
Effect of Smoking on Treatment Efficacy and Toxicity in Patients with Cancer: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Information Sources
2.3. Eligibility Criteria
- (1)
- Included cancer patients regardless of tumor site or type;
- (2)
- Presented data on smoking during a specific oncological therapy irrespective of the type of therapy (external radiotherapy or brachytherapy, chemotherapy, targeted therapies, immunotherapy, endocrine therapy);
- (3)
- Presented data on the association between smoking and treatment efficacy with one of the following outcomes: pathologic complete response (pCR), objective response rate (ORR), locoregional recurrence (LRR; for radiotherapy), event-free survival (EFS; for neoadjuvant setting), disease-free survival (DFS; for adjuvant setting), progression-free survival (PFS; for metastatic setting), treatment-related toxicity;
- (4)
- Compared the treatment efficacy in patients who smoked vs. non-smokers (never or former).
- P: Patients with cancer treated with chemotherapy, radiotherapy, targeted therapies, immunotherapy, or endocrine therapy;
- I: Smoking at the time of therapy initiation and during therapy;
- C: Non-smokers or prior smokers (non-smokers at the time of therapy initiation);
- O: Treatment efficacy in terms of time-to-event measures (LRR for radiotherapy or chemoradiotherapy, EFS for neoadjuvant setting, DFS for adjuvant treatment, PFS for treatment in the metastatic setting), pCR, ORR, and toxicity due to treatment.
2.4. Selection Process
2.5. Data Collection Process
2.6. Outcomes
2.7. Data Synthesis
2.8. Grading the Certainty of Evidence
3. Results
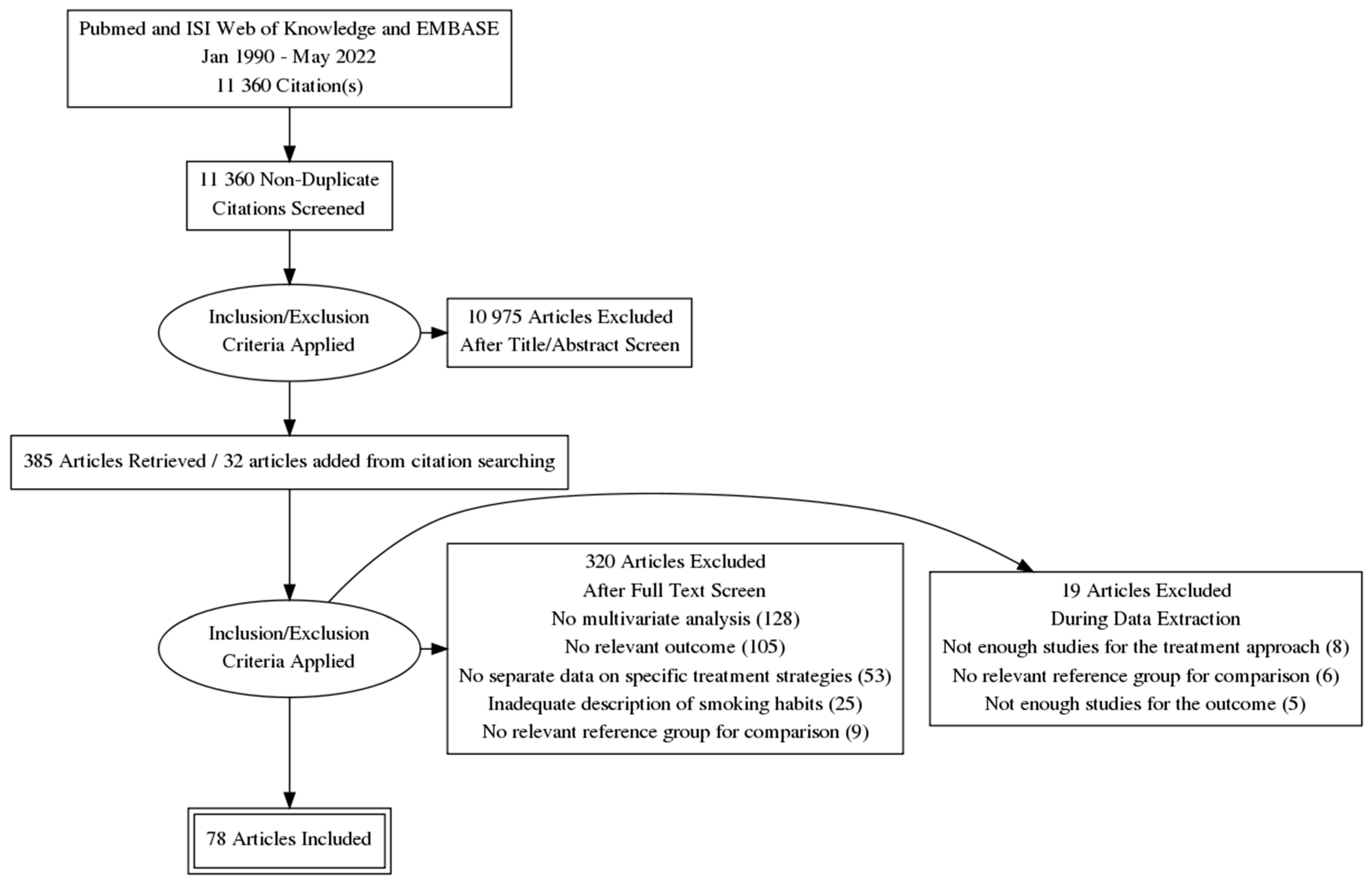
3.1. Literature Search
3.2. Characteristics of Eligible Studies
3.3. Smoking during Radiation Therapy
3.4. Smoking during Chemoradiotherapy
3.5. Smoking during Chemotherapy
3.6. Smoking during Targeted Therapies
3.7. Smoking during Immunotherapy with Checkpoint Inhibitors
3.8. Smoking and Treatment-Related Toxicity
3.9. Subgroup Analyses
3.10. Publication Bias
3.11. Grading the Evidence According to GRADE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agudo, A.; Bonet, C.; Travier, N.; González, C.A.; Vineis, P.; Bueno-de-Mesquita, H.B.; Trichopoulos, D.; Boffetta, P.; Clavel-Chapelon, F.; Boutron-Ruault, M.C.; et al. Impact of cigarette smoking on cancer risk in the European prospective investigation into cancer and nutrition study. J. Clin. Oncol. 2012, 30, 4550–4557. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Botteri, E.; Iodice, S.; Boniol, M.; Lowenfels, A.B.; Maisonneuve, P.; Boyle, P. Tobacco smoking and cancer: A meta-analysis. Int. J. Cancer 2008, 122, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Ordóñez-Mena, J.M.; Schöttker, B.; Mons, U.; Jenab, M.; Freisling, H.; Bueno-de-Mesquita, B.; O’Doherty, M.G.; Scott, A.; Kee, F.; Stricker, B.H.; et al. Quantification of the smoking-associated cancer risk with rate advancement periods: Meta-analysis of individual participant data from cohorts of the CHANCES consortium. BMC Med. 2016, 14, 62. [Google Scholar] [CrossRef] [PubMed]
- Walter, V.; Jansen, L.; Hoffmeister, M.; Brenner, H. Smoking and survival of colorectal cancer patients: Systematic review and meta-analysis. Ann. Oncol. 2014, 25, 1517–1525. [Google Scholar] [CrossRef] [PubMed]
- Bérubé, S.; Lemieux, J.; Moore, L.; Maunsell, E.; Brisson, J. Smoking at time of diagnosis and breast cancer-specific survival: New findings and systematic review with meta-analysis. Breast Cancer Res. 2014, 16, R42. [Google Scholar] [CrossRef]
- van Imhoff, L.C.; Kranenburg, G.G.; Macco, S.; Nijman, N.L.; van Overbeeke, E.J.; Wegner, I.; Grolman, W.; Pothen, A.J. Prognostic value of continued smoking on survival and recurrence rates in patients with head and neck cancer: A systematic review. Head Neck 2016, 38 (Suppl. S1), E2214–E2220. [Google Scholar] [CrossRef]
- Parsons, A.; Daley, A.; Begh, R.; Aveyard, P. Influence of smoking cessation after diagnosis of early stage lung cancer on prognosis: Systematic review of observational studies with meta-analysis. BMJ 2010, 340, b5569. [Google Scholar] [CrossRef]
- Tabuchi, T.; Ito, Y.; Ioka, A.; Nakayama, T.; Miyashiro, I.; Tsukuma, H. Tobacco smoking and the risk of subsequent primary cancer among cancer survivors: A retrospective cohort study. Ann. Oncol. 2013, 24, 2699–2704. [Google Scholar] [CrossRef]
- Taylor, C.; Correa, C.; Duane, F.K.; Aznar, M.C.; Anderson, S.J.; Bergh, J.; Dodwell, D.; Ewertz, M.; Gray, R.; Jagsi, R.; et al. Early Breast Cancer Trialists’ Collaborative Group. Estimating the Risks of Breast Cancer Radiotherapy: Evidence From Modern Radiation Doses to the Lungs and Heart and From Previous Randomized Trials. J. Clin. Oncol. 2017, 35, 1641–1649. [Google Scholar] [CrossRef]
- Mills, E.; Eyawo, O.; Lockhart, I.; Kelly, S.; Wu, P.; Ebbert, J.O. Smoking cessation reduces postoperative complications: A systematic review and meta-analysis. Am. J. Med. 2011, 124, 144–154.e8. [Google Scholar] [CrossRef]
- Sørensen, L.T. Wound healing and infection in surgery. The clinical impact of smoking and smoking cessation: A systematic review and meta-analysis. Arch. Surg. 2012, 147, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, A.L.; Lynch, B.M.; Owen, N.; Aitken, J.F. Lifestyle factors associated concurrently and prospectively with co-morbid cardiovascular disease in a population-based cohort of colorectal cancer survivors. Eur. J. Cancer 2011, 47, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Kenfield, S.A.; Stampfer, M.J.; Chan, J.M.; Giovannucci, E. Smoking and prostate cancer survival and recurrence. JAMA 2011, 305, 2548–2555. [Google Scholar] [CrossRef]
- Smith, J.; Nastasi, D.; Tso, R.; Vangaveti, V.; Renison, B.; Chilkuri, M. The effects of continued smoking in head and neck cancer patients treated with radiotherapy: A systematic review and meta-analysis. Radiother. Oncol. 2019, 135, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Foerster, B.; Pozo, C.; Abufaraj, M.; Mari, A.; Kimura, S.; D’Andrea, D.; John, H.; Shariat, S.F. Association of Smoking Status With Recurrence, Metastasis, and Mortality Among Patients With Localized Prostate Cancer Undergoing Prostatectomy or Radiotherapy: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 953–961. [Google Scholar] [CrossRef]
- de Graan, A.J.; Loos, W.J.; Friberg, L.E.; Baker, S.D.; van der Bol, J.M.; van Doorn, L.; Wiemer, E.A.; van der Holt, B.; Verweij, J.; Mathijssen, R.H. Influence of smoking on the pharmacokinetics and toxicity profiles of taxane therapy. Clin. Cancer Res. 2012, 18, 4425–4432. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, M.; King, A.N.; Conte, M.; Ellingrod, V.L.; Ramnath, N. Effects of cigarette smoking on metabolism and effectiveness of systemic therapy for lung cancer. J. Thorac. Oncol. 2014, 9, 917–926. [Google Scholar] [CrossRef]
- Lee, K.W.C.; Lord, S.J.; Kasherman, L.; Marschner, I.; Stockler, M.; Gralla, R.; Yang, J.C.; Mok, T.; Lee, C.K. The impact of smoking on the effectiveness of immune checkpoint inhibitors—A systematic review and meta-analysis. Acta Oncol. 2020, 59, 96–100. [Google Scholar] [CrossRef]
- Persson, M.; Simonsson, M.; Markkula, A.; Rose, C.; Ingvar, C.; Jernström, H. Impacts of smoking on endocrine treatment response in a prospective breast cancer cohort. Br. J. Cancer 2016, 115, 382–390. [Google Scholar] [CrossRef]
- Sidik, K.; Jonkman, J.N. Robust variance estimation for random effects meta-analysis. Comput. Stat. Data Anal. 2006, 50, 3681–3701. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Andrews, J.; Guyatt, G.; Oxman, A.D.; Alderson, P.; Dahm, P.; Falck-Ytter, Y.; Nasser, M.; Meerpohl, J.; Post, P.N.; Kunz, R.; et al. GRADE guidelines: 14. Going from evidence to recommendations: The significance and presentation of recommendations. J. Clin. Epidemiol. 2013, 66, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.W.; Romano, M.A.; Kudrimoti, M.R.; Randall, M.E.; McGarry, R.C.; Singh, A.K.; Rangnekar, V.M. Nicotinic modulation of therapeutic response in vitro and in vivo. Int. J. Cancer 2012, 131, 2519–2527. [Google Scholar] [CrossRef] [PubMed]
- Wouters, B.G.; Brown, J.M. Cells at intermediate oxygen levels can be more important than the "hypoxic fraction" in determining tumor response to fractionated radiotherapy. Radiat Res. 1997, 147, 541–550. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Ando, M.; Maemondo, M.; Yamamoto, S.; Isa, S.; Saka, H.; Kubo, A.; Kawaguchi, T.; Takada, M.; Rosell, R.; et al. The role of smoking status on the progression-free survival of non-small cell lung cancer patients harboring activating epidermal growth factor receptor (EGFR) mutations receiving first-line EGFR tyrosine kinase inhibitor versus platinum doublet chemotherapy: A meta-analysis of prospective randomized trials. Oncologist 2015, 20, 307–315. [Google Scholar] [CrossRef]
- Li, X.; Huang, C.; Xie, X.; Wu, Z.; Tian, X.; Wu, Y.; Du, X.; Shi, L. The impact of smoking status on the progression-free survival of non-small cell lung cancer patients receiving molecularly target therapy or immunotherapy versus chemotherapy: A meta-analysis. J. Clin. Pharm. Ther. 2021, 46, 256–266. [Google Scholar] [CrossRef]
- Wang, S.; Takayama, K.; Tanaka, K.; Takeshita, M.; Nakagaki, N.; Ijichi, K.; Li, H.; Nakanishi, Y. Nicotine induces resistance to epidermal growth factor receptor tyrosine kinase inhibitor by α1 nicotinic acetylcholine receptor-mediated activation in PC9 cells. J. Thorac. Oncol. 2013, 8, 719–725. [Google Scholar] [CrossRef]
- Hamilton, M.; Wolf, J.L.; Rusk, J.; Beard, S.E.; Clark, G.M.; Witt, K.; Cagnoni, P.J. Effects of smoking on the pharmacokinetics of erlotinib. Clin. Cancer Res. 2006, 12, 2166–2171. [Google Scholar] [CrossRef]
- Nie, R.C.; Duan, J.L.; Liang, Y.; Chen, X.J.; Chen, Y.M.; Luo, T.Q.; Chen, G.M.; Wang, Y.; Li, Y.F. Smoking status-based efficacy difference in anti-PD-1/PD-L1 immunotherapy: A systematic review and meta-analysis. Immunotherapy 2020, 12, 1313–1324. [Google Scholar] [CrossRef]
- Zhao, W.; Jiang, W.; Wang, H.; He, J.; Su, C.; Yu, Q. Impact of Smoking History on Response to Immunotherapy in Non-Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis. Front Oncol. 2021, 11, 703143. [Google Scholar] [CrossRef]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.L.; et al. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421. [Google Scholar] [CrossRef]
- Chae, Y.K.; Davis, A.A.; Raparia, K.; Agte, S.; Pan, A.; Mohindra, N.; Villaflor, V.; Giles, F. Association of Tumor Mutational Burden With DNA Repair Mutations and Response to Anti-PD-1/PD-L1 Therapy in Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2019, 20, 88–96. [Google Scholar] [CrossRef]
- Wang, X.; Ricciuti, B.; Alessi, J.V.; Nguyen, T.; Awad, M.M.; Lin, X.; Johnson, B.E.; Christiani, D.C. Smoking History as a Potential Predictor of Immune Checkpoint Inhibitor Efficacy in Metastatic Non-Small Cell Lung Cancer. J. Natl. Cancer Inst. 2021, 113, 1761–1769. [Google Scholar] [CrossRef] [PubMed]
- Fukuokaya, W.; Kimura, T.; Yanagisawa, T.; Kimura, S.; Tsuzuki, S.; Koike, Y.; Iwamoto, Y.; Enei, Y.; Tanaka, M.; Urabe, F.; et al. Impact of Dose-Effect in Smoking on the Effectiveness of Pembrolizumab in Patients with Metastatic Urothelial Carcinoma. Target. Oncol. 2021, 16, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ricciuti, B.; Nguyen, T.; Li, X.; Rabin, M.S.; Awad, M.M.; Lin, X.; Johnson, B.E.; Christiani, D.C. Association between Smoking History and Tumor Mutation Burden in Advanced Non-Small Cell Lung Cancer. Cancer Res. 2021, 81, 2566–2573. [Google Scholar] [CrossRef]
- Metelli, S.; Chaimani, A. Challenges in meta-analyses with observational studies. Evid. Based Ment Health 2020, 23, 83–87. [Google Scholar] [CrossRef]
- Altman, D.G. Clinical trials: Subgroup analyses in randomized trials—More rigour needed. Nat. Rev. Clin. Oncol. 2015, 12, 506–507. [Google Scholar] [CrossRef] [PubMed]
- Cinciripini, P.M.; Karam-Hage, M.; Kypriotakis, G.; Robinson, J.D.; Rabius, V.; Beneventi, D.; Minnix, J.A.; Blalock, J.A. Association of a Comprehensive Smoking Cessation Program With Smoking Abstinence Among Patients With Cancer. JAMA Netw. Open 2019, 2, e1912251. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N Studies | Assessment of Evidence | Effect | Certainty of Evidence | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Study Design | Bias | Inconsistency | Indirectness | Imprecision | Other | N Patients | Pooled Effect (95% CI) | ||
| Locoregional recurrence after radiotherapy in patients who smoke versus non-smokers | |||||||||
| 10 | observation | Serious | Not serious | Not serious | Not serious | No | 13276 | 1.56 (1.28–1.91) | ⨁⨁⨁◯ Moderate |
| Disease-free survival after radiation therapy in patients who smoke versus patients who do not smoke | |||||||||
| 9 | observation | Serious | Not serious | Not serious | Not serious | No | 11185 | 1.88 (1.21–2.90) | ⨁⨁⨁◯ Moderate |
| Locoregional recurrence after chemoradiotherapy in patients who smoke versus patients who do not smoke | |||||||||
| 3 | observation | Serious | Not serious | Not serious | Serious | No | 339 | 4.28 (2.06–8.09) | ⨁⨁◯◯ Low |
| Disease-free survival after chemoradiotherapy in patients who smoke versus patients who do not smoke | |||||||||
| 7 | observation | Serious | Not serious | Not serious | Not serious | No | 2096 | 1.92 (1.41–2.62) | ⨁⨁⨁◯ Moderate |
| Progression-free survival of chemotherapy in patients who smoke vs. non-smoking patients | |||||||||
| 6 | observation | Serious | Serious | Not serious | Not serious | No | 1489 | 1.22 (0.63–2.36) | ⨁⨁◯◯ Low |
| Progression-free survival of EGFR-TKIs in patients who smoke vs. non-smoking patients | |||||||||
| 16 | observation | Serious | Not serious | Not serious | Not serious | No | 7682 | 1.46 (1.21–1.77) | ⨁⨁⨁◯ Moderate |
| Progression-free survival of immunotherapy in patients who smoke vs. non-smoking patients | |||||||||
| 11 | observation | Serious | Not serious | Not serious | Not serious | No | 4568 | 0.70 (0.61–0.82) | ⨁⨁⨁◯ Moderate |
| Radiation-induced toxicity in patients who smoke vs. non-smoking patients | |||||||||
| 15 | observation | Serious | Not serious | Not serious | Not serious | No | 6776 | 1.84 (1.32–2.56) | ⨁⨁⨁◯ Moderate |
| Chemotherapy-induced toxicity in patients who smoke compared to patients who do not smoke | |||||||||
| 9 | observation | Serious | Serious | Not serious | Serious | No | 3307 | 0.92 (0.53–1.60) | ⨁◯◯◯ Very low |
| Chemoradiotherapy-induced toxicity in patients who smoke vs. non-smoking patients | |||||||||
| 4 | observation | Serious | Not serious | Not serious | Serious | No | 415 | 2.43 (1.45–4.07) | ⨁⨁◯◯ Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bergman, M.; Fountoukidis, G.; Smith, D.; Ahlgren, J.; Lambe, M.; Valachis, A. Effect of Smoking on Treatment Efficacy and Toxicity in Patients with Cancer: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 4117. https://doi.org/10.3390/cancers14174117
Bergman M, Fountoukidis G, Smith D, Ahlgren J, Lambe M, Valachis A. Effect of Smoking on Treatment Efficacy and Toxicity in Patients with Cancer: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(17):4117. https://doi.org/10.3390/cancers14174117
Chicago/Turabian StyleBergman, Marie, Georgios Fountoukidis, Daniel Smith, Johan Ahlgren, Mats Lambe, and Antonios Valachis. 2022. "Effect of Smoking on Treatment Efficacy and Toxicity in Patients with Cancer: A Systematic Review and Meta-Analysis" Cancers 14, no. 17: 4117. https://doi.org/10.3390/cancers14174117
APA StyleBergman, M., Fountoukidis, G., Smith, D., Ahlgren, J., Lambe, M., & Valachis, A. (2022). Effect of Smoking on Treatment Efficacy and Toxicity in Patients with Cancer: A Systematic Review and Meta-Analysis. Cancers, 14(17), 4117. https://doi.org/10.3390/cancers14174117