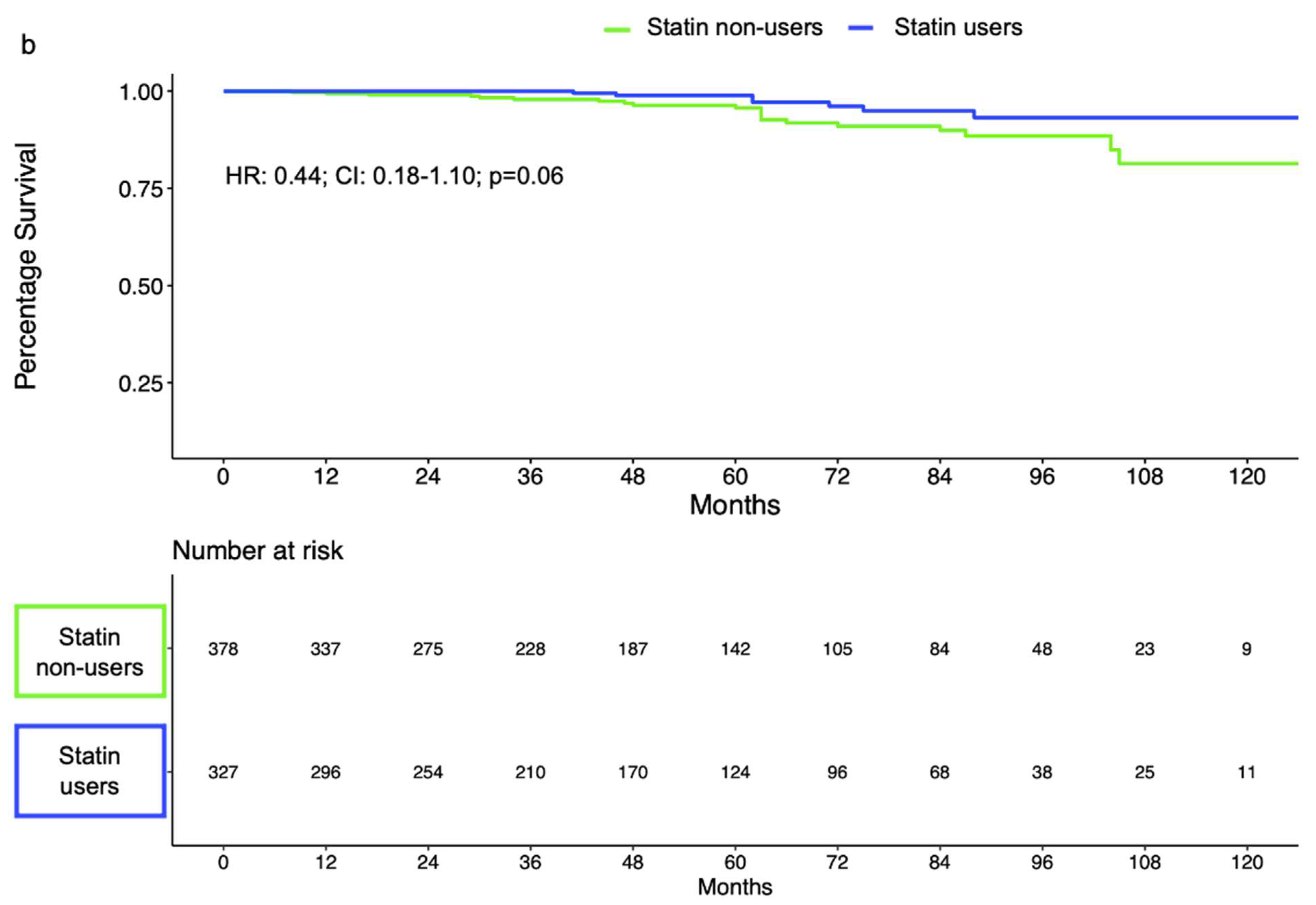
3.4. Biochemical Recurrence within LDR-Treated Patients According to Statin Use
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M.; et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. N. Engl. J. Med. 2016, 375, 1415–1424. [Google Scholar] [CrossRef] [Green Version]
- Van den Broeck, T.; van den Bergh, R.C.N.; Arfi, N.; Gross, T.; Moris, L.; Briers, E.; Cumberbatch, M.; de Santis, M.; Tilki, D.; Fanti, S.; et al. Prognostic Value of Biochemical Recurrence Following Treatment with Curative Intent for Prostate Cancer: A Systematic Review. Eur. Urol. 2019, 75, 967–987. [Google Scholar] [CrossRef] [Green Version]
- Longo, J.; van Leeuwen, J.E.; Elbaz, M.; Branchard, E.; Penn, L.Z. Statins as Anticancer Agents in the Era of Precision Medicine. Clin. Cancer Res. 2020, 26, 5791–5800. [Google Scholar] [CrossRef]
- Félix-Redondo, F.J.; Grau, M.; Fernández-Bergés, D. Cholesterol and Cardiovascular Disease in the Elderly. Facts and Gaps. Aging Dis. 2013, 4, 154–169. [Google Scholar]
- Chin, H.W.; Kim, J.; Rasp, G.; Hristov, B. Prostate Cancer in Seniors: Part 1: Epidemiology, Pathology, and Screening. Fed. Pract. 2015, 32, 41S–44S. [Google Scholar]
- Hutchinson, J.; Marignol, L. Clinical Potential of Statins in Prostate Cancer Radiation Therapy. Anticancer. Res. 2017, 37, 5363–5372. [Google Scholar]
- Yin, P.; Han, S.; Hu, Q.; Tong, S. The association of statin use and biochemical recurrence after curative treatment for prostate cancer: A systematic review and meta-analysis. Medicine 2022, 101, e28513. [Google Scholar] [CrossRef]
- Tan, P.; Wei, S.; Yang, L.; Tang, Z.; Cao, D.; Liu, L.; Fan, Y.; Gao, L.; Wei, Q. The effect of statins on prostate cancer recurrence and mortality after definitive therapy: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 29106. [Google Scholar] [CrossRef] [Green Version]
- Scosyrev, E.; Tobis, S.; Donsky, H.; Wu, G.; Joseph, J.; Rashid, H.; Messing, E. Statin use and the risk of biochemical recurrence of prostate cancer after definitive local therapy: A meta-analysis of eight cohort studies. BJU Int. 2013, 111, E71–E77. [Google Scholar] [CrossRef]
- Mass, A.Y.; Agalliu, I.; Laze, J.; Lepor, H. Preoperative statin therapy is not associated with biochemical recurrence after radical prostatectomy: Our experience and meta-analysis. J. Urol. 2012, 188, 786–791. [Google Scholar] [CrossRef]
- Luo, Y.; She, D.-L.; Xiong, H.; Fu, S.-J.; Yang, L. The Prognostic Effect of Statin Use on Urologic Cancers: An Updated Meta-Analysis of 35 Observational Studies. Medicine 2015, 94, e1523. [Google Scholar] [CrossRef]
- Kollmeier, M.A.; Katz, M.S.; Mak, K.; Yamada, Y.; Feder, D.J.; Zhang, Z.; Jia, X.; Shi, W.; Zelefsky, M.J. Improved biochemical outcomes with statin use in patients with high-risk localized prostate cancer treated with radiotherapy. Int. J. Radiat. Oncol. 2011, 79, 713–718. [Google Scholar] [CrossRef]
- Stish, B.J.; Davis, B.J.; Mynderse, L.A.; Deufel, C.L.; Choo, R. Brachytherapy in the Management of Prostate Cancer. Surg. Oncol. Clin. North Am. 2017, 26, 491–513. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Pasta, D.J.; Elkin, E.P.; Litwin, M.S.; Latini, D.M.; Du Chane, J.; Carroll, P.R. The university of california, san francisco cancer of the prostate risk assessment score: A straightforward and reliable preoperative predictor of disease recurrence after radical prostatectomy. J. Urol. 2005, 173, 1938–1942. [Google Scholar] [CrossRef] [Green Version]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef]
- Abramowitz, M.C.; Li, T.; Buyyounouski, M.K.; Ross, E.; Uzzo, R.G.; Pollack, A.; Horwitz, E.M. The Phoenix definition of biochemical failure predicts for overall survival in patients with prostate cancer. Cancer 2008, 112, 55–60. [Google Scholar] [CrossRef]
- Moyad, M.A.; Merrick, G.S.; Butler, W.M.; Wallner, K.E.; Galbreath, R.W.; Butler, E.G.; Allen, Z.A.; Adamovich, E. Statins, especially atorvastatin, may improve survival following brachytherapy for clinically localized prostate cancer. Urol. Nurs. 2006, 26, 298–303. [Google Scholar]
- Soto, D.E.; Daignault, S.; Sandler, H.M.; Ray, M.E. No effect of statins on biochemical outcomes after radiotherapy for localized prostate cancer. Urology 2009, 73, 158–162. [Google Scholar] [CrossRef]
- Cuaron, J.; Pei, X.; Cohen, G.N.; Cox, B.W.; Yamada, Y.; Zelefsky, M.J.; Kollmeier, M.A. Statin use not associated with improved outcomes in patients treated with brachytherapy for prostate cancer. Brachytherapy 2015, 14, 179–184. [Google Scholar] [CrossRef]
- Liu, X.; Li, J.; Schild, S.E.; Schild, M.H.; Wong, W.; Vora, S.; Herman, M.G.; Fatyga, M. Statins and Metformin Use Is Associated with Lower PSA Levels in Prostate Cancer Patients Presenting for Radiation Therapy. J. Cancer Ther. 2017, 8, 73–85. [Google Scholar] [CrossRef] [Green Version]
- Huynh, L.M.; Keit, E.; Schuller, A.A.; Carrillo, R.C.; Huang, E.; Ahlering, T.E.; Boyle, S.; Enke, C.; Baine, M.J. Impact of statin use on overall and time to biochemical failure following radical prostatectomy or radiation therapy. World J. Urol. 2021, 39, 3287–3293. [Google Scholar] [CrossRef]
- Oh, D.S.; Koontz, B.; Freedland, S.J.; Gerber, L.; Patel, P.; Lewis, S.; Yoo, D.S.; Oleson, J.; Salama, J.K. Statin use is associated with decreased prostate cancer recurrence in men treated with brachytherapy. World J. Urol. 2015, 33, 93–97. [Google Scholar] [CrossRef]
- Gutt, R.; Tonlaar, N.; Kunnavakkam, R.; Karrison, T.; Weichselbaum, R.R.; Liauw, S.L. Statin use and risk of prostate cancer recurrence in men treated with radiation therapy. J. Clin. Oncol. 2010, 28, 2653–2659. [Google Scholar] [CrossRef] [Green Version]
- Zhu, P.-F.; Wang, M.-X.; Chen, Z.-L.; Yang, L. Targeting the Tumor Microenvironment: A Literature Review of the Novel Anti-Tumor Mechanism of Statins. Front. Oncol. 2021, 11, 761107. [Google Scholar] [CrossRef]
- Duarte, J.A.; de Barros, A.L.B.; Leite, E.A. The potential use of simvastatin for cancer treatment: A review. Biomed. Pharmacother. 2021, 141, 111858. [Google Scholar] [CrossRef]
- Di Bello, E.; Zwergel, C.; Mai, A.; Valente, S. The Innovative Potential of Statins in Cancer: New Targets for New Therapies. Front. Chem. 2020, 8, 516. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Overall n = 3555 | No Statin n = 2011 (57%) | Statin Intake n = 1544 (43%) | p-Value | |
|---|---|---|---|---|---|
| Age (years) | 3520 | 67 (62, 72) | 66 (61, 71) | 68 (64, 72) | <0.001 |
| PSA (ng/mL) | 3521 | <0.001 | |||
| 0–10 | 2773 (79%) | 1507 (76%) | 1266 (82%) | ||
| 10–20 | 564 (16%) | 343 (17%) | 221 (14%) | ||
| >20 | 184 (5.2%) | 128 (6.5%) | 56 (3.6%) | ||
| Gleason score | 3479 | 0.080 | |||
| 6 | 1417 (41%) | 827 (42%) | 590 (39%) | ||
| 7 | 1764 (51%) | 949 (49%) | 815 (53%) | ||
| 8 | 199 (5.7%) | 116 (6.0%) | 83 (5.4%) | ||
| 9 | 91 (2.6%) | 52 (2.7%) | 39 (2.5%) | ||
| 10 | 8 (0.2%) | 3 (0.2%) | 5 (0.3%) | ||
| Clinical T Stage | 3498 | 0.046 | |||
| cT1 | 2211 (63%) | 1253 (64%) | 958 (62%) | ||
| cT2a | 884 (25%) | 477 (24%) | 407 (26%) | ||
| cT2b | 176 (5.0%) | 89 (4.5%) | 87 (5.7%) | ||
| cT2c | 47 (1.3%) | 34 (1.7%) | 13 (0.8%) | ||
| cT3-4 | 180 (5.1%) | 106 (5.4%) | 74 (4.8%) | ||
| Treatment | 3486 | 0.9 | |||
| EBRT | 1208 (35%) | 686 (35%) | 522 (34%) | ||
| LDR | 1679 (48%) | 941 (48%) | 738 (48%) | ||
| EBRT + HDR | 599 (17%) | 333 (17%) | 266 (17%) | ||
| ADT | 3555 | 0.5 | |||
| No | 2991 (84%) | 1685 (84%) | 1306 (85%) | ||
| Yes | 564 (16%) | 326 (16%) | 238 (15%) | ||
| D’Amico Classification | 3505 | <0.001 | |||
| Low-risk | 1154 (33%) | 677 (34%) | 477 (31%) | ||
| Intermediate-risk | 1854 (53%) | 984 (50%) | 870 (56%) | ||
| High-risk | 497 (14%) | 302 (15%) | 195 (13%) | ||
| Follow-up (months) | 3277 | 52 (28, 84) | 51 (24, 84) | 52 (30, 84) | 0.4 |
| Univariable | Multivariable 1 | |||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| Statin treatment | ||||||
| No | Ref. | Ref. | ||||
| Yes | 0.80 | 0.62–1.04 | 0.10 | 0.79 | 0.61–1.03 | 0.08 |
| Univariable | Multivariable 1 | ||||||
|---|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | ||
| D’Amico intermediate-risk | Statin treatment | ||||||
| No | Ref. | Ref. | |||||
| Yes | 0.79 | 0.52–1.17 | 0.24 | 0.74 | 0.49–1.11 | 0.15 | |
| D’Amico high-risk | Statin treatment | ||||||
| No | Ref. | Ref. | |||||
| Yes | 0.70 | 0.41–1.19 | 0.19 | 0.73 | 0.42–1.28 | 0.28 | |
| Univariable | Multivariable 1 | ||||||
|---|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | ||
| D’Amico low-risk | Statin treatment | ||||||
| No | Ref. | Ref. | |||||
| Yes | 1.27 | 0.64–2.52 | 0.48 | 1.18 | 0.59–2.36 | 0.63 | |
| D’Amico intermediate-risk | Statin treatment | ||||||
| No | Ref. | Ref. | |||||
| Yes | 0.38 | 0.16–0.92 | 0.03 | 0.44 | 0.18–1.10 | 0.06 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaulanjan, K.; Lavigne, D.; Saad, F.; Karakiewicz, P.I.; Flammia, R.S.; Kluth, L.A.; Mandel, P.; Chun, F.K.-H.; Taussky, D.; Hoeh, B. Impact of Statin Use on Localized Prostate Cancer Outcomes after Radiation Therapy: Long-Term Follow-Up. Cancers 2022, 14, 3606. https://doi.org/10.3390/cancers14153606
Kaulanjan K, Lavigne D, Saad F, Karakiewicz PI, Flammia RS, Kluth LA, Mandel P, Chun FK-H, Taussky D, Hoeh B. Impact of Statin Use on Localized Prostate Cancer Outcomes after Radiation Therapy: Long-Term Follow-Up. Cancers. 2022; 14(15):3606. https://doi.org/10.3390/cancers14153606
Chicago/Turabian StyleKaulanjan, Kevin, Danny Lavigne, Fred Saad, Pierre I. Karakiewicz, Rocco Simone Flammia, Luis Alex Kluth, Philipp Mandel, Felix K. -H. Chun, Daniel Taussky, and Benedikt Hoeh. 2022. "Impact of Statin Use on Localized Prostate Cancer Outcomes after Radiation Therapy: Long-Term Follow-Up" Cancers 14, no. 15: 3606. https://doi.org/10.3390/cancers14153606
APA StyleKaulanjan, K., Lavigne, D., Saad, F., Karakiewicz, P. I., Flammia, R. S., Kluth, L. A., Mandel, P., Chun, F. K. -H., Taussky, D., & Hoeh, B. (2022). Impact of Statin Use on Localized Prostate Cancer Outcomes after Radiation Therapy: Long-Term Follow-Up. Cancers, 14(15), 3606. https://doi.org/10.3390/cancers14153606