
Survival after Multimodal Treatment Including Surgery for Metastatic Esophageal Cancer: A Systematic Review

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Research Strategy
2.3. Selection Criteria and Outcome Measures
- Participants: adults with squamous cell carcinomas (SCCs) or adenocarcinomas (ADKs) with a synchronous metastases of the esophagus; metastatic disease was defined as having a distant metastasis at the time of diagnosis according to the SEER historical stage. The distant stage was defined as a neoplasm that had spread to parts of the body away from the primary tumor through direct extension, discontinuous metastases (e.g., implantation or seeding) to distant organs and tissues, or from the lymphatic system to distant lymph nodes.
- Intervention: esogastric surgery resection with or without concomitant treatment of metastases.
- Comparison: patients with stage IV esophageal cancer not undergoing surgery.
- Outcomes: the main outcome measure was the 3-year overall survival rate. Secondary outcomes were postoperative morbidity and pathological response.
2.4. Quality Assessment of Retrieved Articles
2.5. Data Extraction
2.6. Statistical Analyses and Estimation of Risk of Bias
3. Results
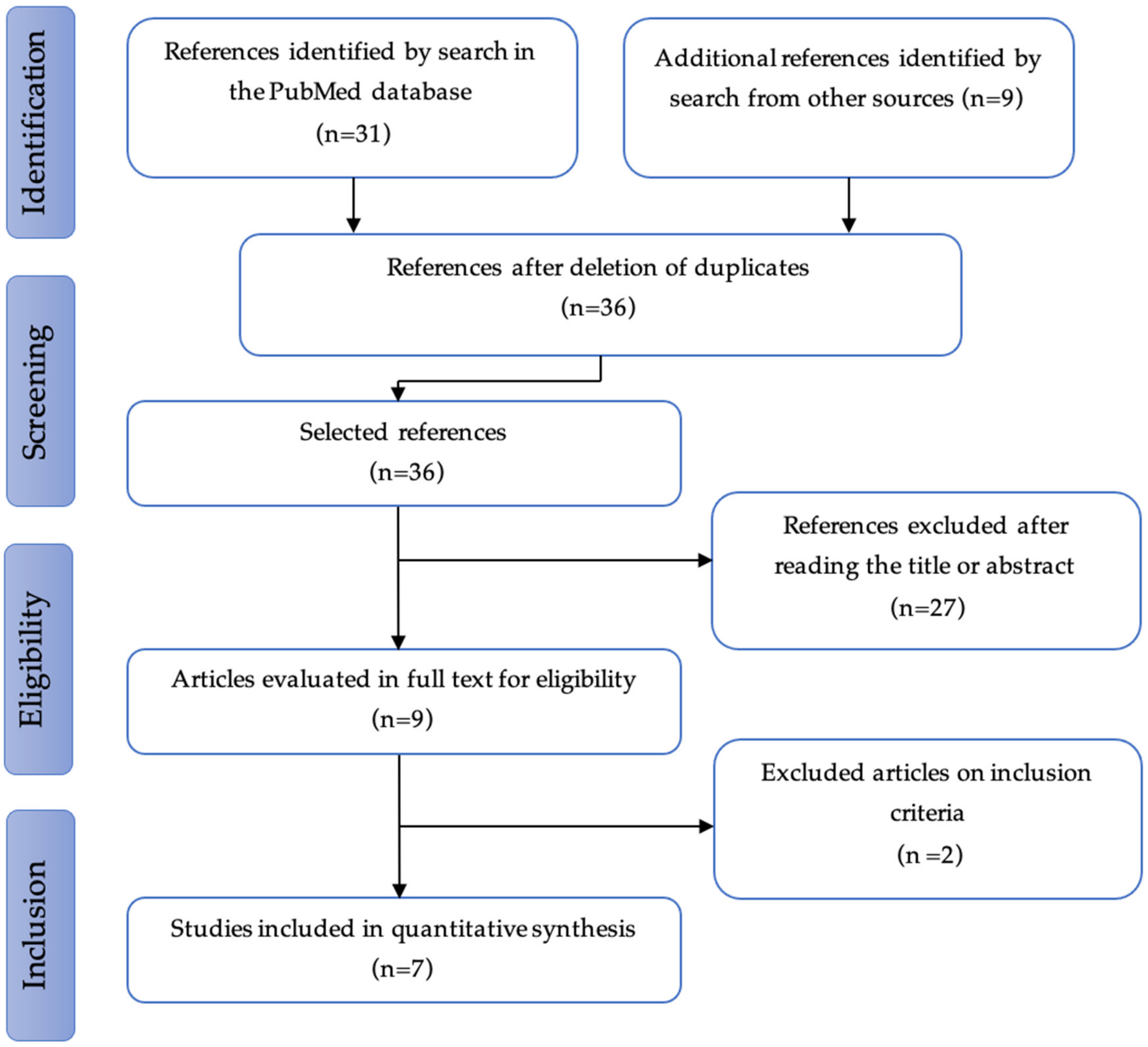
3.1. Study Selection
3.2. Studies and Patients’ Characteristics
3.2.1. Preoperative Multimodal Treatment
3.2.2. Surgical Features and Postoperative Outcomes
3.2.3. Pathological Responses
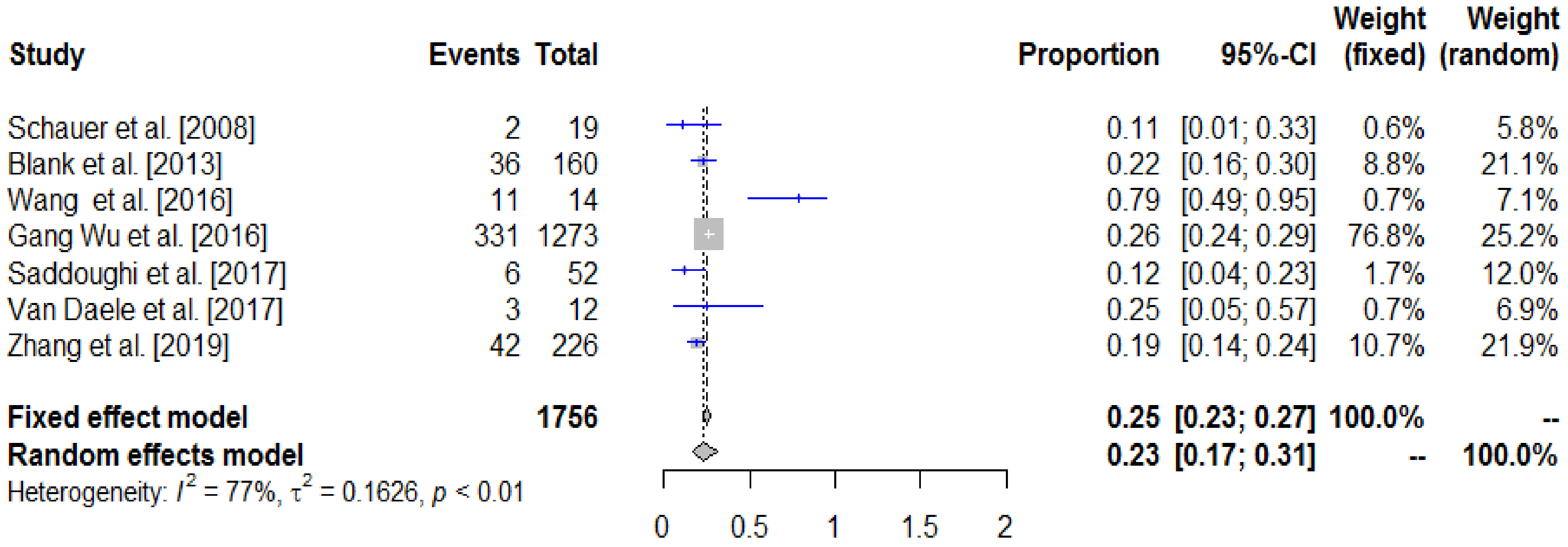
3.3. Survival Analysis
Survival Prognosis Factors
3.4. Risk of Bias Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Horner, M. SEER Cancer Statistics Review, 1975–006. Available online: http://seer.cancer.gov/csr/1975_2006 (accessed on 1 April 2008).
- Wu, S.-G.; Xie, W.-H.; Zhang, Z.-Q.; Sun, J.-Y.; Li, F.-Y.; Lin, H.-X.; Bao, Y.; He, Z.-Y. Surgery combined with radiotherapy improved survival in metastatic esophageal cancer in a surveillance epidemiology and end results population-based study. Sci. Rep. 2016, 6, 28280. [Google Scholar] [CrossRef]
- Ajani, J.A.; D’Amico, T.A.; Almhanna, K.; Bentrem, D.J.; Besh, S.; Chao, J.; Das, P.; Denlinger, C.; Fanta, P.; Fuchs, C.S. Esophageal and esophagogastric junction cancers, version 1.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 194–227. [Google Scholar] [CrossRef] [PubMed]
- Ichida, H.; Imamura, H.; Yoshimoto, J.; Sugo, H.; Kajiyama, Y.; Tsurumaru, M.; Suzuki, K.; Ishizaki, Y.; Kawasaki, S. Pattern of postoperative recurrence and hepatic and/or pulmonary resection for liver and/or lung metastases from esophageal carcinoma. World J. Surg. 2013, 37, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Lo, C.K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Bmj 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Schauer, M.; Stein, H.; Lordick, F.; Feith, M.; Theisen, J.; Siewert, J.R. Results of a multimodal therapy in patients with stage IV Barrett’s adenocarcinoma. World J. Surg. 2008, 32, 2655–2660. [Google Scholar] [CrossRef]
- Blank, S.; Lordick, F.; Dobritz, M.; Grenacher, L.; Burian, M.; Langer, R.; Roth, W.; Schaible, A.; Becker, K.; Bläker, H. A reliable risk score for stage IV esophagogastric cancer. Eur. J. Surg. Oncol. 2013, 39, 823–830. [Google Scholar] [CrossRef]
- Wang, J.; Suri, J.S.; Allen, P.K.; Liao, Z.; Komaki, R.; Ho, L.; Hofstetter, W.L.; Lin, S.H. Factors predictive of improved outcomes with multimodality local therapy after palliative chemotherapy for stage IV esophageal cancer. Am. J. Clin. Oncol. 2016, 39, 228–235. [Google Scholar] [CrossRef]
- Saddoughi, S.A.; Reinersman, J.M.; Zhukov, Y.O.; Taswell, J.; Mara, K.; Harmsen, S.W.; Blackmon, S.H.; Cassivi, S.D.; Nichols, F., III; Shen, K.R. Survival after surgical resection of stage IV esophageal cancer. Ann. Thorac. Surg. 2017, 103, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Van Daele, E.; Scuderi, V.; Pape, E.; Van de Putte, D.; Varin, O.; Van Nieuwenhove, Y.; Ceelen, W.; Troisi, R.; Pattyn, P. Long-term survival after multimodality therapy including surgery for metastatic esophageal cancer. Acta Chir. Belg. 2018, 118, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Zou, J.; Li, P.; Li, Q.; Qiao, Y.; Han, J.; Huang, K.; Ruan, P.; Lin, H.; Song, Q. Surgery to the primary tumor is associated with improved survival of patients with metastatic esophageal cancer: Propensity score-matched analyses of a large retrospective cohort. Dis. Esophagus 2020, 33, doz051. [Google Scholar] [CrossRef]
- Sedgwick, P. Meta-analyses: How to read a funnel plot. Bmj 2013, 346, f1342. [Google Scholar] [CrossRef]
- De Graaf, G.; Ayantunde, A.; Parsons, S.; Duffy, J.; Welch, N. The role of staging laparoscopy in oesophagogastric cancers. Eur. J. Surg. Oncol. 2007, 33, 988–992. [Google Scholar] [CrossRef]
- Mariette, C.; Piessen, G.; Triboulet, J.-P. Therapeutic strategies in oesophageal carcinoma: Role of surgery and other modalities. Lancet Oncol. 2007, 8, 545–553. [Google Scholar] [CrossRef]
- Carmona-Bayonas, A.; Jiménez-Fonseca, P.; Echavarria, I.; Cánovas, M.S.; Aguado, G.; Gallego, J.; Custodio, A.; Hernández, R.; Viudez, A.; Cano, J.M. Surgery for metastases for esophageal-gastric cancer in the real world: Data from the AGAMENON national registry. Eur. J. Surg. Oncol. 2018, 44, 1191–1198. [Google Scholar] [CrossRef]
- Seyedin, S.N.; Parekh, K.R.; Ginader, T.; Caster, J.M. The Role of Definitive Radiation and Surgery in Metastatic Esophageal Cancer: An NCDB Investigation. Ann. Thorac. Surg. 2021, 112, 459–466. [Google Scholar] [CrossRef]
- Takeda, F.R.; Cecconello, I. The complex assessment of anastomosis’ perfusion following esophagectomy: Set in stone? Eur. J. Surg. Oncol. 2021, 47, 1491–1492. [Google Scholar] [CrossRef]
- Blum Murphy, M.; Xiao, L.; Patel, V.R.; Maru, D.M.; Correa, A.M.; Amlashi, F.G.; Liao, Z.; Komaki, R.; Lin, S.H.; Skinner, H.D. Pathological complete response in patients with esophageal cancer after the trimodality approach: The association with baseline variables and survival—The University of Texas MD Anderson Cancer Center experience. Cancer 2017, 123, 4106–4113. [Google Scholar] [CrossRef]
- Bedenne, L.; Mariette, C. Comparison of Systematic Surgery Versus Surveillance and Rescue Surgery in Operable Oesophageal Cancer with a Complete Clinical Response to Radiochemotherapy (Esostrate). Identifier: NCT02551458. Available online: ClinicalTrials.gov (accessed on 11 July 2022).
- Weichselbaum, R.R.; Hellman, S. Oligometastases revisited. Nat. Rev. Clin. Oncol. 2011, 8, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Hellman, S.; Weichselbaum, R.R. Oligometastases. J. Clin. Oncol. 1995, 13, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Al-Batran, S.-E.; Goetze, T.O.; Mueller, D.W.; Vogel, A.; Winkler, M.; Lorenzen, S.; Novotny, A.; Pauligk, C.; Homann, N.; Jungbluth, T.; et al. The RENAISSANCE (AIO-FLOT5) trial: Effect of chemotherapy alone vs. chemotherapy followed by surgical resection on survival and quality of life in patients with limited-metastatic adenocarcinoma of the stomach or esophagogastric junction—A phase III trial of the German AIO/CAO-V/CAOGI. BMC Cancer 2017, 17, 893. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Design | Country | Study Period | Sample Size | M+ Patients Who Underwent Surgery |
|---|---|---|---|---|---|
| Schauer et al., 2008 [9] | Retrospective (vs. M0) | Germany | 1996–2006 | 178 | 19 (10.7) |
| Blank et al., 2013 [10] | Retrospective cohort | Germany | 1987–2007 | 707 | 160 (22.6) |
| Wang et al., 2016 [11] | Retrospective (vs. no surgery) | U.S. | 1999–2012 | NR | 14 (NA) |
| Gang Wu et al., 2016 [3] | Retrospective (vs. no surgery) | China | 1988–2012 | 9125 | 1273 (13.9) |
| Saddoughi et al., 2017 [12] | Retrospective (known versus i.o. M1) | U.S. | 1985–2014 | 3500 | 52 (1.5) |
| Van Daele et al., 2017 [13] | Retrospective cohort | Belgium | 2010–2014 | 602 | 12 (2) |
| Zhang et al., 2019 [14] | Retrospective cohort | China | 2004–2014 | 4367 | 226 (5.2) |
| Study | Selection | Comparability | Outcome | Score | ||||
|---|---|---|---|---|---|---|---|---|
| Patients Who Underwent Surgery | Representativeness of Exposed Cohort (max = *) | Selection of the Non-Exposed Cohort (max = *) | Ascertainment of Exposure (max = *) | Comparability of the Cohorts Based on the Design or Analysis (max = **) | Assessment of Outcome (max = *) | Adequacy of Follow-up of Cohort (max = *) | ||
| Schauer et al., 2008 [9] | 19 | * | * | * | * | * | - | 5 |
| Blank et al., 2013 [10] | 160 | * | - | * | - | * | * | 4 |
| Wang et al., 2016 [11] | 14 | * | * | * | * | * | - | 5 |
| Gang Wu et al., 2016 [3] | 1273 | * | * | * | * | * | - | 5 |
| Saddoughi et al., 2017 [12] | 52 | * | * | * | * | * | - | 5 |
| Van Daele et al., 2017 [13] | 12 | * | - | * | - | * | * | 4 |
| Zhang et al., 2019 [14] | 226 | * | * | * | ** | * | - | 6 |
| Schauer et al., 2008 [9] | Blank et al., 2013 [10] | Wang et al., 2016 [11] | Gang Wu et al., 2016 [3] | Saddoughi et al., 2017 [12] | Van Daele et al., 2017 [13] | Zhang et al., 2019 [14] | |||
|---|---|---|---|---|---|---|---|---|---|
| Number of operated patients | 19 | 160 | 14 | 1273 | 52 | 12 | 226 | ||
| Median age (years) | 60 | NR | 59 | 64 | NR | NR | 63 | ||
| Number of adenocarcinomas | 19 (100) | 160 (100) | 13 (93) | 815 (64) | 46 (89) | 9 (75) | 169 (74.7) | ||
| Primary tumor localization | |||||||||
| Esophagus | |||||||||
| Upper third | 0 | 0 | 0 | 35 (2.7) | 1 (2) | 0 | 6 (2.7) | ||
| Middle Third | 0 | 0 | 1 (2) | 172 (13.5) | 5 (10) | ND | 26 (11.5) | ||
| Distal Third/AEG I | 19 (100) | 25 (15.6) | 13 (98) | 1066 (83.7) | 44 (84) | 2 (17) | 164 (72.6) | ||
| Gastric | |||||||||
| AEG II or III | 0 | 71 (44.3) | 0 | 0 | 2 (4) | 2 (17) | 12 (5.3) | ||
| Other | 0 | 44 (27.5) | 0 | 0 | 0 | 0 | 18 (8.0) | ||
| Lymph node metastases | 2 (10.5) | 16 (10) | 11 (79) | NR | NR | NR | 150 (66.8) | ||
| Metastatic pattern | |||||||||
| ≤ 1 metastasis | NR | NR | 7 (50) | NR | NR | NR | NR | ||
| Single-organ metastases | 16 (84.2) | 119 (68.8) | NR | NR | 52 (100) | 11 (92) | NR | ||
| Multiple-organ metastases | 3 (15.8) | 41 (31.2) | NR | NR | 0 | 1 (8) | NR | ||
| Metastatic sites | Lung, liver, distant lymph nodes, bone, peritoneum, spleen, adrenal gland | Peritoneum, lung, liver | Bone, brain, liver, peritoneum, adrenal glands, distant lymph nodes | NR | Lung, liver, peritoneum, distant lymph nodes | Liver, distant lymph nodes, bone | NR | ||
| Preoperative treatment | |||||||||
| Chemotherapy | 19 (100) | 160 (100) | 14 (100) | NR | 0 | 8 (67) | 184 (81.4) | ||
| Consolidation RCT | 0 | 0 | 14 (100) | NR | 0 | 0 | 0 | ||
| Consolidation RT | 0 | 0 | 0 | NR | 0 | 0 | 0 | ||
| RCT | 0 | 0 | 0 | NR | 17 (32.6) | 4 (33) | NR | ||
| Radiotherapy alone | 0 | 0 | 0 | 523 (61.7) | 1 (1.9) | 0 | 146 (64.6) | ||
| Schauer et al., 2008 [9] | Blank et al., 2013 [10] | Wang et al., 2016 [11] | Gang Wu et al., 2016 [3] | Saddoughi et al., 2017 [12] | Van Daele et al., 2017 [13] | Zhang et al., 2019 [14] | |
|---|---|---|---|---|---|---|---|
| Operated patients | 19 | 160 | 14 | 1273 | 52 | 12 | 226 |
| Surgical approach | |||||||
| Conventional | 19 (100) | 160 (100) | 14 (100) | NR | 51 (98) | 12 (100) | NR |
| Laparoscopic | 0 | 0 | 0 | NR | 1 (2) | 0 | NR |
| Trans-hiatal | NR | 20 (13) | NR | NR | 5 (10) | 0 | NR |
| Two-way (Ivor Lewis) | NR | 5 (3) | NR | NR | 39 (75) | 10 (83) | NR |
| Three-way (McKeown) | NR | 0 | NR | NR | 3 (5) | 0 | NR |
| Other | NR | 135 (84) | NR | NR | 5 (10) | 2 (17) | NR |
| Metastases treatment | If possible | Systematic | NR | NR | 0 | 11 (92) | NR |
| Lymphadenectomy | Two-field | Two-field | Two-field | NR | NR | Two-field | NR |
| Complication rate | 5 (25) | 56 (35) | NR | NR | 27 (51.8) | 5 (41.6) | NR |
| Surgery-related mortality | 1 (5) | 4 (2.5) | NR | NR | 4 (7.7) | 0 | NR |
| Pathological features | |||||||
| R0 resection | NR | 66 (41.5) | NR | NR | NR | 11 (92) | NR |
| Tumor regression rate | |||||||
| Reg 1 | 3 (15.8) | 35 (21.8) | NR | NR | NR | NR | NR |
| Reg 2 | 16 (84.2) | 124 (77.5) | NR | NR | NR | NR | NR |
| Histological grade | |||||||
| G1/2 | NR | 13 (8) | NR | 477 (37.4) | NR | NR | 80 (35.4) |
| G3/4 | NR | 146 (91) | NR | 670 (52.6) | NR | NR | 131 (58) |
| Study | Patients Who Underwent Surgery | Median Follow-Up (Months) | Mortality Rate (Percentage) | Median Survival (Months) | 1-Year OS (Percentage) | 3-Year OS (Percentage) | 5-Year OS (Percentage) |
|---|---|---|---|---|---|---|---|
| Schauer et al., 2008 [9] | 19 | 10 | 74 | 9 | 32 | 10 | 5 |
| Blank et al., 2013 [10] | 160 | 20.9 | 2.5 (30 days) | 13.6 | NR | 22.8 | 11 |
| Wang et al., 2016 [11] | 14 | NR | NR | Not reached | NR | 77 | 50 |
| Gang Wu et al., 2016 [3] | 1273 | NR | NR | 15 | 76 | 26 | 17.5 |
| Saddoughi et al., 2017 [12] | 52 | 10.6 | NR | 10.8 | 29 | 12 | 6 |
| Van Daele et al., 2017 [13] | 12 | 22 | NR | 22 | 41 | 28 | NR |
| Zhang et al., 2019 [14] | 226 | 9 | 14 (90 days) | 11 | 45 | 18.7 | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bardol, T.; Ferre, L.; Aouinti, S.; Dupuy, M.; Assenat, E.; Fabre, J.-M.; Picot, M.-C.; Souche, R. Survival after Multimodal Treatment Including Surgery for Metastatic Esophageal Cancer: A Systematic Review. Cancers 2022, 14, 3956. https://doi.org/10.3390/cancers14163956
Bardol T, Ferre L, Aouinti S, Dupuy M, Assenat E, Fabre J-M, Picot M-C, Souche R. Survival after Multimodal Treatment Including Surgery for Metastatic Esophageal Cancer: A Systematic Review. Cancers. 2022; 14(16):3956. https://doi.org/10.3390/cancers14163956
Chicago/Turabian StyleBardol, Thomas, Lorenzo Ferre, Safa Aouinti, Marie Dupuy, Eric Assenat, Jean-Michel Fabre, Marie-Christine Picot, and Regis Souche. 2022. "Survival after Multimodal Treatment Including Surgery for Metastatic Esophageal Cancer: A Systematic Review" Cancers 14, no. 16: 3956. https://doi.org/10.3390/cancers14163956